
Abstract
This study aimed to examine family members’ attitudes and perceptions regarding their choice of care in the event of terminal illness, based on their experience in a caregiver’s role, while a loved one was terminally ill. All participants (N = 10) had cared for an immediate family member with terminal cancer. Snowball sampling was used. Qualitative data were collected through in-depth, semi-structured interviews. The data were transcribed verbatim and analyzed using thematic analysis. Five themes were identified from the data. These included two themes relating to participants’ experience of care, two themes in relation to participants’ attitudes toward the type of care they experienced and a final theme related to the role of religion and spirituality in dealing with loss. The findings of this study support the integration of multidisciplinary healthcare teams and the introduction of holistic care as early as possible within hospitals for individuals with terminal cancer, using the biopsychosocial–spiritual model.
The death of a loved one through terminal cancer is a hugely traumatic and life-changing experience for those affected. In 2018, there were 59.6 million deaths worldwide, with 9.6 million deaths caused specifically by cancer (Cancer Research UK, 2018). There were 17 million new cases of cancer diagnosed worldwide last year, and there is a projected number of 27.5 million new cases each year worldwide by 2040 (Cancer Research UK, 2018). Each year, approximately 40 million people worldwide live with illness requiring palliative care such as terminal cancer; however, only 14 million receive this type of care (Cancer Research UK, 2018). Palliative care focuses on symptom management and on maximizing the quality of life (QoL) of the patient and their family (Curtis, 2008); this can be distinguished from end-of-life care, which refers specifically to the care one receives during the last stage of life. The need for palliative care is expected to increase due to the rise in cancer, neurodegenerative disease, chronic disease, and the aging global population (World Health Organization, WHO, 2018). Providers of this care recognize the role of the family and address their needs in their role as a support for the patient (WHO, 2016).
In contrast to the focus of palliative care, the biomedical model of illness has traditionally been used by health professionals to treat patients with terminal illness. The focus of care approaches based on this model is to treat the biological aspects of a disease (Farre & Rapley, 2017). The model itself is rooted in a scientific discipline which emphasizes the purely biological basis of disease and treatment (Marks, 2002). According to this model, ill health occurs due to biological changes within the body, and disease should be treated by medical professionals using physical or chemical means in order to return the body to health (Ogden, 2012). It may be considered a reductionist approach to treating illness, whereby the medical profession treats the biological symptoms of disease, without consideration of the subjective psychological or social experiences of an individual, following a dualistic separation of mind and body (Borrell-Carrio, 2004). This model, according to Engel (1977), is not sufficient in taking account of the patient in terms of the social context in which they live. Instead, Engel proposed a biopsychosocial model, which treats the patient from the standpoint of the disease and from a social, psychological, and biological perspective. This model affirms the importance of the social and emotional needs of a patient, which require consideration during treatment and within the doctor–patient relationship (Henningsen, 2015).
This person-centered model can be seen to treat a person’s biological, psychological, and social needs (Farre & Rapley, 2017). For instance, Novy and Aigner (2014) found the use of the biopsychosocial model to be of significance in explaining the psycho-social issues involved in a key symptom of a terminal illness, namely cancer pain (particularly in the development of treatment interventions and in the management of cancer symptoms). This model, however, has been also criticized as being difficult to implement and to integrate into the care of patients within a primary healthcare setting (Kusnanto et al., 2018). Traditionally, the biomedical model of health and illness has tended to place emphasis on the treatment of biological disorders only (Grassi et al., 2017). While some health professionals working under this model recognize the importance of psychosocial needs, there is evidence to suggest that psychosocial care is limited in oncology settings. For instance, Peteet and Balboni (2013) found that, while clinicians identify that psychological care is correlated with less aggressive forms of treatment at end of life, oncology care does not provide adequate support.
Furthermore, Greer and Joseph (2016) found that in a palliative setting, the biopsychosocial model may not be sufficient in meeting the requirements of patients and that their spiritual needs may also need to be addressed. Their clinical study provided evidence to suggest that QoL is maximized through holistic palliative care, which includes a focus on a terminal patient’s spiritual needs to bring about “an easeful death” (Greer & Joseph, 2016, p. 8). The American Consensus Project for Palliative Care states that combining the spiritual aspect of care with the biopsychosocial model is critical, yet patients’ and caregivers’ spiritual needs are not being met in the healthcare system, due to lack of resources and training (Puchalski, 2008). As spirituality is an important factor of wellbeing in patients, it is appropriate that healthcare professionals tend to their spiritual needs in end-of-life care, where a patient desires (Bredle et al., 2011). Interdisciplinary team care involves a complex process of co-operation between medical staff of different disciplines working together to share knowledge and skills to impact on the patient’s care (Nancarrow et al., 2013). There is significant evidence to suggest that it is necessary in the healthcare system to address not only the medical conditions of patients but also the psychosocial and spiritual needs at end-of-life (Connor et al., 2002). In consideration of this, Sulmasy (2002) developed a biopsychosocial–spiritual model, based on the belief that a human being exists within a network of biological, psychological, social, and transcendent relationships. When illness occurs within a person, all aspects of their relationships are affected; as a result, he suggested that a holistic model can be used to care for a patient on every level of being.
The biopsychosocial–spiritual model of care emphasizes the critical role of spirituality in an individual’s health and wellbeing. There is evidence to suggest that spirituality and religion play a significant role in assisting patients’ wellbeing from time of diagnosis through to end-of-life care (Alcorn et al., 2010). While religion focuses on a collective phenomenon and is institutional, based on shared beliefs, traditions, and rituals and the associated formal rules and doctrines (Edwards et al., 2010), spirituality is more individual and subjective in nature (Hatala, 2013). It is associated with a connection to a higher power and relationships that give meaning and purpose in life (Siddall et al., 2015). Spiritual wellbeing has been shown to reduce distress in terminally ill patients (Vachon et al., 2009). A U.S. National Health Interview Survey found that religion and spirituality assisted patients to find meaning in their disease, to come to terms with their existential fears and to find support within a community of like-minded individuals (Jim et al., 2015). Préau et al.(2013) also found a positive correlation between health-related QoL and spirituality, which patients used as a coping mechanism during their illness. Religious and spiritual practices have been found to increase emotional wellbeing for patients (Maiko et al., 2019). Sulmasy (2006) affirms that spirituality is a critical aspect of palliative care and that the spiritual needs of patients in terms of meaning, value, and relationships need to be recognized and addressed by healthcare professionals at end of life.
In addition to spiritual concerns, research suggests that terminally ill patients are often concerned about having a peaceful experience of death. This is a death that occurs in conditions where the patient is comfortable, conscious, dignified, and as pain-free as possible, while allowing time to review their life and important relationships they have had (Battin, 1983). A qualitative meta-synthesis conducted by Meier et al. (2016) identified themes of importance to patients and their families at end of life. These include pain management, maintaining dignity, inclusion of patients’ preferences in care assessments and treatment, addressing of spiritual/religious needs, and improvement of QoL. These themes are consistent with the practice of palliative care (Meier et al., 2016). Challenges to a peaceful death may be perceived in terms of pain, loss of dignity, burden on others, loss of control, spiritual suffering, and hopelessness (Chochinov, 2006). Steinhauser et al. (2000) highlight the challenges associated with the care of terminally ill patients at end of life. The findings of this study show that physicians associate good end-of-life care with management of physical symptoms from a biomedical perspective; in contrast, patients identified a peaceful death as one where the addressing the spiritual needs were as important as effective pain management.
Family members and caregivers often acknowledge the death of a loved one as an immensely stressful experience and, while the majority of people who have been bereaved do not require professional counseling, research suggests that everyone would benefit from relevant information and support (Breen et al., 2017). Recent studies have provided evidence that there is a strong connection between spirituality, QoL, and coping strategies not only for patients but also for families and caregivers. Families of patients at end of life, who suffered from spiritual pain, have been reported to have increased anxiety, depression, and a lower QoL (Steinhauser et al., 2017). Bereavement raises challenges for loved ones regarding their own mortality, spiritual, and religious beliefs as well an examination of their beliefs in the afterlife (Tedeschi & Calhoun, 2006). The role of spirituality and religion can influence the meaning that a person makes of their life and the adjustment needed after a loved one’s death within the bereavement process (Wortmann & Park, 2009), and it serves as a coping mechanism during a time of bereavement. There is also evidence that the belief in an afterlife and a continued attachment to a deceased loved one may serve as coping mechanisms during the bereavement process (Benore & Park, 2004). For those who believe in life after death, the passing of a loved one may not be an ending, but rather a change in the relationship that continues to exist. There may be a spiritual growth through the process as a person finds meaning in their loss and in the subsequent adjustment of their lives (Benore & Park, 2004).
From the above literature, it is evident that individuals with a terminal illness and their families or caregivers often report negative experiences within the biomedical healthcare system, and that families or caregivers have a substantial burden of care associated with their role, which may impact their subsequent perceptions and experiences. We identified a dearth of literature which has explicitly investigated caregivers’ perceptions of the relative merits of the care their loved one received within hospitals or palliative care settings (such as hospices or the home). Following this, the primary aim of the study was to inductively explore family members’ attitudes, perceptions, and experiences regarding their choice of care in the event of receiving a terminal diagnosis themselves, based on their experience in a caregiver’s role while a loved one was terminally ill. A peripheral aim of the study was to examine the relative benefits of the biopsychosocial–spiritual model of care compared with the biomedical model of care from a caregiver’s perspective, and the role that religion or spirituality may have on caregivers during this time. We anticipate that the results of this study may help to inform healthcare practitioners about important considerations in the delivery of care, which appropriately meets the needs of individuals with a terminal illness and their families or caregivers.
Methodology
Participants and Recruitment
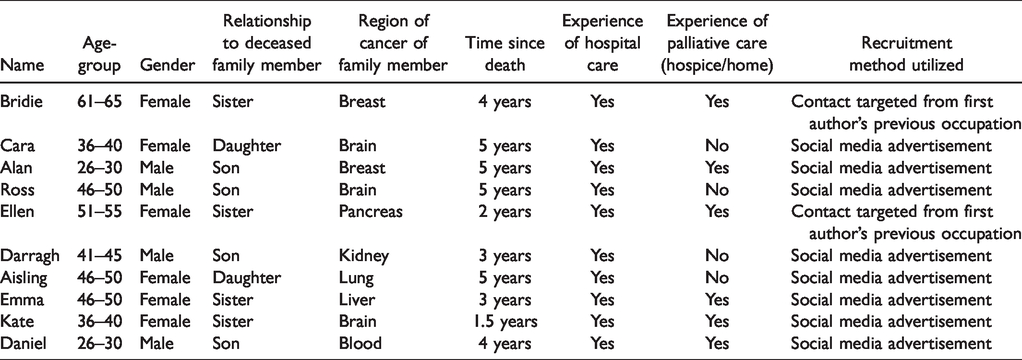
A sample of 10 participants were recruited (N = 10), and each of whom had cared for a loved one with terminal cancer. Further participant demographics and clinical characteristics are provided in Table 1. Due to the specific profile of the respondents required for this research, snowball sampling (Matthews & Ross, 2010) was used. The criteria for inclusion was for the participant to be an English-speaking adult, over 18 years of age, who had experienced the loss of an immediate family member through terminal illness within the last 5 years and who had capacity to give informed consent.
Participant Demographic Information and Type(s) of Care Experienced by Caregivers and Their Loved Ones (N = 10).
A snowball sampling approach to recruitment was utilized in the current study. 1 In line with this approach, a targeted recruitment advertisement for the research was posted on social media by the first author, requesting voluntary participation. The first author supplemented this recruitment method by explicitly targeting contacts from their previous occupation as a holistic therapist for recruitment and encouraged the resharing of the post on social media. The process of recruitment proceeded as participants contacted the first author through SMS text message or email, where the first author replied to arrange a suitable date, time, and location for the interview to take place. In this reply, the first author also ensured that the participant in question satisfied the inclusion criteria. In an effort to ensure as little bias as possible in the sampling approach, no participant of this study had any prior relationship with the interviewer (the first author).
Data Collection
This research study received ethical approval from an institutional review board in the authors’ host institution. The research study had a cross-sectional qualitative research design, in order to obtain data on caregivers’ experiences and perceptions. Due to the potentially sensitive nature of the topic, in-depth interviewing was used (Willig, 2013). Semi-structured interviews were conducted with immediate family members, who supported their loved ones through terminal illness and to investigate their opinions of the care they would choose, in the event of their own illness. Prior to the interview, participants read the plain language statement and signed the consent form to confirm that they were happy to proceed with their participation in the study. A semi-structured interview guide was devised by drawing upon the specific aims of the research and drawing upon previous findings in the research literature. This included specific questions that drew upon core concepts from the biopsychosocial–spiritual and biomedical models of healthcare in order to ensure an appropriate depth and coverage of the core needs of participants and their loved ones. Participants were asked questions regarding their experiences of the death of an immediate family member through terminal illness, their opinions on the care received, their own beliefs and attitudes toward death, illness, and spirituality having lived through this experience, and the type of care they may wish to receive should they find themselves in a similar situation. Participants were also given scope to discuss their own areas of interest within the interviews. At the end of the interview, some demographic details were sought from the participants regarding their age, gender, type of terminal illness experienced by the death of their immediate family member, their relationship with their loved one, and the length of time since the individual had died.
During the first author’s initial contact with participants, the location of the interview was agreed. The preferred location in 9 of the 10 cases was the participant’s own home. One interview was conducted in a secure room at the participant’s place of work.
The duration of the interviews was from 13 minutes to 59 minutes (mean length of 30 minutes). With the agreement of participants, the interviews were recorded through the Voice Memos© application on an iPhone. The data were transcribed verbatim in preparation for thematic analysis.
Data Analysis
Following transcription, all interview data were transferred to NVivo 12© for subsequent analysis. Braun and Clarke’s (2006) six-step model of inductive thematic analysis 2 was used to frame the analysis. The six steps outlined include (a) familiarization of the data, (b) generation of initial codes by the researcher, (c) purposefully identify themes from open-coded extract, (d) checking thematic material against the data transcripts, (e) clear defining and naming of themes, and (6) write up of the results. During the first stage of data familiarization, the first author removed and replaced all identifiable information of participants regarding names, hospitals, and locations from the data. Following this, the first author used open-coding to code the transcripts. The first author then began to identify themes based on an analysis of the codes alone. Once this stage was complete, the first author related these themes back to the coded extracts to ensure they were coherent, clearly defined and named the themes and wrote up the analysis. This process was checked by the second author following each stage of data analysis. From this process, five core themes relevant to the study aims were identified from this data.
Results
Five themes relating to the participants’ experiences and attitudes toward the care received by their loved ones during terminal illness were identified from the data by the authors. These included two topics regarding participants’ experience of care, two prevalent themes in relation to participants’ attitudes toward the type of care they experienced, and a final theme relating to the role of religion and spirituality in dealing with loss. In the analysis which follows, ellipses have been inserted in square brackets where quotations have been contracted to remove irrelevant information. In cases where the context of a quote was lacking, contextual features or a potential meaning has been identified in square brackets. Names of participants and their family members have been replaced with pseudonyms throughout.
Participants’ Experience of Care
Care for the Whole Person: Knowledge and Experience of Palliative Care From a Caregiver’s Perspective
Six out of the 10 participants had experienced palliative care being given to their loved one during their illness, while 4 people had no experience of this care being given to their family member. Participants whose loved ones had received hospital care only, perceived that palliative care was associated with end-of-life care, where additional support, comfort, and counseling for the patient and family is offered.
One participant’s perception of it was that it was delivered at a different stage of care to hospital care. I suppose my perception particularly at the time would be that [palliative care is] linked to hospice care. […]In my mind, they are two separate things. The hospital care is very much “let’s just treat this cancer” nearly, “we don’t have time for how you feel about it.” […]They’re two different stages of illness. [Cara, aged 36–40]. When I hear palliative care, to me, that’s like end of life. There’s no coming back from palliative care, that it’s basically to make the rest of your life, that’s probably going to be a short time, as comfortable for you as possible. [Aisling, aged 46–50] They would have afternoons where the patients and their families would just be in the lobby and take part in the activity of the day, which could have been painting, knitting or anything. But regardless of what the topic was, you could see behind it was just everybody in the hospice was trying to normalize and make sure everyone is equal. [Alan, aged 26–30] [Patient] did get counseling and I think she found it to be very beneficial. I think at the end, she had a peace about her and I don’t think she feared death […]I think that that had to be from the help and support that she got when she was in the hospice. The hospice [staff] seem to care for the whole person and not just the illness; like as well as the mental needs being met, their emotional needs and spiritual needs and that of the family were also met. [Bridie, aged 61–65] There was a multidisciplinary team that met with us all to try and navigate the tensions that were arising. As many of us as possible were invited, siblings and his wife etc. along with the palliative care team in the hospice […] I do think that was good. There was a difference in the care and communication here. [Kate, aged 36–40]
The dignity of terminally ill patients was maintained with care and compassion by palliative care professionals. From my experience, it was through palliative care that we, as a family, could give dad the death he deserved of dying with dignity. I think the hospice workers show more compassion towards the patients and recognize the patient has feelings and emotions as well as their physical symptoms. [Daniel, aged 26–30] Her husband never felt he was on his own. If she became ill […] he always knew […] that he’d just have to lift the phone and help would come straight away and that was a tremendous help to her and to him as well. […] They didn’t just treat her, they treated the whole family and they were a great help to her children and husband as well. [Bridie, aged 61–65] They [counselors] did a great job in preparing us for it [death] and you can never be prepared for it … Even talking to other people whose loved ones had gone through an illness, that was actually nice to talk to someone who “got you” [sic]. [Alan, aged 26–30] There was a sense of peace and acceptance […] They were very good, now maybe it just wasn’t busy at the time but he had his own room and they never once said the children couldn’t come in. It was a very open and welcoming environment […] It was a beautiful death, if that could be said, the best possible death he could have had. [Kate, aged 36–40] I’d like palliative care and to be taken and treated at home, in the comfort of your own home with your family around you. Or in a hospice, as I said, rather than being in and out of A&E in a hospital, where things are taken out of your hands. [Darragh, aged 41–45]
“Everybody Was Kind of Left in Limbo”: Communication Difficulties With Health Professionals and the Absence of Psychological Support Experienced by Participants and Their Loved Ones During Their Hospital Experience
Participants reported disappointment with the way in which health professionals gave a diagnosis to patients. I mean the way the diagnosis was delivered to him was just very factual, very clinical, “this is what you have.” […] Information was handed over to him in booklet form and it was kind of very difficult to get answers from doctors, just “this is your diagnosis, this is your treatment plan, this is what’s happening.” [Cara, aged 36–40] You have to go looking for information from surgeons, nurses or doctors. In many ways, from our experience, that information is dragged out of professional people rather than handed to the families […] everybody was kind of left in limbo [sic]. [Darragh, aged 41–45] There was no suggestion of where to go next or follow-up […]there was none of that at all. In terms of the practical follow up and his treatment plan, he was just given an appointment at a later stage. [Kate, aged 36–40]
Some participants reported a lack of resources in the hospital experience and hence felt that their loved one was not treated as a person but as a “number,” as their psychological needs were not met. “I fully understand there is a lack of resources and doctors, but to be honest, the experience that I can remember was that we were treated like numbers and not people” [Alan, aged 26–30].
Despite the perceived lack of support and information for patients and their families, most participants trusted the doctors completely in terms of their medical knowledge and were willing to follow their treatment advice. It was very much “this is the diagnosis, this is the treatment plan” and we were all on board […] I suppose we were really at the mercy of the doctors and we put our trust in them completely. [Cara, aged 36–40] The decisions were probably made first and foremost by my mum. She was probably getting most of the information and she would have to make decisions on the spot, of again what treatments they might be trying. […]Maybe some of the trials that we gave a go … maybe we shouldn’t have, as they had an adverse effect. [Darragh, aged 41–45]
Participants’ Attitudes Towards the Type of Care Their Loved Ones Experienced
“Who cares for the carer?”: Impact of an illness on the family members in the role of a caregiver
The diagnosis of a terminal illness for an individual also has implications for family members. In many cases, participants found themselves as carers, without any prior knowledge or experience to be equipped for that role. I think that all of us went into “survival” mode […] When everyone is looking out for everyone else it’s like “who cares for the carer?” but unfortunately in those situations you’re not looking out for yourself because all of your loved ones need your support and you need to be strong. [Daniel, aged 26–30]. There was no emotional support for [patient] in particular, but also for his wife and us. I suppose it almost felt like it was my role to be that person in that situation […]I felt very much that it was my purpose and that’s why I was there. [Kate, aged 36–40] There should have been advice and there should have been help with everything he was going through at the time … I think if there had have been some structure there and some additional care, the whole experience might have been a bit easier for the family. [Ross, aged 46–50] Mam could have definitely used a neutral ear to vent to, it could have been beneficial […] So an ear to vent to, external from the situation to provide a support for her, it would have been very beneficial. [Daniel, aged 26–30].
“As early as possible”: The introduction of holistic care
Those who had direct experience of it believed that the early introduction of palliative care would be very beneficial for the patient and their families. One participant identified that palliative care is widely seen as hospice care, thus giving the perception that it’s offered only at end of life. Her experience of it, however, differed completely from this common perception. Before, people had a very wrong impression of the hospice […] But nowadays, I think the hospice has a far more positive sort of view […] It helps not only the patient, but the whole family […] I think it will be beneficial to introduce it as early as possible. [Bridie, aged 61–65]. I think the word palliative care in itself is associated with end-of-life, well that would have been my understanding of it. So really, a holistic approach to care would be a better way to describe it as it would have helped hugely for him. [Kate, aged 36–40]
Participants acknowledged that both hospital and palliative types of care are important and should coexist in the same setting. I know the general hospital has to be involved, and you have to do surgery and you have to do whatever the treatments that are recommended […] but definitely having compared one with the other I would like the whole hospice situation to be involved if I was ever faced with that. [Bridie, aged 61–65]
The Role of Religion and Spirituality in Dealing With Loss
“[It] gave me great comfort”: Role of religion and spirituality for participants while dealing with loss
Religion and spirituality were identified by all participants as being of importance in coming to terms with their grief, after the death of their loved one. Religion brought comfort to those participants who had faith, for example, in the knowledge that they would see their loved ones again. My religion did really help me and gave me great comfort, and I think the fact that you know that the person is not gone. […] It is very comforting to know that your loved ones are in a better place, that they’re not suffering there anymore. [Bridie, aged 61–65]
Many participants also believed that their loved one’s spirit lived on to help cope with loss. I do feel dad is still around me and, when something isn’t going my way, I can call on him and ask him to give me strength […] I do feel it did play an important role and it did help me cope with dad’s death and I do believe he’s still with me today. [Daniel, aged 26–30]
Some participants became more spiritually aware having lived through this experience. When something like that happens, you sort of ask more questions in terms of “well, what’s life all about, what’s going on, what is life after death, what is spirituality?” So, you ask a lot of questions that maybe you hadn’t asked. [Ross, aged 46–50]
Discussion
To our knowledge, this is the first study to explicitly family members’ attitudes and perceptions regarding the choice of care in the event of a terminal illness, based on their experience in a caregiver’s role, while a loved one was terminally ill and the role religion or spirituality has on caregivers during this time. Five themes were identified by the first author following inductive thematic analysis. These included two themes regarding participants’ experience of care, two themes regarding participants’ attitudes towards the type of care their loved ones experienced, and one theme on the role of religion and spirituality in dealing with loss. These findings, and a consideration of the relative benefits of the biopsychosocial–spiritual model of care compared with the biomedical model of care from a caregiver’s perspective in light of these findings, are discussed in detail later.
Many participants in this study highlighted their concern at their inability to make a conscious, informed decision regarding the care of their loved one due to limited resources. Participants observed that, when it came to decision-making in terms of care (e.g., changes to or withdrawal of treatment), due to time constraints and insufficient knowledge, they often complied with doctors’ opinions. Their decision-making was further compounded in situations where there were limited resources. This finding is reflective of the concerns expressed by Desanto-Madeya et al. (2018), whose study highlighted the significant burdens that arise on family members while making decisions on a patient’s behalf, as this often leads to practitioner–compliant decisions. Caregivers in the current study also expressed their concern for the lack of information and support they were provided with during the time of their loved one’s treatment. This meant that they often felt it necessary to research information regarding their loved ones’ disease and treatment plans themselves, mainly through the mediums of leaflets or publications on the internet. Puchalski (2008) suggested that inadequate support from practitioners in hospital settings was due to the lack of resources and training offered to medical staff; the current study extends these findings to suggest there may also be a lack of resources and training offered to caregivers in relation to their caregiving role, which may have a profound effect on their decision-making.
In contrast to the hospital experience, participants who had availed of palliative services in the care of their loved one reported a very positive experience. They experienced it as a more person-centered or holistic approach to healthcare that aimed to meet all the needs of the individual, both treating the physical symptoms of the patient while also respecting their QoL. This type of care, as described by participants, is in line with descriptions of the biopsychosocial–spiritual model of healthcare (Farre & Rapley, 2017). Participants reported that, in addition to the psychological, social, and spiritual needs of their loved ones being addressed, this model of care supported the family’s needs in caring for their loved one. This care for both the patient and family members has been reported in the literature as an important aspect of palliative care in terms of maximizing the QoL of both patients and caregivers (Curtis, 2008). In addition, participants believed that this type of care played a significant role in the sense of dignity and peace that they believed their loved ones experienced at end of life. These concepts are associated with a peaceful death as described in previous studies (Battin, 1983; Chochinov, 2006).
Participants also described how they had initially associated palliative care with end-of-life care and death of any patient who had experienced it. This initial negative perception was associated with a passive type of care (comfort care with no curative intent) when a patient has been given a terminal diagnosis. In reality, however, participants found that this was not the case and palliative care was not only for patients who were dying. These findings are reflective of literature, which has shown that, despite the stigma associated with palliative care, it actually is evaluated positively for those who have experienced it (Zimmermann et al., 2016). To combat such stigmatized perceptions of palliative care, there is growing evidence to support the early integration of palliative care for patients diagnosed with cancer (Dahlin et al., 2010). Despite the substantial benefits associated with early palliative care (e.g., QoL and symptom management) and its integration into oncology services, it is under-utilized in medical settings at present (Zimmermann et al., 2014). In this study, participants who had experienced palliative care believed that it should be introduced soon after diagnosis due to the benefits that it provides, namely it addresses the psychological, social and spiritual needs of patients and family members. This holistic approach to healthcare has been highlighted as an important issue for patients who have not experienced palliative care. A more recent study conducted by Selman et al.(2018) also found that to truly meet the needs and preferences of both patients and caregivers at end of life, spiritual needs should be addressed within a palliative care setting. Other research has found that patients would also welcome the opportunity to talk to their clinician about their spiritual needs, and these issues should be raised routinely to provide a true patient centered approach to care (Best et al., 2019). Based on the compelling evidence for integration of services, the American Society for Clinical Oncology in 2017 recommended that all patients with advanced cancer be provided with palliative care within 8 weeks of diagnosis. This was to run concurrently with existing active treatments. The American Academy of Hospice and Palliative Medicine has called for no delay in the provision of palliative care for any patient who is experiencing distress while receiving treatment (Finn et al., 2017).
Spirituality and religion were acknowledged by participants as playing an important role in both coming to terms with their grief post-death and during the time of their loved one’s illness. Participants were asked about their religious and spiritual beliefs during the course of the interviews. Many participants used religion and spirituality as a coping mechanism throughout the illness of their loved one, and it provided them with a sense of comfort in coming to terms with what had happened despite them not actively practicing their religion. These experiences of participants mirror previous findings that palliative care uses a spiritual approach in helping both the patient themselves and also the family of the patient experience peace and acceptance regarding their situation which then prepares them for end of life (Meier et al., 2016). Wortmann and Park (2009) found that religion and spirituality can not only serve a purpose as a coping mechanism during this traumatic time but also can influence the adjusted meaning a person gives to their life. Religious belief may also diminish the impact negative news regarding cancer progression or test results may have on a patient (George et al., 2019). According to Saad et al. (2017), it is only when the spiritual dimension is integrated into healthcare systems that a true paradigm shift will occur.
The holistic approach to healthcare found in the hospice setting described by participants in the current study was associated with significant improvements in the patient’s QoL, enhanced mood, prolonged survival, and less aggressive treatments at end of life (Temel et al., 2010). There is a substantial amount of documentary evidence supporting the early integration of palliative care with oncology services due to its positive impact on patients, and it is being increasingly recommended as the necessary standard of care by cancer organizations worldwide (Hannon et al., 2016). There is also evidence to suggest that the integration of oncology and palliative services would provide a much more comprehensive care system and maximize the QoL and care for those living with the disease and at end of life stage (e.g., Greer et al., 2013). From the above observations regarding the trust caregivers and patients put in medical professionals, physicians may have an important role in changing perceptions toward this type of care and how it is framed in the minds of patients and family members (Zimmermann et al., 2016). In addition, it has been suggested among caregivers in this study that a change from the term palliative care to supportive care may assist in the change of its perception. The findings of this study support the need for widespread education about palliative care and what it involves.
In this study, participants described the approach to healthcare in the hospital setting in line with definitions of the biomedical model; largely focusing on treating the physical symptoms of the individual. Participants also suggested that, in many cases, medical professionals failed to acknowledge the psychological, social, and spiritual needs of the individual. In such cases, participants reported that their terminally ill family members experienced a lack of dignity, had unaddressed mental health difficulties and received inadequate support from healthcare staff at end-of-life; these experiences are similar to what Chochinov (2006) describes as a “bad death.” This experience of hospital care is reflective of the critiques of the biomedical model of care, as described in the literature by Farre and Rapley, (2017) and Grassi et al., (2017). The results of this study support the findings of Peteet and Balboni (2013), who found that hospital-based oncology care alone did not provide adequate support for patients in the USA, due to the lack of perspective on medical professional’s behalf of respecting the patients’ QoL. From the participants’ perspective in this study, the biomedical approach to healthcare provided in hospitals failed to provide for the psychological, social, and spiritual needs of both patients and caregivers. This supports Fitch’s (2016) findings that from the patients’ perspective, spiritual care was considered to be an important aspect of their care needs. As suggested by participants, it is possible that the busy hospital environment led to oncology staff’s difficulties in identifying spiritual distress in advanced cancer patients and in offering interventions. This reflects findings in the wider literature. For instance, O’Brien et al. (2019) found that nursing and healthcare professionals were less likely to offer spiritual support to patients due to inadequate training in spiritual care.
There are several strengths and limitations to the current study. To our knowledge, this is the first study to investigate the differences between the care received in hospitals and palliative care (in a hospice or home setting) from the perspective of caregivers of individuals with a terminal illness and how the experience of these can influence the caregiver’s perception and attitudes toward the type of care they may wish to receive, should they find themselves in a similar situation. There has also been very little research from a caregiver’s perspective, and this study highlights the need for further research in this area, particularly regarding the need for appropriate supports for this often hidden group. A limitation of this study is that all individuals were terminal cancer patients; it is possible that different findings may be obtained with a different sample of caregivers for terminally ill patients as the finding of this study are limited to describing the cancer population. The cross-sectional nature of this study is another limitation; future research of a longitudinal nature could examine the relative benefits of the biopsychosocial–spiritual model compared with the biomedical model of care from a caregiver’s perspective across all stages of the cancer trajectory. Finally, the convenience sampling recruitment methods and small sample size mean that our findings are limited to a small group of local informal caregivers. Nonetheless, the rich experiential data that were obtained demonstrates the salience of the issues for participants in their daily lives.
To conclude, in the current study, it is evident that caregivers require support, advice, and information, should they be expected to make decisions regarding the care of others or possibly themselves in the event of a terminal illness. The findings of the current study suggest that it may be of benefit to better integrate the delivery of palliative care into oncology services from an earlier stage, perhaps in association with the hospice setting, which promotes a holistic approach to care and recognizes the important role of spirituality in end-of-life care. These findings also suggest that there is a need for communication interventions, particularly in the hospital setting. A study conducted by Laidsaar-Powell et al. (2013) highlighted strategies that may be used by clinicians in communication with cancer patients and caregivers in order to support shared decision-making. It is important to recognize that caregivers play an important role in supporting their loved ones through this traumatic experience and require education and assistance in this endeavor. The findings from this study highlight the need for further research in the area of palliative care and the role of medical professionals and researchers in encouraging patients and families to avail of this service, for example, through education and information campaigns.
Footnotes
Acknowledgments
This is a self-funded study. The authors wish to thank the individuals who participated in this research. The authors also acknowledge the bravery and honesty with which they spoke to them regarding such a sensitive subject.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.