
Abstract
Background
Death is an integral part of neonatal intensive care units’ (NICUs) environment and little it is known about NICU’s staff death concepts.
Aim
To investigate attitudes and experiences towards death of healthcare professionals (HPs) working in NICUs
Design
Totally 131 participants from six hospitals were included in the study. Research instruments were a questionnaire designed by the authors and the scale Death Attitude Profile-Revised.
Results
Gender, marital and educational status, frequent contact with end of life neonates and provision of neonatal end of life care during the research period correlated significantly with dimensions of DAP-R. Impact of NICU neonatal deaths on personal life correlated negatively with fear of death and positively with escape acceptance.
Conclusion
Evaluating the interrelationships among personal characteristics, attitudes and experiences towards death among NICU HPs may increase our understanding concerning working with dying neonates and provide direction for educational intervention and continuing professional support.
The neonatal period is the most crucial period for child survival. Neonates constitute a particularly vulnerable population group as they are often complicated by situations that lead to mortality. Although neonatal mortality is showing downward trends the last two decades, the global incidence is still 18% (Hug et al., 2019), demonstrating that neonatal death is an important issue for healthcare professionals (HPs), especially the ones working in the Neonatal Intensive Care Units (NICUs).
Death is an integral part of human life and NICU environment as well. The NICU staff faces neonatal death on a regular basis and is often thought to be unbreakable and expected to overcome unpleasant situations and proceed to other patients or duties, ignoring frequently the influence of a loss on professional and personal level. Beyond the family, the death of a hospitalized neonate has an undeniable emotional and psychopathological effect on the HPs who work directly with the neonate and its family (André et al., 2020; Camacho-Ávila et al., 2019; Kain, 2007). In previous studies, nurses have described neonatal loss as an enduring, agonizing and stressful experience that makes them undergo their own personal grief (Romesberg, 2004), while they refer to grief, loss and bereavement as major sources of stress in their work environment (Braithwaite, 2008). Professionalism prevails by the time a neonate relapses but emotions such as anxiety, discomfort and guilt usually emerge from a neonatal loss to HPs, as such incidence contradicts the concept of life’s ‘natural order’. The sense of failure is also significant as NICU HPs are expected to meet their social role as adults in which they are supposed to protect and save a child. This is a probable explanation why some NICU nurses have claimed that a neonatal death is less acceptable than the death of a critically ill adult or an elderly patient (Köktürk Dalcalı et al., 2020). As for emotional duress, NICU nurses are at high risk of developing secondary traumatic stress disorder (STSD) because they are regularly exposed to traumatic work-related stressors such as exposure to direct, indirect or threatened death (Favrod et al., 2018). This finding has been described also in other nursing specialties, such as emergency department, oncology, pediatric and hospice nurses (Beck, 2011). However, as far as we are aware, only the study of Favrod et al. has compared NICU nurses to another specialty. That study found higher percentages of STSD in NICU nurses than labor and delivery nurses (Favrod et al., 2018) but further comparative research focusing on specific subgroups of HPs employed in high mortality environments is needed.
Repeated exposure to patients’ death increases moreover the risk of severe anxiety, compassion fatigue, moral distress, burnout and bereavement overload (Bakan & Arli, 2018; Neimeyer & Holland, 2005) affecting potentially the quality of provided healthcare. Such factors have an influence on patient’s safety and are associated with patient injury, hospital-acquired infections, medication and health related errors, uncaring perception of the patients and unsuccessful attempt to rescue (Liu & Aungsuroch, 2018). Communication skills and support towards the bereaved family can be also influenced by HPs’ psychological and emotional issues.
An improved quality of end of life care for each dying neonate can make the final moments of life more soothing and create a warm and supportive relationship between the neonate’s family and the NICU team members. The path that initiates and endures this relationship is influenced by HPs’ attitudes to death and related experiences, perceptions and feelings (Ay & Oz, 2019). All these determine also the grief process, both for parents and HPs, which can affect many aspects of life, including physical, emotional, cognitive, behavioral and spiritual adjustments (Allie et al., 2018).
Although numerous sources of evidence are available to support NICU’s staff work-related stressors (Favrod et al., 2018; Fiske, 2018; Prentice et al., 2016), little it is known about NICU’s staff death concepts. Most of the studies are concentrated only on the experiences of HPs when caring for dying neonates and their families in the NICU (Almeida et al., 2016), end of life decisions (Huang et al., 2013; Samaan et al., 2008) and perceptions of neonatal end of life care (Kyc et al., 2020). Reviewing of the literature revealed studies that defined the HPs’ views and attitudes towards death (Ay & Oz, 2019; Puente-Fernández et al., 2020) but none, to our knowledge, considered solely HPs working in a NICU. Thus, this research issue was considered of great importance and elaborated the aim of our study, which was to investigate attitudes and experiences towards death of HPs working in NICUs and to assess if participants’ characteristics and experiences influenced their attitude towards death. Investigating relationships between attitudes and experiences towards death among NICU HPs may increase our understanding concerning working with dying neonates and provide direction for appropriate intervention and continuing professional support.
Materials and Methods
Study Design—Participants
This is a descriptive cross-sectional study conducted during the period February–June 2020. The study was approved by the Ethics Committees of all public hospitals that include a NICU in Athens, the capital of Greece. These six in total hospitals, are two childrens’ hospitals and four general and maternity hospitals. Three of them (two childrens’ and one university hospital), are referral hospitals as they support cases from all over Greece. All NICUs of the country follow a three-tier system at most. The 3rd level of the participated NICUs is consisted of 8–20 incubators, depending on the hospital. Each NICU involved in the study admits approximately 300–400 neonates per year.
Eligible participants were HPs who worked in a NICU, including doctors, midwives and nurses. According to the inclusion criteria the HPs should: (a) be able to read and write in Greek language in order to have the ability to complete the two questionnaires of the study, (b) work mainly in the 3rd level (intensive care unit) of a NICU, as at that level neonatal death is more common and (c) have at least six months of work experience in NICU (Diel et al., 2013; Mirlashari et al., 2016).
During the recruitment period, 157 HPs were eligible and were invited to take part in the study. Finally, 135 HPs accepted to participate and filled in the two questionnaires of the study (response rate 86%). The final study population consisted of 131 participants, as 4 were excluded from the study due to incomplete answers, and was used for the purpose of conducting analyses concerning experiences and attitudes towards death. Non-participation was mainly due to work overload and time constraints.
Procedure
After identifying the suitable hospitals for our study and obtaining Institutionals’ Review Board approvals, the research team contacted directly the leadership of each NICU in order to adequately explain the purpose and the nature of the study. Afterwards, each leadership team, during a scheduled session of the NICU, gave information about the study to the staff, prior to their enrollment, to help establish interest and willingness to serve as research subjects. Recruitment was consistent with all ethical considerations (promoting voluntariness, protecting privacy etc.) and sufficient time was given to all prospective participants to consider whether or not they are interested in proceeding to the consent process. There were no direct personal benefits of participation in this study.
Once HPs voluntarily agreed to participate, they were given an envelope containing the two questionnaires of the study and an informed consent form. The questionnaires were administered in person by the research team in order to: Avoid systematic errors due to postal handling Give more explanations to the participants when necessary Achieve mostly completeness and clarity of the answers
After completion, the questionnaires and the signed consent form were returned to the research team in a envelope closed in order to be anonymity and confidentiality of the data maintained. Coding of all participants was automatically created by the database used so as to preserve de-identification.
Research Instruments
The research instruments were two questionnaires. The first questionnaire was divided in two sections. The first section referred to demographic and occupational characteristics, including gender, age, marital and educational status, healthcare profession, previous experience in NICU and total working experience. The second section was consisted of 10 questions that investigated experiences related to: end of life care of neonates in the NICU education and death management discussions about end of life decisions and neonatal deaths coping strategies after neonatal death staff support groups within the hospital and death focusing on personal life
These questions were designed by the research team after thorough relevant literature review (Bouri et al., 2017; Göriş et al., 2017; Mazarakou, 2013; Zyga et al., 2015). All questions were close-ended and their types were: (a) polar (b) single-answer multiple choice (c) multiple-answer multiple choice and (d) Likert scale.
The second questionnaire was the 32-item scale Death Attitude Profile-Revised (DAP-R) introduced by Wong et al. (1994), which was used in order to measure respondents’ attitudes towards death. The five dimensions that constitute DAP-R and their implications are: Fear of death (7 items) – negative thoughts and feelings about the state of death and process of dying Death avoidance (5 items) – avoidance of thinking or talking about death in order to reduce death anxiety Neutral acceptance (5 items) - view of death as a reality that is neither to be feared nor welcomed Approach acceptance (10 items) - view of death as a gateway to a happy afterlife Escape acceptance (5 items) - view of death as escape from a painful existence
Scores for all items are based on a 7-point Likert scale in the direction of strongly disagree (1) to strongly agree (7) and the possible score ranges from 32 to 224. For each DAP-R dimension, a mean scale score can be calculated by dividing the total scale score by the number of items comprising each scale. Higher scores in a dimension indicate a higher inclination to it (Wong et al., 1994).
The DAP-R has been translated in Greek language and validated in the Greek population by Malliarou et al. (2011a), with acceptable reliability.
Statistical Analysis
Quantitative variables were expressed as mean (Standard Deviation) and qualitative variables were expressed as absolute and relative frequencies. Multiple linear regression analysis was used with dependent the dimensions of DAP-R. The regression equation included terms for gender, age, marital status, education, healthcare profession, professional experience, frequency of care related to end of life neonates, education related to patients'/neonates’ death management, providing currently neonatal end of life care, colleague conversation about neonatal deaths, impact of NICU neonatal deaths on healthcare professionals’ personal life and personal death experience. Adjusted regression coefficients (β) with standard errors (SE) were computed from the results of the linear regression analysis. Diagnostics for regression models were performed to check if the conditions for regression had been met with the residuals of each model being normally distributed and their variance being constant. Multicollinearity was assessed via variance inflation factor (VIF) and indicated no presence of multicollinearity. All reported p values are two-tailed. Statistical significance was set at p < (⩽0.05) and analysis was conducted using SPSS statistical software (version 22.0).
Results
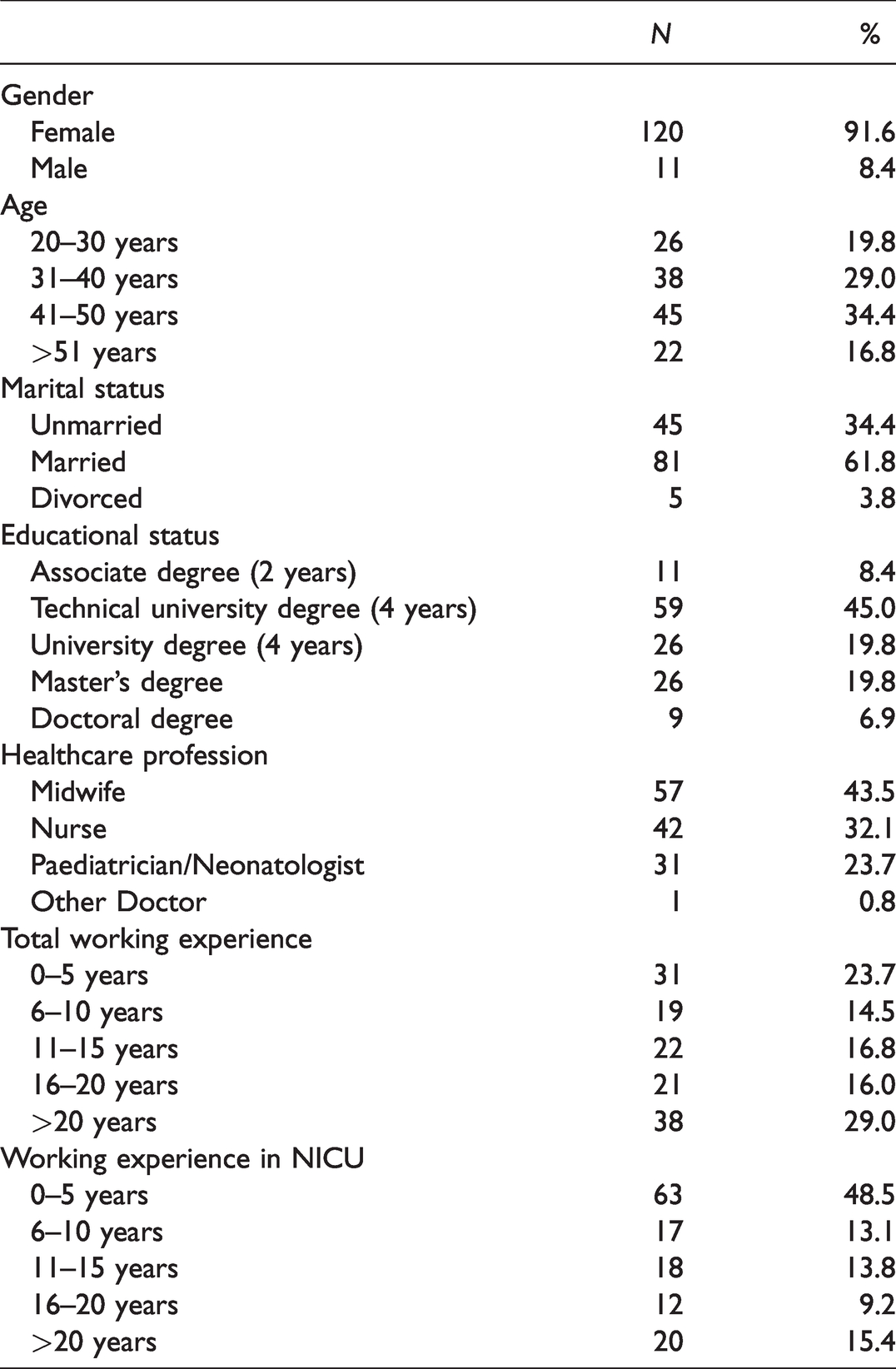
The study included 131 HPs, most of whom were women (91.6%). The majority of the participants (34.4%) were between 41–50 years old and the 61.8% were married. Besides, the 45.0% of the participants had acquired a technical university degree (4 years) and the 43.5% were midwives. Finally, the 29.0% of the participants had at least 20 years of total working experience and the 48.5% had no more than 5 years of working experience in a NICU. Participants’ characteristics are presented extensively in Table 1.
Participants’ Characteristics.
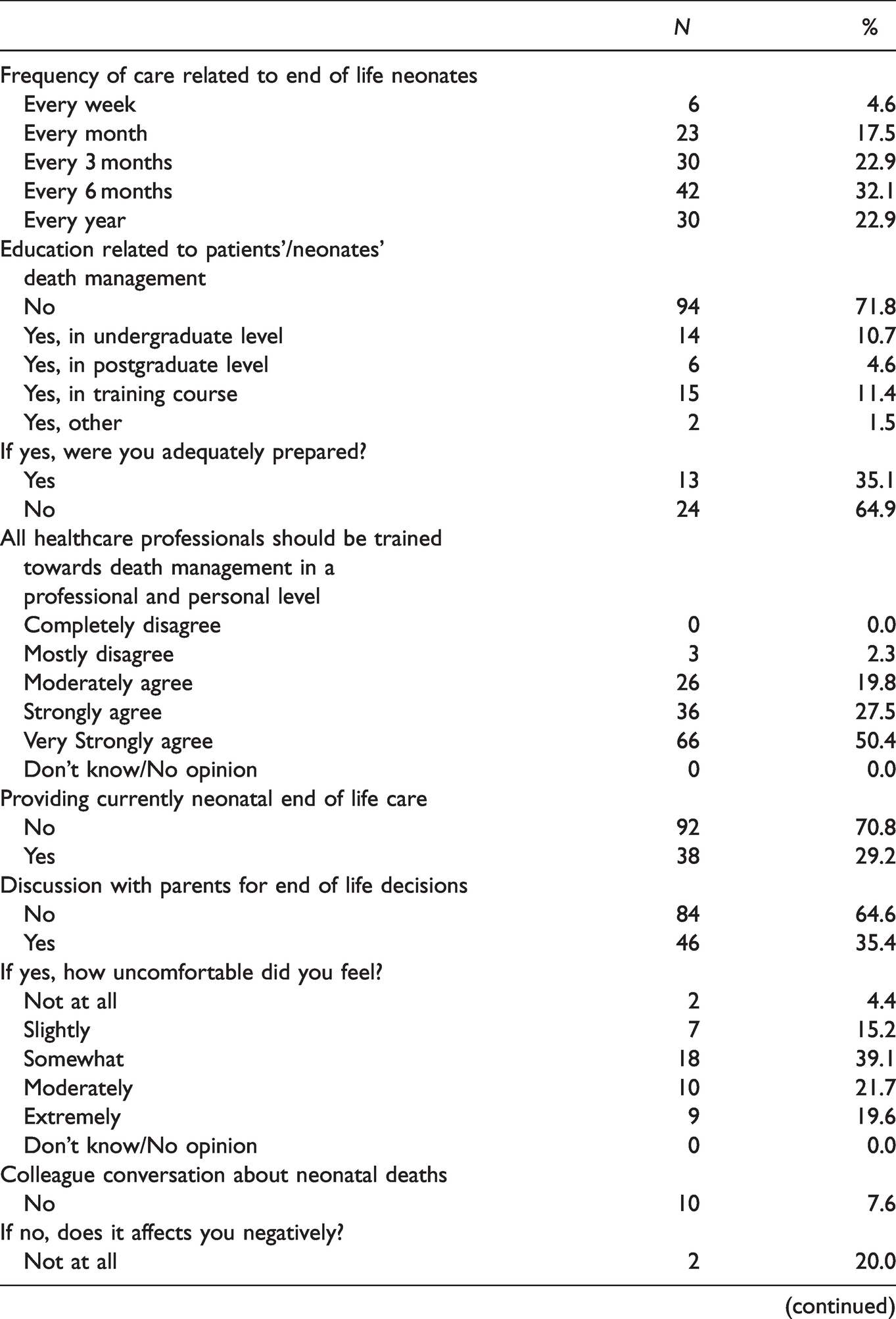
Regarding experiences towards death, the 32.1% of the participants answered that they provide neonatal end of life care every 6 months. Most of the participants had no prior training towards death management either in a professional or personal level, with the percentage being 71.8%. Of those who were trained, the 35.1% thought to be adequately prepared. Almost half of the participants (50.4%) agreed very strongly with the statement that ‘all healthcare professionals should be trained towards death management in a professional and personal level’. Additionally, the 29.2% of the participants were providing currently neonatal end of life care and the 35.4% had discussed in the past with parents for end of life decisions. Moreover, the 92.4% of the participants used to make conversations with colleagues about the occurrence of neonatal deaths in NICU and the 73.6% of them felt more relieved after that. Among participants, the most frequent strategy for coping with feelings after neonatal death in NICU was sharing thoughts and emotions with their loved ones. None of the hospitals that participants worked, had availability of staff support group for HPs. Lastly, the 86.3% of the participants had experienced loss among their friends or family. Information concerning participants’ experiences towards death is presented broadly in Table 2.
Participants’ Experiences Towards Death.
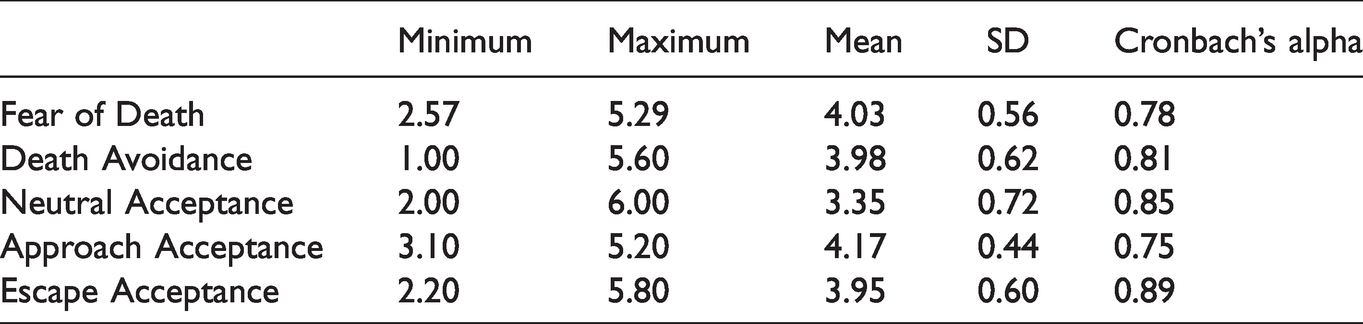
The range in all DAP-R dimensions as well as their mean and standard deviation are presented in Table 3. When multiple linear regression analysis was conducted with DAP-R dimensions as dependent variables, it was found that greater ‘frequency of care related to end of life neonates’ and lower ‘impact of NICU neonatal deaths on personal life’ were significantly associated with greater fear of death. Male HPs had significantly lower score in the dimension of death avoidance, indicating less death avoidance, compared to women. Furthermore, participants who were providing neonatal end of life care during the recruitment period, had significantly greater death avoidance while the higher educational status was associated with lower death avoidance. Males and married participants had significantly lower score in the dimension of approach acceptance, indicating lower acceptance of death. The dimensions neutral acceptance was not associated significantly with any of the studied characteristics and experiences. At last, greater ‘impact of NICU neonatal deaths on personal life’ was found to be positively associated with greater scores on escape acceptance dimension. Results of DAP-R are shown in Table 4.
Descriptive Measures of DAP-R Dimensions.
Multiple Linear Regression Analyses Results With DAP-R Dimensions as Dependent Variables.
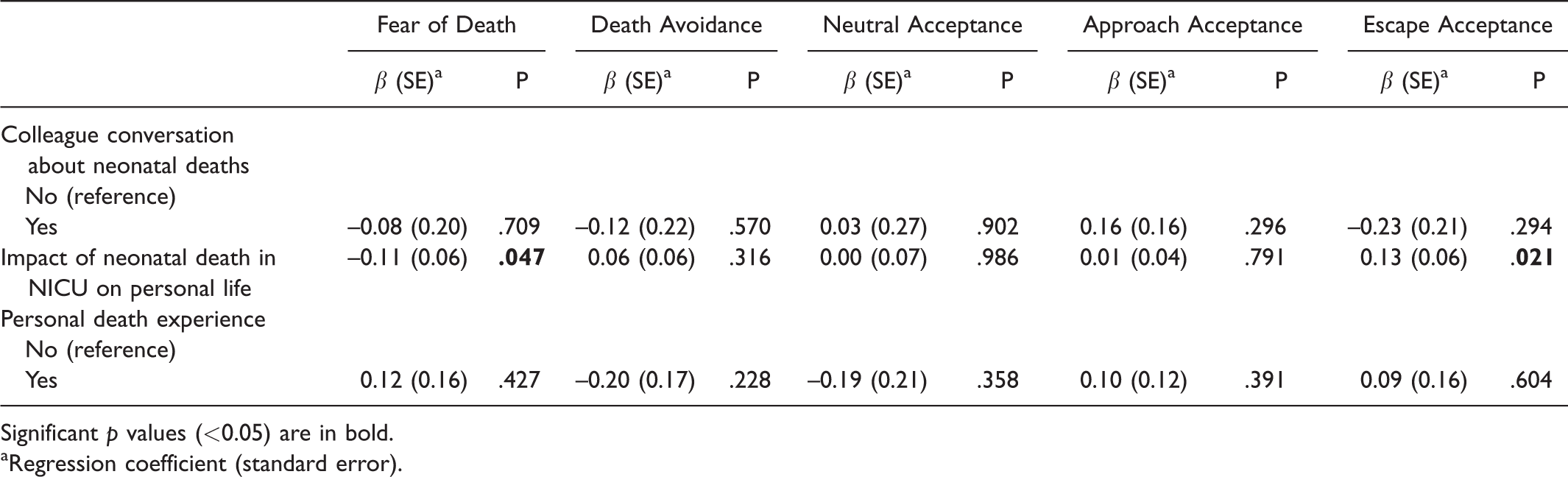
Significant p values (<0.05) are in bold.
aRegression coefficient (standard error).
Discussion
The present study investigated for the first time attitudes and experiences towards death of HPs working in NICUs, especially in the 3rd level (intensive care unit).
The results of the current study showed that men HPs avoided less thoughts and conversations about death in order to reduce death anxiety (death avoidance) in contrast to women, a finding that is consistent with the study by Asadpour et al. (2016) which was conducted on a sample of medical students, but disagrees with Malliarou et al. (2011b) who studied Greek nurses that provided palliative care to adults. Also, our study supports that men HPs believed less in the existence of a happy afterlife (approach acceptance), which is in accordance with other studies (Gama et al., 2012; Zdziarski et al., 2020) but contradicts the findings of Malliarou et al. (2011b), where men showed greater faith in a happy afterlife. It may be assumed that men in our study were probably under the influence of social stereotypes that want them strong and invulnerable in adversities, pushing them in a way to discuss death issues more comfortably. Specifically in the case of a neonatal death, women seem to be affected more on a personal level due to their female nature (motherhood) and ultimately avoid thoughts and discussions about death. In previous studies (Abu Hasheesh et al., 2013; Asadpour et al., 2015, 2016; Malliarou et al., 2011b) a significant correlation between gender and fear of death was found, finding that was not demonstrated in our study, perhaps because of the small sample of men HPs.
Regarding the marital status of the participants, it was found that married HPs had a negative correlation with approach acceptance, but Asadpour et al. (2016) correlated negatively the married HPs with escape acceptance. Married people appear to have a negative trend towards death possibly due to family attachment and inclusion of a spouse, children or dependents in the family. In Greece, marriage usually takes place between the thirties and forties, age which is often associated with unresolved experience of past deaths, loss of a beloved one or unfulfilled life goals.
As far as educational status is concerned, our study found a significant negative correlation with death avoidance suggesting that the higher the educational level of HPs the less they avoided thoughts and discussions about death. Our finding, in line with Zyga et al. (2015), implies that more advanced education may be a responsible factor for positive attitudes towards death since it increases awareness and professional competency in the care of dying patients. Besides, it attains specialized knowledge, psychosocial skills and sensitivity to social differences leading in a more philosophical and scientific approach of death.
Furthermore, when contact with end of life neonates was more frequent, that led HPs to an increased fear of death. Contrarily, the HPs who came more often in contact with adult patients at the end of life, reported an indecisive attitude (neither agree/nor disagree) in the study of Mazarakou (2013) and such frequent contact was negatively correlated with death avoidance in the study of Braun et al. (2010). The result of our study points to the likelihood that accompanying more often a neonate during the process of dying might be a reason for reflection on the death of a beloved one or a perinatal loss, facts whose memories increase death anxiety. Additionally, most of the participants in our study had short length of experience in a NICU and thus, could find very hard and distressing to cope with neonatal death.
In several studies (Black, 2007; Bouri et al., 2017; Dunn et al., 2005), age and total working experience were significantly correlated with the dimensions of DAP-R, whereas in our study such correlations were not found, possibly beacause of the small sample of participants.
It is worth mentioning that in our study the impact of NICU neonatal deaths on personal life correlated negatively with fear of death and positively with escape acceptance. We hypothesize that HPs in our study, stated a low ‘impact of NICU neonatal deaths on personal life’ while they faced unconscious fear of death which was however recorded in their answers of the DAP-R questionnaire. Even though most of the participants talked with colleagues about neonatal deaths and reported to share thoughts and emotions with their loved ones as a coping strategy, it cannot be ruled out that in their personal life they did not allow a free flow of emotions and predisposed withdrawal into a more inward, self-protective and self-nurturing behavior pattern. The tendency for fear of death to increase with smaller impact of neonatal death on personal life, in our opinion means that people become increasingly defensive and try to maintain a certain psychological distance from the death of the neonate as a coping mechanism. Furthermore, the positive correlation with escape acceptance, indicates that HPs believed that the death of the neonate was an alternative to a miserable life, thoughts that are consistent with irreversible medical conditions, pain and suffering. Nevertheless, it must be argued that the interrelationships between attitudes and experiences towards death should not be interpreted as causal and directional of the results of our study; these variables partially influence and interact with each other.
Providing a high quality neonatal end of life care, requires an inner commitment from the HPs who are involved, which is associated with how they view death and the dying neonates but also with death education. In the present study, it was demonstrated that the majority of HPs had no prior training towards death management, either in a professional or personal level, and those who were trained believed that courses were inadequate. Death education helps HPs to become familiar with death, adopt a professional attitude, develop communication and empathy skills, acquire confidence and competence in death management and besides, teaches HPs how to cope positively with grief (Dodd et al., 2020; Gocmen Baykara et al., 2020). That is probably why half of the participants (50.4%) agreed very strongly that all HPs should be trained towards death management in a professional and personal level. Interventional educational programs with didactic and experiential methods of teaching, although still under research, have been found to be effective on altering attitudes of HPs towards death, usually from negative to positive, as well as improving knowledge, confidence, symptom management, pain assessment, communication skills and breaking bad news. Such programs have been applied somehow to HPs working with pediatric, oncology or critically ill adult patients (Balicas, 2018; Bouri et al., 2017; Göriş et al., 2017) but very few refer to HPs who confront neonatal loss (Hammond et al., 2020; Knighting et al., 2019). Therefore, it is considered crucial the presence of certain educational courses in relevant faculties, such as medicine and health and care sciences, as well as the development of continuing educational programs within hospitals, in order for HPs to become able to offer a holistic care and improve quality of the health services in the terminal stage of a patient’s life, no matter the age. Appropriate death education however, is considered essential also for HPs’ well-being, as it can provide deep knowledge of potential interventions that facilitate adjustment to deaths of patients (Redinbaugh et al., 2001).
Although all hospitals in Greece employ at least one psychologist, a significant weakness of the National Health System was highlighted by our study. None of the hospitals involved in our study, organised staff support groups for HPs within the hospital. This issue should be probably addressed to each hospital’s administration, as supervised staff support groups have been found to be beneficial regarding intensive work-related stress, compassion fatigue, cognitive behavioral approaches, emotional management, coping strategies, communication skills and interdisciplinary cooperation (Deodhar & Goswami, 2017; Wenzel et al., 2011).
Our study, moreover, had some strengths and some limitations. Although not cost-effective, the fact that the questionnaires were administered in person by the research team and its members were available for explanations and clarifications, increases the reliability and therefore the strength of our survey. Additional strengths were the high response rate (86%) and that participants came from all the public tertiary level institutions that included a NICU in Athens, not just one, indicating a more representative sample. However, the sample was small and drawn from a single big city; thus, the generalization of the findings in all NICU HPs is restricted. It is also acknowledged that findings of the current research are limited only to the Greek context, although not a lack of the research design. Cultural, philosophical and religious frameworks as well as indicators of mental health were not taken into account, indicating main constraints of our study. The significant low percentage (8.4%) of men participants, was also an extra weakness of the study, but NICU staff is mainly consisted of women HPs all over the country. Despite of these limitations, our study suggests some possible directions for future research. Future studies may investigate additional correlations between NICU HPs’ death attitudes and other factors determining them, such as cultural frameworks, mental health disorders and attitudes towards care of the dying. Furthermore, future studies with larger samples from various countries and cultures, could investigate whether there are differences in death attitudes between NICU HPs and other occupational groups that are highly subjected to patients’ death.
Finally, taking into account results of previous studies and ours as well, specific demographic and professional characteristics together with experiences around death, have a strong relationship with the formation of attitudes, perceptions and feelings about death of HPs. This fact can affect the HPs’ mental health, the provided end of life care to patients of all ages and the effective management of the patients’ family during bereavement period. Therefore, implementation of training and consulting services with reflection on the topic of death and coping strategies of professional stress regarding exposure to death and dying, should become an integrated part of undergraduate, postgraduate and continuing educational programs so as to be applied efficiently in every day clinical practice and form to HP’s positive attitudes towards death.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.