
Abstract
Introduction
Legacy videography, the creation of a video statement incorporating aspects of emotional processing, constructed meaning, and life review, has emotional benefits for terminally ill patients and their families.(Keim-Malpass et al., 2015) In adult studies, these benefits included spiritual well-being and quality of life.(Rigazio-Digilio, 2001; Taylor-Brown & Wiener, 1993) Videography allows patients a convenient therapeutic outlet for addressing some of the many tasks of dying, including: creating an intentional mechanism to say good-bye, facilitating an opportunity to complete unfinished business, potentially relieving spiritual distress and pain associated with dying, and fostering a means for patients to grieve their losses as well as for parents of pediatric patients to grieve their child’s death.(Chalfen, 1998; Lawrence, 1992; Martinson & Papadatou, 1994) As a media form, videography is an especially feasible way for patients, especially pediatric patients, to leave something of themselves for their families after death.
Leaving a legacy has been associated with health benefits in studies with adults and adolescents as young as 18 years old. Piderman and colleagues have demonstrated the value of legacy documents with Hear My Voice, which develops a spiritual legacy document using a semi-structured interview to facilitate life review by engaging participants in meaning-making.(Piderman et al., 2015) Meaning-making is associated with positive growth for pediatric cancer survivors and their families.(Duran, 2013) Piderman and colleagues demonstrated Hear My Voice’s feasibility and acceptability to patients aged 18–102 years with brain cancer and progressive neurodegenerative diseases;20,21 in subsequent testing, Hear My Voice improved quality of life, spiritual coping, and spiritual well-being, and positively impacted patients’ sense of meaning.(Piderman et al., 2017; Piderman, Radecki Breitkopf, et al., 2017; Sytsma et al., 2020)
Keim-Malpass and colleagues explored legacy-making through blogging by a group of young adults with cancer.(Keim-Malpass et al., 2015) Similar to Hear My Voice participants, the bloggers addressed meaning-making topics important for personal growth and created a legacy for their followers. Akard and colleagues tested a legacy intervention to improve quality of life for children with cancer.(Akard et al., 2015) They reported that the use of digital legacy eased communication and emotional expression.
The use of videography has been previously described in patients with terminal illness.(Rigazio-Digilio, 2001; Taylor-Brown & Wiener, 1993) The purpose of this study was to (1) demonstrate the potential of videography as a therapeutic medium for pediatric patients to address some of the varied tasks of dying; and (2) quantify the feasibility and acceptability of making legacy videos with pediatric patients with a life-shortening condition. We hypothesized that video legacy recordings would be (1) feasible to implement by pediatric palliative staff; (2) acceptable to pediatric patients as a means to share stories and address some of the tasks of dying; and (3) that measures of emotional states would improve after patients completed the videography intervention.
Methods
Participants
This was a mixed-methods study of the feasibility and acceptability of giving children with end-stage life-shortening conditions the opportunity to make a legacy video recording for themselves and their family and friends. The study was approved by the institutional review board. Eligibility criteria included referral to the study by the child’s physician, English-speaking, and ages 8 years of age or older. All patients treated at the children’s hospital for diseases of childhood were eligible for the study, even if over age 18 years. Patients were excluded from the study if either parental consent or child assent could not be obtained, if there were known cognitive deficits or developmental delays in speech and language that precluded successful completion of a video, or if the patient did not speak English.
Procedure
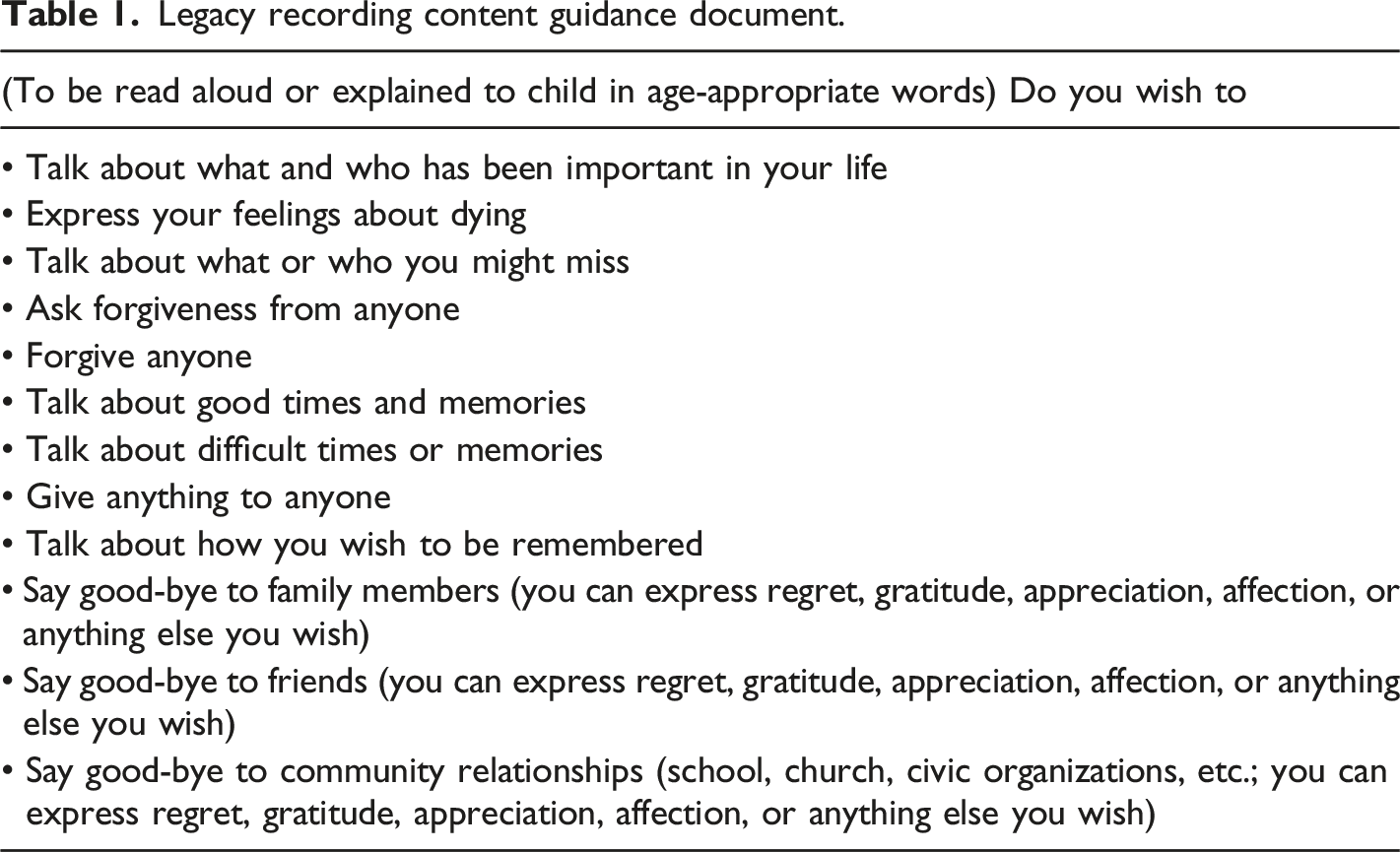
Legacy recording content guidance document.
Study-specific pre-videography participant questionnaire.
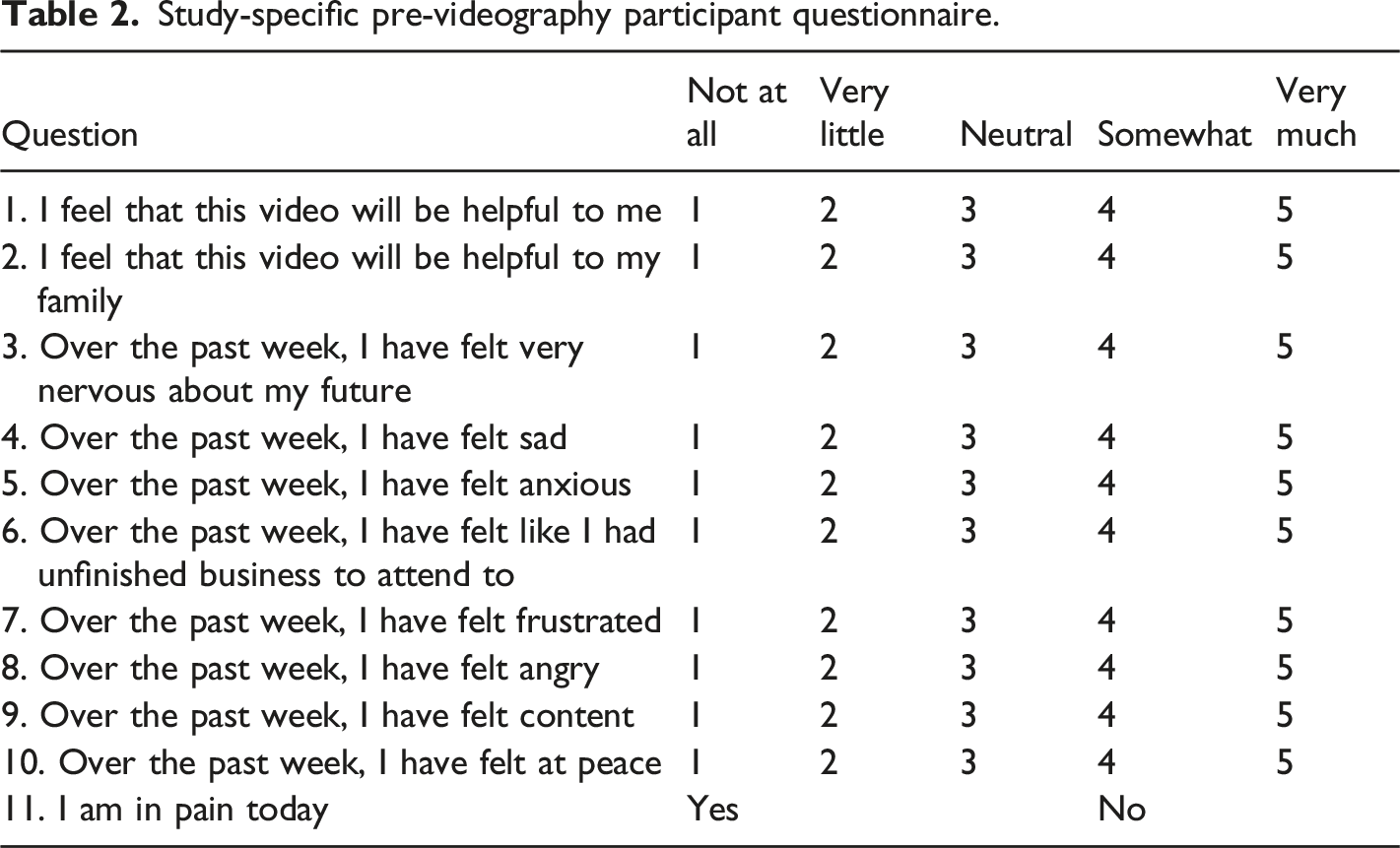
The participant was then given instructions on how to make the video and was informed that he/she could say or do anything he/she wished on the video with no time limit. Approximately two to five days after the video was made, the participant (and the family if they were feeling uneasy or distressed) was invited for an audiotaped exit interview, in which the patient completed a post-videography questionnaire and the family was debriefed. The post-videography questionnaire was identical to the pre-videography questionnaire; an additional question was asked at the exit interview regarding patient feelings about doing the taping (“On a scale from one to five [one being wish you hadn’t and five being very glad you did] describe how you feel about doing this taping.”). For patients who died, a post-videography questionnaire was sent to the parent/guardian to be completed approximately 3 months after the death.
Participants were given a copy of their video which they could view and share with friends and family immediately and/or could choose to have it viewed after their death. The investigator kept a copy of the video as well. Participants were then followed and monitored by research staff for support/additional debriefing needs. If additional assistance was needed, the palliative care psychologist was available to provide care as necessary.
Analysis
Feasibility was calculated descriptively by the proportion of patients who were able to complete all outcome measures of this study. Acceptability was determined by analysis of patient responses to the exit interview question of “feelings” regarding the video recording. A Wilcoxon-signed rank test was used to evaluate pre/post changes in individual emotional states around the making of the video. Qualitative analysis of the video recordings proceeded using thematic analysis (Braun & Clarke, 2012). The recordings in possession of the first author were transcribed by the third author and verified for accuracy by the second author. Transcriptions were read independently, and significant themes identified. Differences in themes and the depth of content in each theme were resolved by consensus.
Results
Ten participants were enrolled, and eight patient participants (four females) completed the surveys and video; seven videos were available for research analysis. The median length of the videos was 6 minutes (range: 2–11 minutes). The mean (SD) age of the patients was 13.4 (5.1) years; median (range) was 11 (8–20) years old. Two participants chose to make their video from home, the remainder in the hospital. One patient did not complete the pre-videography questionnaire, and only four exit interview responses to the question of “On a scale from one to five describe how you feel about doing this taping” were recorded. An additional patient participant was only able to complete the initial interview prior to his death. A 10th patient completed the consent/assent process and subsequently withdrew. Five parents completed pre-video questionnaires, and only one post-questionnaire was returned.
Feasibility and Acceptability
The study was judged to be technically feasible, but would be improved with modifications, such as earlier referral and recording earlier in the trajectory of the participant’s condition. Study team members listening to the audio noted that some participants sounded weak and/or short of breath, and were unable to make videos longer than a few minutes. Of the patients that participated in surveys, two reported being in pain pre-video, and two others reported pain at the time of the post-video survey. The fact the participants were judged to be end-stage by their referring physician may have limited the practical feasibility of completing the video. There was an 80% video completion rate, so the study was judged to be acceptable to the participants. The one person who consented and withdrew before making their video did so due to a change in health status. For the four responses concerning participant impression of doing the taping, the median response was five (very glad you did) with only one response of three on the 1–5 scale. This response indicated that video-making was highly acceptable for those asked. There was a non-significant trend suggesting that participants felt less certain of the video’s helpfulness after making it than they were before (“I feel this video will be helpful to my family”); Wilcoxon signed rank test; test statistic −1.89; p = 0.059). Four of the five pre-video parent responses indicated they believed the video would be very comforting to them at a later date.
There were several potentially interesting findings which trended towards significant relationships (implications discussed below). Patient participants felt less sad and less angry after making the video compared with their feelings before the video (“Over the past week, I have felt sad”; test statistic = −1.66, p = 0.098; “Over the past week, I have felt angry”; test statistic = −1.89, p = 0.059). Patient participants’ self-reported anxiety was decreased after making the video. Prior to making the video, all patients felt some amount of anxiety, and 50% indicated experiencing anxiety somewhat or very much in the week prior to making their video. After making their video, 50% of patients indicated they had felt no anxiety at all (test statistic =3.5, p = 0.13). Actual improvement in mood would support the acceptability of the video. The small sample size suggests caution in interpreting these values.
Thematic analysis
Final themes were identified as Gratitude, Willing Items to Others, Memories, Death/Dying, Disease Experience, and Faith/Spirituality. All participants expressed gratitude to their families and/or friends (“I want to say thank you to my brothers for helping take care of me over the years”). Some participants gave instructions about who should have some of their personal items after their death. While the sample size is quite small, it was only female participants who willed items to others in their video. A 20-year old female said, “something I would like to give to somebody would be these two prayer shawls I have and I say I’d like to give them to my mom because she’s always been there for me and um I just pray that she will take them and anytime she just needs a break and needs to think of me she can just crawl under them and say I love her and there I’ll be with her.” The majority (n = 5) of participants recalled positive memories (”…we went to Disney World and it was fun. We stayed, we got free food, free ice cream, all the ice cream you can eat”). Participants made comments related to death/dying, as well as to missing family, friends, or experiences (“If I do die, I would say goodbye to all my family and friends and everybody”). Participants described some of their disease experience (“I’ve been in the hospital for one whole year and it’s so frustrating to just be in the hospital”) as well as the stigma of disease (“…when I was in Walmart, there was a little kid in the cart and he standed up and said, ‘Hey Daddy, why does that kid have scars on his head?’ I didn’t want to say tumor, so I said, ‘What happened was, aliens abducted me’ and the kids were like, so freaked out.”). Spiritual statements were made by some participants reflecting spirituality as a source of comfort (“…those people at home are watching me and praying for me and just hope for the best”) or as a means of coping by pleading with God (“And I want…to have the rest of my life better. I know you can do it, God, I know you can do it, I know you can fix me…”).
Discussion
We present results of a legacy videography trial with a sample of end-stage pediatric patients. Enrollment and completion rates support the feasibility and acceptability of this type of intervention in a pediatric hospital setting. Post-videography questionnaire data from pediatric participants also support its acceptability. This medium is a tool available to clinicians to aid children and adolescents who may be approaching their end of life.
This study extends the work of Piderman and colleagues on feasibility and acceptability of legacy video interventions to patients under age 18. The findings are also consistent with other research. Spirituality is an important and well-described aspect in lives of many children and adolescents (Cotton & Berry, 2007; Cotton et al., 2012; Cotton et al., 2006) Pendleton and colleagues showed that children and adolescents use spirituality as a coping mechanism, and do so in ways that overlap, but are broader than, the use of spirituality to cope by adults.(Pendleton et al., 2002) Seeking comfort through beliefs, and pleading with the Divine to change one’s situation are common forms of spiritual coping by both children and adults.(Cotton et al., 2012; Grossoehme et al., 2016; Pargament, 1997; Reynolds et al., 2014) The intervention thus at least partially supported one of the tasks of dying; while spiritual coping by pleading is not indicative of spiritual distress, it may be one way in which spiritual distress manifests. Altruism has previously been noted among adolescents with cancer; Kuntz and colleagues described altruism as providing purpose in their experience.(Kuntz et al., 2019) Expressing emotions, which participants in the present study certainly did, has been shown to relate to improved outcomes, including emotional/mental health if not physical outcomes.(Pennebaker, 1997a, 1997b) The quantitative data from the present study also suggest that the intervention’s opportunity to allow participants to express emotions was experienced as a positive one. We chose to report findings that were not statistically significant (which may be due to the sample size) because of their potential clinical importance if the findings are replicated in a subsequent, adequately-powered study. The potential decrease in anxiety post-videography is salient, as anxiety (state and trait) impacts pain intensity and other symptoms that often require medical management.(Tang & Gibson, 2005)
Offering children with life-shortening conditions the opportunity to a make a video to leave a legacy seems to be have been beneficial, and not harmful, especially regarding emotional state. For children who may have been hesitant to share some of these thoughts directly with their parents/caregivers, this videography intervention provided them an emotionally safe, controlled space in which to accomplish that task of dying. The expressions of gratitude to family members may be an example of utterances which might otherwise have been left unsaid, and would be beneficial for the patient to voice out loud, facilitating their grief work prior to their end of life (anticipatory mourning), and decreasing death anxiety (Lau & Cheng, 2011). For families, it also provided something tangible that families could watch and hear after their child had died. This video intervention thus facilitates accomplishing some of the tasks of dying described above.
This study has the following limitations. Participants were considered by their referring physician to be end stage; such gatekeeper bias may have limited the sample size, video duration, and content, as well as acceptability. Participation rates may also have been due to reluctance to be involved in the study because of health status at the time, desire to spend the time at end of life with family and friends instead, unwillingness to participate in another study, disinclination to discuss illness, and discomfort with being videotaped. Although the question stem on the pre-videography questionnaire was “Over the past week, I felt…” some patient participants may have responded based on immediate pre-video anxiety, and thus the decrease may not represent a decrease in overall anxiety, but in situational anxiety after the stressor had passed. While VHS video format is no longer common, the principal findings of this study may be transferable to phone-based video recording. Nevertheless, important conclusions can be drawn. Making a legacy video may assist children and adolescents with life-shortening conditions by providing a safe outlet for expressing their feelings to their parents and friends. Implementing a practice of legacy recordings in a pediatric palliative care setting would likely be feasible and accepted. Despite changes in availability and popularity of recording formats in which anyone can record themselves and widely share it through social media, hospital-based legacy video recordings are highly relevant. They give the child or adolescent greater control over when to share their content and with whom, compared to online sharing where content may be subsequently shared beyond the originator’s intent or control. They minimize the risk inherent in online social media interactions, including depressive symptoms, social isolation, and cyberbullying.(Best et al., 2014) Interventions initiated in hospital such as this provide greater structure and have emotional support available (e.g., psychology, chaplaincy, and child life) if the act of recording or viewing the video produces emotions difficult for the child or adolescent, or family, to manage themselves.
In the future, involving patients earlier in the trajectory of their condition (prior to being considered end stage) may both increase intervention uptake and allow patients and families to experience the beneficial effects. Further research is also needed to understand the relationship between making a legacy video and mood change. Specific attention to anxiety and the stability of any significant mood change would support further development and implementation of legacy video-making among pediatric patients with life-shortening conditions.
Footnotes
Acknowledgments
The authors gratefully acknowledge the children and parents who participated in this study, and the following staff: Kristine Allmendinger-Goertz, Matthew Brady, Rachel Jenkins, and Valerie Shaner.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the Summer Pediatric Research Scholars Program of the Rebecca D. Considine Research Institute, and the Haslinger Family Pediatric Palliative Care Center, Akron Children’s Hospital, Akron, Ohio.