
Abstract
Frequent exposure to patient deaths prompts nurses to experience grief. Unresolved grief leads to harmful consequences of nurses’ mental health and quality of nursing care. A cross-sectional study using an online survey was conducted to determine the psychometric properties of the Grief traits and State Scale for Nurses. Exploratory factor analysis revealed two factors measuring the level of nurses’ grief traits (Cronbach’s alpha: 0.84) and two factors in grief state (Cronbach’s alpha: 0.86). Nurses’ feelings of unable to provide good care were associated with a higher risk of grief (odds ratio (OR): 4.30, 95% confidence interval (CI): 1.45–12.75), uncomfortable feeling toward deaths (OR: 11.29, 95%CI: 1.48–85.91), and emotional exhaustion (OR: 7.12, 95%CI: 1.63–30.99). Results indicated that the scale was reliable in determining the levels of their grief. Nurse managers can use the scale to identify their nurses’ levels of grief, creating opportunities to influence the resolution of the grief experiences.
Nurses caring for patients in critical conditions can experience patient deaths. The deep emotional involvement in caring for patients who die can cause grief and heightened psychological burden. With the current Covid-19 pandemic, mortality rates increased, which caused nurses to witness a high number of deaths in a short period of time more than they were used to do (Lusher et al., 2020).
While patient deaths are unavoidable events in hospitals, not every nurse is prepared to deal with it (Zheng et al., 2018), frequently leading to nurses’ grief being unrecognized and unresolved. This type of grief is known as disenfranchised grief, an unacknowledged and often not openly recognized or socially supported expression, which makes the mourning process more difficult and reactions of grief becoming more complicated (Doka, 1999). Furthermore, grief can be related to the actual loss due to death and can be related to other losses not caused by death itself, for example the hidden distress from job loss, illness, and infertility (Doka, 1999).
In addition, disenfranchised grief arises when the loss, the relationship, and the griever are not recognized, such as the loss of a caregiver (Doka, 1999). Nurses as the primary caregiver in hospital settings were reported to experience actual loss due to the death of their patients. Often, this loss is unacknowledged but manifested as chronic depression at home and at work and as guilt, with nurses continually pondering how their patients died (Boyle & Bush, 2018). If the grief is not resolved, it can result in the decreasing quality of nursing care, chronic depression at work (Boyle & Bush, 2018), compassion fatigue (Carton & Hupcey, 2014), burnout, job dissatisfaction, intention to leave the workplace and nursing profession (Adwan, 2014).
Another consequence related to nurses’ grief is vicarious trauma, the ongoing process of grief expressions over time as caused by witnessing other people’s pain and suffering (Jefferson Center, 2021). Taylor et al. (2016) has found that vicarious trauma in nursing practice is mostly related to death and dying. This can be influenced by work and non-work factors, including working environment, working attitude, individual characteristics, and coping strategies (Sabo, 2008). Nurses who provide continuous care for patients who are suffering and dying have experienced this effect of vicarious trauma expressed as fear, helplessness, and feeling of awfulness (Sabo, 2008). Still, another type of grief is traumatic grief, a combination of trauma and loss due to sudden death of a significant other in a traumatic event such as homicide, violence or accident (Neria & Litz, 2004). However, in this study, nurses’ grief does not qualify as traumatic grief.
Providing care to dying patients requires knowledge and adequate stress coping abilities (Karadag et al., 2019). In these situations, nurse managers must identify ways to support nursing staff, especially those who practice in critical care by preparing, supporting, and establishing environments for grief resolutions. To facilitate the identification of nursing staff grief situations, an instrument to measure the grief of nurses is needed. Several measuring instruments on grief exist, but these focus on patient families, caregivers, and general healthcare workers, namely: the Grief Support in Healthcare Scale (K. A. Anderson et al., 2010), Prolonged Grief Disorder-13 questionnaire (Prigerson et al., 2013), and the Revised Grief Experience Inventory (Lev et al., 1993).
With nurses’ grief being different in nature and without instruments to measure their grief, Betriana et al. (2021) realized that developing a grief scale specific for nurses is essential. The significance of developing the Grief traits and State Scale for Nurses (GSSN) and testing the psychometric properties of GSSN is recognized for measuring nurses’ grief experiencing patient deaths in clinical settings (Betriana et al., 2021). The GSSN can be used as a way that provides basic information to programs as interventions of grief during the pandemic. By helping nurses to resolve their grief, further depletion of invaluable nursing care can be prevented.
Review of Literature
Grief is defined as the emotional feelings of the individual who experiences the loss. Nurses may experience grief personally or become the support system for patients and their families who experience grief and loss (Oates & Maani-Fogelman, 2020). Grief experienced by nurses depends on their practice specialty but is realized depending on their experience around the loss of their patients (Wisekal, 2015). While some nurses are prepared and have adequate abilities toward resolving their grief, Charalambous and Kaite (2013) found that many nurses require professional grief support.
Studies have been conducted to examine nurses’ experience of grief. Betriana and Kongsuwan (2020) found that nurses expressed their grief in terms of crying, feeling sad, feeling disappointed, and feeling guilt. Khalaf et al. (2018) found that reactions before and after patient deaths are manifold, such as blaming themselves for causing the patient’s death, advancing intentions to move out of their units where deaths occurred, altogether influencing the way nurses deal with patient deaths. Nevertheless, Kellogg et al. (2014) reported that while nurses provided emotional care for patients’ families, emotional support for them was found to be unavailable, while Kain (2013) noted that in encountering patient deaths, nurses were found to desire an acknowledgment of their own loss (of their patients), and support from peers.
However, in other studies, nurses admitted suppressing their feelings and emotions when encountering patient deaths because they were trained to do so. The results were feeling vulnerable and being burned-out (Liu & Chiang, 2017). Jonas-Simpson et al. (2013) found that even if the experience of grief was found to be difficult and hard, it was also viewed as inspiring change and growth as a person, enabling nurses to gain abilities communicating with bereaved families over the years.
Aim
This study determined the psychometric properties of the GSSN to measure levels of nurses’ grief.
Methods
Study Design
This study is a cross-sectional study using an online survey (Survey Monkey®) format to measure the grief levels of nurses who experienced caring for patients who were dying and who have eventually died.
Sample
The GSSN was distributed to professional nurses who met the inclusion criteria: 1) Registered nurses (age less than 70 years old), 2) Understood and spoke English, 3) Experienced caring for patients who eventually died, and 4) Who were willing to participate in the survey. The exclusion criteria included: 1) Registered nurses without direct experience in caring for patients who eventually died, and 2) Registered nurses who did not speak/understand English.
The following recommendations for sampling of 5:1 (subjects-to-items) ratio (Habing, 2003), or 200 participants were considered to constitute a fair and acceptable sample size (Comfrey & Lee, 1992). The total number of subjects who responded was 263, however 57 responses were excluded because of incomplete data, and unusable data because subjects failed to meet the qualification criterion of having direct experience of caring for patients who eventually died. The final number of 206 subjects consisted of usable data obtained from the subjects’ responses.
Ethical Consideration
This study was approved by the Ethics Committee of a University Hospital in Japan. In the Survey Monkey® link, after the participants read the invitation and information about the study, their consent to participate was acknowledged after clicking the “agree” box. Participants’ personal data and responses to the questionnaire were kept anonymous, with only the researchers able to access these for analysis and interpretation. Their information was kept in the researcher’s personal computer secured with passwords.
Data Collection Procedure
Data were collected from August to November 2020. After obtaining ethical approval, key persons of the Filipino Nursing Diaspora network (FiND) were contacted to request their assistance in conducting the survey among Filipino nurses in the United States and in other countries. After that, the link to the questionnaire was distributed through Survey Monkey®. Colleagues and friends of the researchers who met the criteria were provided with the questionnaire link and were also requested to distribute it to their colleagues and friends who met the criteria.
The Grief Traits and State Scale for Nurses
Before developing the The Grief Traits and State Scale for Nurses (GSSN), the researchers had already conducted a literature review focusing on nurses’ grief (Betriana & Kongsuwan, 2019a), and had conducted qualitative studies to explore the experience of nurses’ grief in an ICU in Indonesia (Betriana & Kongsuwan, 2019b, 2020). Items of GSSN were constructed from contents of the reviewed literature and studies centered on nurses’ grief experiences in various areas in the hospital settings (Anderson et al., 2015; Betriana & Kongsuwan, 2019a, 2019b, 2020; Marcella & Kelley, 2015; Shimoinaba et al., 2014; Wenzel et al., 2011; Wilson, 2014). Those items were confirmed by the experts in grief and end-of-life care. The configuration of the State-Trait Anxiety Inventory (Spielberger et al., 1983) was referred to develop the GSSN. The GSSN was developed to measure levels of nurses’ grief (Betriana et al., 2021) and designed with a global application. It was developed in English but has not been tested in this original version; however, a translated version in Indonesian (Bahasa) was tested among Indonesian nurses who experienced patient deaths, revealing that the GSSN could measure levels of grief among Indonesian nurses (Betriana et al., 2021).
The GSSN is a 31-item self-report grief measure with 12 items measuring grief traits and 19 items measuring grief state. The GSSN measures two types of grief: 1) grief trait, as a personal characteristic, and 2) grief state, which is about an event. Responses to the items in the scale were measured using a 5-point Likert Scale. Grief traits were rated as follows: 1= not at all, 2= slightly so, 3= somewhat so, 4= very much so, and 5= extremely so. Grief state is rated as follows: 1= never, 2= rarely, 3= occasionally, 4= frequently, and 5= always.
Statistical Analyses
Data were analyzed and interpreted using the IBM SPSS version 26.0. Descriptive statistics were used for demographic characteristics. For analyzing the GSSN questionnaire items, the Kaiser-Meyer-Olkin (KMO) test and Bartlett’s test of Sphericity were applied for sampling adequacy. The KMO value of 0.5 and above indicated that the analysis could proceed to EFA (Kaiser, 1974). Exploratory Factor Analysis (EFA) was performed with principal axis factoring and Promax rotation. Factors were generated with factor loading of > 0.40 with at least three items (Samuels, 2016).
To ensure the reliability of GSSN, Cronbach’s alpha was calculated with the acceptable value ranges from 0.70 to 0.95 (Tavakol & Dennick, 2011). The total score of each Grief trait and Grief state of each factor were calculated. Pearson product-moment correlation coefficient was computed to examine the relationship between Grief traits and Grief states using their total scores. The identified factors used mean factor points. The scores of the GSSN were categorized into three levels: normal, high, and severe level of grief. These categories were determined by the cutoff point of the mean and standard deviations (SD) (Singh, 2006). “Normal level” was determined by the score of ≤Mean+SD. A “High level of grief” was established between >Mean+SD to Mean + 2SD, and “Severe level of grief” was ascertained with scores of >Mean + 2SD.
The Odds Ratio (OR) and 95% Confidence Interval (CI) were calculated to determine the risk of grief in the total score, and the individual factor in both the Grief traits and Grief state. To examine the OR, subjects with high and severe levels of grief comprised the risk group.
Regarding sample size estimation for correlation, a statistical power analysis was performed. The effect size is considered to be large based on Cohen’s (1988) criteria. With an α = 0.05 and power = 0.95, the estimated sample size needed with effect sizes using G*Power 3.1.9.7 (Faul et al., 2007) was the correlation coefficient (N = 134), and the contingency tables (N = 172). Therefore, the proposed sample size was acceptable for this study.
Results
Descriptions of Subjects
Of the 206 subjects, the majority were in the age range of 31–40 years old, female, graduated with a baccalaureate degree in nursing, practiced in acute care settings, with work experience for 8 months − 10 years. Before completing the questionnaire, these subjects experienced patient deaths for a period of more than one month, experienced caring for 1–15 patients who eventually died, with a frequency of experiencing patient deaths of once or more in a month. However, there was a smaller number of subjects indicating their educational qualifications and last death of patients because of missing information (Please see Table 1).
The Grief Traits and State Scale for Nurses
The results for the Grief traits as revealed by the KMO was 0.81 and Bartlett's Test of Sphericity was p < 0.001, indicating that sampling was adequate for factor analysis. EFA generated two factors (see Table 2), namely: Factor 1: Emotional mood swings (Cronbach’s alpha = 0.88), and Factor 2: Uncomfortable feeling toward death (Cronbach’s alpha = 0.70).
Characteristics of Subjects With Corresponding Distribution of the Level of Grief.
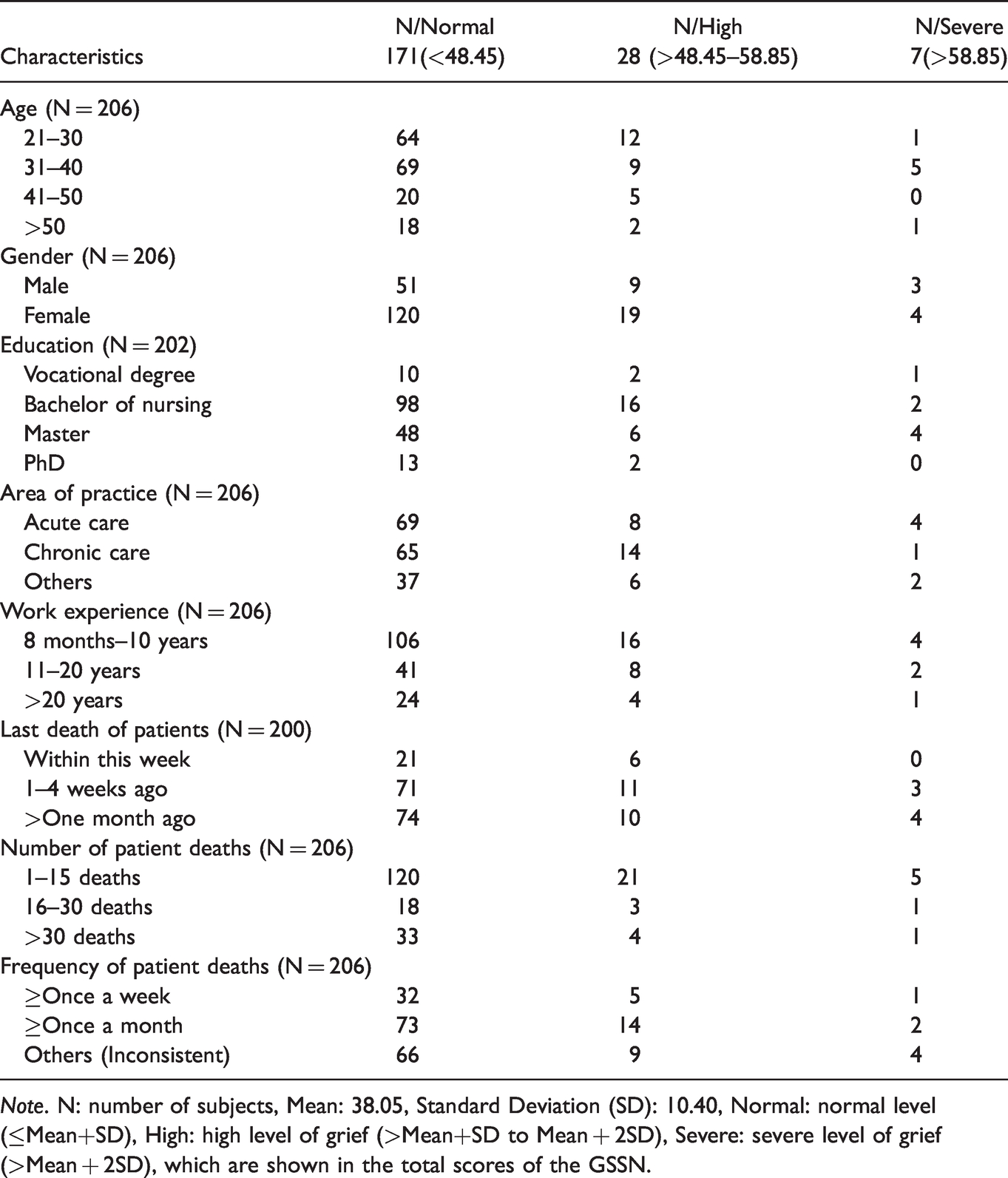
Note. N: number of subjects, Mean: 38.05, Standard Deviation (SD): 10.40, Normal: normal level (≤Mean+SD), High: high level of grief (>Mean+SD to Mean + 2SD), Severe: severe level of grief (>Mean + 2SD), which are shown in the total scores of the GSSN.
Factor Analysis of Grief Traits.
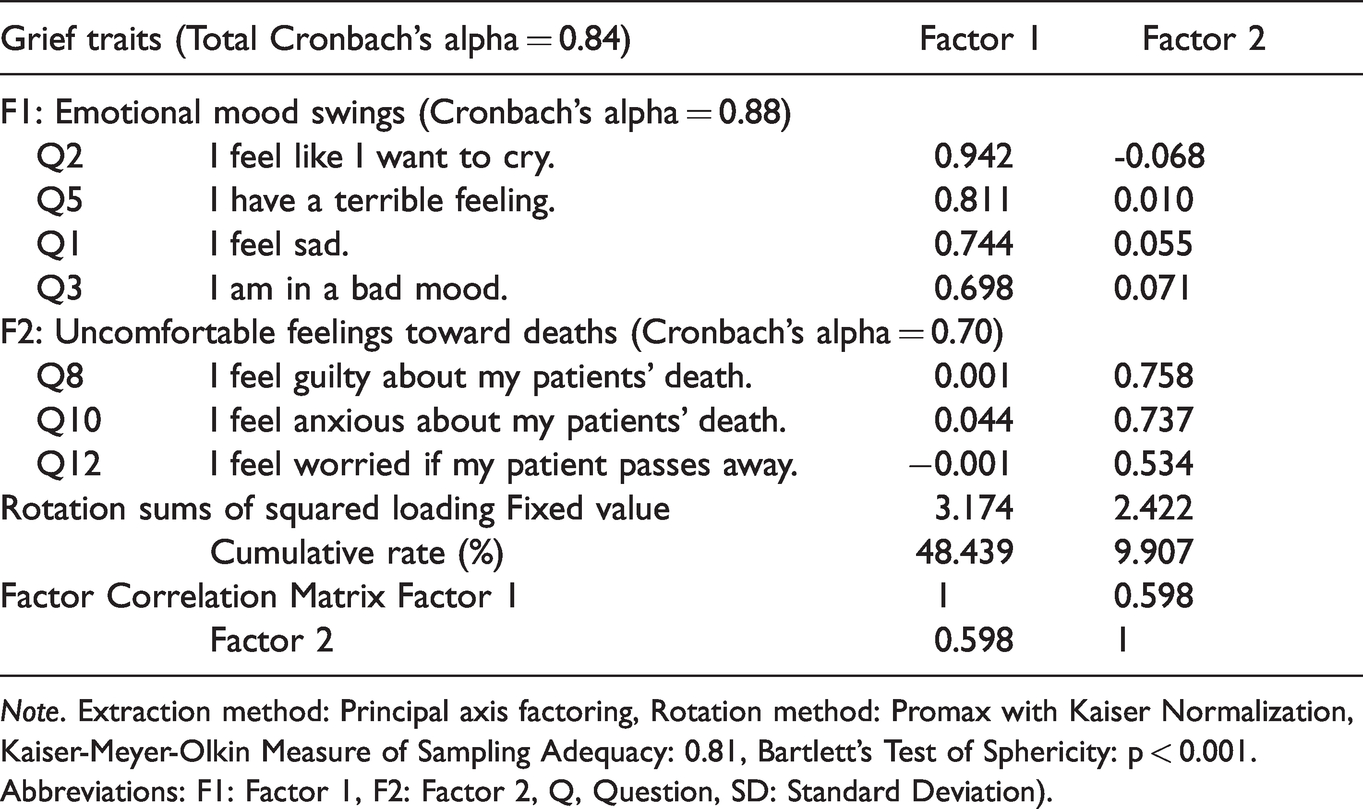
Note. Extraction method: Principal axis factoring, Rotation method: Promax with Kaiser Normalization, Kaiser-Meyer-Olkin Measure of Sampling Adequacy: 0.81, Bartlett's Test of Sphericity: p < 0.001. Abbreviations: F1: Factor 1, F2: Factor 2, Q, Question, SD: Standard Deviation).
From twelve items comprising the Grief traits, five items were discarded because of factor loading, which was less than 0.4. The total number of items in the Grief traits scale (after EFA results) was reduced to seven items, with a total Cronbach’s alpha of 0.84, indicating reliability was established.
For Grief states, the KMO value was 0.84 and Bartlett's Test of Sphericity was p < 0.001. EFA resulted in two factors (Table 3), namely: Factor 1 (feeling sadness toward patient deaths) with Cronbach’s alpha of 0.84, and Factor 2 (emotional exhaustion after caring) with Cronbach’s alpha of 0.81. The total Cronbach’s alpha for both factors was 0.86. EFA retained 10 items. Nine items were removed.
Factor Analysis of Grief States.
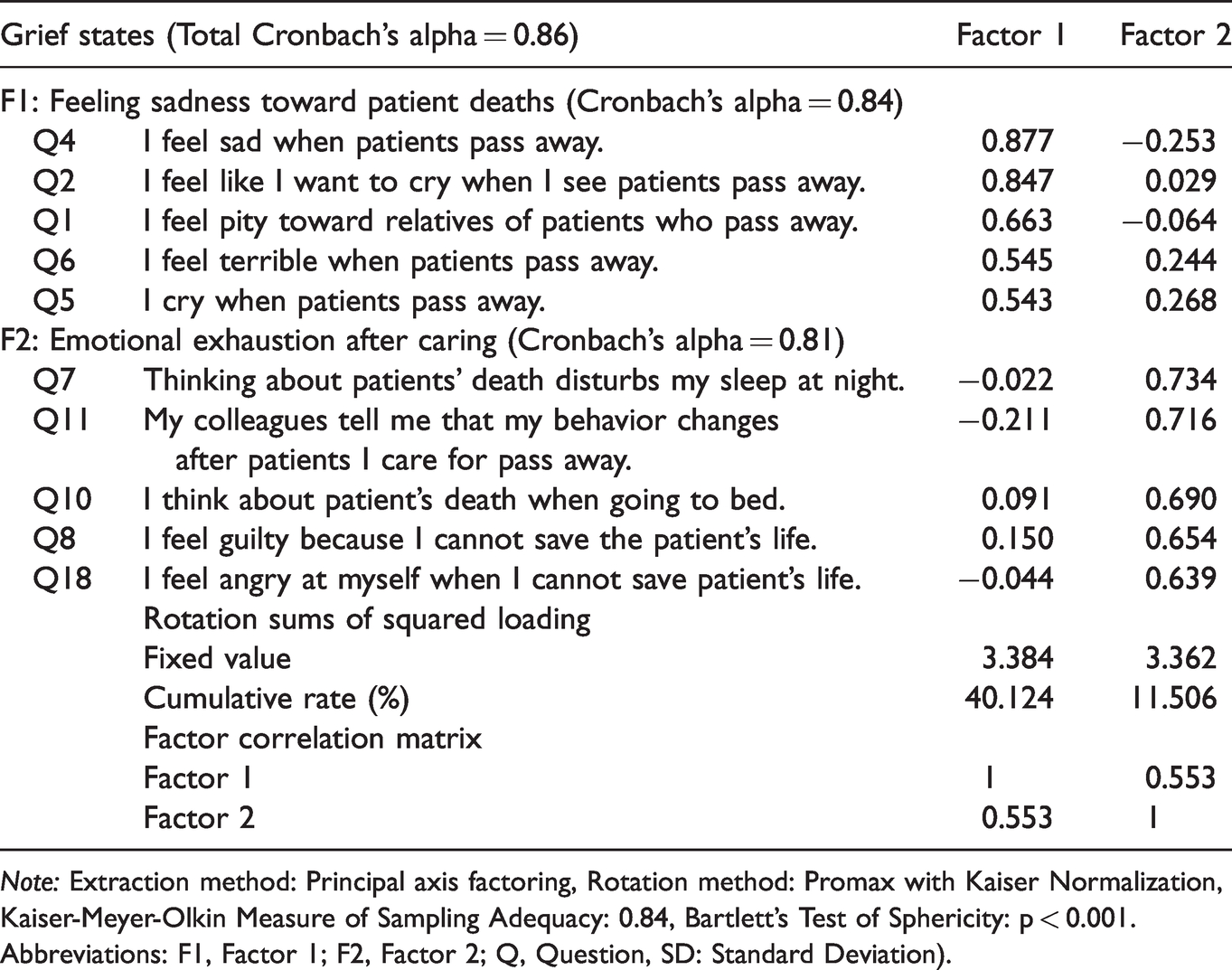
Note: Extraction method: Principal axis factoring, Rotation method: Promax with Kaiser Normalization, Kaiser-Meyer-Olkin Measure of Sampling Adequacy: 0.84, Bartlett's Test of Sphericity: p < 0.001. Abbreviations: F1, Factor 1; F2, Factor 2; Q, Question, SD: Standard Deviation).
Furthermore, subjects were asked to respond to the four items related to their understanding of causes of grief and coping strategies. These items were whether the nurses felt grief due to witnessing patients’ deterioration before death, whether the nurses felt grief due to feelings of having been unable to provide good care when the patient was still alive, whether the nurses had a place where to express their grief, and whether the nurses could express their grief after the patients’ deaths.
In the case of subjects experiencing a “feeling grief due to feelings of having been unable to provide good care (Item 2),” OR and 95% CI showed significant higher grief risk in the total score of GSSN (OR: 4.30, 95%CI: 1.45–12.75); Grief traits Factor 2 (OR: 11.29, 95% CI: 1.48–85.91); and Grief state Factor 2 (OR: 7.12, 95% CI: 1.63–30.99), respectively (Table 4).
Odds Ratio of Subjects’ Characteristics With Level of Grief in Total Score and Each Factor.
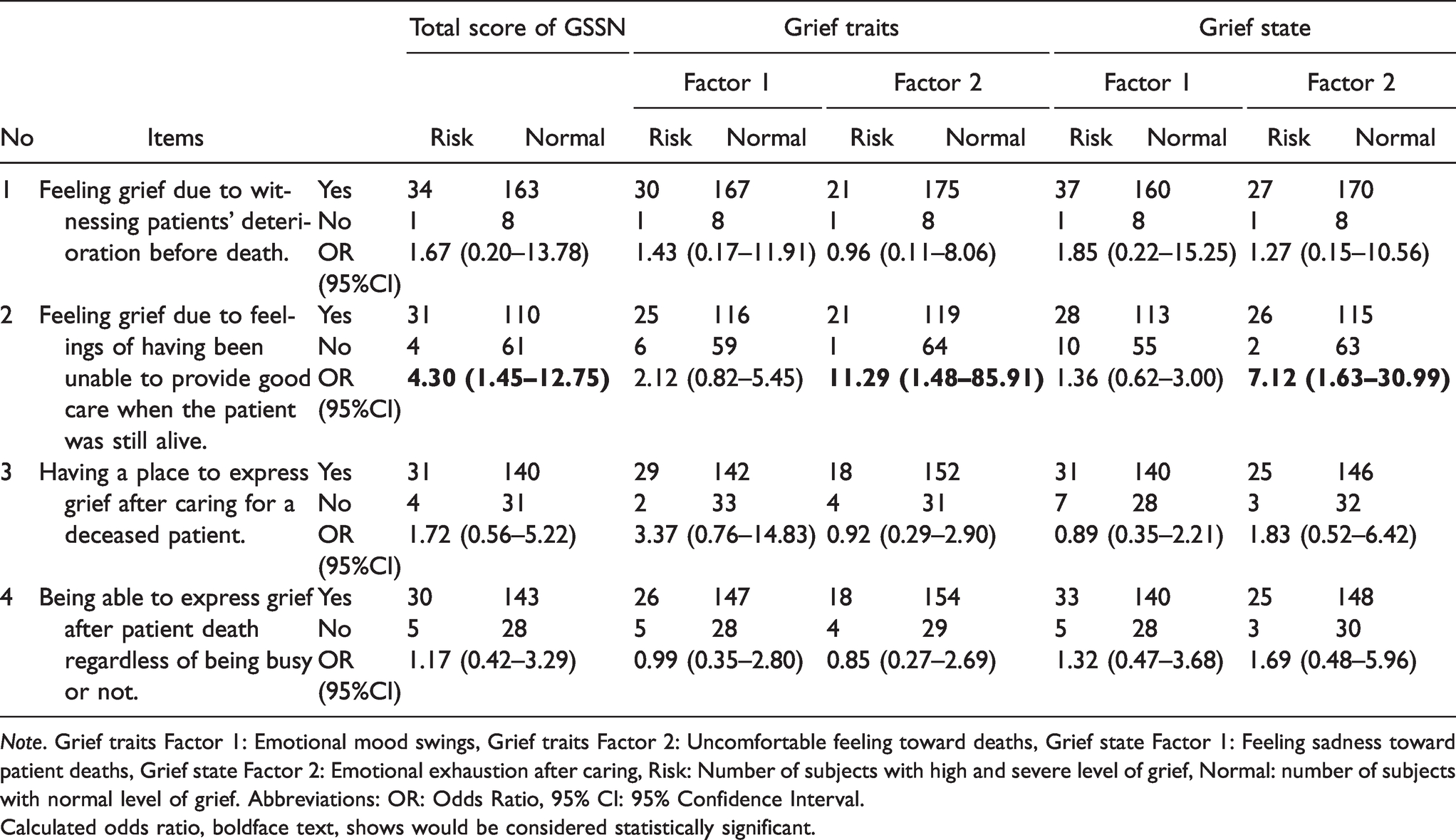
Note. Grief traits Factor 1: Emotional mood swings, Grief traits Factor 2: Uncomfortable feeling toward deaths, Grief state Factor 1: Feeling sadness toward patient deaths, Grief state Factor 2: Emotional exhaustion after caring, Risk: Number of subjects with high and severe level of grief, Normal: number of subjects with normal level of grief. Abbreviations: OR: Odds Ratio, 95% CI: 95% Confidence Interval.Calculated odds ratio, boldface text, shows would be considered statistically significant.
For the OR calculation, the distribution of grief level of Grief traits and Grief state within each factor is presented as normal and risk groups (Table 5).
Distribution of Subjects by the Grief Level in Grief Traits and Grief State and Each Factor.
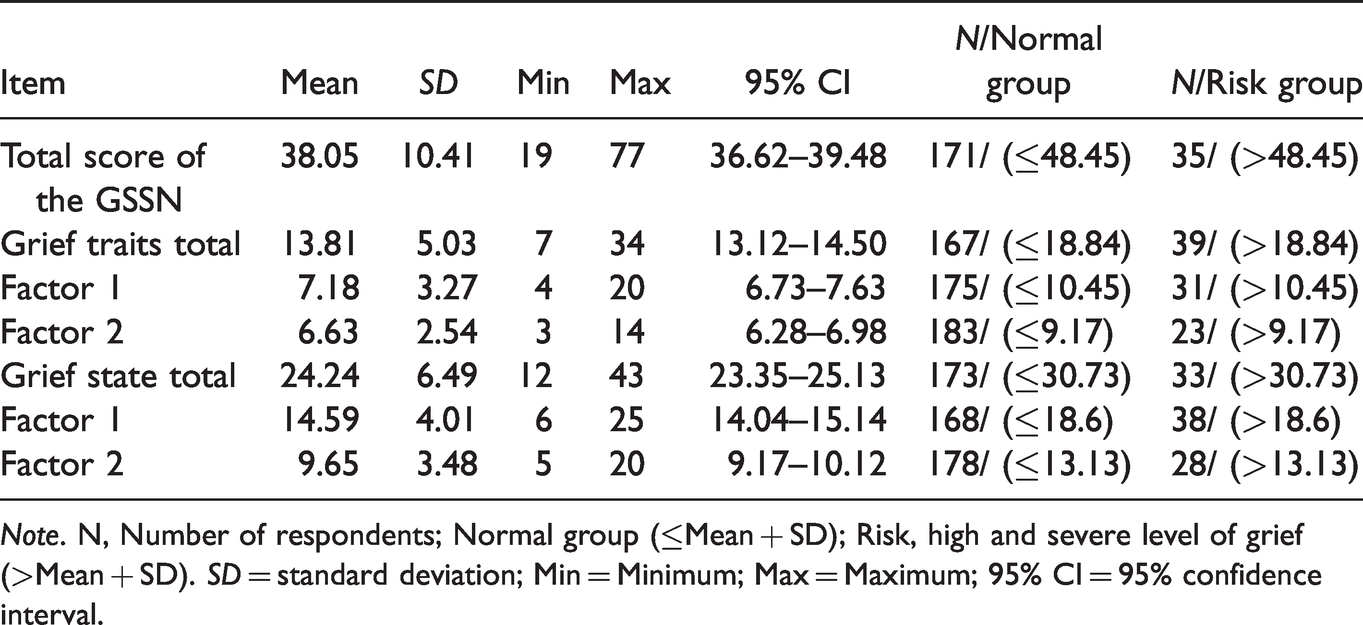
Note. N, Number of respondents; Normal group (≤Mean + SD); Risk, high and severe level of grief (>Mean + SD). SD = standard deviation; Min = Minimum; Max = Maximum; 95% CI = 95% confidence interval.
Figure 1 presents the results of the GSSN analysis. The GSSN measures nurses’ grief traits and grief state. The idea for calculating the GSSN total score was refered from the two dimensions of STAI (Spielberger et al., 1983). In the STAI, the scores were separated from state and trait anxiety. In the GSSN, however, the total scores are calculated by combining grief traits and grief state, which ranged from 17 to 85, with higher scores correlating with higher grief. In the Grief traits, the normal level score is ≤18.84, high level is in the range from 18.84 to 23.87, while severe level is >23.87. In grief state, normal level is ≤30.73, high level is in the range from 30.73 to 37.22, and severe level is >37.22. In the total score, normal level score is ≤48.45, high level is in the range of 48.45 to 58.85, while severe level is >58.85.
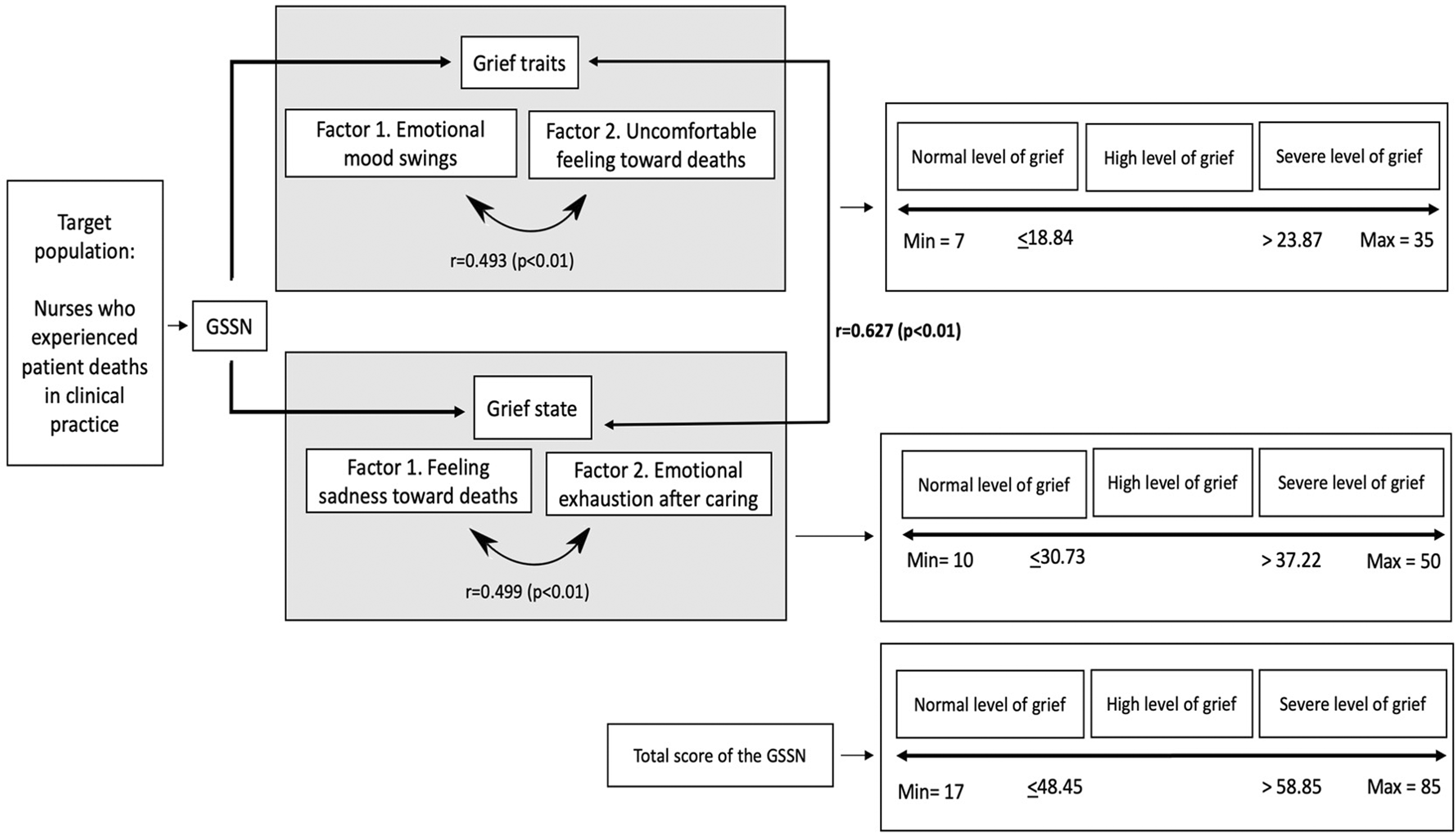
Conceptual Model of the GSSN Analysis.
Correlations show the total score of Grief traits and Grief state (r = 0.627, p < 0.01), factors 1 and 2 in Grief traits (r = 0.493, p < 0.01), and factors 1 and 2 in Grief state (r = 0.499, p < 0.01).
Discussion
The GSSN considers that nurses’ grief is influenced by their personality (Robinson & Marwit, 2006) and emotional state after patient deaths, and is reflected as grief traits and grief state (Betriana et al., 2021). The findings for Grief traits show a positive correlation among factors 1 (emotional mood swings) and 2 (uncomfortable feeling toward deaths) (see Table 2). Given that Promax rotation allows factors to correlate (Howard, 2016), this result is considered valid. Further analysis with Pearson's correlation coefficient showed that emotional mood swings and uncomfortable feelings toward deaths have a moderate positive relationship (see Figure 1). These findings demonstrate that nurses’ personal traits, especially mood swings, influence how they respond to patient deaths.
The personal traits that influence grief are known to manifest as moodiness, emotionality, guilt, and anxiety (Robinson & Marwit, 2006). These manifestations were incorporated as items in the Grief traits. The influence of grief trait highlights the need to control the mood swings and uncomfortable feelings toward deaths, which can be done by creating a supportive working environment for nurses.
Findings of EFA in Grief state showed that both factors are correlated (Table 3), indicating that the result of factor analysis by Promax rotation is considered valid. The result of Pearson Correlation Coefficient shows significant positive relationship, in which feeling sadness toward patient deaths (Factor 1 of the Grief state) has approximately a moderate relationship with emotional exhaustion after caring (Factor 2 of the Grief state) (Figure 1). Rice et al. (2014) found that nurses admitted feeling exhausted and expressing compassion fatigue after caring for dying patients. Similarly, Carton and Hupcey (2014) also found that inadequate grief after patient deaths can result to compassion fatigue.
Compassion fatigue is defined as a biological and psychological exhaustion occurring after caring for traumatized people (Carton & Hupcey, 2014), resulting from exposure to cumulative stress and neglect of one’s emotional needs over time (Adimando, 2018). Unmitigated compassion fatigue can bring about negative consequences to nurses’ physical and emotional well-being, the quality and safety of care, and degree of engagement with the employer. In this situation, establishing the need to reduce compassion fatigue through education and on-site training can enhance nurses’ self-awareness and self-care to deal with stress (Adimando, 2018).
If nurses have feelings of having been unable to provide good care when the patient was still alive, it demonstrates a higher risk of overall grief amounting to 4.3 times greater than normal, uncomfortable feeling toward patient deaths amounting to 11.29 times greater, and an emotional exhaustion after caring amounting to 7.12 times greater than normal (see Table 4). These findings can address the cause of uncomfortable feelings and emotional exhaustion experienced by nurses. For example, nurses who have felt they did not provide good care to support their patient experienced ineffective grief (Shimoinaba et al., 2014).
While patient death is unavoidable, nurses should understand that having feelings of not having provided good care, is not an effective way to cope within their long-term professional life. This understanding and the effective coping strategies can be explained to nurses through death education. Death education and death-related training such as hospital in-service training, continuing education, or education integrated in the basic nursing course was shown to be useful to protect nurses against emotional exhaustion following patient deaths (Guo & Zheng, 2019).
In addition, suggestions to achieve grief resolution include creating a supportive work environment, debriefing with colleagues, and providing grief and death education, thereby resolving nurses’ grief and maintain nurses’ retention from unresolved grief (Hildebrandt, 2012).
EFA was employed for analysis due to population and language changes. From the study of GSSN among Indonesian nurses (Betriana et al., 2021), the EFA generated two factors in Grief traits and two factors in Grief state. Feelings of having been unable to provide good care was found to be significant. These findings indicate that grief is a global phenomenon experienced by nurses regardless of country of origin or residence.
With the results of the EFA being similar between the current study and the study by Betriana et al. (2021), it is suggested that grief resolutions should be culturally and spiritually appropriate for individual nurses. For example, in Indonesia, a country with the largest Muslim population in the world, Islamic belief influences the way nurses experience and cope with grief. Nurses in Indonesia admitted that performing dhizkr (Islamic prayer) helped them control their emotions when dealing with patient deaths, thus end-of-life care with a spiritual approach is appropriate for Indonesian Muslim nurses (Betriana & Kongsuwan, 2019b). While the GSSN helps nurses, nurse managers, and organizations to screen the nurses’ grief and informs the general risk factors, the grief resolutions should be provided based on the appropriate context, situation, culture, and belief of nurses.
Furthermore, in losing significant others, an acute phase of grief can last up to 2 months, although milder symptoms may also linger until a year or more (National Library of Medicine, 2021). During the acute phase, intense reactions usually occur. In this study, the period of mourning of more than one month was determined to occur after the last patient deaths.
As grief has gained interest for researchers, Prolonged Grief Disorder (PGD) was included as a new mental disorder to the 11th edition of the International Classification of Diseases (ICD-11) (Killikelly & Maercker, 2017). The PGD was diagnosed using PGD-13 by Prigerson et al. (2013) based on the criteria of experiencing significant yearning and having at least five symptoms, which involve functional impairment on a daily basis beyond six months after the mourned death. PGD-13 is commonly used to measure grief experienced by people who have lost significant others, such as the loss of family members (Prigerson et al., 2013), losing children (Pohlkamp et al., 2018), losing a spouse (Kim et al., 2020; Schaal et al., 2010), and losing parents (Schaal et al., 2010).
However, nurses’ grief is different from that of family members. Nurses did not have a significant close relationship with their patients and did not meet the patient daily before the patient was hospitalized. Nevertheless, nurses provide care for patients in their end-of-life stage within a range of time that allows them to build relationships with patients, causing a feeling of loss when the patient dies. Multiple factors can cause nurses’ grief, such as nurses’ personality, but more are related to caring relationship such as feeling guilty because of having been unable to save their patients’ life, representing conditions related to caring that are unlikely to occur in other bereaved groups. Thus, the GSSN address those conditions which may not be found in the case of grief due to losing significant others. While the PGD covers period of six months and beyond after a loss, the GSSN can assess nurses’ personal grief traits and state without a considering a fixed period since deaths experienced by nurses are recurrent during their professional life. In view of its appropriateness in assessing grief in nursing and healthcare situation, the GSSN is expected to be useful to assess the grief among nurses and other healthcare professionals in the future.
Limitations
Four limitations were identified: (1) Using one test makes it difficult to answer the complex questions usually asked in the clinical situation. This GSSN survey was conducted without test battery to compare nurses’ grief with similar phenomena such as stress and burnout; (2) Nurses in a state of intense grief may not have participated in this survey because they may have had no desire to participate; (3) It seems that nurses from other countries may not have a tradition of responding to on-line research studies as evidenced by the high number of incomplete questionnaire copies returned; and (4) Duration of this survey was extended up to 3 months. Relying on Survey monkey© as the on-line “server” did not allow for subjects to continue after they had to stop for any reason. This led to a high number of incomplete questionnaires that had to be discarded.
Conclusions
Results of this study demonstrated that the GSSN is a reliable scale to assess the level of nurses’ grief considering grief traits and state. Nurses with emotional mood swings are likely to have uncomfortable feelings toward patient deaths, while nurses who feel sad toward patient deaths also experience exhaustion after caring for patients who died. A higher risk of grief was found among nurses who have feelings of not having provided good care when the patient was still alive. These findings highlight the importance of preparing nurses for patient deaths in their practice by facilitating them to express their grief, creating supporting working environments, and providing education related to death.
Relevance for Clinical Practice
Nursing work, which is susceptible to mental burden, tends to accumulate work stress and has various effects on physical and mental health, especially in the current pandemic where nurses are frequently exposed to patient deaths than they were used to. If mental health care is not properly managed, will not only physical and mental problems arise but the risk of burnout will also lead to rapid turnover. Burnout can reduce the quality of nursing care for patients and pose an organizational problem.
Given that nurses are often found to have difficulty expressing their grief, the GSSN is expected to help nurse managers and institution policy makers to screen their nurse staff, especially those who are at high risk. By answering the GSSN questions, the nurse staff can describe their grief condition and how the grief impacts their nursing work. Nurse managers play an important role in promoting the importance of mental health care for their nursing staff, provide a place and space for nurse staff after the patients they care for pass away, and prepare the professional grief resolution.
Since grief is considered a normal reaction to any type of “emotional” loss in which people need time to heal, there is no ideal time to administer the GSSN. However, this scale was suggested to be administered regularly as one of the mental health monitors for nurse staff, for example every six months. This was suggested because oftentimes, patient deaths take place unpredictably in hospital settings, and nurses can experience symptoms of grief from their patient deaths, several times in many months. Nonetheless, due to the different working environment in each organization, the GSSN should be applied in accordance with the organization culture. If the nurse staff members are uncomfortable in being screened and treated individually as it can create a stigma from colleagues, it is suggested that nurse managers would screen in the group, when necessary, not to disclose the results to others, and prepare debriefing in the group instead of to individuals as the regular activity for nurses in their unit.
Footnotes
Acknowledgments
We would like to express our deep gratitude to the Philippine Nurses Association of America (PNAA), Chair of PNAA Research Committee Dr. Sigrid Ladores, RN, PNP, CNE, and Professor Jerome Babate, RN, MBA, CTC, DMc for their support in endorsing the study to Filipino nurses in the US and in other countries.
Authorship Statement
All authors listed meet the authorship criteria and all authors are in agreement with the manuscript.
Ethical Approval Statement
Ethical approval was obtained from the Ethics Committee of Tokushima University Hospital, Japan (#3586).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.