
Abstract
Studies on end-of-life experiences (ELEs) suggest that caregivers and loved ones of dying patients also have ELEs, though these are rarely explored. This article introduces the Spectrum of End-of-Life Experiences (SELE) as a descriptive list of types of ELEs reported by all members of the care unit, including dying patients, their caregivers, and their loved ones. We applied SELE towards identifying ELEs reported by 143 caregivers and loved ones and successfully identified every experience. Interviews revealed that participants viewed their ELEs as profound communicative events, yet a substantial minority also reported struggling to name and process these experiences. We propose that SELE be included in death education to raise awareness about ELEs that can occur within the care unit, and we suggest that SELE has additional applications, including use as a prognostic aid in end-of-life care and as a therapeutic aid for bereavement support.
Introduction
The earliest empirical studies into phenomena eventually known as end-of-life experiences (ELEs) began in the late 19th century with the founding of the Society for Psychical Research. One of this organization’s first major studies was an analysis of sociological data pertaining to sensory hallucinations, which revealed a substantial number of reports of “apparitions”: non-physical phenomena resembling or referencing a human being. Their analysis revealed that no event coincided with the appearance of an apparition more than that of a death (Gurney et al., 1886). Shortly thereafter, Frederic Myers charted the frequency of apparitions relative to the moment of death and found that there was a steady increase of apparitions in days and hours before a death, while the highest frequency of apparitions occurred at the moment of a death. This was followed by a gradual decrease of apparitions sighted during the days, weeks, and months after a death (Myers, 1903). Just over two decades later, Sir William Barrett published a study of “deathbed visions” in which he presented a typology of end-of-life experiences; exactly half of the number of types that Barrett identified were those reported by loved ones and caregivers of the dying (Barrett, 1926). In sum, early psychical research revealed that the living and the dying alike may experience a variety of non-ordinary phenomena around the event of a death.
Interest in psychical research eventually waned and most studies on ELEs shifted away (for a time) from experiences reported by caregivers and loved ones. Within contemporary medical literature, studies on the ELEs of dying patients have offered significant insights, most notably that the dying commonly report dreams and visions of deceased family and friends (Kerr et al., 2014; Nosek et al., 2015), patients and caregivers may require specialized support in processing ELEs (Brayne et al., 2006), there is a correlation between ELEs and posttraumatic growth (Levy et al., 2020), and there is a need for specialized training on ELEs for those working with individuals at end of life (Fenwick & Brayne, 2011). Not least of all, we also know that ELEs are underreported in patient records and are underrepresented in death education (Claxton-Oldfield et al., 2020). However, the corpus of studies on ELEs exhibits variation in terms used and phenomena described. For instance, the term “deathbed visions” has been used to identify instances where deceased family members and loved ones appear to the dying (e.g., Fenwick, Lovelace, & Brayne, 2007), “deathbed communication” has referred to any kind of communication between a dying person and deceased family and friends within 30 days of dying (Lawrence & Repede, 2013); and “death-related sensory experience” has been used to name any spiritually transformative experience involving a vision of otherworldly messengers or guides appearing to a dying person (Ethier, 2005).
Similar issues exist in recent studies that have included personal reports of ELEs by caregivers and loved ones of dying patients. For instance, studies have focused on family members’ reports of hearing about the ELES of dying loved ones (Kellehear et al., 2011; Muthumana et al., 2011), the impact of ELE reports by dying persons on family members (Grant et al., 2020, 2021; Morita et al., 2016), caregiver reports of the ELEs of dying patients (Fenwick, Lovelace, & Brayne et al., 2009; Lawrence & Repede, 2013), and reports of caregiver attitudes and beliefs about ELEs (Claxton-Oldfield & Richard, 2020). Some studies have merged reports of direct, first-person encounters of ELEs by caregivers and loved ones with second-hand reports of hearing about an ELE or witnessing a patient react to an ELE (Brayne et al., 2008; Claxton-Oldfield & Dunnett, 2018). There remains a scarcity of research focused on those first-hand ELEs reported by caregivers and loved ones (Fenwick & Fenwick, 2008; McDonald et al., 2014; Shared Crossing Research Initiative, 2021).
We see great value in standardizing the language employed in identifying various types of end-of-life experiences to include those first-hand experiences reported by caregivers and loved ones of dying patients. This would serve to further normalize these experiences, to better reflect the fact that ELEs occur among members of the entire care unit, and to bring together disparate lines of research. It is crucial for end-of-life and death education to include ELEs reported by loved ones and caregivers because these individuals often need to discuss, process, and integrate their experiences in a safe and supportive environment. To develop and incorporate the “best practice” to accommodate this first requires better understanding the nature of ELEs. We approach ELEs as fundamentally interpersonal events, as these experiences—whether reported by dying patients, loved ones, or caregivers—inform and are informed by the ongoing relationships that people have with others, whether living or deceased. This perspective drives an aspect of contemporary grief therapy known as “Continuing Bonds,” which is discussed below.
The present article introduces the Spectrum of End-of-life Experiences (SELE) as a comprehensive, user-friendly list of the kinds of end-of-life experiences reported by all member of the care unit, including dying patients, their caregivers, and their loved ones. SELE is intended to raise awareness about ELEs so that they are not viewed as aberrant or delusional. SELE situates all end-of-life experiences within a timespan of approximately 1 year outside the time of a death, which closely mirrors the timeline of the Medicare mandate requiring hospices to provide bereavement services for a minimum of 13 months following a patient’s death. William Peters initially designed the Spectrum of End-of-life Experiences (SELE) in 2014 in response to his psychotherapeutic work with hundreds of bereaved clients reporting extraordinary experiences around the time of death of a loved one or patient. Most of these clients were not fully able to process these experiences, and some questioned their mental health. Peters drew heavily upon his professional work, as well as upon literature on psychical research, thanatology, hospice care, and end-of-life experiences (especially the work of Peter Fenwick)—to construct SELE. Since 2015, he has presented SELE to both clients and colleagues. With the input of experts in various disciplines, SELE has been further revised.
Method
Participants
Demographic Information.
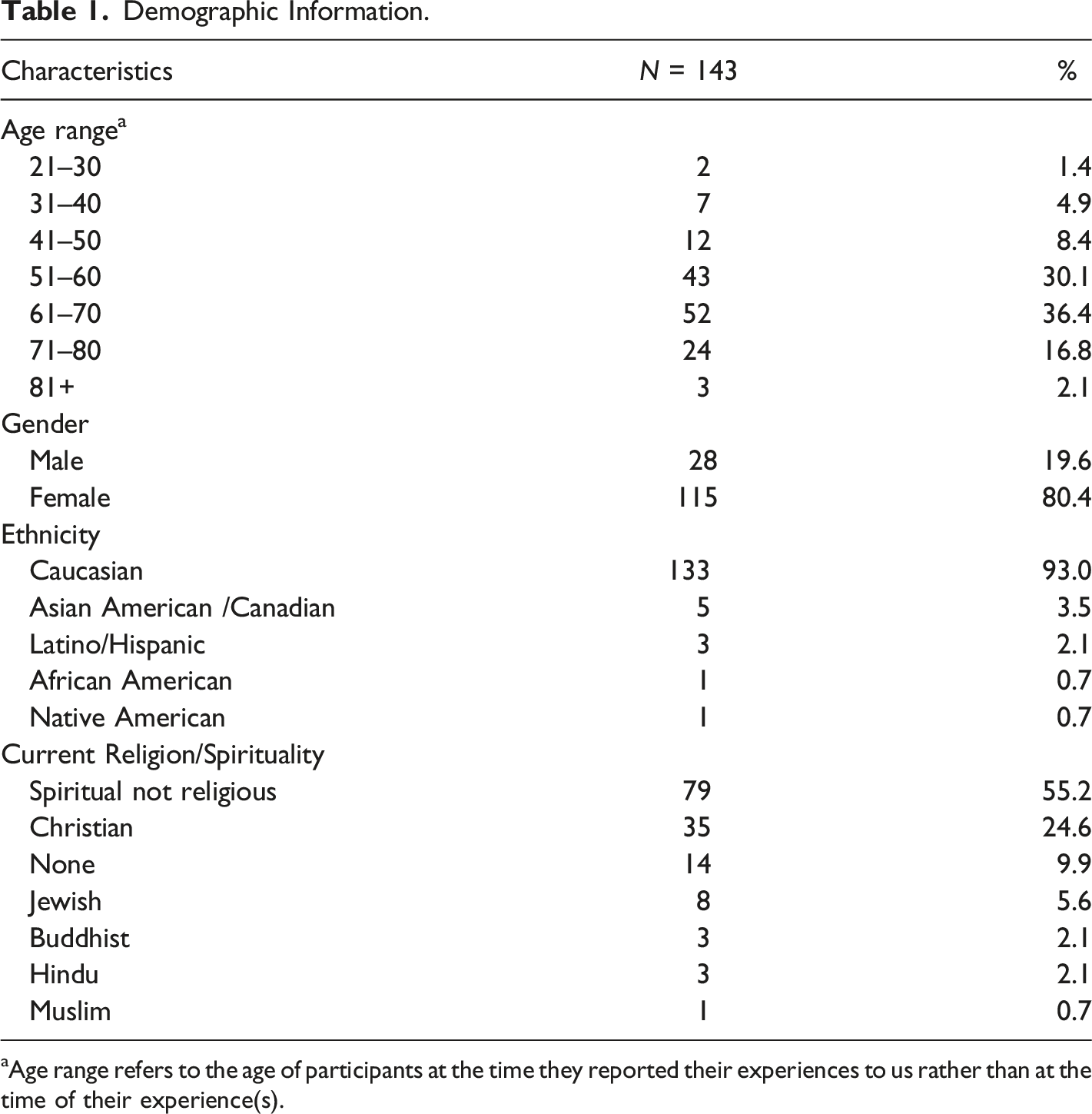
aAge range refers to the age of participants at the time they reported their experiences to us rather than at the time of their experience(s).
Procedure
Interview protocol consists of Kinsella and Peters implementing an interview questionnaire to collect demographic information and to ask each participant to describe (1) their prior involvement with religious or spiritual activities and any history of anomalous experiences, (2) the individual(s) whose deaths they believed were catalysts for their experiences, (3) the context of their experiences, (4) any effects they attributed to their experiences, (5) whether they had told others about their experiences, and (6) whether there was anything else that they would like to share with us regarding their experiences. Several clarifying, follow-up questions are also asked. All interviews are recorded, and nearly all take place through Zoom, a remote conferencing service. Exceptions include Peters having conducted four interviews in-person. Recordings are transcribed and, along with any previously submitted written reports of their experiences, coded for content. Excluded from our interviews were five individuals who reported being professional psychics or spiritual mediums and three individuals who appeared to exhibit extreme fantasy-prone personalities.
Kinsella and Peters, together with research assistants Noël Christensen and Michelle Johnston, carry out a content analysis on all written reports and interview transcripts. This consists of noting when the experience transpired relative to the time of a death, identifying key features and traits attributed to each specific ELE, determining whether the experience fits within a type of ELE listed on the Spectrum of End-of-Life Experiences (SELE), and analyzing both participants descriptions and interpretations of their ELEs. We do not utilize inter-rater reliability as we are embedded in the research context, coding requires little interpretation, and participants’ own interpretations of the data drive our analysis (McDonald et al., 2019). This study has been approved by an ethics review board at the Family Therapy Institute of Santa Barbara, and all contributing participants have given documented informed electronically signed consent via Docusign. Qualitative findings presented below include the identification of distinct types of ELEs that were well represented throughout the data examined.
Results
Every ELE reported and described by our 143 participants was readily identifiable on the Spectrum of End-of-Life Experiences (SELE). Furthermore, interviews revealed a number of specific aftereffects that participants regularly attributed to their ELEs: 120 participants (83.9%) were convinced that their ELE had provided them with experiential evidence that individual human consciousness continues beyond death, 91 participants (63.6%) stated that their ELE had significantly reduced or completely diminished their grief, 82 participants (57.3%) reported being at peace knowing that their deceased patient or loved one was okay, and 76 participants (51.3%) claimed that their ELE had diminished or completely removed a prior fear of death and dying. We also found that 115 participants (80.4%) reported having had more than one ELE. The majority of ELEs were viewed as positive transformative events, although 21 participants (14.6%) reported distressing or negative experiences. Out of these 21 participants, 16 described their negative experiences as resulting from social stigmas attached to sharing such accounts with others. An additional 15 participants emphasized being fearful of ridicule by colleagues, family, and friends. These observations reinforce the idea that raising awareness about ELEs would contribute towards individuals being better able to discuss, process, and integrate these experiences.
We noted that nearly every participant interpreted their ELEs as a communicative event initiated by a dying person, previously deceased loved ones, a recently deceased person, otherworldly beings (such as angels or benign spirits), and/or some higher power (such as God, the Universe, the One, Collective Consciousness, etc.). The only exception to this were those instances of pre-death premonitions, which were typically understood to be intuitions or the results of comprehending information not normally available (i.e., psychic ability) when not attributed as coming from a higher power. The remaining ELES that were viewed as communicative events were understood by participants to convey an important message, which often focused on an affirmation that death is not the end; that a loving, higher power exists; and that deceased loved ones continue to exist in some form in a benevolent afterlife. In fact, many participants referred to their ELEs as being “a gift,” and some participants spoke of their frustration at not being able to freely discuss their experiences with others. Every participant expressed gratitude for having the opportunity to discuss their experiences with sympathetic professionals working in end of life and to learn more about ELEs. Elsewhere we have discussed other aspects of this ongoing study (Shared Crossing Research Initiative, 2021).
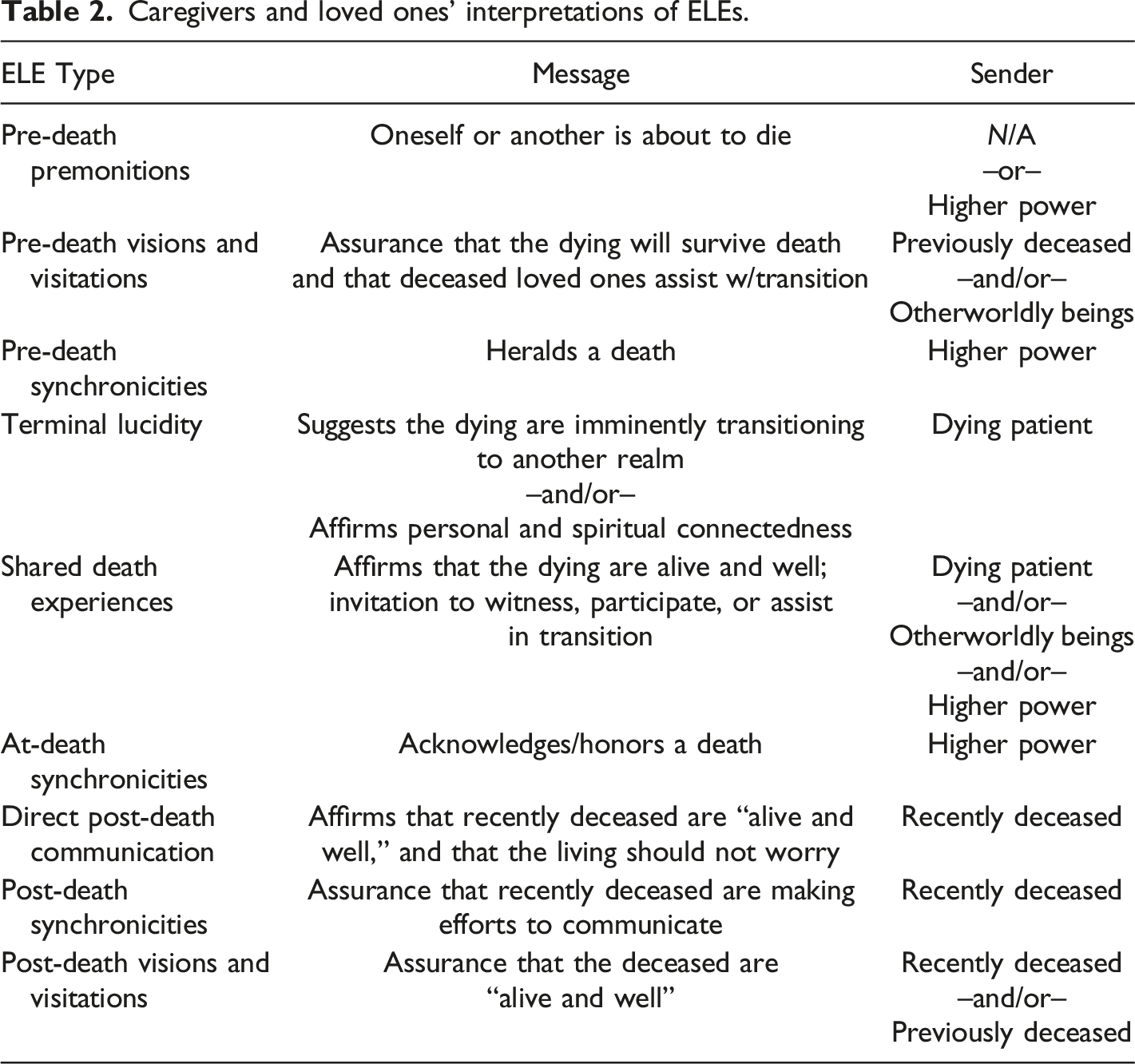
Below we present SELE (Figure 1) and a summary of caregivers and loved ones’ interpretations of each type of ELE (Table 2). This is followed by brief descriptions and examples of each ELE type as found in our interviews. SELE. Caregivers and loved ones’ interpretations of ELEs.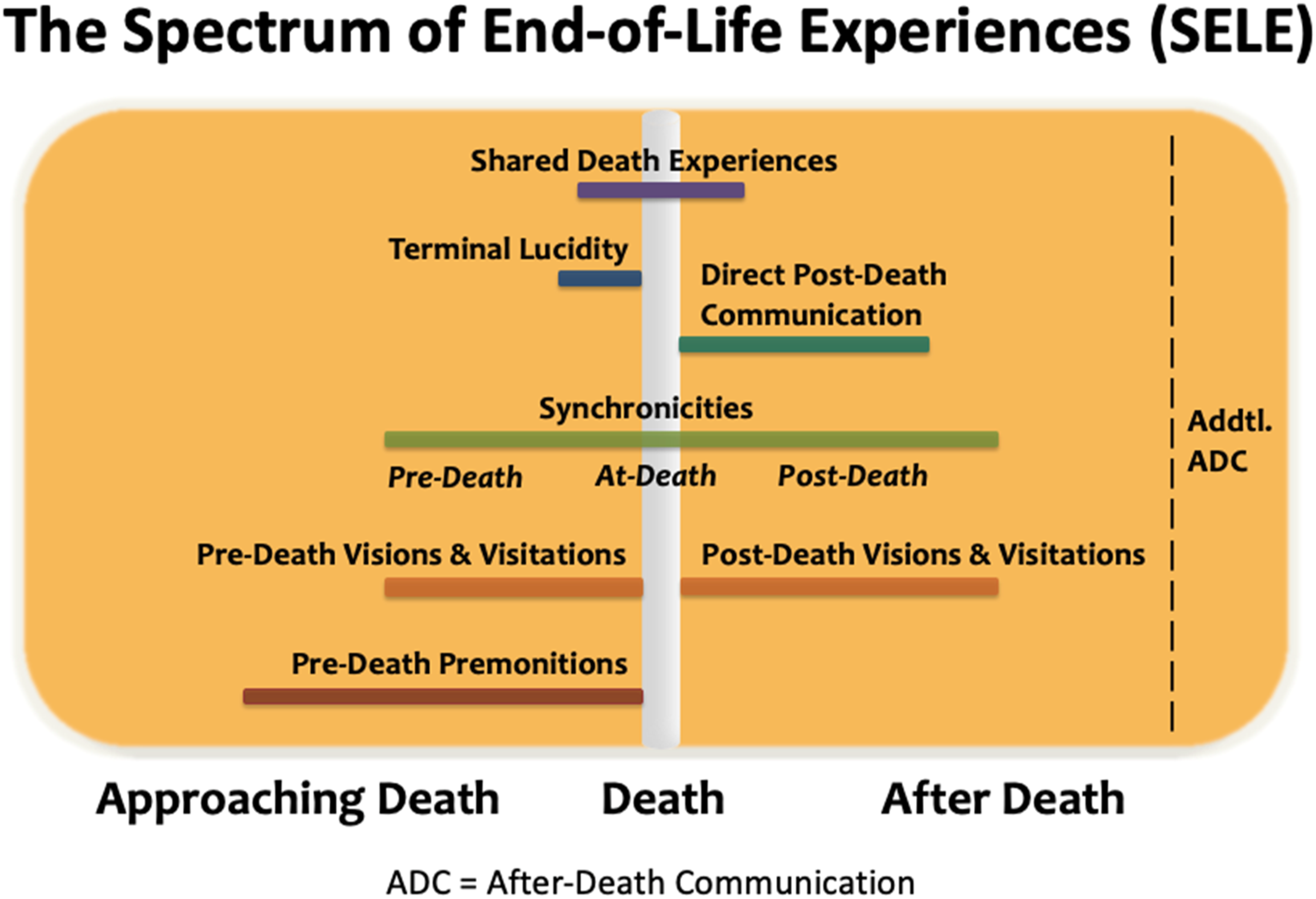
Pre-Death Premonitions
Pre-death premonitions consist of strong feelings or thoughts that either oneself or another is about to die (e.g., Hardoin et al., 2007; Ngeh, 2003). These premonitions typically appear days to hours before a death, although some reports include premonitions of a death that occurred months or even years beforehand. Pre-death premonitions, like other kinds of ELEs, may occur while awake or dreaming but if occurring while dreaming, the contents of the dream are reported to be much more salient than ordinary dreams and they are often described as fully conscious experiences with transformational aftereffects (in fact, the main reason we intentionally refrain from identifying ELEs reported to occur during sleep as “dreams” is that individuals make it a point to express that these experiences had an intense clarity and were qualitatively different than usual dreams). One participant shared the following: “My brother and I had taken the train to Zermatt. And the next day we were going to go glacier skiing. The two of us were staying in a little pensionné. And in the middle of the night, all of the sudden, I’m terrified and I’m not sure why. And I’m looking over at my brother, whose sound asleep. And I’m just checking whether he’s breathing. . . And because he’s obviously fine, I go back to sleep. And the next day, we’re on the slope in Zermatt. And my brother decides to ski off trail. Skis off a cliff and breaks his neck. He’s dead at the scene. And so, I had a premonition that that’s what was going to happen. I just didn’t know it at the time. This confused me for years afterwards.”
Pre-Death Visions and Visitations
Pre-death visions and visitations consist of seeing, hearing, or otherwise sensing the presence of otherworldly realms and entities, many of whom are identified as deceased loved ones that appear to be comforting and providing support for the dying (e.g., Mazzarino-Willett, 2010; Nosek et al., 2015). These may occur hours, days, weeks, or even months before a death, and they may occur to a dying patient as well as to a caregiver or loved one. One participant who had cared for his dying father shared the following: “Sometimes Dad would have conversations with people up in the corners of the room. And you would see his mouth moving, and he would be gesticulating as if he’s actually having a conversation. I said, ‘Dad, who are you talking to?’ He wrote down, ‘H.’ That was his best friend who had passed away about 10 years ago. Then he started having conversations with different people, always up in the corners of the room. At one point he started introducing me to somebody. Dad said to this other person, ‘This is my older son. I’d like you to meet my older son.’ He grabbed my hand and he wanted me to shake hands with this being that I couldn’t see or hear. And so, I said, ‘Hello, it’s very nice to meet you. I wish I could hear you, and I wish I could know what’s going on between you, but my father seems comforted and able to have a real clear relationship with you.’ Eventually, my dad wanted me to introduce myself to other people around the room that were there. And then every night he continued having these very meaningful, apparently comfortable conversations with people that I never saw, never heard, but could feel.”
Pre-Death Synchronicities
Pre-death synchronicities are events wherein seemingly unrelated events or coincidences are viewed as messages related to or signaling an impending death (these are often referred to as “deathbed coincidences”; see Fenwick & Fenwick, 2008). Such phenomena typically include an unusual natural situation, such as unusual weather or the appearance of a certain animal, or electronic devices malfunctioning in personally meaningful ways. Because synchronicities consist of highly subjective interpretations, audiences often dismiss such experiences for not carrying the same “evidential weight” as other kinds of ELEs. Yet it is important to be aware that individuals reporting these experiences consider them to be highly significant communicative events. One participant shared the following event that had occurred shortly before her father’s death: “One morning it was apparent that his energy was fading. He was dying in the home that he and mom had built over fifty years ago on the Intracoastal waterway in Fort Lauderdale. I left his bedroom to go into the den, then I saw everyone out on the dock pointing at the water. I went outside to discover that three dolphins had gathered right next to the dock and were jumping all around. In all the years of living in that house we had never seen dolphins in the Intracoastal. . . I immediately knew that this display of nature’s playfulness was orchestrated for me and for Dad and for everyone gathered. . . As everyone once again came to his bedside, I told dad about the dolphins outside right then and thanked him for that one final gift. Within minutes, Dad made his transition.”
Terminal Lucidity
Terminal lucidity involves the demonstration of an unexpected and physiologically unexplainable surge of vitality at end of life that may manifest as dramatic improvements in mental clarity, physical functioning, and/or spiritual relatedness (Nahm, 2009; Nahm et al., 2012). Terminal lucidity usually occurs moments, hours, days, or even weeks before a death. One participant shared the following experience that had unfolded while she and one of her sisters, M, sat vigil for their dying sister, C: “C’s breaths are coming very, very far spaced, far in between. She’s having one gasp, and it sounds like her last one, and then 40, 45 seconds later there’s another one. . . I know it’s coming quickly. All of the sudden—this is somebody with no brain stem—her eyes open and she looks into the corner behind me where the light is. We were amazed and elated just at this, that she had opened her eyes. Her eyes were so wide that the whites were showing completely around her eyes, but nothing on her face was moving, only her eyes. I don’t know how they got so big. She started tracking very, very slowly behind us. Then they came back and looked straight at my sister and I, and then. . . the eyes became very vacant. She gave three very small exhalations, and then as far as I’m concerned, she was gone. It felt like the room was filling up with people to meet her. It just felt like it was a gift to us. We became quite elated. M couldn’t stop repeating, ‘I will never fear death again! I will never fear death again!’ That was so beautiful to me.”
At-Death Synchronicities
At-death synchronicities are events wherein seemingly random events occurring at the moment of death are viewed as messages from some higher power (e.g., Fenwick & Fenwick, 2008). Again, while synchronicities are highly subjective interpretations of events, they are nonetheless imbued with profound meaning for individuals reporting them. Two participants, the daughter and niece of a man who had died, both reported being profoundly affected by an event occurring at the time of his death. The daughter stated the following: “I had just said, ‘Whenever you need to go, dad, we’re here, we’re with you,’ and then all of the sudden we heard the birds at the window, and they were so loud. [The niece] and I looked at each other like, ‘What is that?’ And then dad opened his eyes and looked toward the window, and he smiled. It was beatific—he smiled and then he was gone. . . I certainly didn’t expect to get the megaphone call from the birds outside the window. That was like, ‘Wow!’ Shocking is the word that comes to mind. How distinct it was and how loud it was. In retrospect, I think perhaps it was so loud because they were calling him. It wasn’t to let us know that it was time for dad to go. They were trying to get dad’s attention and he wasn’t wearing his hearing aids, so they had to be loud.”
In a separate interview, the niece shared with us the following: “He had his last breath and then. . . [the daughter] and I just looked at each other in shock because she was on one side and I was on the other, and the birds were so, so loud. . . Then he smiled and that was it. And the birds just went crazy. . . I’ve never experienced anything like that. And I don’t think I’ve ever heard birds so beautiful. It was beautiful. I mean, it was really gorgeous, and it happened right after he passed. So, I don’t think I’ve ever experienced anything quite like that before. It truly makes you question things a bit, I guess.”
Shared Death Experiences
Shared death experiences consist of caregivers and loved ones feeling that they have participated in a dying person’s transition to a post-mortem existence (Shared Crossing Research Initiative, 2021). Individuals may sense (physically and/or intuitively) that a loved one is dying; witness various unusual phenomena associated with death (such as seeing what is believed to be the spirit leave the body); find themselves either out of body or in a visionary realm where they seem to be accompanying the dying to some destination; and/or feel that they are somehow actively assisting the dying to transition.
Several phenomenological features appearing in SDEs are nearly identical to those reported in near-death experiences (NDEs), which constitute a category of extraordinary experiences occurring while an individual is psychologically or physiologically close to death (e.g., Greyson, 1983; Long & Perry, 2010; Moody, 1975). For instance, one study found that deceased family and friends appeared in over 13% of 617 near-death experience narratives (Long & Perry, 2010: 123–124), whereas we found that deceased family and friends appeared in 22 of 164 (13.4%) shared death experiences reported by 107 of our participants. Some features appear to be more common in NDEs than SDEs. For example, Long and Perry found that 64.6% of 617 NDEs included the appearance of a brilliant or mystical light (Long & Perry, 2010:10), whereas this feature appeared in 25% of our SDE accounts. Other features found in both NDE and SDE accounts include alterations of time and space, visions of otherworldly or heavenly realms, the appearance of tunnels or gateways, and life reviews in which individuals reported having witnessed past events in the lives of the dying. Personal interpretations of NDEs and SDEs are remarkably similar as well, as experiencers of each have commonly interpreted them as spiritual in nature and the results of a spirit detaching from a body. What ultimately distinguishes NDEs from those experiences listed on SELE is that NDEs do not include the actual, irrevocable death of a human being; they do not conform to the theme of experiencing the death of another, nor are they experienced by someone who is not nearing death themselves. Still, the similarities between NDEs and SDEs are intriguing and warrant further study.
Shared death experiences typically occur right around the time of death, but some are reported to occur moments, hours, days, or even weeks before or after a death. One participant shared the following experience that had occurred on the night of her mother’s death: “I woke up and the room was just filled with this extreme light. I could feel that my mother was close and was coming to say goodbye. She was in the room, but not with a body. It sounds impossible, but she was there, and she was telling me that she loved me but there were no words said. It was like it was all telepathic communication. Time didn’t exist in this realm. I say ‘realm’ because suddenly the walls and the ceiling and everything was crooked or somehow off. The law of physics didn’t abide. She slowly went upwards into the so-called ceiling. Behind her, I could see this being of light that was making the whole room shine. My mom invited me up to this being that was complete love, complete knowledge, complete compassion. It was all those things. I acknowledged that it must be a divine being of some kind. We went to this black void. There I felt the presence of other souls. The strangest thing! We were floating around in this realm, and every question I ever had was answered in some strange way. What was also extremely strange was that I felt connected with the souls around me and this divine being and my mother. I felt like we were one. I didn’t want to leave but I understood that my mother was going further. I couldn’t go with her. I was just visiting, and I had to go back. The next thing I remember is being woke up the next morning from the phone call from hospice telling me my mother had died, which I was perfectly aware of.”
Direct Post-Death Communication
Direct post-death communication consists of experiences in which persons feel that they are in direct mental contact with a recently departed loved one (e.g., Daggett, 2005). Such experiences most often occur immediately or shortly after a death, and they may continue for days, weeks, or sometimes even months. One participant shared the following: “The first few weeks after my grandmother died, I was constantly talking with her. It started immediately after she died. I felt like I could really hear her voice, like she was so there. The day that she died. . . so, they lost Jenny, which was their eldest. . .it was the most painful thing that had happened to our entire family. My only question to her was, ‘Did you see Jen?’ And she said to me, so vividly, ‘If I had known how close she was this whole time, I wouldn’t have been so sad.’ And it was so strong that night! It was just so clear. I remember continually trying to ask her questions to see if it was me answering, like I was doubting myself that this was really her. In the very beginning, it was clear, I was like, ‘No, that’s her. She said it. That’s amazing.’ Then, as time went on, I’d say, ‘Grandma,’ and then I’d start a question. In the very beginning, the answers were just there. It was just, she was there. Then, as time went on, she wasn’t anymore. There was no response. Before, with her tone, I could hear her voice, I could sense happiness. I couldn’t really see her, but I sensed her behind me, and I felt just happy.”
Post-Death Synchronicities
Post-death synchronicities are experiences in which seemingly random events or coincidences are understood to be signs or messages from the deceased (Todaro-Franceschi, 2006). Post-death synchronicities may appear shortly after a death, and they may continue for days, weeks, months, or even years (thus moving from the category of an ELE and into the category of additional after-death communication). Like their pre-death and at-death counterparts, post-death synchronicities are highly interpretive events. A participant who had lost her son shared the following: “Whenever I’m in doubt about different things that might be going on and I’m trying to figure out a solution, it never fails. I’ll be driving along, and I’ll think, ‘Maybe this is the right solution,’ and if I see a red Toyota Tacoma truck coming in the opposite direction or if I see one right in front of me, this is [her son’s] truck, and I know right away that I’m making the right decision. He sends me these signs all the time, and so that communication to me is huge. I put a lot of credence in what I get from him, and he never has steered me wrong.”
Post-Death Visions and Visitations
Post-death visions and visitations consist of consist of seeing, hearing, smelling, or otherwise sensing the presence of a deceased person (e.g., Grant et al., 2014). These experiences may occur shortly after a death or may manifest days, weeks, or even months following a death. One participant shared the following, which transpired shortly after his mother’s death: “I went to the cemetery to visit her grave, knowing of course there’s no spirit there per se, but I went to it out of respect, and there were flowers all over the place. I mean, it was just completely covered, and so was my father’s. I knelt down between the two graves with my left hand on my mother’s grave and my right hand on my father’s grave. It dawned on me then that they were passed. Both of them are gone. That connection is gone. I felt a hand on my left shoulder. It was my mother. I felt a hand on my right shoulder. It was my father. It was quite a moment. I rejoiced at that, and I asked that if they got together very often or not because I was curious about that aspect. I was told no, but this was a special occasion. It was the only time in my life that I really truly felt I was in a family, that my natural mother, my natural father, and son were all together.”
Additional After-Death Communication
Additional after-death communication (ADC) consists of any experiences in which individuals report seeing, sensing, or otherwise communicating with a deceased person after approximately 1 year after that person’s death. As such, they are no longer considered by SELE to be end-of-life experiences. ADC may be an ongoing extension of earlier ELEs, cultivated by certain practices, or occur spontaneously (Hardoin et al., 2007). These kinds of experiences are a significant component to the Continuing Bonds model of grief, which is discussed below in the section “SELE as Therapeutic Aid.”
Discussion
Limitations of Study
Most of the participants in this study were from the United States, though we also had participants from Spain, Scotland, England, France, Germany, New Zealand, Australia, Norway, and Canada. Participants reached out to us after having come across our work, and so there is an obvious bias in our research. Several participants stated that they had decided to share their experiences with us because they felt safe and supported by us, and some participants said they wanted to learn more about end-of-life experiences. Direct end-of-life experiences are likely encountered by caregivers and loved ones of dying patients throughout the world, but we know relatively little about how these experiences are interpreted and described among different sociocultural populations. We assume these kinds of end-of-life experiences are underreported in modern Western culture due to concern that these experiences will be dismissed, discounted, or disparaged. Though biased, we hope that this study will nonetheless advance investigations into the varieties of end-of-life experiences.
With regards to the seemingly high percentage of participants (80.4%) reporting more than one ELE, we are not certain whether or to what degree various intrapersonal, interpersonal, intragroup, and intergroup forces play in either experiencing or reporting ELEs. Perhaps there is a personality type more predisposed to ELEs, or perhaps the effects of ELEs make an individual prone to additional similar experiences. We did find that 100 participants (69.9%) reported having had a regular meditative or mindfulness practice at one time (though not always before an ELE), and this may be a significant correlation to explore in future studies. We also observed that the majority of participants (55.2%) identified as “spiritual not religious,” and many had gravitated towards New Age spirituality as a readily available interpretive framework that identifies ELEs as spiritually transformative events (Shared Crossing Research Initiative, 2021). It remains uncertain whether SELE in its current form can fully account for a cross-cultural continuum of end-of-life experiences.
Below we discuss some possible applications of SELE. We see the primary value in SELE as helping to raise awareness about ELEs and to normalize these experiences; as such, we also think SELE has considerable utility in medical and therapeutic contexts.
Spectrum of End-of-Life Experiences (Types of Pre-Death End-of-Life Experiences) as Prognostic Aid
Researchers have mentioned that certain aspects of end-of-life experiences, namely the occurrence of dreams of traveling with deceased loved ones, may be prognostic signs of an impending death (Grant et al., 2014). Just as Frederic Myers noted a steady increase of apparitions in the days and hours before a death, contemporary researchers have also noted increased frequency of end-of-life experiences as death nears (Dam, 2016). One study of rural and urban Indian hospice patients noted a positive correlation between the incidence of end-of-life dreams and visions and increasing symptom burden (Dam, 2016). Corroborating studies from New York to India suggest cross-cultural validity of this finding (Ibid.; Grant et al., 2014). Other pre-death ELE types, such as terminal lucidity, are also identifiable by workers in end of life; for instance, nurses have observed that the sudden lucidity of patients who are confused or who have dementia often signals an impending death (Brayne et al., 2008; Osis & Haraldsson, 1977).
There is a wealth of unofficial or folk knowledge shared among hospice and palliative care workers and volunteers regarding ELEs. For instance, the manner in which patients interact with unseen beings and/or objects, as well as the identity of those beings and/or objects, may all signify that death is near. Dr. Martha Jo Atkins, the Executive Director at Abode Contemplative Care for Dying in San Antonio, Texas shared with us the following: “Somebody said to me the other day, ‘Are all those buildings out there y’all buildings?’ ‘Everything inside the fence is ours,’ I said. She said, ‘Oh, that bridge is so beautiful.’ We don’t have a bridge in our backyard. I love that imagery. Eventually, she began to see things inside the house. If people do see things, it’s outside to inside. They hear things outside. Then, people begin to come in. I call them friendlies. . . these are really common experiences that I watch for, and my staff watches for. They’re not predictors. I can’t say because someone saw a bridge that they’re going to die two days. It does tell me that she’s on the path.”
Dr. Atkins also shared another indicator that death is nearing, which is the way that people physically react to and reach out for visions: “It happens a lot, the reaching. They’re seeing something, and they’re reaching towards something. As they’re farther in the trajectory, they’re reaching towards the end of the bed like somebody is standing there. Then, eventually, they’re reaching up. And you’re seeing them [track] midway around the room. Then, it’s this [looking directly above]. There’s a difference in their eyes. There’s a difference in their countenance. There’s a difference in intensity.”
Although the appearance of ELEs cannot predict the exact time that death will occur, as we have discussed, their appearance, frequency, and qualities do usually indicate nearness of death. Given these findings, we propose that the presence of pre-death ELEs be included in standard tools used to assess the trajectory and needs of those approaching the end of life in healthcare. For example, many hospice agencies utilize the Palliative Performance Scale (PPS) as a tool with which to determine whether a patient qualifies for hospice care (Anderson et al., 1996). The PPS includes five “observer rated” domains: ambulation, activity and evidence of disease, self-care, intake of food, and levels of consciousness. We suggest the inclusion of a sixth domain titled “End-of-Life Experiences.” This would be the only column to potentially document an observed increase in “activity” (ELEs) as an individual nears death (all current columns document observed decreases in activity of the body and conscious mind). The registered nurse or observer could ask the patient and family if they had had any meaningful dreams, visions, or unusual occurrences since the last visit, and replies could be interpreted and documented. In contrast to the PPS as a generalized observer-rated scale, standard hospice qualifications also include specific clinical indicators (such as “Identifying a Primary Hospice Diagnosis”); here the inclusion of “Appearance of Pre-Death ELEs” could be quite useful in supplementing the clinical findings as an indicator of the appropriateness of transitioning to hospice care. In these examples, the clinical presence of pre-death ELEs can serve as an additional marker in the assessment of patients for accelerating end of life healthcare needs or transitions in care; it can also provide other members of the care unit with a safe and supportive opportunity to report ELEs and talk with specialists, should they wish. We think this is an intriguing path for future directions.
Spectrum of End-of-Life Experiences as Therapeutic Aid
Caregivers and loved ones can be deeply affected by ELEs; individuals may find these experiences so profound as to completely realign their worldviews to accommodate their experiences (Tedeschi & Calhoun, 2006). People who have had ELEs are often convinced that consciousness continues beyond death, that their departed loved ones are, in effect, “still alive and well,” and that they will eventually be reunited. Researchers have commented that many medical professionals are not comfortable with the subject of ELEs and tend to avoid the topic or to dismiss ELEs as nothing more than subjective hallucinations (Lawrence & Repede, 2013; Nosek et al., 2015). However, these are not effective strategies to successfully support individuals in processing and integrating these experiences. Rather, professionals working with caregivers and loved ones who report ELEs must be comfortable with discussing both individuals’ experiences and the meanings that people have attached to them for full integration.
One particularly useful way to work with individuals reporting ELEs is found within an aspect of contemporary grief counseling known as Continuing Bonds: this is a model of grief whereby individuals redefine rather than terminate their relationships with deceased loved ones (Klass et al., 1996). Counselors and therapists working within this model approach the ontological status of post-death experiences with openness and flexibility, and they are sensitive to the fact that to dismiss outright the objective reality of ELEs and ADCs for clients who have had them may lead to alienation (Hayes & Steffen, 2018). At present there is growing interest in the overlap between Continuing Bonds griefwork and after-death communication (Klass & Steffen, 2018).
In modern Western culture, individuals deeply impacted by ELEs tend to move away from organized religion and toward an individualized spirituality, new age spirituality in particular (Kinsella, 2017). There are several reasons for this. First, new age spirituality is non-dogmatic, highly idiosyncratic, and privileges personal experience (Albanese, 2007; Bender, 2010). Second, new age spirituality is one of the few Western meaning-making systems to explicitly focus on end-of-life experiences and to accept them at as objectively real events (Kinsella, 2017). Third, new age spirituality attempts to merge science and spirituality together, which can effectively serve as a bridge between the materialistic and the transpersonal (Hanegraaf, 1996). Fourth, the varied practices of new age spirituality generally consist of small group workshops and therapeutic dyads which tend to conform well to the needs of the grieving and bereaved (Taves & Kinsella, 2013). And fifth, new age spirituality actively supports individuals in reexperiencing or reproducing the effects of ELEs, whether it be through guided visualizations or through seeking the assistance of psychics and mediums (Beischel et al., 2018). As such, those who work with individuals reporting ELEs should be sympathetic and appreciative of how this meaning-making system is especially useful for individuals operating within the contemporary Western materialist paradigm. Professionals working with individuals reporting ELEs should also be aware that ELEs—like other extraordinary human experiences—often have different meanings across different populations, groups, and cultures (i.e., Belanti et al., 2008; Taves, Barlev, & Kinsella 2017). Not least of all, professionals should take care to prioritize therapeutic benefits over ontological certainty.
The Spectrum of End-of-Life Experiences identifies the known spectrum of commonly reported end-of-life experiences, effectively normalizing these experiences without adhering to any particular worldview or belief system. By identifying specific ELEs according to general phenomenological characteristics, individuals are better able to view these experiences as natural (and non-dogmatic) aspects of death and dying; this is precisely why SELE is an especially valuable tool in a therapeutic context. Once the social stigma of discussing these experiences is removed, a major hurdle faced by individuals who report them is overcome. Within hospice, bereavement services are required by Medicare for a minimum of 13 months following a patient’s death. We suggest that the use of SELE coupled with a Continuing Bonds model of grief would be especially therapeutic for bereaved survivors struggling to discuss, process, and integrate these experiences in a safe and supportive environment.
Spectrum of End-of-Life Experiences as Educational Guide
Increasing general awareness about ELEs would go far in preventing the alienation that can often arise from perceived social stigmas attached to the reporting of these experiences. Educating the public about these experiences and their common aftereffects does not translate to accepting any one viewpoint or belief regarding them; it does, however, mean, that the beliefs individuals have regarding their experiences would be better understood. As far as informing behaviors related to death and dying, raising awareness about ELEs would better allow loved ones and caregivers of the dying to take advantage of opportunities to share in these experiences more fully and readily. Oftentimes pre-death experiences are misunderstood, as in cases where pre-death visions and visitations are viewed as delirium (Depner et al., 2020) or in instances where family members of a dying patient fail to recognize terminal lucidity as an indicator that death is close and instead assume that the dying patient is beginning to miraculously improve (Chiriboga-Oleszczak, 2017; Nahm, 2017), thereby risking the introduction of aggressive medical treatment. Raising awareness of the former as deeply meaningful experiences for the dying and the latter as a window of opportunity to say “farewell” would go far in alleviating potential concerns and would better prepare individuals for any possible manifestation of these experiences. Again, once these experiences are understood to be naturally occurring phenomena, the less they will be viewed as aberrant, deviant, or frightening. In fact, when accepted on their own terms, ELEs can be highly therapeutic and life affirming.
Conclusion
Regardless of how a person comes to interpret or construct meaning out of ELEs, these experiences occur, and they occur among caregivers and loved ones as well as among the dying. Seemingly a natural part of the dying process, the modern Western world has nonetheless placed these experiences at the margins of supernaturalism. We suggest it is time to move these experiences directly into general death education. To do so would provide better care and support for dying patients as well as their caregivers and loved ones. We argue that it is critical to move research into the entire spectrum of ELEs forward, and we envision the inclusion of SELE in death education and healthcare as a move towards more compassionate and holistic attention to the entire care unit.
Footnotes
Author’s Note
Individual contributors to the present article include Michael Kinsella, PhD, SCRI Chief of Research, Monica Williams, MD, SCRI Medical Director, and William Peters, MFT, SCRI Founder and Executive Director.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the NoVo Foundation, the J.S. Bower Foundation, and the Natalie Orfalea Foundation.