
Abstract
Based on an ethnographic and mixed-methods research design, the article explores the social and interactive processes of disenfranchisement of perinatal grief through the mechanisms of silence, silencing and self-censorship in encounters between bereaved women and the social milieu. The analysis finds that disenfranchisement results from the constriction of the social space of bereavement along various lines of discourse, cultural values, practice and materiality, that include: the passing of time (expectations of a quick ‘recovery’); competing discourses of loss (simplistic-dominant vs. complex-subordinate meaning-making); the biometrics of pregnancy (lower gestational age being equated with less intense grief); gendered ideas of reproduction and feeling rules; asymmetries in social power; social spheres (hospital, home, community, support groups); socio-materialities and performance/ritual; and structural aspects of social and familial organization (gender, age, intergenerational and kin v. non-kin relations). These processes are intimately linked to the complication of grief by undermining support, meaning-making and continuing bonds.
Keywords
Perinatal grief relates to the experience of loss following the death of a baby at anytime during pregnancy (miscarriage, stillbirth, termination of pregnancy for medical reasons) or in the neonatal period. Research finds that a significant proportion of women, and to a lesser degree men, suffer from complicated grief, post-traumatic stress, and other forms of morbidity following this type of death (Gold et al., 2016; Kersting et al., 2005). This is likely because it often involves the trauma typical of a sudden and unexpected death, low levels of social support, difficulty finding meaning, and is often experienced as the death of a child; all of which are factors that increase risk of complicated grief (Burke & Neimeyer, 2013; Lobb et al., 2010).
Disenfranchised grief pertains to a conflict or tension between a bereaved persons sense of entitlement to grieve and the denial of the opportunity or right to grieve publicly (Doka, 1989). The basic premise being that the social institutions and the milieu regulate grief through cultural norms and grieving rules (Doka, 1989; Fowlkes, 1990). One of the principal ways that disenfranchisement is evident in Western societies is the prioritization of kin-based relations over extra-familial attachments (Doka, 1989; Fowlkes, 1990). From this perspective, cultural values related to family and social roles pre-determine perceptions of grief intensity and the need for support. Other forms of disenfranchisement relate to a lack of recognition of grief or where stigma and questions of morality affect the social status of the relationship, the bereaved, or the deceased, such as might happen in the case of murder, suicide, addiction, etc. (Pine, 1989; Riches & Dawson, 1998b; Valentine et al., 2016).
While Robson and Walter (2013) argue that disenfranchisement works in hierarchies related to social roles, they also observed their study participants reordered the priority assigned to grievers when given contextual information, including promoting non-kin above family members. This suggests a local, relational and negotiated aspect to disenfranchisement that operates within the broad cultural values of death and dying (Averill & Nunley, 1988; Hochschild, 1979). This is consistent with knowledge about the way grief is mediated (and also varies) by family members and close social networks (Dyregrov & Dyregrov, 2008; Nadeau, 2001; Rosenblatt, 1993). These ideas are also congruent with general micro-sociological and interaction theory (Garfinkel, 1967), which holds that social meaning is established during interaction and is therefore in a constant reflexive process of negotiation, revision, and adaptation.
Conceptually, perinatal grief was believed to be disenfranchised on the basis that the relationship wasn’t recognized (Nichols, 1989). However, this understanding is somewhat problematic or simplistic in Western Christian societies. Stillborn babies and those that died before baptism were heavily stigmatized within Christian orthodoxy since at least the fifth century . A situation that persisted in religious and healthcare institutions until the late twentieth century (Cosgrove, 2004; O’Leary & Warland, 2013), if not longer in many locations. In this respect, when perinatal grief is described as silenced or taboo (Layne, 2003; Lewis, 1976) it is also due to active processes of stigma-based disenfranchisement at structural or local level. The fact that a significant percentage of women experience guilt, shame and self-blame following perinatal loss (Gold et al., 2017) points to the impact that stigma still has on bereavement and spoiled maternal identity (Murphy, 2012). On this basis, the disenfranchisement of perinatal grief should be considered an unrecognized, undervalued and stigmatized form of loss that works on the relationship between the bereaved and the deceased, as well as individually on the object and subject of grief.
This research takes place in the context of Spain, where perinatal bereavement has only recently entered the institutional consciousness and healthcare practices are underdeveloped compared to other high-income countries (Cassidy, 2018). The objective of this paper, however, is to consider three broad questions: To what extent is perinatal grief disenfranchised and what form does this take? What are the norms and rules that govern the regulation of grief and, how, in an active sense, are these applied in order to establish who can and cannot grieve publically? And, finally, how does disenfranchisement impact bereavement?
Within the fields of sociology and interactionism, the concepts of silence, silencing or self-censorship provide a useful way to examine social processes around stigma and the delegitimization of grief. At broad socio-cultural and historical levels silence can be considered in terms of the other side of what it is possible to say at certain times, in specific social spaces, and by whom (Foucault, 1978). Metaphorically, it can also be understood in a material sense of absence, such as a lack of presence or existence (Jaworski, 1997). Interactively, it may be both discrete and manipulative, such as an avoidance of a sensitive or taboo topic, refusing to name a social object, or a question left unanswered (Huckin, 2002; Jaworski, 1997). While silence is ambiguous due to its lack of specificity, silencing represents more explicit attempts to limit, remove or delegitimize particular forms of thought through strategies such as deflecting, minimizing, and reformulating, amongst others (Coupland & Coupland, 1997; Thiesmeyer, 2003).
With a few exceptions the actual dynamics of silence in the context of perinatal grief have received little attention. While Layne (2003, pp. 59–80, 235–250) treats it broadly throughout her book, it is mostly considered from a structural perspective related to broad classificatory and divisory systems, lack of scholarly attention, and conflict with reproductive rights (Hazen, 2006; Miller, 2015). This article looks more specifically at the interactive dynamics of silence and silencing and has a number of implications for understanding the social processes that delegitimize grief following perinatal loss and how this can complicate bereavement.
Materials and Methods
The study employed a critical ethnographic methodology and mixed-methods design (Thomas, 1993) that included observation of an online support forum, an anonymous non-probabilistic online survey (closed-end and open-ended questions) and narrative style interviews. This epistemological approach views all phenomena as physically, socio-culturally and historically contextual and all scientific observations as inseparable from the observer (Barad, 2007, pp. 139–140). Within the mixed-methods approach proposed by pragmatic, new-materialist and feminist epistemologies, the focus shifts from collecting ‘data’ to developing evidence that helps address or elucidate a particular research problem, rather than the presentation of data for its own sake. At another level, the purpose of triangulation goes beyond validation to create dialogue between data at all stages of the research, including design (theory, instrument), analysis (convergence and divergence) and reporting (Creswell, 2009; Fox & Alldred, 2015; Oakley, 1998).
The study population was differentiated to each methodology: the qualitative sampling focused on all pregnancy losses (stillbirths or pregnancy terminations) and neonatal deaths, while the survey addressed only intrauterine and intrapartum deaths from 16 weeks onwards, including pregnancy terminations for medical reasons.
Qualitative Methods
Ten narrative style interviews were conducted with three heterosexual couples and seven women in heterosexual relationships. The interview sampling followed a purposive procedure that attempted to ensure an even distribution of participants across gestational ages, type of death, socio-economic status and nationality, although the final sample is skewed toward the university educated and Spanish nationals. Three interviews were arranged through a support association, one following an encounter at a memorial event for parents, and six following expressions of interest in further research following participation in the survey. The interviews lasted from two to three-and-a-half hours and were transcribed verbatim. The asynchronous online mutual support forum was a publically accessible space. The forum administrators were approached about participating in the project and agreed on the basis of ensuring the anonymity of forum members. To capture users engaged in dialogue and to exclude moderators, the initial sample frame was restricted to the 450 members that had made between five and thirty entries. The final sample of 22 members was drawn using the SPSS random number function. The sample features more first and second trimester losses than were gathered in the interviews and survey. The qualitative data from the survey related to a series of open-ended questions that focused on the ‘least’ and ‘most’ helpful aspects of experiences during care in the hospital, as well as questions on post mortem contact with the baby (or lack of), and the disposition of the body. From a total of 796 responses to the survey, 622 participants provided at least some answers to the open-ended questions, of which 52 were selected for analysis based on a preliminary content and thematic analysis. Table 1 provides details of the samples according to the three sources of qualitative data. All bar one of the participants (a forum member) had experienced their loss in the Spanish national health system.
Trimester and Type of Loss: Participants Included in the Qualitative Data Analysis.
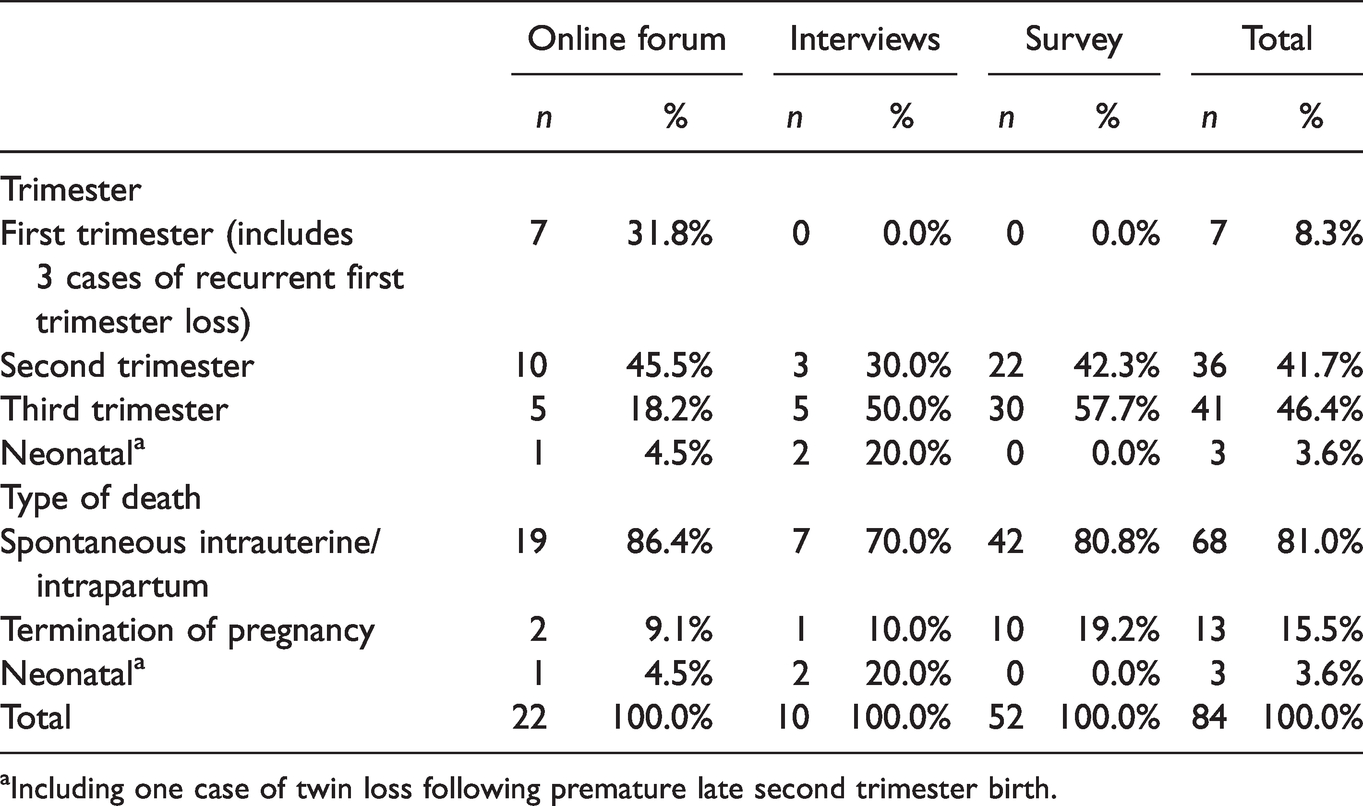
aIncluding one case of twin loss following premature late second trimester birth.
The qualitative analysis used a narrative, linguistic and discursive approach (De Fina & Georgakopoulou, 2015; Potter & Wetherell, 1994) that examines grammar, form and narrative structure. This approach assumes that the narratives will contain at the very least the story of an event or complicating action, and in many cases, an orientation, evaluation and resolution (Mishler, 1986, p. 78). Collectively, the analysis permits the study of how meaning and positions are constructed and negotiated during social interactions (Garfinkel, 1967), as well as taking into consideration the context of production, broader cultural discourses, and historical situatedness.
Quantitative Methods
The anonymous online survey contained just over 100 questions and addressed a number of research objectives beyond the issues presented in this article. The survey was carried out over a three-year period between 2013 and 2016 using a snowball recruitment method through support association mailing lists, social media, and press releases. In total, 796 interviews were completed with women who had lost their baby in the five years prior to participating. Like the qualitative interviews, the sample was biased towards Spanish nationals and women with university level educations, although a sizeable subgroup of women with lower educational attainment was recruited. Further details and information on the sample and abandonment rates is presented in the supplementary material. Apart from the open-ended questions, the data collected and presented in this paper relates to the prevalence of healthcare practices (levels of postmortem contact and memory-making), terminology used to refer to the object of loss (the baby), women’s subjective rating of emotional support and information provision (using a 5-point Likert agreement scale), and rating of support received from members of their social network (partner, close family, extended family, close friends, extended friends and work colleagues), using a four-point scale: none, a little, some, a lot.
Ethics approval for non-clinical trials was not required by the author’s institution (University Complutense Madrid) and could not be provided. However, by working with mental health professionals and parent support associations, a comprehensive ethics and participant safety plan was put in place prior to conducting fieldwork. In the case of the survey, information was provided on the introductory page of the questionnaire and qualitative interviewees gave consent firstly through email and then by signed consent before commencement of the interview. Information on psychological support was provided to all participants as well as follow up contact to check on wellbeing. The anonymity of participants has been ensured through the use of pseudonyms and removal of any identifying data.
The quotations presented in the text were translated by the author, a native English speaker and experienced Spanish to English translator. Further details of the samples, study design, questionnaire, ethics plan, and the qualitative analytic procedure are provided in the supplementary material.
Results
The results are structured in three sections. To start, some general findings in relation to social support are presented. This is followed by two sections that address how processes of silence/silencing and self-censorship make poor support and stigma manifest at an interactive level during encounters with members of the social milieu (healthcare professionals, family, friends, work colleagues etc.).
Overall Evaluation of Social Support
The analysis of the survey question on social support (Table 2) found that overall only 37.9% of participants received a ‘high’ level of support (a lot) across five main sources (partner, close family, close friends, extended family, and extended friends), while nearly one-in-five women received ‘low’ support (none or little). Partners provided the greatest level of support: 95.2% were rated as giving ‘some’ or ‘a lot’ of support. In contrast, extended family and friends and work colleagues were rated the lowest. For most sources of support, the analysis found significant differences between second and third trimester losses, but with small effect sizes.
Sources and Ratings of Support in the Close and Extended Social Network According to Gestational Age (n = 796).
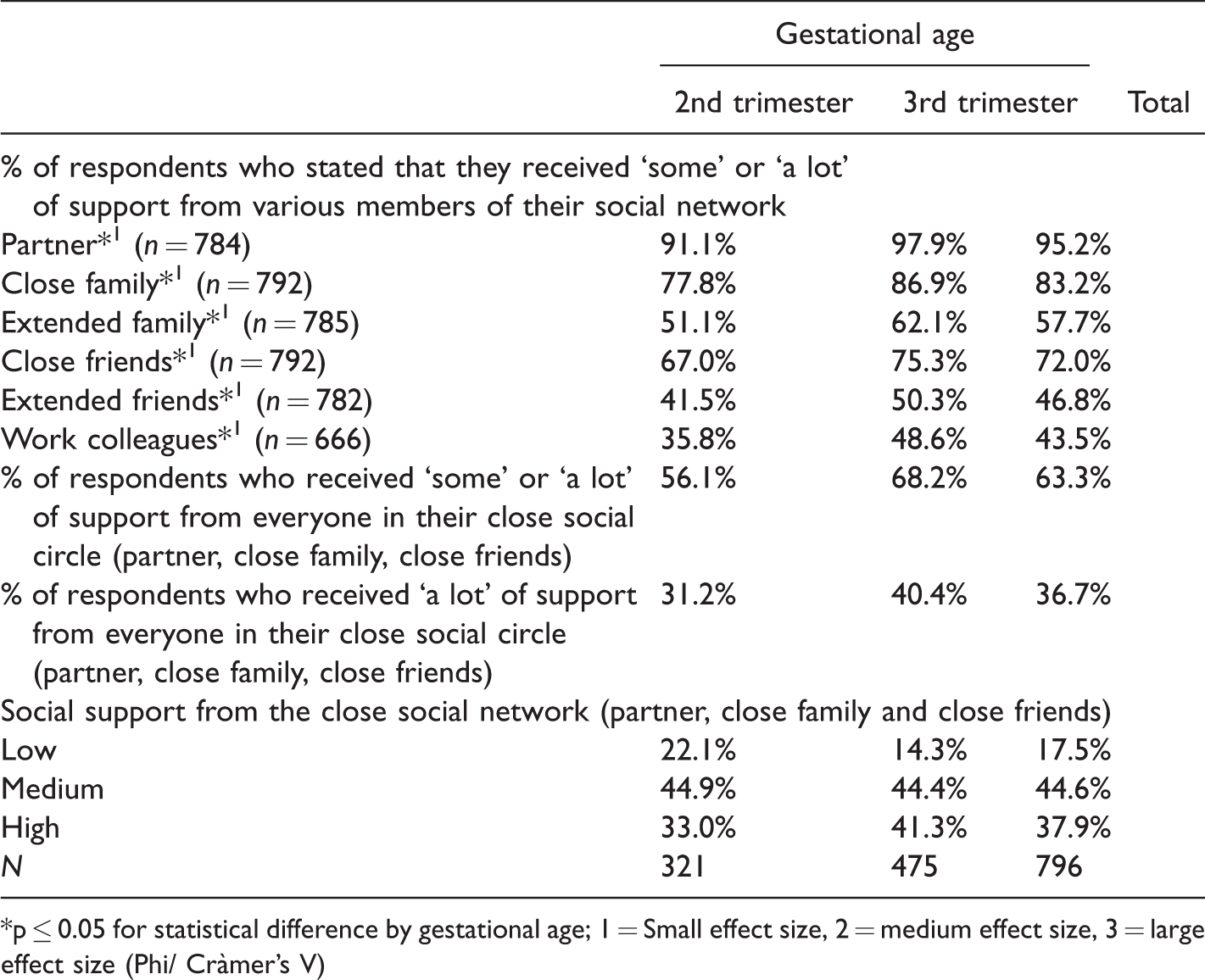
*p ≤ 0.05 for statistical difference by gestational age; 1 = Small effect size, 2 = medium effect size, 3 = large effect size (Phi/ Cràmer’s V)
Silence, Silencing and Absence
The analysis found five main interactive mechanism of silence, silencing and absence: i) medical framing of loss through exclusion of emotion and repositioning of the object and subject of grief; ii) absence of knowledge and control over decision-making; iii) material and performative absences; iv) silence in the home and community; and v) silencing through conflicting meaning-making.
Medical Framing of Loss, Exclusion of Emotion and Repositioning of the Object and Subject of Loss
A major theme of the narratives is how lack of empathy in care provision is synonymous with an exclusive focus on the body and physical interventions that frame perinatal death as a ‘medical’ issue, leaving little social space for loss, grief and “emotional pain”: […] the protocol dehumanizes everything: putting in a drip, admitting me and leaving me alone with someone else I was so scared of giving birth to my dead girl … the rushing. all of a sudden they all want to do something quickly and at that stage there isn’t anything, right? … they called her dead fetus … […] we felt abandoned in a room until we asked for the epidural it was like: now we can do something… they felt very uncomfortable with my emotional pain
(Extract 1. Ana María, third trimester stillbirth, survey respondent)
However, the inappropriateness of (negative) emotion displays often has to be established through interaction. Camino recalled how the female doctor responded to her crying when she received the news that her baby had died. By minimizing her response through infantilizing and gender-based positioning, the doctor delegitimizes her reaction as exaggerated and rejects Camino’s implicit request for support: when we got the news, when I started crying the [female
1
] doctor said “well child, it’s not that bad” […]
(Extract 2. Camino, second trimester stillbirth, survey respondent)
These mechanisms of silence and silencing make it possible to understand why around one-third of women who responded to the survey ‘disagreed’ that they received ‘emotional’ support during the hospital stay (see Table 3). Importantly though, the analysis also shows that emotional support varied along two important lines: doctors (male or female) were less likely to be supportive than nurses/midwives (55.9% supportive vs. 71.4%) and second trimester losses received significantly less support overall (p < .001).
Results Related to Processes of Care According to Gestational Age (n = 796).
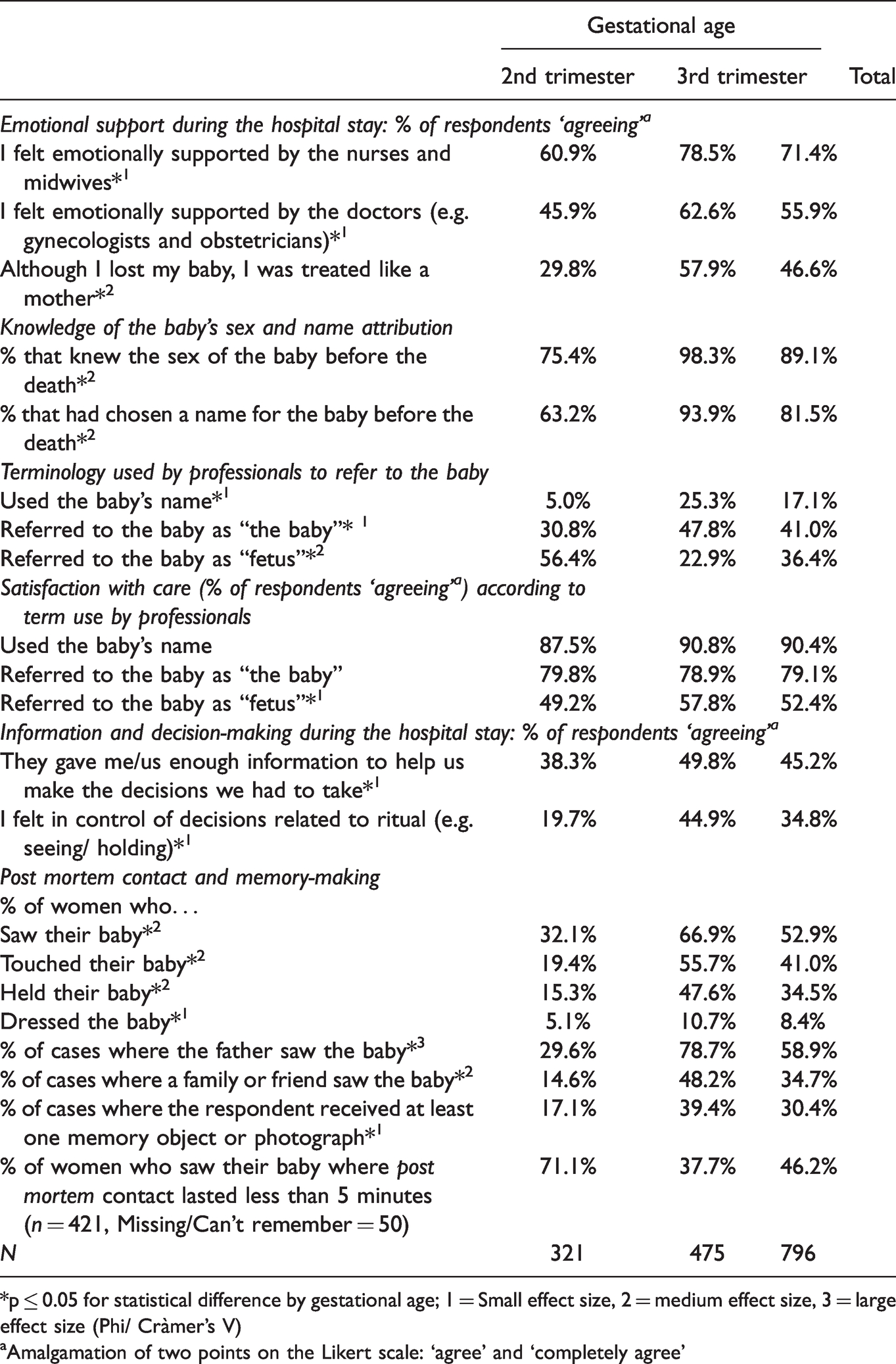
*p ≤ 0.05 for statistical difference by gestational age; 1 = Small effect size, 2 = medium effect size, 3 = large effect size (Phi/ Cràmer’s V)
aAmalgamation of two points on the Likert scale: ‘agree’ and ‘completely agree’
Silence and silencing also relates to the object of grief. The analysis found that the terms used by health professionals to refer to babies are strong indicators of sintony (loss-oriented frames) or dissonance (medical frame) in health professional-patient encounters, as we have already seen in extract 1, above. Although the survey research found that over 90% of participants knew the sex of the baby before it was born and over 80% had chosen a name, use of the baby’s name by health professionals was very rare: only one-in-four cases in the third trimester and one-in-twenty in second-trimester deaths. Use of ‘baby’ was far more common (41.0% of all cases), followed by ‘fetus’: 56.4% in the second-trimester and 22.9% in third-trimester losses (see Table 3). In this respect, it is interesting to conisder Leticia’s account of a particularly conflictive interaction with a public health psychiatrist who attempted to deny the possibility of a relationship with a baby during pregnancy by associating the term “fetus” as meaning non-person/child, and therefore deconstructing her identity as a “mother”: She said, no, it wasn’t true, that I hadn’t lived with her, that to live with a person they have to be out [of the womb] and that you have to act as a mother and the child as a child, […] and this woman wouldn’t stop saying: “it’s a fetus, a fetus, a fetus”
(Extract 3. Leticia, third trimester stillbirth, interview)
The impact of term use is evident in its association with ratings of care: when at least one health professional used the term ‘fetus’ satisfaction with care was almost half that when health professionals used the baby’s name (see Table 3). The analysis also found that positive emotional support (two-in-three cases) didn’t necessarily extend to name use and an unequivocal recognition of the personhood of the baby. In fact, terms such as ‘baby’ appear to represent a form of ‘hedging’, which avoids full enfranchisement. This can help explain why nearly half of women (46.6%) responded that they didn’t feel like they were treated as ‘mothers’ during the hospital stay (Table 3). Hence, not naming can be understood as both silence and silencing, be it the use of ‘fetus’ or the absence of the use of a name, when one exists.
Absence of Information and Knowledge
It is evident from a number of the quotations included in this article that a common theme in the narratives is that many women found themselves at a significant discursive disadvantage in terms of being able to evaluate what constituted good and bad care. Often this only became apparent afterwards. The survey results underscore the extent of this problem as only half of women ‘agreed’ that they received ‘enough information’ to help them make decisions in the hospital. Ultimately, this translates into lack of autonomy and disenfranchisement from the processes and story of care whereby less than half of women ‘agreed’ that they felt in control of decisions related to ritual and care of the body (see Table 3). However, it is also important that less than one-in-five women rated information received on the ‘process of grief’ as ‘some’ or ‘a lot’. This highlights how, even in hospitals where care was empathetic and good information was provided, grief and loss are rarely addressed in any direct terms.
Material and Performative Absences
Material and performative absences are evident at various levels in the data, in particular the possibilities of rituals related to seeing and holding the baby: just over half of mothers (52.9%) and fathers (58.9%) and only one-third of family members saw the baby after the birth, although this varied significantly between trimesters (p < .01). Acts such as touching (41.0%), holding (34.5%), and dressing (8.4%) the baby were absent for the majority of women. Most parents left the hospitals with no material trace of the baby or photographs (see Table 3). These outcomes are largely reflective of lack of opportunity and asymmetric decision-making processes.
However, even when parents did see their children these events could be better described as ‘viewings’ than practices focused on loss and grief. In just over 40% of cases women spent less than five minutes with the baby (see Table 3) and in many instances there was an absence of symbolic materials and acts related to normative expectations of how a person or “baby” should be treated in death: she was naked and they hadn’t cleaned her either and. […] she wasn’t laid out like a baby, she was laid out like a corpse I mean, they hadn’t even cleaned her, they hadn’t even put some little clothes on her. Nothing, nothing at all.
(Extract 4. Montse, third trimester stillbirth, interview)
The following extract is compelling because it demonstrates a connection between interactive silence and broader cultural discourses of taboo and shame. Here the sense of being observed, in silence, leads the parents to access the only cultural values that are available at the time: that to engage with the baby’s body would contravene some social code. This type of behavior is evident in various forms throughout the data and has a limiting effect on social action because it invokes stigma and a shame based dilemma that brings the parent-child relationship into conflict with the more authorative patient-professional relationship: My husband felt that that we shouldn’t take too long, because we could see them [the health professionals] through the window, it made us think that we shouldn’t spend too long seeing her. It was more like by not saying anything we understood that we could only see the baby very briefly.
(Extract 5. Sonia, third trimester stillbirth, survey respondent)
Silence in the Home and Community
Silences in the community mirror those of the hospital, they are a dominant theme of experiences of perinatal grief, but must also be considered as complex and inconsistent. The majority of the interview participants and forum members discussed members of their social network that had never talked to them about the loss, as well as fractured and irreparable relationships. Yet, none of the interview participants had experienced complete silence, although one seemed very close. Silence was often structured in terms of family and kin relations: older versus younger members, along gender-lines, or in-laws compared to blood relations.
In the following extract, Beatriz, whose baby had died five years before the interview, responded to my question about why she liked talking to her psychologist: Well I liked the advice that she gave me from the very start, the naturalness that, I mean, of how she talked about it, because I could only talk to her about it, everyone else, no one wanted to talk about it with me, so as not to hurt me, but I need to talk because she was my daughter and it had happened and I couldn’t deny it, when I tried to talk about it with someone, people changed the topic.
(Extract 6. Beatriz, third trimester stillbirth, interview)
Here, it is notable that the interactions with the psychologist are “natural”, a space where Beatrix feels comfortable, which contrasts to the awkwardness and lack of capacity to communicate in the social milieu. The crux of Beatriz’s story though relates to how silence acts to deny her daughter’s existence. This also creates a conflict in the mother-milieu and mother-child relationships; if she does not talk about her daughter she fails in her basic social role of mother, but if she does talk, she is sanctioned with silence.
Silencing Through Conflicting Meaning-Making
The analysis found that attempts to provide support by framing the death in a positive light is one of the primary ways that differences in understandings of the nature of perinatal death are evident in social interactions. Leticia (third trimester stillbirth, interview participant) talked about how hurtful it was to hear people offer the opinion that it would have been worse had her daughter died later. This deterministic and biometric arrangement of expectations of grief intensity differentiates perinatal loss from other forms of grief.
Ideas that women are expected to recover in a relatively short period of time and get back to their old selves are another important form of meaning-making. Discursively, this is expressed in normative concepts of grief as linear and reaching a resolution and recovery. Interactively, they silence or exclude alternative understandings of grief as variable, unpredictable and related to a changed sense of self and the world. Montse talked about tensions with her partner that centered on his lack of understanding about the duration and variability of grief. She contrasted his relatively straightforward and simplistic expectations with her own experiences of a complex and difficult process of meaning-making that placed her outside normative stories of maternity and happiness: he doesn’t understand me, he says: “but you’re alright now, it’s been …” Because I’m, I mean, I have a relatively normal life, ehm., and so, to see me unwell all of a sudden, one day, well, he doesn’t, ehm., he doesn’t understand that I’m, that I can feel bad when I see other women who have had wonderful births, wonderful children, healthy pregnancies. But I didn’t, so, I think that the stage of grief of thinking, “why me? why me?”, it’s still there.
(Extract 7. Montse, third trimester stillbirth, interview)
Francisca, like Montse, wrote in the forum about her struggle with this changed sense of self and identity, which conflicts with her social networks desire that she “get back to being the same as before”: Amongst my family and friends I have many people that love me and help me, but a type of impatience has started because they want me to recover emotionally and get back to being the same as before. and inside I think I’ll never be the same.
(Extract 8. Francisca, first trimester loss, forum member)
In both of these cases, family and friends are viewed as generally ‘supportive’ but also impatient and lacking a fundamental understanding of the long struggle to understand the impact of death and develop new life narratives.
Other common discourses related to positivity and rationalizations of loss that draw on ideas of youthfulness, the innate capability of the female body to reproduce, and how having another child will help the process of recovery: almost all of us have heard unfortunate phrases such as you’ll soon have more, you’re young, better now than later. We know that a child can’t be substituted, that each child is unique
(Extract 9. Alicia, second trimester termination, forum member)
Collectively, these findings highlight how normative discourses of ‘time’, ‘recovery’ and female reproduction are crucial markers of support and its limitations.
Self-Censorship and Disenfranchisement
Acts of self-censorship are largely unified by common themes of an altered sense of self, self-protection, and maintaining social harmony. Analytically, they can be organized into four primary forms: i) self-exclusion from loss related rituals; ii) othering and self-isolation due to shame and guilt; iii) remaining silent in order to protect the self and maintain social harmony; and iv) invalidation of one’s own emotions and hierarchization of loss.
Self-Exclusion From Loss Related Rituals
The most immediate way that self-disenfranchisement materializes is within the hospital when women or their partners decide pre-emptively to not see their baby or reject an offer to do so because they feel that the appearance of the baby will disturb positive memories of the pregnancy or cause long-lasting psychological damage: I decided myself not to see him because I didn’t want to have that memory and to get pregnant again without getting it out of my head
(Extract 10. Monica, second trimester stillbirth, survey respondent)
This type of self-disenfranchisement draws on cultural ideas of dead babies and contact with them that positions them as threatening or contravening social norms (see also extract 5). However, the majority of decisions to not see a baby are founded in poor decision-making processes (lack of information, empathy) where we find a temporary symmetry between parents and untrained professionals connected by the common values of stigma and fear. For women, the consequences can be twofold: regrets about actions in the hospital and spoiled identity due to perceptions of having failed to live up to social roles and obligations. Although a significant amount of women express no regrets, the following sentiment is quite common: now I live with a horrible regret, sadness and I feel like a very bad person for not having wanted to see him. When some time had gone by I wanted to die for not having said goodbye to my boy. I’ll never forgive myself for that.
(Extract 11. Sara, second trimester termination, survey respondent)
Othering of the Self: Deconstructed Social Identity
In the following extract, when talking about why she tended to avoid social gatherings where babies and infants would be present, Montse elaborates on her changed sense of self (see extract 7) and how she feels anomalous, incompatible with her own idea of a woman: It was like going back to the start, I felt the same as the first few days, I felt, I didn’t feel, well that, eh, like that, incapable of the most basic thing, you know? Like a woman, that is, man is born, grows and reproduces and dies. I didn’t know how to do the most basic thing, you know?
(Extract 12. Montse, third trimester stillbirth, interview)
Similarly, Beatriz spoke about how, when the cot was taken out of her room, that she thought everyone on the ward saw her as “the one who lost her baby” (emphasis added). In the absence of a baby, she saw little sense in friends and family coming to see her, and therefore also rejected the possibility of support, at least in the immediate term. Like Montse, Beatriz defines her self in terms of broader cutural ideas that equate being a woman to motherhood and fulfilling that role.
Protecting the Self From Harm and Maintaining Social Harmony
Elisabeth provides a relatively straightforward example of self-censorship as a form of self-protection from social sanction and as a way of maintaining social harmony: you’re in work one day, you start crying because you just can’t handle it anymore and they look at each other like: “Fuck, what a show”. And that doesn’t help me, you know? It’s like: “yeah, what a show, I’m annoying you”. Well now I don’t cry, now I just go and cry by myself.
(Extract 13. Elisabeth, second trimester pregnancy termination, interview)
Self-censorship, however, is often a strategic response that bereaved women adopt over time, when they come to realize that attempts at enfranchising and resisting incompatible meaning-making are ineffective or too hurtful (see also Beatriz, extract 6): I don’t deal with it the same now, […] I don’t have the need to convince, I have, I have the, the need to say that, ehm, I don’t want to have that conversation, that conversation: “what are you saying, that you love your son more than me? I’m not, I’m not going to talk about this topic with you.” And so I don’t get into it.
(Extract 14. Blanca, neonatal death, interview)
In this respect, Blanca adopts a form of ‘moral high-ground’ that permits her to self-protect while surrendering to the social milieu and the established norms. However, even though she gains control by ceding control, it is evident that it falls on her and other women to maintain social harmony by being quiet, forgiving, or just accepting the social circumstances (see also extracts 6 and 8). By coercing women to present a ‘false’ face publically, this imbalance in social power can place a serious strain on the self, as illustrated by the anger and frustration that Ines communicated in the forum: When I talk with them [female friends with babies], I pretend to be ok and I need to scream that I’m not. I’M NOTTTTTTT, I’M NOT ALRIGHTTTTTT, OK??????: because come on, pretending to be alright, just so that you don’t get a lecture about how “that’s life”
(Extract 15. Ines, first trimester loss, forum member)
Thus, self-censorship comes at a cost: the loss of potentially valuable support and, by ‘pretending’ and not talking about loss publicly, women also choose to not talk about their dead children. This places them in a situation that challenges their identities as ‘good’ mothers, which may already be under attack in various forms. Leticia spoke about this “dilemma” of talking and not talking about her baby: [when someone] says: “is it your first?” and you find yourself in a dilemma, I mean, if it’s, if you say that it is, if you leave Carla out, eh, because what they say will hurt, the comments that they make, […] if you say “yes”, I only have Ruth, I'm avoiding talking about Carla, but if I mention her…
(Extract 16. Leticia, third trimester loss, interview)
Invalidation of Emotion and Hierarchization of Loss
Finally, the silencing discourses and sanctions that seek to avoid and control emotional expression in institutions and the social milieu are also evident in bereaved women’s own discursive interactions, creating a dynamic of self-disenfranchisement. This was notable in the narrative interviews when women would apologize for crying, or because they thought they were ‘going on’ too much. In the support forum, part of the process of socialization into the community by other bereaved women was to reassure new members that this was alright and that it was perfectly acceptable to be emotional and to talk about problems and feelings at length.
Similarly, the hierarchization of loss by age, which is evident across society, was also present in bereaved women’s own discourses. In the following extract Nerea, minimizes her own experience of grief while consoling another woman whose baby had died at a more advanced gestational age, reproducing disenfranchising categories of loss and self-censoring: how hard to lose your baby after the birth…. I lost mine at 21 weeks and I can’t imagine what you went through
(Extract 17. Nerea, second trimester loss, forum member)
Discussion
Using a research design that permitted the analysis of a single population from differing locations and through various techniques, the research provides only a ‘view’ of the interactive experiences of the disenfranchisement of perinatal grief amongst the women who participated in the study. At a general level, the research finds that the disenfranchisement of perinatal grief was multi-faceted, complex and entangled with broad cultural values and discourses, which is similar to disenfranchised grief in general (Corr, 1999; Doka, 1989). As women engage in reflective social processes of negotiation about the significance of perinatal loss and their own social identity as bereaved mothers, an understanding of perinatal grief emerges that is differentially related to: the biometrics of pregnancy (lower gestational age is equated to lower grief and support needs); the passing of time (expectations of a relatively quick ‘recovery’); competing discourses of loss (simplistic-dominant vs. complex-subordinate meaning-making); gendered ideas of reproduction (moral, responsible mothers, innate capacity to reproduce); feeling rules related to sadness and gender (expression, stoicism); absence of knowledge and imbalances in social power; differing and conflicting practices in the social spaces of the hospital, home, community, and support groups; lack of socio-material and performance resources for bereavement and ritual; and structural aspects of the social and familial organization of grief according to gender, age (intergenerational), and kin relations (family vs. friends). At an experiential, as opposed to purely structural level, disenfranchisement relates to how the social space for grief and support is narrowed and constrained along all or some of these lines, as well as to the degree of constriction (complete or partial).
In overall terms, the research could establish that only a small proportion of women experienced complete disenfranchisement of grief. Most had some members of their close social network that provided support and acknowledged the loss, although this often fell to partners alone. However, only very few, if any, experienced what could be properly described as fully enfranchised grief. Most experienced some conflictive social interactions or contradictions in how the significance of the loss was established during care or in the community. And, even when grief was accepted it tended to occupy a lesser category. At a broader level, feeling rules in relation to sadness play a highly important role in disenfranchisement across all social spheres. This is heavily influenced by gendered ideas of emotion, although that is not to say deterministically. Expressing ‘negative’ emotion is perceived as unfairly burdening those who must listen, leading in many cases to sanction and other mechanisms of suppression, which closes off avenues to loss-oriented communication. The analysis also shows that empathy and emotional support alone do not necessarily equate to the enfranchisement of grief.
The impact of disenfranchisement on the bereaved can be considered in two ways. On the one hand, inadequate social support can have a double impact as there is no middle ground between support and no support; the bereaved not only lose the protective effects of social support but also experience a worsening of the impact of grief, caused by isolation, abandonment and deprivation (Parkes & Prigerson, 2009, p. 11). Consistent with other research (White et al., 2008), the primary order of deprivation in this study relates to a lack of emotional support and processes of silence and silencing that constrict accompaniment, talk, non-judgmental listening and acknowledgement of the loss. As disenfranchisement and lack of social support, this has clear implications for health (Burke & Neimeyer, 2013; Gold et al., 2016).
On the other hand, from the perspective of grief theory, a number of observations can be made. Firstly, attempts by the social network to force the pace of grief would seem to pressure the bereaved into restoration-oriented grieving while they are still loss-oriented (Stroebe & Schut, 1999). Through processes of self-censorship and isolation, the bereaved may subsequently resist the social milieu and push further into loss as a means of remembering and defending their dead child. As such, conflict related to the reality of the loss, sharing of pain, relocation of the deceased, and acceptance of a changed world may create additional stress and complicate coping through a disturbance of the natural oscillation between loss and restoration (Stroebe & Schut, 2015).
Secondly, as a central component of grief, meaning-making is heavily implicated in complicated bereavement (Holland et al., 2006) and is particularly relevant in traumatic deaths (Davis, 2001). One of the key ways that disenfranchisement influences perinatal grief is through the imbalances in social power that result in narratives of grief that are overly-determined by healthcare institutions or the social network, disenfranchising the bereaved from their own story. The taken-for-granted meanings that the social network or healthcare professionals draw on are often simplistic and oriented toward ‘positive’ meanings, frequently drawn from gender-based discourses. This contrasts to the complex process of bereavement that challenges women’s very sense of self and social identity. As empathetic failure, the hurtfulness of these meanings encourages silence (self-censorship), which in turn creates a failure of communication. This deprives the bereaved of the social processes of negotiated meaning-making that take place through conversation and narrative within families and social networks (Nadeau, 2001; Walter, 1996). By undermining rights and entitlements to tell particular stories, there is also a direct link to normative cultural ideas of women and motherhood to which pregnancy loss creates a position of “other”, founded in guilt, shame and a sense of reproductive failure, as has been observed by Murphy (2012).
The ambiguous nature of silence as a mechanism of disenfranchisement is also highly relevant to meaning-making and support. Silence is entirely context dependent, it requires the ‘receiver’ to correctly draw on inferred meaning or presupposed knowledge to understand the significance of the unsaid (Huckin, 2002). As silence is open to a wider range of interpretations, it requires greater cognitive effort and is prone to complications of communication (Sobkowiak, 1997). Its potency relates to it being simultaneously categorical and ambiguous, making it difficult, stressful and exhausting to address or resist. As such, silence, silencing and self-censorship are highly effective in their capacity for the social reproduction of stigma.
Finally, if we consider disenfranchisement in terms of the social dynamics of continuing bonds (Klass, 2006), it is apparent that the social processes of isolation and reconfiguration of the deceased as a non-person complicates any attempts to relocate them within the family and social network. As Klass (1997, 2001) points out, the degree to which the dead are integrated into the social network is directly related to the level of validation of the child, the amount of social support provided, and the avoidance of complications in grief. When this isn’t possible, parents can feel that they are failing in their obligations to their children (Riches & Dawson, 1998a), introducing toxicity into the bond at precisely the time when positive post mortem relationships are key to healthy bereavement.
Supplemental Material
sj-pdf-1-ome-10.1177_00302228211050500 - Supplemental material for The Disenfranchisement of Perinatal Grief: How Silence, Silencing and Self-Censorship Complicate Bereavement (a Mixed Methods Study)
Supplemental material, sj-pdf-1-ome-10.1177_00302228211050500 for The Disenfranchisement of Perinatal Grief: How Silence, Silencing and Self-Censorship Complicate Bereavement (a Mixed Methods Study) by Paul Richard Cassidy in OMEGA—Journal of Death and Dying
Footnotes
Acknowledgements
Jillian Cassidy, Umamanita, Ángel Gordo, Universidad Complutense Madrid, Carolina Rodríguez Palenzuela, Asociación Cometa.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted as part of a doctoral research program at Universidad Complutense de Madrid and in collaboration with the Spanish stillbirth and neonatal death charity Umamanita, who provided a small amount of funding (€600) to cover the cost of survey hosting, recording material and travel to congresses.
Supplemental Material
Supplemental material for this article is available online.
Note
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.