
Abstract
The study sample consists of participants as the patient, patient relatives, and nurse. In our study, a significant relationship was found between the ages of patients, and fear of death, avoidance of death, accepting approach, non-acceptance, and the DAP-R scale total score. A positive moderate correlation was found between the fear of death and death avoidance among my nurses who participated in the study. The nurse, the patient, and patient relatives had a good perception of death and had a higher attitude toward death. Additionally, that found to nurses’ fear of death and death avoidance behavior are higher than patients and their relatives.
Introduction
Individuals’ death experiences include the death of a friend or family member. The entire family is affected when an individual is in the process of death and death. In studies conducted with individuals whose relatives have died, individual, medical, spiritual, and spiritual factors have attracted attention (Miyajima et al., 2014; Stajduhar Funk & Outcalt, 2013). The relatives of dying patients have good or bad experiences related to the death process. These experiences affect death and mourning processes. Many definitions are made in the current literature on the concept of good death. The importance of well-managed death for patients and their relatives has been emphasized (Cottrell & Duggleby, 2016; Scarre, 2012). Good death is a death in which patients and their relatives are psychologically prepared and their symptoms and pain are under control. Good death includes a combination of factors such as feelings of loss and grief, existential concerns, family and community support, life satisfaction, and hope for a good journey after death (Miyajima et al., 2014; Scarre, 2012). Yun et al. (2018), in their study with the general population, cancer patients, their families, and physicians to identify the components of a good death to have defined three components. These components are defined as “not burdening the family,” “the existence of the family,” and “completing unfinished works.”
Good death is influenced by the factors of the nurse, patient, and patient relatives, and death experiences. Patient factors include the patient’s clinical condition, (diagnosis, treatment, stage of the disease), the patient’s and family’s financial status, and other accompanying health and social conditions (Rainsford et al., 2017; Stajduhar et al., 2013). Nurse-related factors include the nurse’s age, gender, educational background, socioeconomic status, belief status, experience related to death, the ability to speak death, the experience of caring for dying patients, and their attitude toward the care of dying patients (Çevik & Kav, 2012; Koç & Sağlam, 2008; Ceyhan, Özen, Zincir, Şimşek, & Başaran, 2018; İnci & Öz, 2012). In particular, age affects attitude toward death, and this attitude changes with age. As the individual ages, he thinks death as a natural process and experiences more positive emotions in this process. Education is another important variable that affects nurses’ approach to death, such as age. It is stated in the literature that as nurse education status and experience increases, their approach and attitudes toward the dying patient are better and more effective (Anja, Tarja, &Anna-Maija, 2016; Cipolletta & Oprandi, 2014; Çevik & Kav, 2012; Ceyhan et al., 2018; Zheng, Lee, & Bloomer, 2016).
The nurses’ perspectives on good death should include optimal symptom management and holistic care for the patient and family. In the literature, nurses describe a good death as a peaceful but sad event that occurs in a peaceful environment, preferably at the dying person’s home (Anja et al., 2016; Bakanic, Singleton, & Dickinson, 2016; Ceyhan et al., 2018; Scarre, 2012; Zheng et al., 2016). Death without pain is also an important aspect of good and dignified death for nurses; therefore, it is emphasized that adequate pain management is critical during end-of-life care (Cipolletta & Oprandi, 2014; Cottrell & Duggleby, 2016). Anja et al. (2016) surveyed 82 nurses through social media to investigate nurses’ thoughts on good death in Finland. In this study, four categories defined as “respect for one’s autonomy and human dignity in care,” “qualities of a good death,” “preparation for death,” and “contextual aspects of a good death.” The nurses stated that they regard death as a valuable event in which the dignity of the dying person will be preserved to the fullest.
Nurses who care for patients in the process of death must take time to communicate with patients and their relatives. Some of the important nursing interventions that nurses who care for the patient in the death process should help the patient make short targeted plans for the remaining days, review his patient’s past and think about what can be done today, and talk about what he wants to do on behalf of him in the future or after his death. (Bakanic et al, 2016; Çevik & Kav, 2012; İnci and Öz, 2012). However, it is stated in the literature that nurses are insufficient in providing care to patients in the death process and they need to be supported. In a study by Nguyen, Yates, and Osborne (2014) with 251 nurses working in oncology clinics, it was stated that nurses were insufficient in end-of-life patient care, psychological and spiritual care, effective communication, and talking about death. In the study conducted by Çevik and Kav (2012), almost half of the nurses (44.6%) stated that they felt inadequate in communicating with patients and their relatives, 19.6% in pain control, and 17.8% in answering questions about death.
There are many studies in the literature regarding the care of dying individuals and the perception of death by nurses who care for cancer or intensive care patients (Anja et al., 2016; Bakanic et al, 2016; Çevik & Kav, 2012; Cipolletta & Oprandi, 2014; İnci & Öz, 2012; Nguyen et al., 2014; Periyakoil, Stevens & Kraemer, 2013; Zheng et al., 2016). However, the number of studies on thoughts of patients and their relatives about death is limited (Miyajima et al., 2014; Rainsford et al., 2017; Stajduhar et al., 2013; Yun et al., 2018). Yun et al. (2018), in their study with the general population, cancer patients, caregivers of cancer patients, and physicians, have stated that “relief from pain or pain” is an important component that ranks first among good death components. Also, there are no studies including the opinions of patients and their relatives on death in our country. For nurses to provide quality, individualized care to dying patients, they must know and recognize people’s different understandings and a good perception of death. It is also important to discuss the thoughts of patients and their relatives regarding good death. In line with this information, this study was planned to determine the views of cancer patients, relatives, and nurses on death and well-being. It is thought that this study will make a significant contribution to the literature.
Study questions
Within the scope of this study, answers to the following questions were sought: 1. How do cancer patients, relatives, and nurses define good death? 2. What are the attitudes of cancer patients, relatives, and nurses toward death? 3. What are the factors that affect the opinions of cancer patients, patient relatives, and nurses on good death?
Method
Objective
This study determined the perspectives of nurses, cancer patients, and their families toward good death.
Design
This was a descriptive study.
Samples and settings
The study population consisted of patients who were hospitalized in adult-bed clinics and treated in an outpatient chemotherapy outpatient clinic, primary caregivers of these patients, and nurses providing care to cancer patients working in these clinics. The research was carried out between July 15, 2018,andDecember 01, 2018. The study sample consisted of 100 nurses, 100 cancer patients, and 100 patient relatives who agreed to participate in the study. The inclusion criteria were as follows: a bachelor’s degree, care for a cancer patient, and willingness to participate in the study. Patients in the study were included in patients who were diagnosed with cancer for at least 1 year, who were over the age of 18, could read and write, and could communicate verbally, volunteered to participate in the study. In our study, as the relatives of the patient, family members who meet the patient’s care needs while staying in the hospital and stay with him as a companion is accepted. Family members included spouses, fathers, mothers, children, and siblings. The inclusion criteria of relatives of the patient were to be over the age of 18, who could read and write, and who could communicate verbally, volunteering to participate in the study
Data Collection Tools
The data were collected using the literature, “Nurse, Patient and Relatives of Patient Information Form,” “Death Attitude Profile (DAP-R),” and “Good Death Scale.” The nurses, patients, and relatives of patient information forms were developed by the researchers based on the literature review. With the information forms were collected the demographics characteristics of the nurses, patients, and their relatives and their thoughts on death and good death. The information form in each group included everyone their age, sex, marital status, and education. For nurses, the information form includes work experience, the experience of caring for a dying patient, training for a good death, thoughts on good death, and preference for the place of death of cancer patients. The patients and family members included occupation and monthly income. For patients, health insurance, duration of cancer, type of treatment, family support, place of living, and preference for the place of death (home, hospital, or I do not know). For family members, information form includes the relationship with the patient, the participation of other family members, the length of care for the cancer patient, the experience of having other relatives with cancer, the experience of caring for a dying patient at home, thought of good death, and their preference for the place of death of their patients (home, hospital, or I do not know).
The Death Attitude Profile Scale (DAP-R) was developed in 1994 by Wong et al. The reliability and validity of the Turkish version of the scale was valuated by Çevik and Kav in 2013. Cronbach’s alpha reliability in Çevik and Kav study was .80. In our study, Cronbach’s alpha value of the DAP-R scale was .89 of the nurses, .92 of the patients, .90 of the patient relatives, and .89 of the nurses. The DAP-R is a multi-dimensional scale consisting of 32 items. The DAP- R scale contains Likert scale items scored from 1 (strongly disagree) to 7 (strongly agree). The scale includes five sub-dimensions; fear of death, death avoidance, neutral acceptance, approach acceptance, and escape acceptance.
The Good Death Scale was developed in 2003 by Schwartz et al. to determine the characteristics of nurses on the concept of good death. The reliability and validity of the Turkish version of the scale was assessed by Fadıloğlu and Menekli in 2010. The scale includes 17 questions and three subdimensions. The first subdimension, the psychosocial spiritual subdimension, consists of nine questions and describes the psychosocial and spiritual aspects of death. The second subdimension, the personal control subdimension, consists of three questions and describes mental concentration, communication ability, and physical functions. The third subdimension, the clinical subdimension, consists of five questions and describes the medical and clinical aspects of death. Each statement in the scale was evaluated by a quartet Likert-type grading system as none (1), some (2), mild (3), and much (4). The total score ranged from 17 to 68. Reliability increases as the scale score increases. The Cronbach’s alpha reliability in Fadıloğlu and Menekli’s study was .91. In this study, Cronbach’s alpha value of the good death scale was .91 of the nurses, .90 of the patients, .81 of the patient relatives.
Data Collection
Before data are collected in the study, nurses, patients, and patient’s relatives were informed verbally and in writing and their consent was received. Data forms were collected over 2 months due to the nurses' intense working conditions. When determining the patients, help was obtained from the nurse responsible for the clinic. The patient’s room was entered and interviewed. The purpose of the study was explained to the patients who provided the sample conditions and agreed to participate in the study. Patient data were collected by either the patient or the researcher reading the patient and marking the patient’s response to the forms. Patients who marked the research questions themselves filled the form within approximately 30–45 minutes. When the forms were filled with the help of the researcher, it was completed on an average of 45–55 minutes. Patient data were collected over 5 months. To determine the relatives of the patients, family members who were accompanying their patients were interviewed during the patient visit hours. The purpose of the research was explained to the family members who complied with the sample criteria and agreed to participate in the study. The relatives of the patients filled the data forms within 35–40 minutes. Data were collected from patient relatives for over 5 months.
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS/22.0 for Windows). Descriptive statistics were expressed as mean, SD. The suitability of the data for the normal distribution was used with the Shapiro–Wilk test and Student’s T-test was used to compare the two independent groups. Mann–Whitney U test was used to compare non-normally distributed properties between two independent groups. One-way variance analysis test (ANOVA) for properties with a normal distribution in comparison with more than two independent groups, and the Kruskal–Wallis test for non-normally distributed properties. Spearman Pearson correlation analysis was performed. In our study, statistically significant was set at p < .05.
Ethical Considerations
The study was approved by the Ethics Committee (2018–2207). Permission was obtained from the institution. Informed consent was obtained from a nurse, cancer patient, and patient’ relatives before the study.
Results
The mean age of nurses was 29.01 ± 6.65 (minimum 22; maximum 54) and 66% of the nurses are in the 22–28 age range. Almost all (%94) were female and 64% were single 94% were university graduates. Thirty six percent of nurses had 0–1 years of experience working. A total of 79% of the nurses received end-of-life care training. Fifty four percent of the nurses stated that the end-of-life education they received was insufficient. Ninety eight percent of the nurses stated that they had encountered death before.
There were 100 cancer patients (42 men, 58 women) with a mean age of 50.60 ± 13.13 years (minimum:23–maximum:82). Of these, 85% were women, 78% were married, 44% had a high school diploma, and 41% were housewives. A total of 47% of the patients live with their spouse and children and 79% of them live in the city center. 63% of the patients were diagnosed with cancer between 0and 1 year. More than half of the patients (58.2%) received chemotherapy. In addition to cancer diagnosis in patients participating in the study (28%), hypertension, diabetes, coronary artery disease, chronic kidney failure, and hypothyroid disease.
There were 100 cancer patients (40 men, 60 women) with a mean age of 45.25 ± 13.6 years (minimum:20–maximum:78). A total of 60% of patients’ relatives were women, 72% were married, 37% were high school, 31% were university graduates, and 39% were housewives. In the study, 50% of patient relatives lived in the same house with their patients and 84% lived in the city center. Hypertension in 35.7% of patients’ relatives, diabetes mellitus in 27.6%, cardiovascular disease in 16.5%, and 18% had thyroid disease COPD, acute renal failure. Almost all (92.4%) of patients' relatives received treatment related to their diseases.
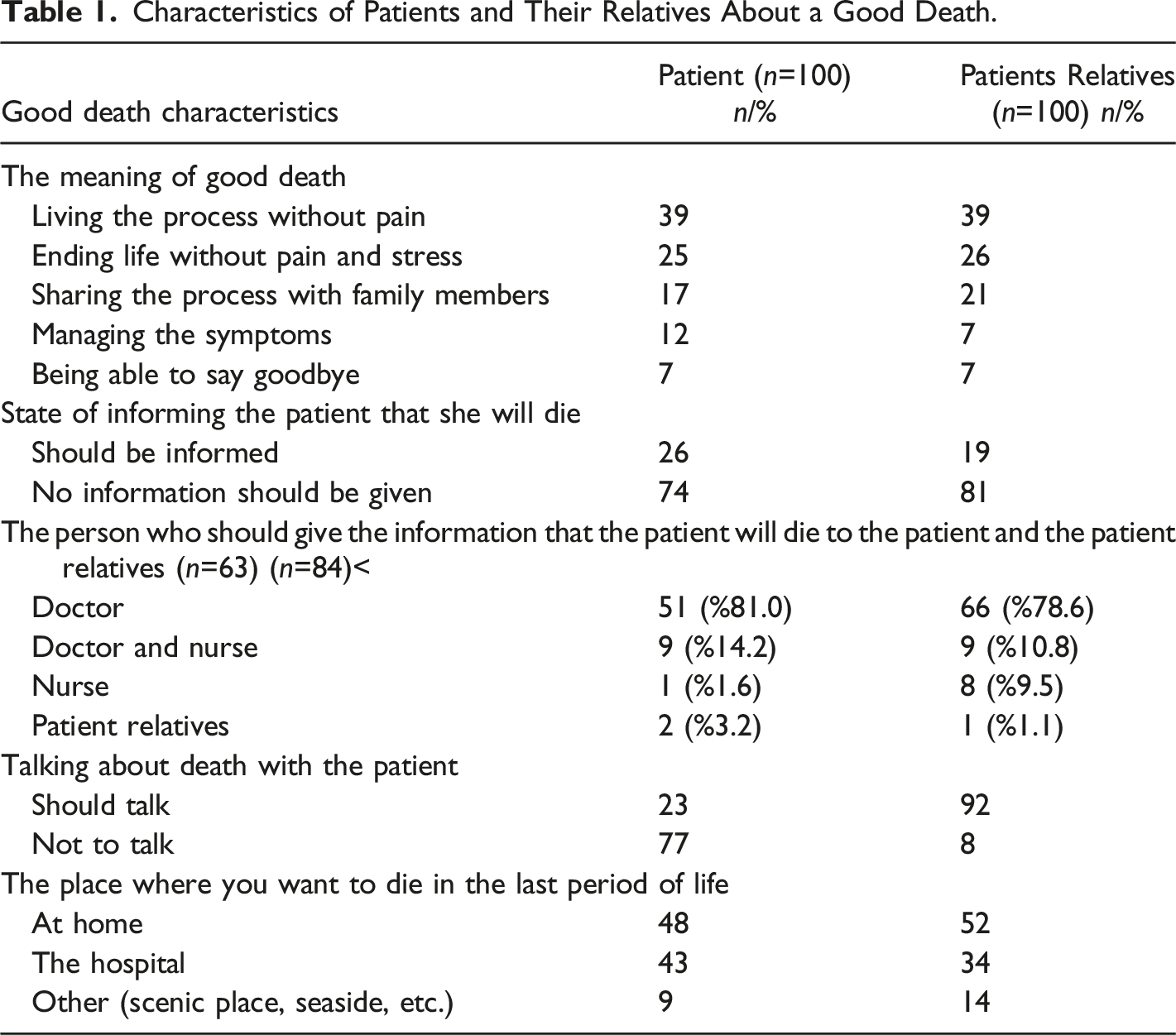
Characteristics of Patients and Their Relatives About a Good Death.
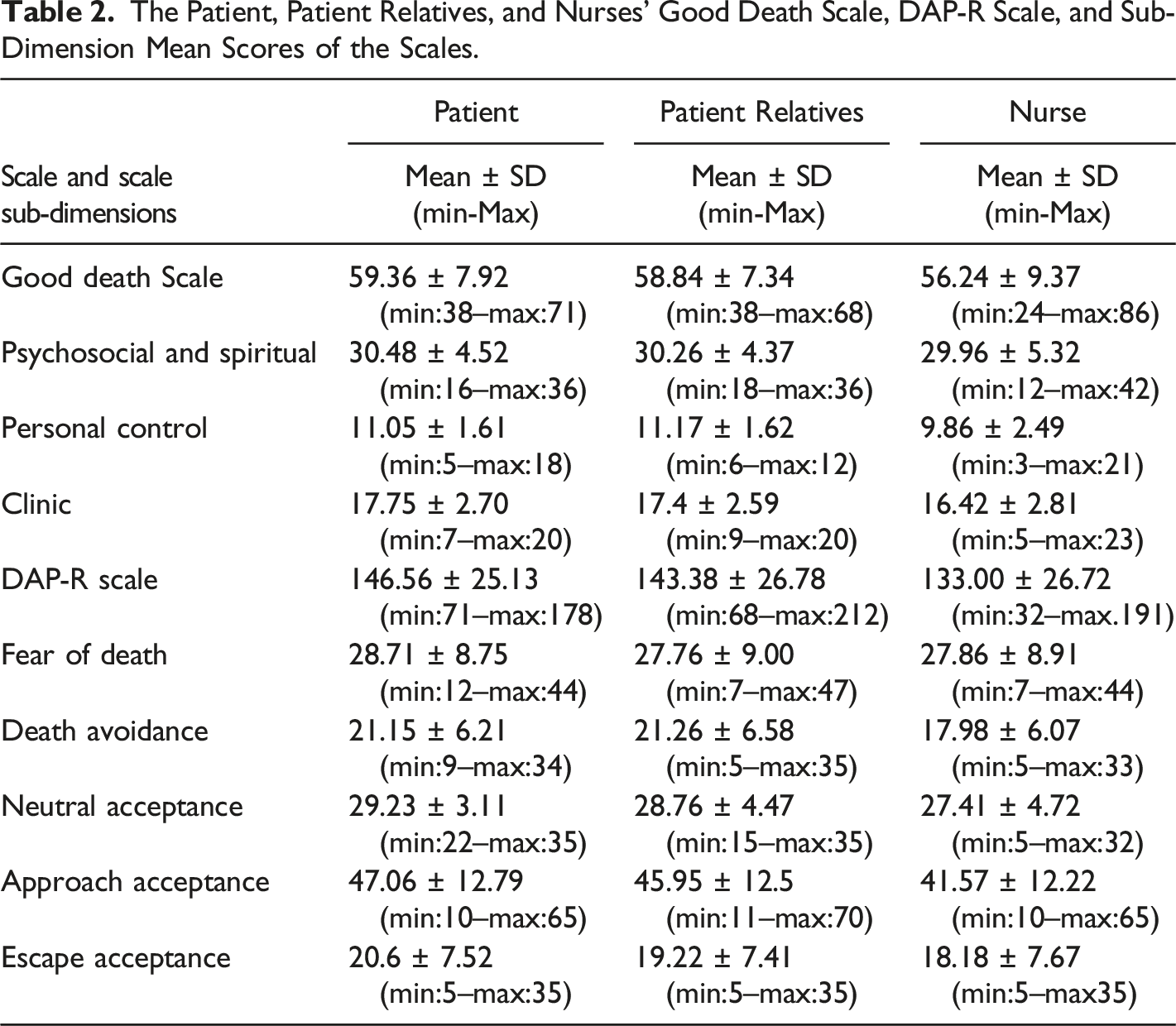
The Patient, Patient Relatives, and Nurses' Good Death Scale, DAP-R Scale, and Sub-Dimension Mean Scores of the Scales.
Nurses’ Characteristics and DAP-R Scale and DAP-R Scale Subgroup Mean Scores.
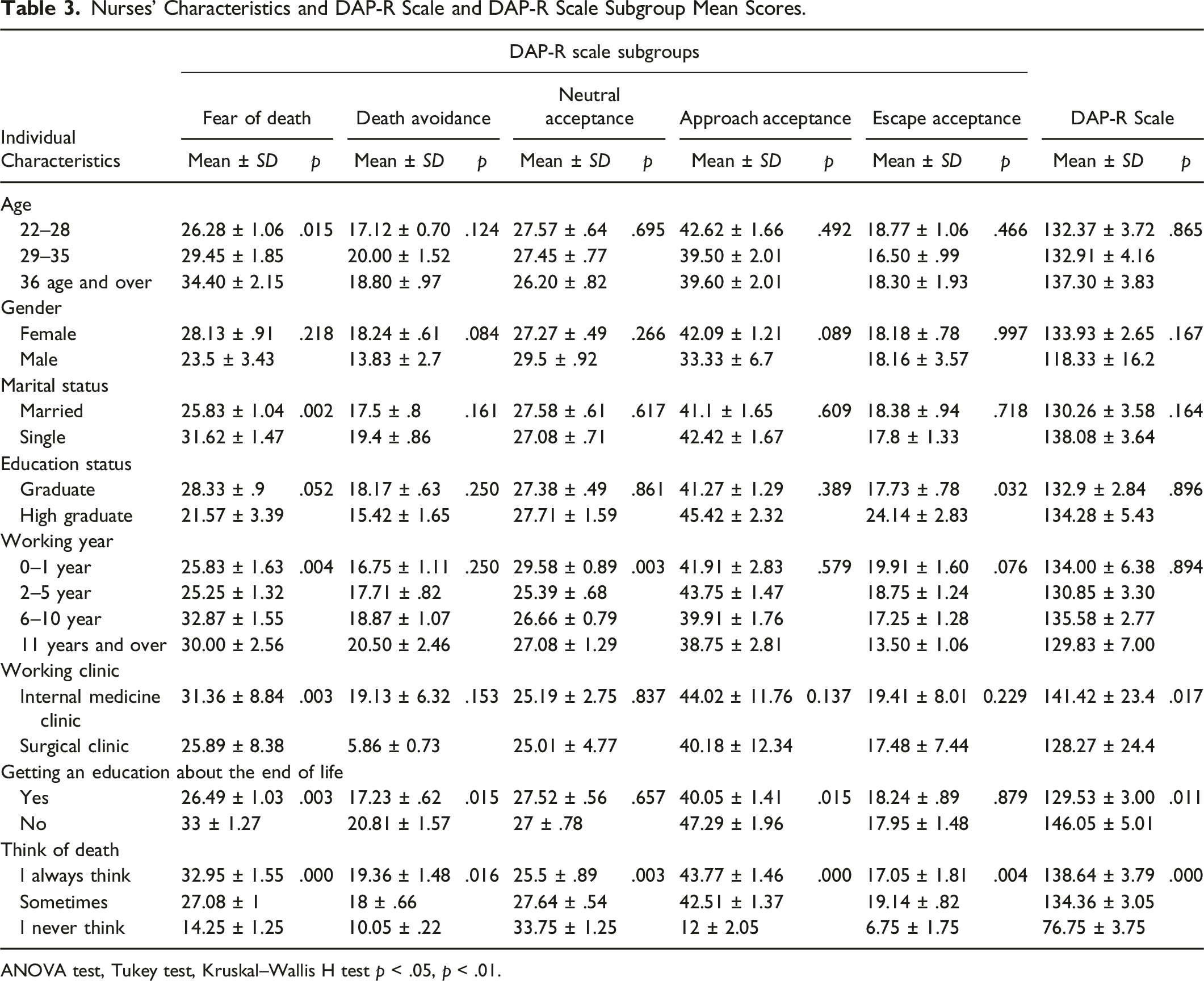
ANOVA test, Tukey test, Kruskal–Wallis H test p < .05, p < .01.
The personal subdimension mean score of married patients was higher than single patients. The total scale score of patients living with their spouses and children was significantly higher than those living alone with their parents and spouses. Patients who lived alone had the lowest mean good death scale score. Good death scale scores, psychosocial sub-dimension, personal dimension, and clinical dimension score averages of the patients who want to die in the hospital were significantly higher than those who want to die at home and in different settings (p < .05).
In our study, a significant relationship was found between the age of patients, and fear of death, avoidance of death, accepting approach, non-acceptance, and DAP-R scale total score. In our study, the fear of death score of patients in the 45–55 age group was found to be 30.55 ± 1.45 and was significantly higher than other age groups (p < .05). The accepted approach, non-acceptance, and DAP-R scale mean scores of the married patients are higher than the single ones and are significant. In this study, the fear of death and death avoidance score averages of patients who did not want to hear the information that they would die was found to be higher than the patients who wanted to learn the death information. (p < .05). The DAP-R scale mean scores of the patients who willing to die at home were higher than the average scores of those who willing to die in the hospital or other places. The difference was statistically significant. (p < .05).
The average psychosocial score of patients living in the city center (30.73 ± 0.47) was found to be higher and statistically significant than those living in the district (27.73 ± 1.08) and those living in the village (29 ±.) (p < .05).
It was found that as the fear of death score of patients participating in the study increased, their avoidance and neutral acceptance scores decreased. There was a moderate negative relationship between fear of death and death avoidance between strong fear of death and neutral acceptance (r = −.758, p = .000 < .05; r = −.539, p = .000 < .05). A low positive correlation was found between the good death scale of the patients and the DAP-R scale (r: 0.214, p = .041 < .05). Accordingly, as the patients’ good death score increased, the score on the attitude profile scale increased slightly.
The mean death avoidance score of the patients’ relatives between the ages of 33–47 was higher than in other groups (p < .05). The mean death avoidance score of the relatives of young and old patients was lower. The fear of death points of the relatives of married patients was 28.86 ± 1.02 which was 24.93 ± 1.87 times higher than the mean score of death fear of single people. The average death avoidance score of married people was 22.32 ± 0.72, and the average death avoidance score of single people was 18.54 ± 1.35, and this difference was significant (p < .01). The mean score of the death-accepting approach was 46.45 ± 1.31 for patients living in the city center, 44.6 ± 3.41 for those living in the district, and 13 ± .02 for the people living in the village. In advanced analyses, it was found that this relationship was between the province and the village in the approach of accepting death. The averages acceptable approach score of the patients living in the province was higher. In this study, there was a moderately positive correlation between the fear of death of patients’ relatives and death avoidance (r: .611, p < .001). As the death fear of the patient relative increases, the mean of avoiding death increases. A strong positive correlation was found between the acceptance of death and acceptance of the death of patient relatives (r: 0.856, p < .001). A weak positive correlation was found between the DAP-R scale and the good death scale of the relatives of the patients (r: 0.402, p < .001).
The Distribution of Good Death Scale and Scale Subgroups of Patients, Patients' Relatives and Nurses.
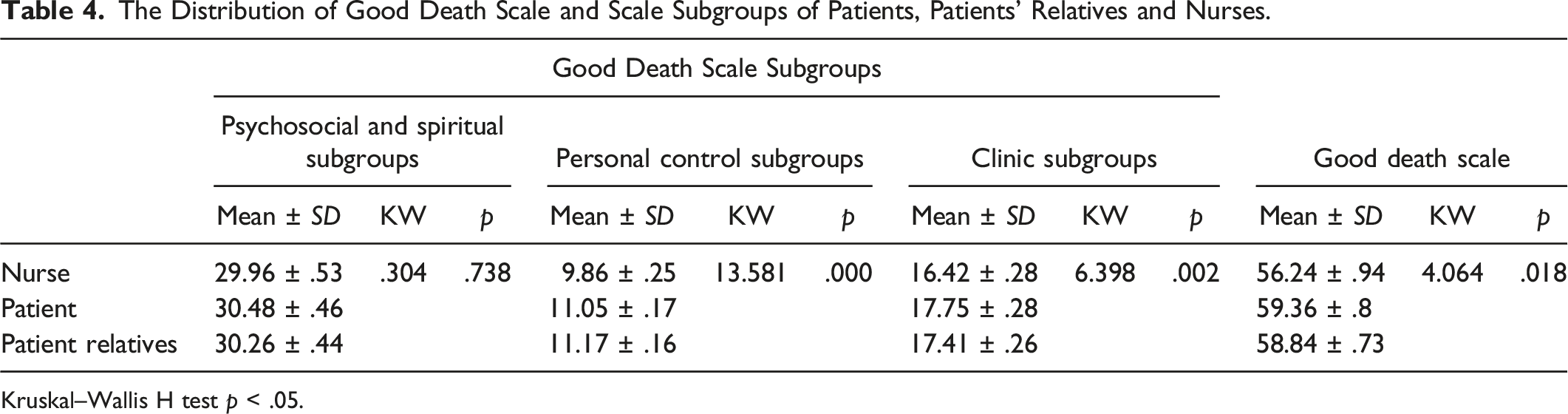
Kruskal–Wallis H test p < .05.
The Distribution of DAP-R Scale and Scale Subgroups of Patients, Patients' Relatives and Nurses.
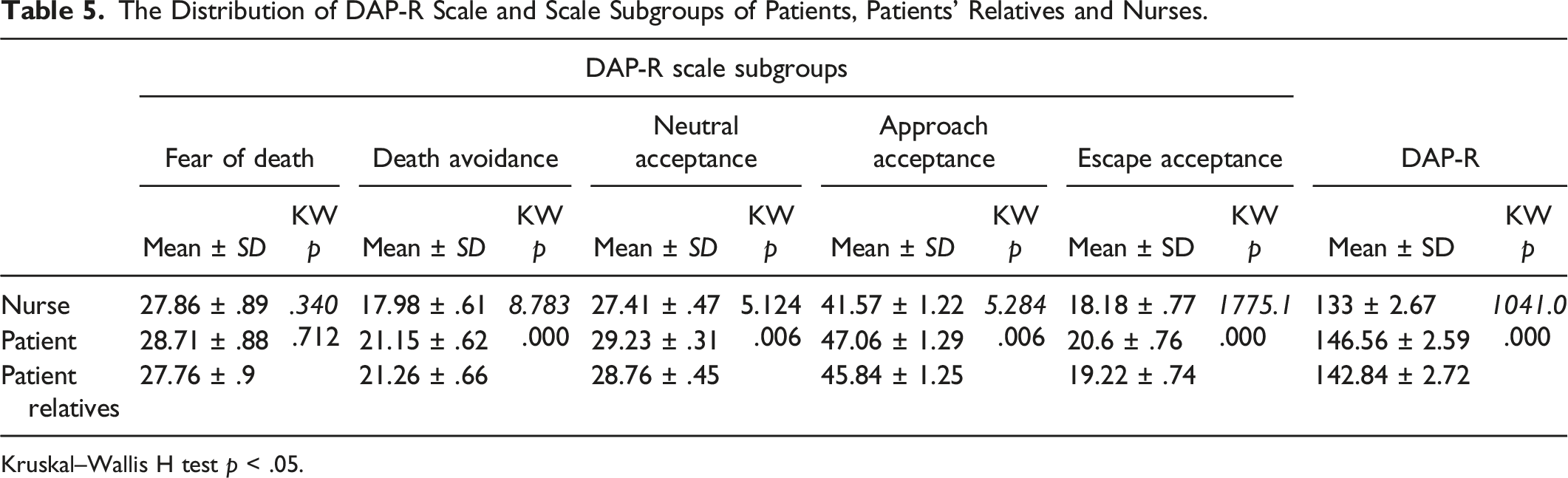
Kruskal–Wallis H test p < .05.
Discussion
Death fascinates us, and most of us hope for a good death. However, what is a good death? Previous studies of what constitutes a good death have shown that the concept is complex and that a good death cannot easily be defined in general terms. There may be the same or different opinions between the views of what patients and nurses perceive as a good death. However, there are some recurrent themes in terms of what would be considered a good death from the perspective of patients having cancer. These include pain and symptom management; preparation for death, decisions about treatment preferences, the importance of family, and being treated as “a whole person.” (Granada-Cameron & Houldin, 2012; Steinhauser, Christakis, & Clipp., 2000; Volker & Wu, 2011; Yun et al., 2018). The results of this study bear some similarities to the literature on good death. In our study, patients and their relatives defined good death as “dying without pain,” “ending life without pain and stress,” “being with their families,” “managing death symptoms,” “and “saying goodbye to loved ones.” In the study of Yun et al. (2018), it was stated that they define the concept of a good death as cancer patients “not being burden with the family,” “being with the family,” finishing the unfinished works, “no pain and suffering.” In the same study, relatives of patients expressed good death as “dying without burden and pain in the family” (Yun et al., 2018). In another study, most cancer patients defined good death as “ending life without pain.” Similar to our study, in the literature, patients define good death as “removing pain, not suffering, not burdening their relatives” (Rainsford et al., 2017).
Nurses defined good death as “dying without pain and suffering.” In a study conducted with 82 nurses in Finland, it was stated that nurses defined good death in four categories. These categories are “respecting one’s autonomy and human dignity,” “the quality of good death,” “preparing for death,” and “content of good death.” In the same study, nurses defined the concept of a good death as “making little pain, making their own death decision, dying naturally without any intervention” (Haishan et al., 2015). In another qualitative study conducted with 15 nurses working in the intensive care unit, three themes related to good death were determined. These three themes are “not dying alone,” “dying without suffering,” and “acceptance of death by patients and their relatives” (Bratcher, 2010).
One of the important components of a good death is dying without pain or suffering. Patients’ relatives and nurses frequently expressed “pain and painless death” by the literature while defining good death. However, an important component of a good death is desire to die at home. (Rainsford et al., 2017; Stajduhar et al., 2013; Yun et al., 2018). In our study, almost half of the patients stated that they wanted to die at home, and more than half stated that they preferred to die in the hospital. More than half of the patient’s relatives of the loved one stated that they preferred their loves ones to die at home. Similar to our study, studies in the literature show patients too often wish to die in hospitals, in contrast to their wish to die at home. This may be because families prefer a more skilled medical environment, or patients may want to save family members the burden of care at home even though they want their loved ones present; however, in some studies in the literature, relatives of patients want their loved ones to die at home. In a study, Japanese patient relatives were stated to prefer home for the death of their loved ones (Choi et al., 2010). In a study conducted to determine the preferences of the place of death in Taiwan, it was stated that the relatives of the patients preferred their patients to die at home as the place of death (Tang et al., 2005) which is thought to stem from the cultural characteristics of patients’ relatives and their previous death experiences.
A good death is influenced by individual characteristics, education, personal experience, and culture. In our study, no significant relationship was found between the patients’ good death scale and the patients' age, education, gender, occupation, disease diagnosis, duration of diagnosis, and treatment received. (p > .05). Yao et al. (2007) stated that there was no significant relationship between the gender of the patient and the good death scale. Yun et al. (2018) in their study determined the perceptions of patients, relatives, and physicians about good death; they stated that there was no significant relationship between the education level of the patients and the good death scale. In our study, the average score of the Good Death Scale was found to be higher in patients who wanted to die in the hospital. (p < .05). Similar to our study, Yao et al. (2007) stated that those who want to die at home have higher good death scale scores than those who want to die in hospital.
In our study, it was found that the good death scale scores of female patient relatives were significantly higher than men (p < .05) suggesting that women take responsibility for taking care of their patients more than men.
Nurses’ thoughts and attitudes toward good death are influenced by individual characteristics such as age, gender, socioeconomic status, education, and culture. In our study, no significant relationship was found between the individual characteristics of the nurses and their average scores on the Good Death Scale. However, there is a significant relationship between the psychosocial sub-dimension, which are sub-dimensions of the good death scale, and the frequency of thinking about death, and between the clinical sub-dimension and the frequency of caring for the dying patient. This result shows that the psychosocial sub-dimension mean scores of nurses who always think about death are significantly higher than nurses who occasionally think and never think. However, in a study similar to our study in the literature, no significant relationship was found between the perception of good death and frequency of thinking about death (Ceyhan et al., 2018). In our study, a significant relationship was found between the frequency of nurses thinking about death and attitude toward death scale and scale subgroups. DAP-R scale total score, the avoidance of death, the fear of death, acceptance approach mean scores of nurses who constantly think about death are higher. According to these results, it can be accepted that nurses who think about their death frequently have more positive attitudes toward death and good death perceptions. Similar to our study results, Asadpour et al. (2015); Braun et al., (2010); Çevik and Kav (2012); and Wang, Li, Zhang, & Li (2018) reported a significant relationship between the frequency of nurses thinking about death and the DAP-R scale and scale sub-dimensions. In our study, there was no relationship between nurses’ receiving education about end-of-life care and the good death scale, while there was a significant relationship between the scale of attitude toward death. Nurses who received training on end-of-life care had lower averages of fear of death, avoidance of death, accepting approach, and DAP-R scale total scores than those who did not receive training. This difference was statistically significant (p < .05). In the literature, similar to our study, there is a positive relationship between the “neutral acceptance” and “accepting approach” score averages of nurses who have received end-of-life care training. (Gama et al., 2012; Khader et al., 2010; Nguyen et al., 2014).
When we looked at the mean scale scores of the participants regarding good death in our study; the Good Death Scale scores of the patients were found to be higher than their relatives and nurses. The mean scores of good death in the nurses, patients, and patient relatives were 56.24 ± 0.94, 59.36 ± 0.8, and 58.84 ± 0.73, respectively. The difference was statistically significant (p < .05). The results show that even though nurses offer end-of-life care, perspectives of a good death are lower than the patient and the patient relatives, and the patients have more positive thoughts about a good death. In other words, this result shows that patients indicated more importance to the concept of good death and believe that death can be good. The other reason for this result may be that the nurses are younger than the patients and they do not have a disease with high mortality such as cancer, and it is that the person whose death is imminent wants her death to be well painless and comfortable. The mean score of DAP-R in the nurses, the patients, and the patient relatives were 133 ± 2.67; 146.56 ± 2.59; 142.84 ± 2.72, respectively. The difference was statistically significant (p < .05). In our study, this result shows that the patients' good perception of death, their attitude toward death, and acceptance of death are better than patients and nurses. In the literature, individuals have more positive attitudes towards death as age increases. In our study, no significant relationship was found between good death perceptions of patients, relatives and nurses, and age. A significant relationship was found between the age of the patients and the DAP-R Scale, fear of death, accepting approach, and acceptance of death among the scale subgroups. The mean scores for the fear of death of the patients who are young and over 65 were lower than other age groups. Among the patients, the age group with the highest fear of death is the 34–44 age group and the 45–54 age group. Looking at the approaches of patients to accept death, the average score of the patients aged 67 and over is the highest and the 22–33 age group is the lowest. It was observed that as age increased, patients displayed more positive attitudes toward death. There is a significant relationship between age, fear of death and avoidance of death in patients' relatives. It was observed that the patients in the age group of 59–78 had lower mean scores for fear of death and avoidance of death. A significant relationship was found between the age groups of nurses and the average score for fear of death. It is seen in all three groups that the age group with the highest score for fear of death is between the ages of 30 and 45. The lowest scale score for fear of death was in the advanced age (65 years and over) and young age (20–28 years) groups. These results are consistent with the literature (Çevik & Kav, 2012; Ceyhan et al., 2018; İnci and Öz, 2012; Rainsford et al., 2017; Yun et al., 2018). It can be concluded that the acceptance of death with the advancement of age in nurses, patients, and their relatives has a positive effect on their attitude toward death.
As a result, a feeble positive correlation was found between the perception of good death and the DAP-R scale in all three groups in our further analysis. Accordingly, as the perception of good death by patients' relatives and nurses increases, attitudes toward death become somewhat positive.
Conclusion
In conclusion, our study results showed that the nurse, the patient, and patient relatives had a good perception of death and had a higher attitude toward death. Among the three groups, nurses had the lowest perception of death and attitude toward death. Based on these findings, we recommend that regular and up-to-date training on death should be provided to nurses, and programs that would support their communication skills should be organized. Patients had the highest perception of death and a positive attitude toward death. For this reason, it is recommended to talk to patients about death and to conduct more studies on this subject. Besides, we think to be important to organize training programs and to provide information about good death to enable patients’ relatives so that they can better manage the death process and cope with this process.
Limitations
The sample size was small in this study, as it was conducted with nurses, patients, and patient relatives at a single center. A cross-sectional design was used. The data could not be sufficiently discussed in our study because there is no study involving the use of the DAP-R scale with patients and their relatives in the literature. Further, large-scale studies must to confirm these findings.
Footnotes
Acknowledgments
We would like to thank the administration of the University Hospital, which granted the necessary permissions for the implementation of the study and all nurses who participated in the study.
Authors’ Contribution
D.Ö. collected data and analyzed the data and results conducted interpretation.
B.Ç. designed the study, collected, and analyzed the data and results. She carried out interpretation and drafted the manuscript, conducted interpretation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.