
Abstract
This study investigates medical trainees’ experiences with dying and death, by means of semistructured interviews. Nine medical students and nine residents reported a total of 114 experiences. The great majority of these experiences took place during the final year of medical school. The authors identified the latent characteristics, which illustrate an in-depth understanding of the significance of the described experiences. Three main themes emerged: circumstances of death, personal relationship, and one’s own role. The age of the dying person, the extent of suffering, time frame and setting, and the patients’ behaviors were factors that influence the perceptions of the experiences. The interviewees reported powerful emotional consternation by the patients’ deaths with whom they had developed a close relationship. Failure, helplessness, and guilt were negatively associated perceptions of one’s own role. This study illustrates the tension between emotional concern and professional detachment. It highlights the continuing existence of a physician image, in which control represents the key issue.
Dealing with dying and death is an inevitable aspect of the medical profession, which often poses strong emotional challenges to physicians, especially to younger doctors and medical students (Aase, Nordrehaug, & Malterud, 2008; Jackson et al., 2005; MacLeod, 2001; MacLeod, Parkin, Pullon, & Robertson, 2003; Wilson & Ayers, 2004). The clerks and residents in Jackson et al.’s (2005) study, for example, were more likely to describe death as a shocking event than the attending physicians. Physicians’ emotional reactions to patients’ deaths can affect their sense of well-being and the manner in which they deal with (dying) patients, hence influencing the quality of their patient care in general (Jackson et al., 2005; Meier, Back, & Morrison, 2001). These consequences are reinforced by the widespread absence of reflection on these emotions in the medical practice (Meier et al., 2001).
The number of studies that deal with medical trainees’ experiences with regard to dying and death is surprisingly low. The existing studies largely focus on the evaluation of end-of-life (EOL) curricula as well as on the aspirations for preparation for EOL care (Anneser, Kunath, Krautheim, & Borasio, 2014; Fraser, Kutner, & Pfeifer, 2001; Hall, Lieto, & Martin, 2017; Maxwell, Passow, Plumb, & Sifri, 2002; Ratanawongsa, Teherani, & Hauer, 2005; Wear, 2002). Like the doctors in the study by MacLeod (2001), students do not think that they are adequately prepared by their preclinical training and sufficiently supported by their supervisors concerning EOL issues (Anneser et al., 2014; Fraser et al., 2001; Rhodes-Kropf et al., 2005; Wear, 2002). The patients approaching death also indicated gaps in the medical education and could sense the discomfort that physicians felt in discussing the illness with them (Janssen & MacLeod, 2010). Furthermore, some previous research has investigated the physicians’ emotional experiences of dying and death. It has been reported that witnessing death causes strong feelings of sadness, anxiety, guilt, helplessness, frustration, and anger both in experienced physicians and in medical trainees (Batley et al., 2017; Jackson et al., 2005; MacLeod, 2001; Pessagno, Foote, & Aponte, 2013; Rhodes-Kropf et al., 2005). Coping strategies such as talking, focusing on work, crying, rationalization, and cognitive avoidance have been identified (Bovero, Tosi, Miniotti, Torta, & Leombruni, 2018; Pessagno et al., 2013; Ratanawongsa et al., 2005; Rhodes-Kropf et al., 2005; Smith-Han, Martyn, Barrett, & Nicholson, 2016). Experiences with death also often lead to a change in young physicians’ perceptions of the role of the doctor from being one of curative to one that is caring; their perceptions of medicine may also change from preventing death to preserving quality of life and lead them to see death as part of life (Maxwell et al., 2002; Ratanawongsa et al., 2005; Smith-Han et al., 2016). Finally, concerning ways of addressing the emotional impact of patients’ deaths on trainees, positive role-modelling from clinical staff, and reflective practices can turn these unpleasant events into rich learning experiences for trainees (Ratanawongsa et al., 2005).
In this study, we seek to close the gap in the literature which does not sufficiently address becoming physicians’ authentic experiences with dying and death of patients and which does not take private experiences with this into account. The current research is set out to address the following question: Which experiences with regard to dying and death do final-year medical students and residents in the midterm of their residency describe as most significant?
Method
Sample
All the students in the second and third tertial of the final year (Praktisches Jahr) 1 at TUM School of Medicine were invited by e-mail to participate in the study. Nine medical students agreed to participate in the study. Nine residents in the midterm of their residency 2 from different specialties at the TUM University Hospital Rechts der Isar were purposely recruited for the interview. We strove for a heterogeneous group of medical professionals to investigate possible differences between the students’ and residents’ experiences and also record the possible differences in the physicians’ areas of expertise. We offered a book voucher as an incentive. Interviewees’ characteristics are shown in Table 1.
Characteristics of Final-Year Medical Students and Midterm Residents.
Data Collection
From December 2013 to April 2014, we conducted 18 semistructured interviews. We obtained informed consent from all participants before data collection. Initially, the interviewees were asked to elaborate their most significant experiences of dying and death. To elicit the participants’ authentic perspectives without influencing their stories, we refrained from specifying the contexts. The interview guide (see Appendix) was used to delve into the participants’ responses to the relevant topics, which were not raised by them.
Two pilot interviews were performed in the presence of an expert in qualitative interviewing to optimize our interviewing techniques. As the quality of these two interviews was considered satisfactory, these were subsequently included in the data set. Each interview lasted for about an hour (an average of 57 minutes, ranging from 45 to 70 minutes) and was tape-recorded and transcribed verbatim. Ethical approval was granted by the Ethics Committee of the Faculty of Medicine at Technical University of Munich (Project Number 42/14).
Data Analysis
The data were analyzed using the qualitative content analysis (QCA) approach by Schreier (2012). This is a method for systematically describing the meaning of qualitative data by assigning successive parts of the material to the categories of a coding frame. QCA aims to gain an understanding of social phenomena through interpretation of recorded communication. The strength of QCA is its systematic nature that requires the same sequence of steps and therefore contributes to reliability. The inductive category development, through which the categories emerge from the data, ensures that the coding frame adequately represent the concepts in the data. Finally, QCA is a resource-efficient approach as it reduces the data by limiting the analysis to the relevant aspects of the material.
The data analysis consisted of five steps: (a) Two researchers independently open coded four randomly selected interviews to generate data-driven categories. (b) The data categories were arranged into a hierarchical structure, and a coding frame was created. This consisted of the main categories (specifying the relevant aspects) and subcategories (specifying the relevant meanings concerning these aspects). The initial coding frame was tested on four interviews. In an iterative process, the researchers discussed the differences and modified the coding frame. (c) The researchers applied the coding frame to all the transcripts by assigning segments of the material to the categories using MAXQDA 12 for Windows. (d) Following Schmidt’s (2009) suggestion, we generated quantitative category tables, containing information about the occurrences of certain categories and the possible connections between the categories in the data. (e) Finally, we performed a cross-case analysis of each subcategory and wrote memos against each category to structure and reflect on the data.
Results
The interviewees reported a total of 114 experiences of dying and death. The number of recounted experiences ranged widely from 3 to 11 per interviewee (an average of 6). The analysis revealed (a) the manifest characteristics that capture the circumstances of the described experiences, answering the key questions such as who, what, where, when, and in which context; and (b) the latent characteristics that indicate deeper understanding of the significance of the interviewees’ personal experiences. We present the main findings of our study following the same structure as the coding frame.
Manifest Characteristics of the Experiences
We identified five manifest themes that described the experiences of the participants: type of dying person, cause of death, location of experience, time of experience, and type of educational format.
In 71% (81 out of 114) of the described experiences, the dying person was a patient, only about 17% (19) of the cases described the death of family members, most notably grandparents. The most frequent cause of death was oncological (35%, 40), which echoes the findings from previous studies (Jackson et al., 2005; Rhodes-Kropf et al., 2005). Trauma was the second most frequent cause of death (10%, 11). In many cases, caring for accident victims was associated with dramatic images of injuries. The confrontation with an accident that resulted in a sudden death often increased worries about one’s own mortality. Of all the cases, 67% (76) of the described experiences occurred in a hospital. We identified three significant wards in hospital settings: the intensive care unit (26%, 20 out of 76), pediatric oncology (21%, 16), and internal medicine (16%, 12). Only two experiences in the palliative care units were shared. This may be due to the fact that working in the palliative care unit is not compulsory for students and residents in Germany. In 43 (38%) out of 114 cases, the stage of educational training in which the described experiences took place could be determined. In 47% (20 out of 43) of the cases, most of the described experiences occurred in the final year of the trainees’ studies. This illustrates clearly that the interviewees chose to recount the more recent incidents. In 26% (11) of the cases, the nursing clerkship 3 was the second frequently mentioned period in which the narrated experiences took place, albeit dating back to many years earlier. In several cases, these shared experiences concerned the first encounters with death or caring of a dying patient. Table 2 presents more detailed information on the identified subcategories and their relative distribution among the described experiences.
Distribution of the Manifest Characteristics of the Experiences Described by Final-Year Medical Students and Midterm Residents.
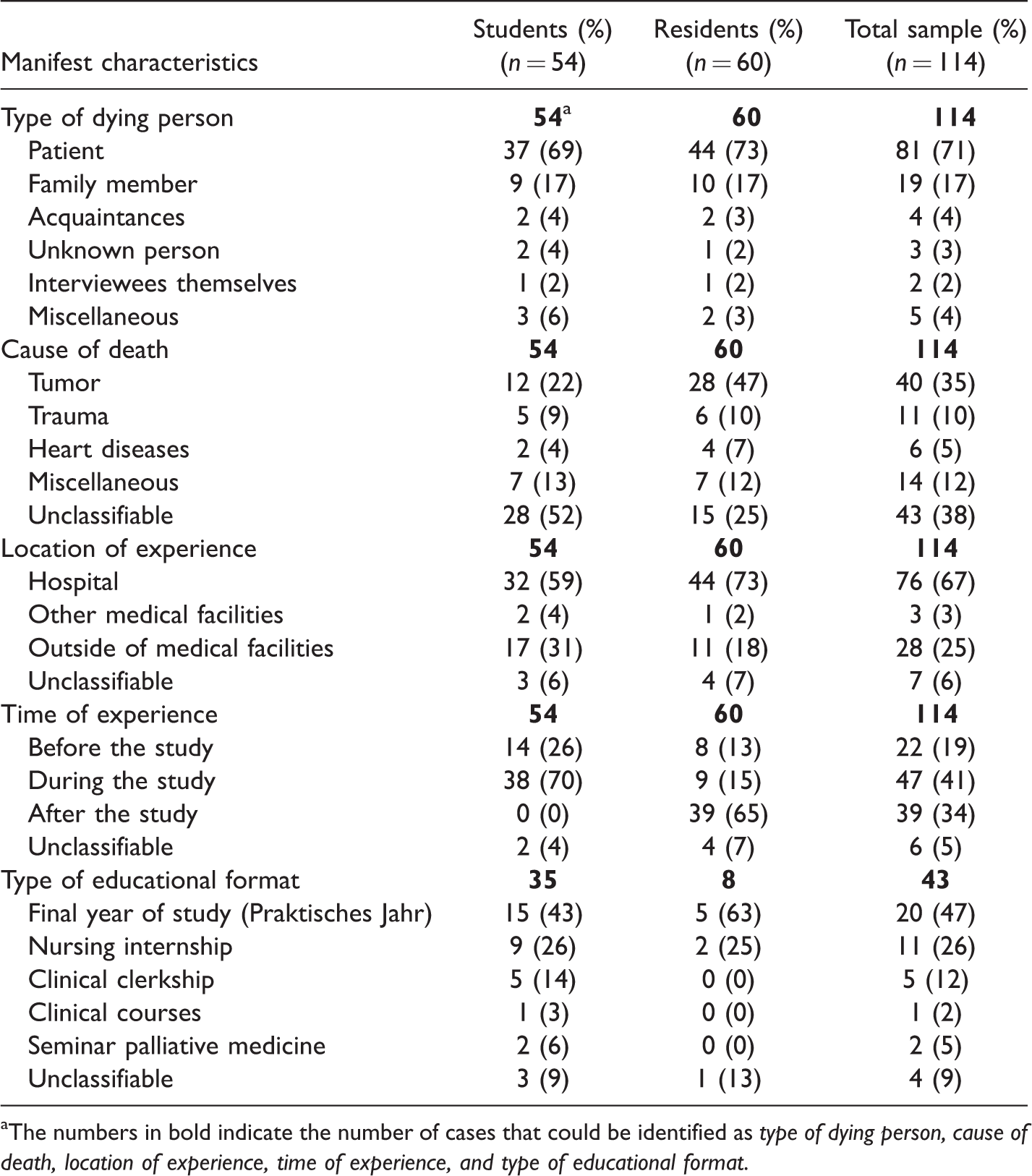
The numbers in bold indicate the number of cases that could be identified as type of dying person, cause of death, location of experience, time of experience, and type of educational format.
Latent Characteristics of the Experiences
We also focused on the latent characteristics of the experiences, which indicate deeper understanding of the significance of the personal experiences. The following three main themes were identified: circumstances of death, personal relationship, and ‘one’s own role.
Circumstances of death
This first main latent theme defined the qualitative character of the experiences, which was mentioned by all the interviewees. The following six thematic variations were identified: sudden death, beautiful death, young death, suffering death, dramatic death, and lonely death. We discuss these variations in accordance with their frequency.
Sudden death
Of all the participants, 78% (14 out of 18; 7 students and 7 residents) mentioned sudden death. In accordance to previous studies, sudden death is primarily associated with the most intense and negative emotional experiences (Batley et al., 2017; Jackson et al., 2005; Kelly & Nisker, 2010; Rhodes-Kropf et al., 2005). It tends to evoke shock and strong feelings of anxiety, particularly among the medical students. This is how one interviewee described the experience: The decay. At first, when you can still talk to the person in a normal way at the beginning and then you see, then it goes rapidly. And that was actually the shocking thing, when you think okay, it can go that fast now […]. From one hundred percent to zero.
4
2. Beautiful death
Of all the interviewees, 72% (7 students and 6 residents) described their experiences of beautiful or good death. Echoing previous studies, the participants stated the absence of physical and mental suffering as a precondition for this type of death (Jackson et al., 2005; Meffert, Stößel, Körner, & Becker, 2015). Moreover, being at home and surrounded by one’s loved ones was a factor that rendered this death beautiful (Meffert et al., 2015). Several interviewees emphasized that the dying person’s attitude toward their own death is crucial. Acceptance of death was somehow seen as a precondition for a beautiful death.
Some interviewees associated sudden death with less suffering and distressing confrontation with the approaching death and hence synonymous with beautiful death. However, other participants appreciated the significance of having enough time to say goodbye to one’s loved ones, to settle unresolved matters, and to develop an accepting attitude toward one’s own death. Several participants stressed the importance of timely and clear communication from medical professionals concerning patients’ prognoses to enable beautiful death: […] both my private and professional experiences have shown me that you have to deal openly with the situation, when you see it comes to an end or the patient has an incurable disease that will probably also lead to death in the near future, that you prepare people so that they have time for arrangements and providing for a closure.
3. Young death
The theme of young death was mentioned by 72% of the interviewees (8 students and 5 residents), where grief, anger, and guilt were identified as leading emotions. In several cases, the interviewees—being young people themselves—projected their own life expectations on the dying person. This led to high levels of empathy but also considerable psychological distress: “So that’s sadder and it touches you more because it’s closer to yourself, because you know yourself how you are at that age, that you have made plans, but that all this doesn’t work out any more […].”
In line with previous studies, young death was perceived as meaningless, unfair, and difficult to deal with (Aase et al., 2008; Batley et al., 2017; Jackson et al., 2005; Kelly & Nisker, 2010; Pessagno et al., 2013). One resident described it thus: […] I somehow always have the feeling, when very young people die, that this is much, much worse than when very old people die, because an 84-year-old grandpa who has five grandchildren and had a job and kids and they have kids themselves, he has had a nice life and that is also good and okay, one day you can and must just die. And for patients who die very young, especially when they die under somehow very pointless or tragic circumstances, it just touches me more, because I always have the feeling that half their lives has simply been stolen. And that’s why I think it’s so bad.
4. Suffering death
Of all the interviewees, 44% (4 students and 4 residents) spoke about death following a period of suffering. The presence of severe physical discomfort (pain and deterioration of health condition) and emotional suffering (anxiety and unrest) were contributing to the perception of death as being suffering, and hence contrasting the notion of beautiful death described earlier. Echoing Rhodes-Kropf et al.’s (2005) findings, our interviewees reported powerful emotional reactions to suffering death. As noted earlier, time was identified as one crucial factor: Long-term suffering before death led to experience death as anguish. Moreover, this type of death roused some participants’ anxiety that they would experience such death themselves, and hence their wish for sudden death. Interestingly, for several participants, the experience of suffering death had changed their attitudes toward death, viewing it as a release: So I also have patients, so now in the practical year, where I say myself, he really is so worse off, then has really oedema on his arms and then I shall put a needle there, but he doesn’t react at all and, he lies there only with an open mouth, the one old man, then I think also, that’s okay if he dies now.
5. Dramatic death
Of all the participants, 28% (2 students and 3 residents) mentioned dramatic death. The image of dramatic death was primarily associated with the use of life-saving medical measures, which were often perceived as desperate, invasive, or brutal by the interviewees: And where even as an outsider, when you watch, you think whether this is still human, what is being done or whether it is also extremely inhuman, to still do so many things and at some point you also have to say where the limit is and where the limit is crossed. I found it tough to watch it. 6. Lonely death
Two students recounted episodes of patients who had died in solitude. They described these experiences as unpleasant and tragic, especially when compared with beautiful death, which happens at home where patients are surrounded by their loved ones.
Personal relationship
This second main latent theme specifies the characters of the interviewees’ personal relationships with the patients. This topic was raised by 78% of the interviewees (7 students and 7 residents). The following crucial factors led to the building of a personal relationship with the patients: (a) medical care lasting for an extended period of time; (b) friendly personality of the dying person and her or his relatives; (c) patients’ dealing with their own illness, especially when exhibiting a positive attitude or a strong willpower; (d) patients’ resemblance, either in appearance or in medical condition, to the interviewees’ family members; (e) identification with the patients; and (f) interviewees’ own participation in the surgery and invasive procedures. One participant related the following comment: […] that touches you much differently, if it is someone, who has just the same age, at least for me, when you have someone, who has the exact same age as you, yes. […] And she then also had her iPod with her, for example, and she listened to exactly the same music as I do, yes, and that’s just really, that’s even a bit closer to you.
Confirming previous research findings, our results illustrate that personal relationships with patients can lead to more emotional consternation following patients’ death (Batley et al., 2017; Jackson et al., 2005; MacLeod et al., 2003; Redinbaugh et al., 2003). These strong emotional responses often led to the interviewees feeling dissatisfied and sad over longer periods of time. In such circumstances, several residents emphasized the importance of keeping a certain distance from the patients to protect their mental and emotional well-being. Consistent with previous research results, many participants spoke about the conflict between emotional concern and professional detachment (Kelly & Nisker, 2010; Kuczewski et al., 2014; Smith-Han et al., 2016). The students specifically displayed uncertainty about the extent to which a physician should be emotionally engaged with their patients and the consequences of their involvement: But on the other hand I also thought, maybe it is almost desirable that one somehow in course of your job learns this sober approach […], to be able to push it away even better and simply to be able to deal with these people better or whether I just want to keep a little more feeling in it. For that reason, I really always was very confused and torn between, whether I shall find this good or bad, how the physician and the whole staff has dealt with these things.
One’s own role
Awareness of one’s own role also influenced perceptions of the experienced events. This subject was mentioned by 89% of the interviewees (8 students and 8 residents), where they discussed their own contribution and efficacy when encountering the event.
The following six thematic variations of the category one’s own role were identified in our study: helplessness, failure, feelings of inner satisfaction, not in charge, avoidance, and guilt. We discuss these variations in accordance with their frequency.
Helplessness
Half the participants (50%, 1 student and 8 residents) spoke about helplessness. This notion was associated with a lack of professional competence and uncertainty about the accuracy of one’s own decisions as well as with the inability to prevent death: So that was panic and fear, I must say quite honestly. So that we really stand next to it helplessly and say, he will turn and turn and turn and can’t do anything. Where you’ve always learned, yes, morphine helps. […] Yes, it was such a feeling where you just have to watch helplessly as someone dies. Where they say there’s nothing they can do about it and they can’t even make it easier for him.
2. Failure
Half of the interviewees (50%, 3 students and 6 residents) mentioned failure. Feelings of failure were experienced when the respondents did not succeed in fulfilling the expectations they had of themselves, such as curing diseases, enabling beautiful death, keeping control over clinical situations, and concealing one’s own emotions.
In addition, patients’ and their relatives’ behaviors, blaming the medical staff for the patients’ hopelessness, and absence of healing induced a strong sense of responsibility and led the participants to interpret therapeutic failure as a personal failure, which resulted in doubts about their own competencies. This is what a resident said: […] the worst feeling was actually, losing control so completely in this situation. […] And to have this loss of control and to know exactly, that exactly the opposite is expected of you, namely to keep the overview and to keep control, that was something very, very difficult, yes?!
3. Feelings of inner satisfaction
Less than half the participants (44%, 4 students and 4 residents) talked about inner satisfaction, induced by feeling that one has done the right thing This was the only positive theme that we found was associated with the participants’ perception of their own role. The most frequently mentioned cases in this regard included those where the interviewees had acted to enable the patients to die a beautiful death (Jackson et al., 2005): “[…] this fulfilled feeling, that you have just accompanied someone in a very beautiful process of dying.”
In this context, the residents primarily focused on the pragmatic and somehow technical dimensions of dying, including the effective management of pain, fulfilling the desires of the dying person, and having open and honest communication about the dying person’s prognoses and prospects. The students focused more on the psychosocial or spiritual aspects of dying and thought that it was particularly important to have respectfully accompanied a dying person.
4. Not in charge
The subject of not in charge was referred to by 33% of the interviewees (3 students and 3 residents), who mainly recalled situations in which they had criticized their senior colleagues’ excessive use of aggressive therapies and life-prolonging measures. The interviewees describe being in a passive position in these situations. They criticized the physicians’ late or dishonest communication about the patients’ prognoses, hence depriving them of their desired way of death: That is a general point, too, that physicians do not do that, they still like to put options on the table, although there are actually none left. Because this is the easier way than saying yes, we’re sorry, but there’s nothing more we can do. And that’s actually something I don’t want to do. Well, I would actually like to try to tell the patient honestly, but I can’t say it yet either, because I haven’t been in the physician role yet. Now, as a medical student, I don’t see myself in that role. 5. Avoidance
Only 28% of the participants (2 students and 3 residents) recounted experiences in which they had consciously avoided confronting specific situations to protect themselves against negative feelings. In most of these cases, they described how they had avoided direct contact with the dying person. Two even said that they had avoided a member of their own family who was dying. The participants’ professional knowledge and experience affected the ways in which they handled the death of their family members. One interviewee explained how he had deliberately avoided visiting a dying family member in an intensive care unit in an effort to save himself a pleasant memory of his relative: […] my experience is basically, that patients, in intensive care who are intubated and ventilated and dying, have very little to do with patients, who are awake at the normal ward. And you also don’t recognize them anymore. They have a completely different face and they just look completely different. And then I thought to myself, so I really don’t want to go there, to see how he looks different now, I want to save myself from this.
6. Guilt
Only 22% of all the participants (1 medical student and 3 residents) spoke about the feeling of guilt. Guilt was induced by participants’ actions or by inaction, resulting in a patient’s death (Jackson et al., 2005): Yes, that is quite strange, because on the one hand, you start to weigh things up a bit. […] then you think, did you somehow do something wrong procedurally and was it really such a negligent fault or was it just something that simply happened, because it would have happened anyway, yes, and then you also fluctuate between all these extremes relatively often, yes?
Discussion
This study investigated final-year medical students’ and midterm residents’ most significant experiences with regard to dying and death. The interviewees recounted a total of 114 experiences. We identified five manifest themes, which captured the circumstances of the described events, answering the key questions of who, what, where, when, and in which context: type of dying person, cause of death, location of experience, time of experience, and type of educational format. The great majority of the described experiences involved encounters with patients’ deaths, with the oncological diseases constituting the leading cause of death. Most of the experiences took place in a hospital and occurred in the final year of the medical school and during nursing clerkships. Our findings exemplify the great importance of the first encounter with dying and death. These results correspond with the findings of the study by Wilson and Ayers (2004) where medical students were asked to write thought-provoking episode reports and described their first clinical encounter with patients who were suffering, were dying, or had died. The significance of the small number of personal experiences should not be overlooked, especially because several interviewees explicitly stated that they were most strongly influenced by the death of a close relative.
In addition, the latent characteristics illustrate a profound understanding of the significance and the qualitative judgment of the personal experiences. Three main themes emerged: circumstances of death, personal relationship, and one’s own role. These themes exhibit further differentiations and are closely interconnected.
Concerning the circumstances of death, the age of the dying person, the extent of the suffering, the time frame and the setting, and the patients’ and their relatives’ behaviors were identified as factors that can determine the qualitative character of the dying experience and decisively influence the perceptions of these events. Corresponding to previous studies, while death at a young age was viewed as emotionally disturbing, death at an older age was seen as less emotionally distressing (Kelly & Nisker, 2010; Pessagno et al., 2013). Echoing previous research, the presence of physical and mental suffering made the experience difficult to deal with (Wilson & Ayers, 2004). The absence of suffering, on the contrary, was seen as a precondition for beautiful death. Moreover, conditions surrounding death, especially being at home surrounded by one’s loved ones, play an important role in perceiving death as beautiful, while dying in solitude in a clinical environment was perceived as daunting and undesirable. With regard to the time frame of death, we discovered two contradictory perspectives. On one hand, the interviewees associated sudden death with a reduction in suffering and with avoiding a distressing mental confrontation with the approaching death. Therefore, sudden death was often viewed as beautiful death. On the other hand, the participants appreciated creating the space for one’s EOL. The patients’ and their relatives’ behaviors, especially the dying patients’ attitudes toward their own death, were identified as another factor that influences the extent to which death is described as beautiful. We found that different circumstances of death rouse different intense emotional experiences. Hence, witnessing sudden death, death of a young person, and death after a period of suffering were particularly stressful and emotionally disturbing for our interviewees. Shock, grief, and anxiety were found as the leading emotions.
Among others, long-lasting medical care and patients’ dealing with their own illness were identified as factors that led to a personal relationship between the interviewees and the patients. Confirming the previous literature, our findings show that patients’ death caused the participants to feel strong emotional consternation, especially if they had built intimate personal relationships with them (Jackson et al., 2005; MacLeod et al., 2003; Redinbaugh et al., 2003). This led the interviewees to blame themselves for their patients’ death, causing them to feel sad. Our study illustrates the tension between emotional concern and professional detachment, particularly for the students; the literature has identified this conflict as a central dilemma worrying aspiring physicians (Kuczewski et al., 2014; Ratanawongsa et al., 2005; Smith-Han et al., 2016).
Failure, helplessness, and guilt were negatively associated perceptions of one’s own role and primarily characterized the narratives of the residents. This can be explained by their higher extent of accountability compared with the students (Batley et al., 2017; Jackson et al., 2005). These negative assessments of one’s own actions seem to emanate from the existence of a physician image, requiring that they should prevent death, cure diseases, and not make mistakes (Fox, 1997). Control represents a key issue in this context (Kelly & Nisker, 2010). Controlling the clinical situations and one’s own emotions was repeatedly mentioned as a precondition for the medical profession by our interviewees. Strong emotional consternation at times of intimate relationships with patients caused our interviewees to fear losing control. Loss of control by witnessing sudden death or death of a youngster evoked feelings of helplessness, failure, and guilt in our participants, causing them to doubt their own competencies and to realize the impossibility of keeping control over all situations as a physician.
The professional hierarchy in work contexts in health care constituted another recurring topic in our data. This subject was primarily discussed in connection with life-saving medical measures and doctor–patient communication. Some participants sharply criticized the excessive use of aggressive therapies and life-prolonging measures, particularly when describing dramatic deaths upon which they had limited influence and responsibility due to their low status in the professional hierarchy. Furthermore, interviewees criticized physicians’ late or dishonest communication regarding the patient’s prognosis, hence depriving them of their desired way of death. These findings are consistent with those of Wilson and Ayers (2004): These authors identified disrespectful doctor interactions with patients as one of the major themes in the medical students’ thought-provoking episode reports leading them to question their own role in the medical ward. Furthermore, medical students appeared to be less comfortable in their role of learning student in relation to their patients. Wilson and Ayers (2004) assume that the limited opportunities for medical interventions and the extended period of time as observers could lead to anxieties about their role and less comfort with practicing on patients for their educational benefits. Our interviewees also complained about this lack of accountability and their limited decision-making power.
Feelings of inner satisfaction were the only positive assessment of one’s own role, gained either by acting in favor of others or through performing actions that positively affected the interviewees’ self-perception.
Our study is performed at one institution. As always in qualitative research, caution is advised when extrapolating the findings of this research to other contexts. However, it gives useful and differentiated insights into the manifest and latent characteristics of significant experiences of two crucial groups (i.e., final-year medical students and midterm residents).
In summary, the results illustrate that experiences relating to dying and death in the professional medical practice are complex and multifaceted. Not only do they pose severe personal, cognitive, emotional, and social challenges to (aspiring) physicians, but they also rouse feelings of inner satisfaction, interpersonal relationship, and of doing something meaningful and important. The results illuminate the uncertainties that medical trainees have to grapple with dying and death. One important strand of mental negotiation encompasses their role in accompanying dying individuals and their relatives. Here, they are faced with many existential questions: When is the right time to accept death as inevitable? How to provide high-quality palliative care which is a core element of the medical care? How to manage symptoms, meet emotional and social needs, and address spiritual and practical concerns of dying patients and their relatives?
Our study also shows that the final year of medical school and the nursing clerkship are by far the most relevant periods offering opportunities for experiencing dying and death in the German medical education context. It is worth considering the extent and manner in which students can be supported during these stages, with the intention of converting their unpleasant encounters with dying patients and death into illuminating learning experiences. The witnessing of sudden death, the death of a youngster, and death after a period of suffering were shocking experiences for our participants, leading them to understand that not all situations can be controlled in the medical profession. A discussion of these, apparently very powerful, constellations regarding dying and death along with reflections on the formative factors that determine the qualitative character of the dying experiences would be an important step for the discussion of the inevitability of death and for the development of adequate coping strategies. Feelings of helplessness, failure, and guilt seem to be largely the result of the existence of an unrealistic physician image, which requires physicians to cure diseases, avoid mistakes, and control the clinical situations and one’s own emotions. There are some diversifications in this understanding of physician’s role particularly with regard to their perceiving of patients’ deaths as their failure (Pessagno et al., 2013; Smith-Han et al., 2016; Sullivan, Lakoma, & Block, 2003). However, the persistent presence of such professional self-concepts illustrates the need for special attention to this issue by medical trainers. In this context, particular attention should be paid to the subject of control and to the conflict between emotional concern and professional detachment. Further studies are required to investigate the effects of the proposed measures described earlier.
Footnotes
Author Note
This work was presented at the Gesellschaft für Medizinische Ausbildung annual conference in Münster, Germany, on September 22, 2017.
Acknowledgments
The authors would like to express their gratitude to the medical students and residents for their participation in this study and sharing their experiences. The authors would also like to thank Kristina Schick for her insights and expertise, which greatly assisted this research project. The authors especially thank Dr. Johanna Anneser and Prof. Gian Domenico Borasio for content support and Prof. Dr. Hella von Unger and Prof. Dr. Maria Wasner for the methodological support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.