
Abstract
In many countries, an increasing proportion of deaths occur in residential aged care (RAC) (nursing homes) meaning that these have become both a place to live - a home- and a place to die. This paper reports on death practices and rituals in 49 RAC facilities in Aotearoa/New Zealand narrated in semi-structured interviews with staff. Themes coalesced around ‘good death’. Dying alone was not seen as a good death and the demands of trying to prevent this caused tension for staff. Meeting family wishes, post death decision-making, after death practices and rituals, including communicating and remembrance of the death, were explored as part of good death. Overall, death rituals in RAC were limited. Balancing the needs of the living, the dying and the dead created tension. The rituals and practices facilities are currently enacting in death/post-death require attention, since more people will die in RAC with increasingly diverse needs.
Background
New Zealand (Aotearoa), the setting of this study, is constitutionally and politically, a bi-cultural country, despite increasingly being a multicultural nation. The likelihood of dying in residential aged care (RAC) (nursing home) increases with age. Fifty nine percent of women and 48% of men aged at 85 and over die in RAC in NZ (McLeod, 2016). Indigenous Māori constituted approximately 15% of the New Zealand (NZ) population in 2017 (StatsNZ, 2020), and represented 2% of deaths in RAC (Palliative Care Council of New Zealand, 2011). The total number of Māori deaths is projected to increase from 3,300 in 2016 to 4,900 in 2038 (McLeod, 2013) and an increased use of RAC is predicted for Māori as a result. As well, the proportion of deaths in RAC is projected to increase dramatically in coming decades, in line with trends reported in many other developed countries (Bone et al., 2018; Broad et al., 2013). This has led to RAC facilities being characterised by some authors as ‘de-facto’ hospices (Connolly et al., 2014b). In addition, research that finds practices surrounding dying in aged care remain a hidden discourse (O’Connor & Pearson, 2004) adds to the need for end of life and post-death practices employed in these facilities to receive specific research attention.
Thanatology and the ‘Good Death’
Thanatology, or the specific scientific study of death and its rites and meanings, emerged in the literature in the 1950s, reflecting a shift away from a theocentric view of life and death where God is central to interpretation, towards a human-centric view of life (Fonseca & Testoni,2011–2012), as well as a marginalisation of mortality and death (Gorer, 1955). Categorisations and typologies of deaths have continued to evolve, especially around what might be a considered a ‘good death’, (Bradbury, 1996; Clark, 2002; Hart et al., 1998; Krikorian et al., 2020; McCray Beier, 1989; Timmermans, 2005, 2010). Irrespective of its context, a ‘good death’ is informed by an ideology that “constructs a socially approved form of dying and death with powerfully prescribed and normalized behaviours and choices” (Hart et al., 1998, p. 72). At present, these behaviours reflect the bio-medicalization (Timmermans, 2010) of death and are embedded in current palliative care practice which has dominated the philosophical and social context of a ‘good death’ in the West. Currently ‘good deaths’ are seen to be those which are foreseen, planned for and occur in line with personal preferences after clear decision making. They are peaceful, free from pain, anxiety, and distress and do not occur alone (Clark, 2002; Gott et al., 2019; Krikorian et al., 2020; Rich, 2014; Seale, 1995). These ideas are so embedded in current thinking and practice that it is easy to overlook the fact that they are reflective of certain assumptions and realities about a person and the social world in which they exist.
Residential Aged Care and Death Rituals
RAC facilities have developed their own norms for dealing with death and loss. Doka (2002) frames these sets of norms as grieving rules which are driven by the social context. The sociologist Emile Durkheim (1915) developed the study of collective ritual in relation to their integrative effects and the ways in which they bind communities together. For him, and later sociologists such as Parsons (1971) and Bellah (1975), rituals are an expression and affirmation of collective ideals. Myerhoff (1984) states “ritual is a form by means of which culture presents itself to itself” (p. 320) and is “inherently connective” carrying a “message of order, continuity and predictability” (p. 306) through its repetitive nature. Rituals can structure grief (Doka, 2002) and “provide opportunities to mark transitions or ongoing connections, to affirm the person, or to find reconciliation” (p. 4). Studying rituals in RAC facilities can reveal the culturally constructed notions of old age and, death and dying (Hood, 2011).
Research has found a scarcity of post-death rituals and social practices in RAC settings (Ewen et al., 2016), leaving some involved with a perception that post-death care practices lack dignity and respect (Barooah et al., 2015). Enduring patterns of work or daily routine in RAC facilities have been found to be minimally impacted by death (Moss et al., 2002; Moss et al., 2003). These researchers also found an associated lack of rituals around death and dying. As Glaser and Strauss (1964) concluded, the values of society are imported into hospitals and by implication, RAC facilities.
In contrast, other research has found death and dying rituals in RAC to be highly valued by staff, residents and families, including formalised bereavement practices such as formal room blessing rituals after a death (Maitland et al., 2012). Not only does the ritual provide a vehicle to acknowledge and celebrate the life lived through sharing stories and connecting to family and the care community, but it can also serve “to make the space fresh and new and to bless it for the next person” (Maitland et al., 2012, p. 244). More broadly, Bern-Klug (2011) argues that without healing rituals signposting a resident’s death, others in that community “may feel their own death will go unnoticed, their life unremarked” (p. 62). Whether or not these findings provide evidence of a RAC culture that prefers to deny the existence of death is contested (Zimmermann & Rodin, 2004).
Staff have also reported deficits in the provision of emotional support to other residents and staff after deaths occurred in the facility (Moss et al, 2002). For example, the practice of filling beds quickly after a death was a negative experience for health care assistants. This was especially true if the caregivers had not been informed of the death, and only learned of it by walking into the room and finding the bed empty (Barooah et al., 2015). Fryer et al. (2016) also found that health care assistants struggled with the quick turn-over of beds after a death, especially in terms of managing their own grief experience. Staff grief has been found to be more intense if staff had had a close relationship with the patient over a longer period of time and if they had been unable to prepare emotionally for the death (Boerner et al., 2015). Interestingly, Boerner et al. (2015) also found that RAC staff grief reactions mirrored those of bereaved family caregivers.
Tension in the Liminal Space of Living and Dying
The resident experience of living in a facility with continuous exposure to the reality of death and dying and the liminality or “border of death” in that space is not well-documented (Djivre et al., 2012; Quartier, 2010). RAC residents have described the sense of family-like bonds they have with each other and the ensuing sense of loss when a member of their group (albeit, dining room mates or card-playing mates) dies (Djivre et al., 2012). Residents also employ behaviours to avoid the emotional weight of being close to on-going death and dying in the facility. Residents also grappled with a feeling of betrayal and frustration at the routinized and depersonalised care they experienced, both of the living and the dead, citing the practice of exiting bodies out of the back door (Djivre et al., 2012). That avoidance of emotional weight resulting from death can be viewed through a lens of disenfranchisement of grief, which Doka (1989) describes as, the grief people experience “when they incur a loss that is not or cannot be opening acknowledged, publicly mourned, or socially supported” (p. 4). Grief disenfranchisement may occur because the relationship is not recognized, the loss is not acknowledged, or the griever is excluded (Doka, 2002).
Moss and Moss (2002) considered there was disenfranchisement of grief around the death of older people in residential care for staff because of the lack of social legitimacy, which may be due to the death being judged as routine, timely and fair. There is also ample documentation of staff and resident bereavement support needs not being adequately addressed (Barooah et al., 2015; Chróinín et al., 2011; Ewen et al., 2016; Gleason et al., 2016; Kwak et al., 2013; Maitland et al., 2012). Subtle ageism may also be associated with the lack of public mourning rituals to mark the death of older people with advanced frailty because of the current cultural value of older people whose death is expected and part of the routine (Carney & Gray, 2015; Kane & Kane, 2005; Moss & Moss, 2002; Moss et al., 2003).
With these observations from the literature, we were curious to further explore the liminality of death in residential aged care in New Zealand, given the RAC facilities are residents’ homes, places to live, as well as places most die (Parker, 2011). Within this context, the purpose of this study is to explore and document the practices and rituals found in RAC facilities at the end of residents’ lives and post-death.
Methodology
This qualitative study was the second phase of a larger mixed-methods study (Boyd et al., 2019; Foster et al., 2019) (retrospective cross-sectional design) which investigated deaths in a stratified representative sample of 61 RAC facilities across New Zealand. The participating facilities represented typical RAC facilities in New Zealand with diversity in size (under and over 70 bed), ownership models (profit/non-profit) and scope of practice. See Boyd et al. (2019) for further details of methodology for the first phase.
Semi-Structured Interviews
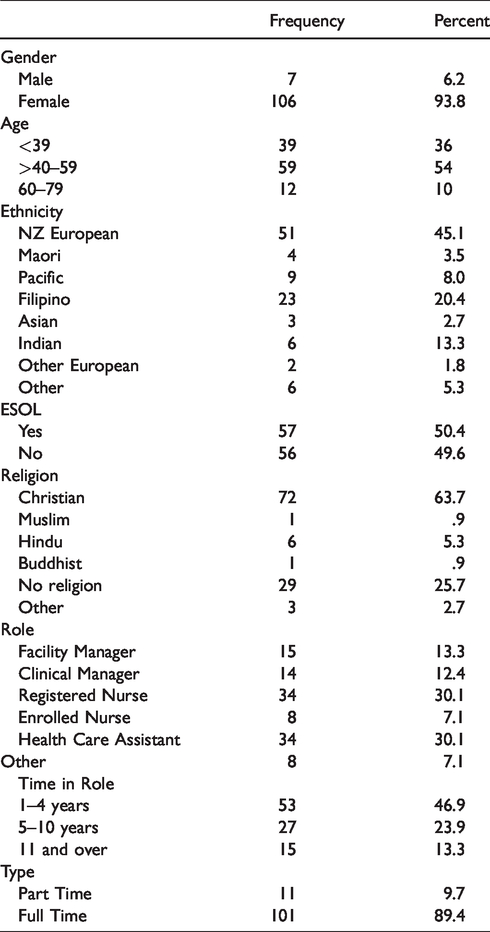
Data collection through semi-structured interviews took place between January 2016 and February 2017 across 49 of the 61 facilities in the larger study. A convenience sample of eligible participants included any registered nurses (RN), clinical or facility managers, enrolled nurses (EN)(smaller scope of practice than an RN), health care assistants (HCA) and others (e.g. clinical co-ordinators, facility owners) who were directly involved in the care of a dying resident during the 14 days prior to the death (see Table 1) and were part of the 61 facilities in the larger study. Facility management and/or clinical management helped identify eligible participants. Audio-recorded semi-structured interviews were conducted in the facilities, as soon after the time of death as possible. Written consent was obtained from interviewee participants and facility management in accordance with ethics approval granted by the University Human Participants Ethics Committee (#015461 & #015650). The interview guide focused on: exploring the experience of the death; identifying facility death and dying practices and subsequent communication with resident families; management of grief for family members, staff and other residents; any self-identified training and support needs relating to end of life care; and staff views on palliative care provision more generally within the facility. Staff recalled either from memory and/or by review of clinical notes the health status of the decedent and the story of the final days of the resident’s life. Interviews were transcribed by a transcriptionist who had signed a confidentiality agreement.
Interviewee Characteristics.
Analysis
The qualitative data used a general inductive approach (Thomas, 2006) with a social constructionist perspective (Gergen, 1985). Quartier’s (2010) classification of rituals in death and dying assisted in distinguishing between individual and collective rituals. Transcribed interview transcripts were manged using NVivo 12 (NVivo Qualitative Data Analysis Software, Version 12, 2018). The authors collaborated in initial line-by-line open coding of the transcripts, research notes and artefacts into nodes. Comparative analysis was undertaken through axial coding (relating concepts together) (Corbin and Strauss, 2008), asking questions of the data with the nodes then coalescing into themes (Braun & Clarke, 2006). Regular meetings with the larger research group reviewed data collection, coding and domain analysis.
Findings
Of the 113 participants interviewed, the majority were female (n = 106). Over half were over the age of 40 (n = 71). The majority (n = 101) were in full-time employment and English was not the first language of half of respondents revealing a mix of ethnicities (see Table 1).
Themes
Participants described an array of dying and post death rituals and practices in participating RAC facilities. Contrasting attitudes toward the public compared to the private nature of death in facilities created differing practices, especially with post-death grief practices, dead body removal, repopulating of the space after the death, communication about the death, and spiritual/religious rituals. Tension/s was a common thread throughout the themes identified in the analysis. Major themes include: 1) A good death: never die alone, 2) A good death: meeting family wishes 3) A good death: “who decides?”, and 4) A good death: after death practices and rituals.
A Good Death: Never Die Alone
A striking finding in the data was the expectation RAC’s placed upon themselves that actively dying residents should not be alone at the time of death. Interviewees revealed the tension this expectation generated between accompaniment and capacity.
But no there’s no way we’d let them die alone, no.(HCA)
I mean, it’s the end of their lives, … but we don’t have that capacity of giving them one on one care … Which is quite sad, you know? That would be good if there was someone that can stay with them bedside, and, you know, just be there, you know, with them. Who would like to die alone? (RN Manager)
So we had to have someone sit with him, cos when he did wake up he just wanted someone there. We rang the family and said it’s time, but we didn’t really have the staff to do it.(RN)
And that they feel like they’re not alone, you know, that’s really, like, I can’t bear the thought of them lying there dying alone. You know, with no one. And if family can’t be there it’s nice that you, you feel like you can be there. (HCA)
I always try and encourage the staff if they know that somebody’s low that they try and be there as much as they can. Coz I don’t like to think of somebody dying on their own. It’s just me but, yeah. (RN Manger)
I think this particular death was, it was, it was nice –It was nice for everybody as, as much as death can be. He, you know he did eventually drift off nicely, it was, the family all got to spend some time with him, he was comfortable, the pain was well managed … . I mean actually when, when something goes well and end of life is done well you, you actually go well that, that was nice, it was, that’s the way it should be. Because people got what they, they wanted out of it, you don’t get that empty kind of oh I didn’t manage to get the family here in time, or (RN)
A Good Death: Meeting Family Wishes
Staff responded to any end of life caring practices that the family may have wanted, “Well, it depends on the family … we just let them deal with it the way that they want to” (HCA). Knowing and staying in their place as professional staff was also evident, “We, the staff, work here; this is not our home, it’s their home. We are the intruders here; we are the ones delivering a service for people. Respect them for who they are” (RN). How someone died also had ramifications for a facility’s reputation and their relationship with the deceased’s relatives. If families were unable to be with their relative at the time of death, they often asked staff if it had components of a ‘good death’, especially if the death had been alone.
So a few of the families ask, want to know what they were like when they passed away, who was with them, or who found them … . They want to know, were they alone, whether they were in pain. (RN)
A Good Death: Who Decides?
For those working in a RAC facility there was an inevitable tension between an individual staff’s view of a ‘good death’ especially regarding post-death practices, and that of the dying resident, their family, or facility management. For example, interviewees often reported deep connections with residents and their consequent grief after residents died. Most of our residents, when they’re gone, like mean when they die, we always in tears, you know, even for, you know, we’re not related … (HCA)
There’s not even a debriefing of staff. We used to sit down and talk about the person years back, but we don’t do anything like that now. It’s almost like they’re just a patient; they’re not your family - why are you worried about it - why does it upset you? If you’ve nursed someone, or had them and their families - the nursing home is different to a hospital; you do become part of their lives - they become part of yours. You see them every day, their families come and go, and they call you by name … . It’s not about just, they’re not just another patient that you’re looking after like in a hospital for two weeks and they go home. (EN)
Then they [family] stayed there. I don’t know how long they stayed but it’s different from my culture. If it’s my culture we’ll stay with the body. We won’t leave the body alone. I think they left the body early morning … all of them went home. Then they came back in the morning when the funeral director came. (RN)
The family in this instance as well had decided that they would just go with the cremation and no service, so there was some staff that were quite upset about that. (EN)
Oh, we just – we just, oh, well we, basically we just talk with each other, and talk the family, and, yeah … . we just carry on, yeah. Just carry on, move on … but that’s just the way it is, we just move on, and yeah, and try and make it easy for the ones that are still here, coz some of the other residents can get quite emotional.(HCA)
Yes, some need some counselling from, you know, from their peers and the nurses around them, especially the newer ones who’ve not been there and seen it. (Manager)
But I think as you do this job for a long time you grieve, you go to the funeral, and then you do move on. You have to, because there’s another, I mean there’s a lady who came in like the next, two days later, into the room, and you know, you have to move on, don’t you? … That’s the cycle, so isn’t it, just like we, we share in their journey, we’re there, and help them in their journey. There’s another bed empty, there’s another person that comes along … . You have to move on. Yeah, but it’s not easy. (RN)
A Good Death: After Death Practices and Rituals?
Specific remembrance rituals were limited in the RACs and if they existed, were generally for staff rather than for other RAC residents, revealing the tension between RAC facilities as a place of work, and also a place to call home and a place to die.
We would have our own service for him here in the chapel … for the staff, not really for the other residents but for the staff. You know, some closure (RN Manager)
We’ve just started again, to put a little photo with flowers and a little candle, fake candle, once the person’s died so that people know that someone has left us. Because you’re a community and sometimes people don’t know that residents have left. That has been a bit controversial with some of our families. Some of our families don’t like it, they say we don’t want to see it, we don’t feel everyone should be exposed to death. We know that person’s gone, why are you doing this. (Facility Manager)
Many facilities had a ‘front door’ approach to removal of a dead body, often augmented with a ritual where there would be an impromptu guard of honour formed by staff members who were around at the time. This ritual sees staff line either side of the route of the exiting dead resident’s body as a way to show respect. Yet, it was acknowledged as ‘quite a divisive issue’ by one facility manager who made sure the dead were not “shushed out like, you know the cleaners’ entrance or the tradesman’s entrance” but were “good enough to go out the front door”. This sentiment was echoed in other facilities, where body removal practices and rituals were portrayed as a sign of dignity.
No, no we’ve got a very strong thing that you come in the front door, you go out the front door. (Facility Manager)
And we’re always very aware of other people around because you know, you don’t want death … . So we will always make sure that the funeral directors arrive out of busy hours. So not around lunchtime when there’s lots of people in the dining area, and you go past. You’ve got to think about other people, so we always look at the timing. And then we will always, I’ll always walk with the body or if I’m not here someone will. And just, we might put up a screen if there’s an activity going on, we might just put a screen up discreetly, for both parties really.(Facility Manager)
Rituals of Cleansing and Re-Populating the Space
The presence of some sort of post-death room cleansing ritual was reported by several participants. A prayer or blessing was offered (or simply spoken into) once the body had been removed to spiritually cleanse the room and prepare it for the next resident. For some, a staff member performed the ritual; for others, a designated chaplain or nun from a Christian denomination did so; and some designated this role to an appropriate Māori staff member or kaumatua.
1
That some of the religion, they want to bless the room before admitting another person … . Open the windows, let the spirits out – … We do it here, we just get [manager] to go and bless the room.(RN)
No, we go say goodbye to the person if it’s in our shift, we go, knock on the door and say, oh goodbye, Mr. [name] you know may you rest in peace. We say something like that, and then we close the door, you know other staff will just go and check (RN)
We always open the window, … And I said, we leave it for twenty-four hours, and he asked me why, and I said, we get somebody to come in and bless, or when the family have taken everything out, then we get it blessed.
We try to give family twenty-four hours if we can, or forty-eight at a stretch (Facility Manager)
Yeah, it’s slightly awkward that, death, because we’re not really meant to tell them [residents] that others have died until the family either tells them or it’s in the paper. And I mean that’s really hard sometimes, cos there’s often a delay.
In a small number of facilities, residents were ‘told’ of a death through the social practice of displaying a photo of the recently deceased in a public area.
We have a very good photo of them framed and we place that in the dining area with an angel which will probably inform … the other residents that lady’s gone (RN)
We were … about two minutes late when she passed [at 5.00am]. She’s been here for a long time, one of the longest, Ray [pseudonym] was a piano player and singer, played Amazing Grace, a full song on the piano, and then on the last note, she took her last breath … And Ray is actually forgetting notes now, you put a book in front of him, he wouldn’t play it at all. … So we do have cameras, so I had a look at - this really happened, and yes, he did play the piano. And I was shocked to see. (RN, Facility Manager)
We take their photo … and we always put that up in the nurses’ station … they can look at that [staff] and see who’s died and maybe a vase of flowers.(RN)
Discussion
This study set out to explore the death and post-death practices and rituals found in the 49 RAC facilities in the dataset. The numerous practices and rituals revealed in the results illuminated a wide variation in RAC’s beliefs and assumptions about death and post-death, as the facilities function as both places to live and places to die.
Alone at Death
Dying alone is still not currently part of our constructed notion of a ‘good death’ (Seale, 2004; Timmermans, 2010), despite challenges to this premise (Kellehear, 2009). A good death is linked to dying with dignity (Onishi, 2014). Unsurprising then was the pressure that RAC staff expressed to not let someone die alone and the consequent extra demands created for staffing at times when residents were actively dying. However, accompaniment behaviour during the active dying phase in a RAC facility is governed by the dominant hegemony of what is acceptable and unacceptable in that organisation (Kanitsaki, 1999; Osterlind et al., 2011). A facility’s orientation to death – whether death is seen as public or private, accompaniment behaviour during dying, the existence of dying and death rituals or practices – all signify aspects of more deeply held beliefs about death in a RAC facility. For example, RAC facilities need to be caring communities. Dying alone poses a threat to that ideal (Seale, 1995) and could accentuate the inequality of palliative care offerings in RAC as compared to other settings (Connolly et al., 2014a; O’Connor, 2009). The lack of integration of specialist palliative care in residential care for older adults (Johnston et al., 2019) is another example, revealing also the liminality of RAC facilities between places for living and places for dying.
Passing on
The belief that death is a spiritual passing on, and not just a medical or biological process was central to the findings. Indeed, the frequently reported presence of room cleansing or blessing rituals post-death indicates that there is still a religious/spiritual element in RAC death practices in New Zealand, even if, this was often a step away from formal, commissioned rituals performed by ‘qualified’ clergy. Rather, practices in the study were undertaken informally by culturally or spiritually appropriate individuals within an organisation who had sufficient agency to conduct the ritual. Aotearoa/New Zealand is a society where worldviews overlap to varying degrees, especially European and indigenous Māori worldviews. The model for Māori health, Te Whare Tapa Wha (Durie, 1985), places Te Taha Wairua (spirituality) central to Māori health. The spiritual room ‘cleansing’ practices revealed in the data, though revealing a drift away from formalised Western religious rituals, signals a continued acknowledgement of a spiritual dimension to death. The presence of ‘hidden’ or informal spiritual advisors on staff who are called on to carry out certain rituals needs to be part of further research exploring spirituality at end of life for staff, residents and families (Egan et al., 2017).
Rituals
Findings regarding staff grief practices are in line with previous research (Moss et al., 2003), including in relation to the use of informal talk and sharing practices to remember the deceased resident, and caring for each other in processing loss. However, collective life-transitioning death and dying rituals (Quartier, 2010) were scarce in the RAC facilities. Our finding of the paucity of post-death remembrance rituals among other residents (and staff) was also reported by Maitland et al. (2012) and Komaromy (2000). This deficit has been previously criticised by Bern-Klug (2011) who contends that rituals are needed to re-establish an appreciation of meaning and connection. These deaths are seen as predictable and cast as “of course they are dying, they are old” (O’Connor, 2009, p. 267). In New Zealand, like other secular, high-income countries, the scant ritual around the death of an older RAC resident, the absence of family from most immediate post-death practices (e.g., preparing the body) and its professionalization (e.g., undertaker) perhaps signifies the continued move towards the secularisation of death and dying where there is no belief in an afterlife or a god (Walter, 2015). The on-going public discussion around assisted death and euthanasia may also signify this move (Danyliv & O’Neill, 2015).Jupp (2015) notes that in a secular society, meaning-making in death has new challenges for those with a humanistic disposition as religious rituals and practices that heralded life after death no longer hold the same meaning. As well as the collective life-transitioning rituals for residents, there is a place for collective and individual facility rituals (Quartier, 2010) with resources available to support staff in the substantial death and dying responsibilities they bear. Consideration must be given to what RAC staff consider to be important, and also reflect the RAC’s organisational values around death and post-death.
Implications and Recommendations
Acknowledgment of and formal support processes for the heavy load of end of life care provided by RAC staff is vital. This need will only intensify as the number of deaths in RAC is projected to increase dramatically in the coming decades. In addition, with a rise in multi-religious and multi-cultural societies, an increase in post-Christian spirituality, and an admonishment in Aotearoa/New Zealand to adopt Māori health perspectives in public health (Waitangi Tribunal, 2019), RAC facilities will face increasing challenges in providing good death experiences for all of its staff, residents and families. Forms of dying and death will be less normalised across a diverse society, requiring innovation and increased training and support for staff at the leading edge of death and dying in RAC facilities, and greater transparency from RACs concerning their approach to the liminality between life and death. Future research should further examine the informal role that various cultural and spiritual advising staff play in RAC facilities to capture and understand these informal death practices as well as further investigation of disenfranchised grief in the RAC context, both for residents and staff. This knowledge can be used to inform RAC’s own policy approaches to collective death and dying rituals and practices thus clarifying what the RAC facility considers to be important and reflective of their organisational values for any death/post-death ritual, while also providing opportunity for individual ritual and practices which cater to the dying, and the grieving loved ones involved.
Limitations
The relationship between the themes explored and the cultural groups represented in the data set (Table 1) are unknown, given the interpretive nature of the research. The research would have benefitted from having a broader cultural mix of deceased residents (89% NZ European; Boyd et al., 2019) that RAC staff were referring to when talking about death and dying rituals and practices for residents in their context.
Conclusion
Overall, death and post-death rituals in RAC facilities were limited. Practices to facilitate current approaches to good death in RAC facilities reflected the tensions surrounding death and dying for residents, staff and families in the RAC context. Further consideration of death practices and rituals is warranted, given RAC facilities are increasingly a more common place of death in most resource rich countries and given observations of ageism and disenfranchised grief in the sector. RAC facilities need to make visible, approaches and beliefs about death in their facility, both for staff and for residents and their families. This will require innovation and increased training and support for staff. In-depth ethnographic research would go further in highlighting ritual and practice surrounding death in RAC facilities. It would also provide deeper insights into the hegemonies adhered to in practice.
Footnotes
Acknowledgments
Thank you to the staff involved from the residential care facilities for their time and willingness to be part of this research project. Thank you also to Sue Foster, a researcher on this project for her fabulous work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by New Zealand National Science Challenge: Ageing Well (Grant #UOOX1508) and New Zealand Perpetual Guardian/Ted and Mollie Carr Trust.
Note
Author Biographies
![]() .
.