
Abstract
This study was carried out to determine the relationship between the fear of COVID-19 in the elderly aged 65 years and over and their levels of adaptation to the “new normal.” This descriptive cross-sectional study was completed with 623 elderly individuals. It was determined that the individuals who adapted well to the “new normal” had high levels of adaptation to old age, while their levels of fear of COVID-19 were slightly above average (p < 0.01). Elderly individuals have tried to adapt to the “new normal” while also experiencing fear of COVID-19. In order to minimize the fear experienced by the elderly during COVID-19, adequate support and psychological support should be provided.
Introduction
The coronavirus, known as COVID-19, is an acute infectious pandemic that spreads rapidly through most countries in the world (Zhong et al., 2020). The World Health Organization (WHO) declared that this disease, which spreads regardless of language, religion, and race, most affects elderly individuals who have chronic diseases, that most deaths in the past year have occurred in this age group, and that this is a cause for international concern. According to the WHO, 89.0% of COVID-19 related deaths occurred in those aged 65 years and over (World Health Organization, 2021). In the daily report of the Turkish Ministry of Health, a total of 9.296 COVID-19 related deaths were reported, of which 72.0% were over the age of 65 (Ministry of Health, 2021). It cannot be foreseen how and to what extent the COVID-19 virus, which is at the time of writing continuing to mutate, will affect the future health of individuals (Altın, 2020).
The rapid spread of the virus and its transformation into pandemic led nations to take serious countermeasures. As in the rest of the world, various measures were also taken in Turkey. Between 21 March and June 9, 2020, a curfew was imposed on citizens over the age of 65 and those known to have chronic diseases, making elderly people the first group to be excluded from social life. In June, these restrictions were lifted to inaugurate a “new normal” and the elderly were allowed to go out from 10:00–13:00 on weekdays and travel long-distance providing that they received permission. After the partial and full closure periods, a “controlled normalization process” was started. As of July 1, 2021, all bans have been lifted, but it has been decided to continue wearing masks. However, with the lifting of the bans, there has been a rapid increase in the number of cases, and it has been started to talk about the restrictions again (Ministry of the Interior, 2021).
The fact that these restrictions have been in place for more than a year has increased the risk of death due to chronic disease, as well as social and economic losses, separation from loved ones, the inability to have a normal funeral after death, because relatives are unable to attend, discrimination, loneliness, panic, anxiety, and stress; these issues have all placed psychological pressure on the elderly and led to anxiety that could otherwise have been avoided (de Leo & Trabucchi, 2020; Duan & Zhu, 2020; Dunford et al., 2020; Gyasi, 2020). One psychological aspect of the COVID-19 pandemic is fear and anxiety (Pakpour et al., 2020). Extraordinary situations, such as epidemics, may cause many people to feel afraid (Goyal et al., 2020). When fear is at a high level, it may have negative effects on mental and general health problems such as phobia and social anxiety in individuals, and wider social issues of depression, panic, alienation, and xenophobia (Hossain et al., 2020; Pakpour et al., 2020). If the level of fear experienced is low, it may, on the other hand, lead to individual and social harm as individuals ignore what is said and fail to comply with pandemic rules, thereby experiencing a concomitant decrease in psychological endurance (Kımter, 2020).
Over the course of the pandemic, the increasing effects of COVID-19, the fear of the spread of the mutated virus, and the fact that the whole society had not yet been vaccinated gave rise to an acceptance of the increasing impact of COVID-19, and a habituation to a “new normal” (Yazıcı Çelebi, 2020). In other words, owing to the long-lasting pandemic, elderly people changed their customary behaviors, habits, and lifestyles. The pandemic caused them to try to adapt to a new lifestyle and, as a result to, experience problems in adapting. Although some individuals could adapt to the new lifestyle relatively comfortably, others had difficulty adapting and showed psychological symptoms (Kımter, 2020). Given that the COVID-19 pandemic disrupted the daily life of elderly people, and increased infection and death rates, it may also have led them to not be able to adapt to this “new normal” and brought about greater levels of fear, anxiety, and vulnerability (Payette et al., 2016; Aburub, Phillips, Curcio, Guerra, & Auais, 2020; Gerhold, 2020). No study in the literature has directly assessed the relationship between fear and adaptation to the “new normal” in individuals aged 65 and over.
Aim
This study was thus carried out to determine the relationship between the fear of COVID-19 in the elderly aged 65 and over, and their levels of adaptation to the measures taken to establish a “new normal.”
The following research questions were asked
• What are the levels of compliance of the elderly aged 65 and over with the measures taken in the process of establishing a “new normal” and how do these relate to the fear of COVID-19? • What factors affect the level of adaptation of the elderly aged 65 and over to the measures taken to establish a “new normal” and how do these relate to the fear of COVID-19? • Is there a relationship between the fear of COVID-19 in the elderly aged 65 and over and their level of compliance with the measures taken to establish a “new normal?”
Methods
Design and Study Population
A descriptive and cross-sectional design was used in this study. 756 individuals aged 65 and over, who lived in the city center of Mersin and were registered at Family Health Centers, constituted the universe of this study. The study sample was comprised of 623 (82.4%) people who met the research criteria: (a) were 65 years or older, (b) had no vision or hearing problems, (c) were able and willing to communicate and collaborate, (d) could speak and read Turkish, and (e) agreed to participate in the study.
Instruments
The questionnaire was prepared by the researchers according to the literature (Chee, 2020; Gashi, 2020; Hossain et al., 2020; Karal & Biçer, 2020; Mertens et al., 2020; Yadav et al., 2020). The questionnaire consisted of 16 close-ended questions about the elderly individuals’ socio-demographic features and COVID-19.
“Fear of COVID-19 scale (FCoV-19S)” was developed by Ahorsu et al., 2020 to measure the levels of fear of COVID-19 in individuals. The Turkish validity and reliability study was carried out by Bakioglu et al., 2020. The questionnaire has a single-factor structure and consists of seven items in a five-point Likert-type structure, with options ranging from 1 (“Strongly disagree”) to 5 (“Strongly agree”). All items were scored positively. The internal consistency of the scale was found to be 0.82 and test retest reliability was 0.72. The total score ranges from a minimum of seven to a maximum of 35. A high score from the scale indicates that the fear of COVID-19 is high. In this study, the Cronbach’s alpha value of the scale was 0.72.
“Assessment Scale of Adaptation Difficulty for the Elderly (ASADE)” was developed by Şişman & Kutlu, 2016. It is a four-point Likert-type scale consisting of 24 items. The lowest possible score from the scale is zero and the highest is three. The scale score is calculated by adding up the score for each item and dividing the total by the number of questions. There are four subscales, namely “Role and self-actualization mode,” “Interdependence mode,” “Physiological mode,” and “Self-concept mode.” The points that can be obtained vary between 0 and 3. The closer the individual’s score is to 0, the higher the level of adaptation. The Cronbach’s alpha value of the scale was 0.83 in the original study; it was found to be 0.88 in this study.
Data Collection
Data were collected between December 2020 and March 2021. Due to the COVID-19 pandemic, the Personal Information Form, the FCoV-19S and the ASADE were implemented face-to-face using protective equipment and following the “1.5 m distance” rule. An explanation was given to the elderly individuals about the purpose, process, and form of the study, and their consent was obtained by stating that participation in the study was voluntary. It took about 10 or 15 minutes to complete the scales.
Data Analysis
The research data were statistically analyzed using the SPSS 21.0 (Statistical Package for the Social Sciences, Chicago, Illinois). Categorical variables were presented as frequencies and percentages. Continuous variables were expressed as mean and standard deviation (SD). For evaluating the normality of the data distribution, the Kolmogorov–Smirnov test was used. The Mann–Whitney U Test was used in two groups which had continuous variables and Kruskal–Wallis analysis of variance for more than two groups. The Dunn–Bonferroni test was used to determine the difference between the groups. The Cronbach’s alpha value was found using reliability analysis. Spearman correlation analysis was also performed to finds the relationship between the scales. A two-sided p value <0.05 was considered significant for all analyses.
Ethical Approval
Before data collection, approval was received from the Ethics Committee for Non-Interventional Clinical Studies of Burdur Mehmet Akif Ersoy University (Decision Number: GO 2020/240). Written and verbal consent was obtained from the elderly individuals who participated in the study. In addition, written permission was obtained from the developers of the scales to use their scales. This research was carried out in accordance with the Good Clinical Practices of the Helsinki Declaration.
Results
Distribution of Those Aged 65 and over According to Their Socio-Demographic Characteristics (n=623).
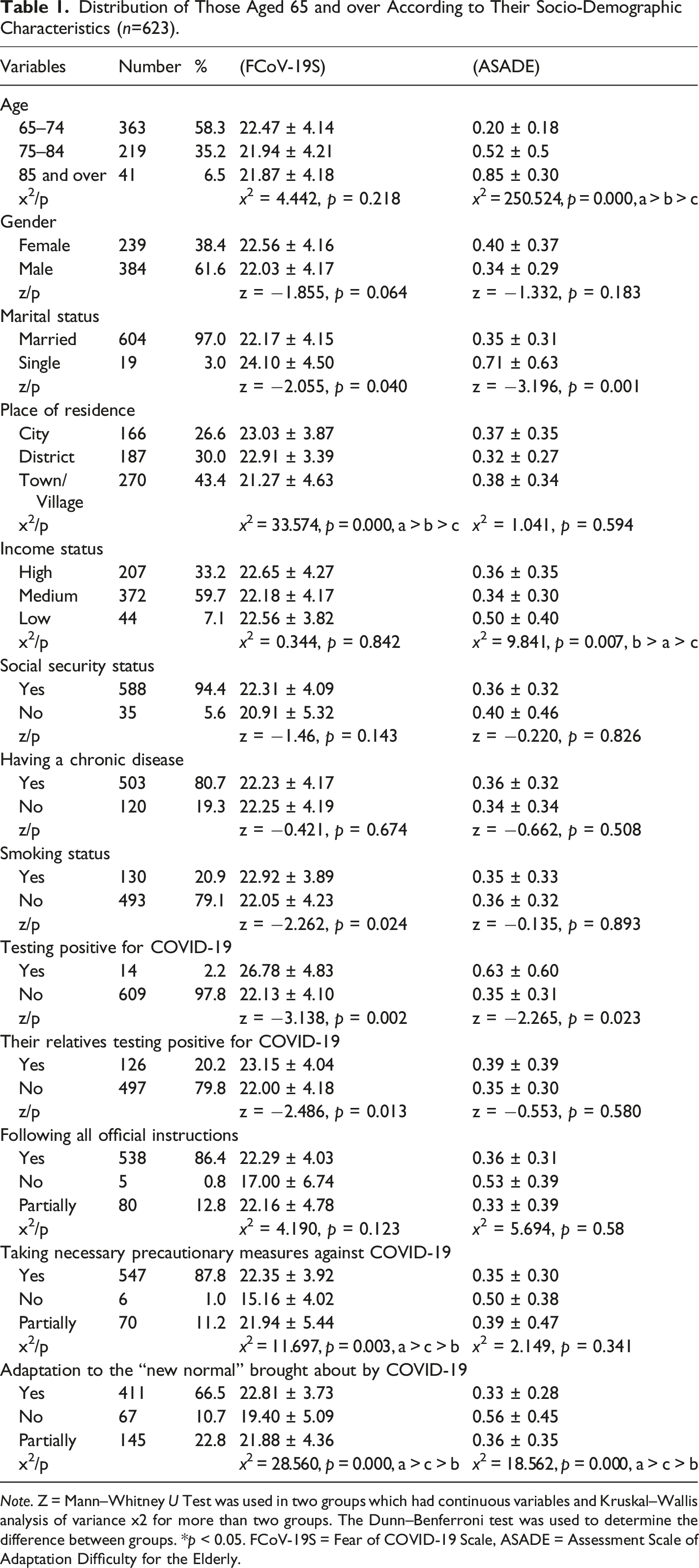
Note. Z = Mann–Whitney U Test was used in two groups which had continuous variables and Kruskal–Wallis analysis of variance x2 for more than two groups. The Dunn–Benferroni test was used to determine the difference between groups. *p < 0.05. FCoV-19S = Fear of COVID-19 Scale, ASADE = Assessment Scale of Adaptation Difficulty for the Elderly.
It was determined that the mean FCoV-19S of single individuals (p = 0.040) and ASADE (p = 0.001) scores were significantly higher. It was determined that the average FCoV-19S scores of the people living in the city were significantly higher than those of the elderly living in the wider district and villages (p = 0.000). It was seen that the mean scores of the elderly who defined their income as low were significantly higher than those of those with a medium and high income (p = 0.007). It was observed that the average FCoV-19S scores of the elderly who smoked were significantly higher than of those who did not (p = 0.024). It was shown that the average FCoV-19S scores of the elderly who had tested positive for COVID-19 (p = 0.002) and whose relatives had tested positive for COVID-19 (p = 0.013) were significantly higher than those who had not or who did not have relatives who had tested positive. It was determined that the FCoV-19S scores of the elderly who took the necessary precautionary measures for COVID-19 were significantly higher than those who only partially took or did not take any such measures (p=0.003). It was observed that the elderly who had a fear of death related to COVID-19 had a significant level of fear of COVID-19 compared to those who did not have such a fear (p=0.000). It was found that the average scores obtained from, respectively, the FCoV-19S (p= 0.000) and the ASADE (p= 0.000) for the elderly who had adapted to the “new normal” brought about by COVID-19 were significantly higher than the scores of those who had not (Table 1).
There was no statistically significant difference between the FCoV-19S based on the gender, income status, and social security of the elderly individuals. There was no significant difference between the mean ASADE averages, and the gender, place of residence, and social security status of the elderly individuals (Table 1).
The Mean FCoV-19S and ASADE Scores of the Elderly Individuals.
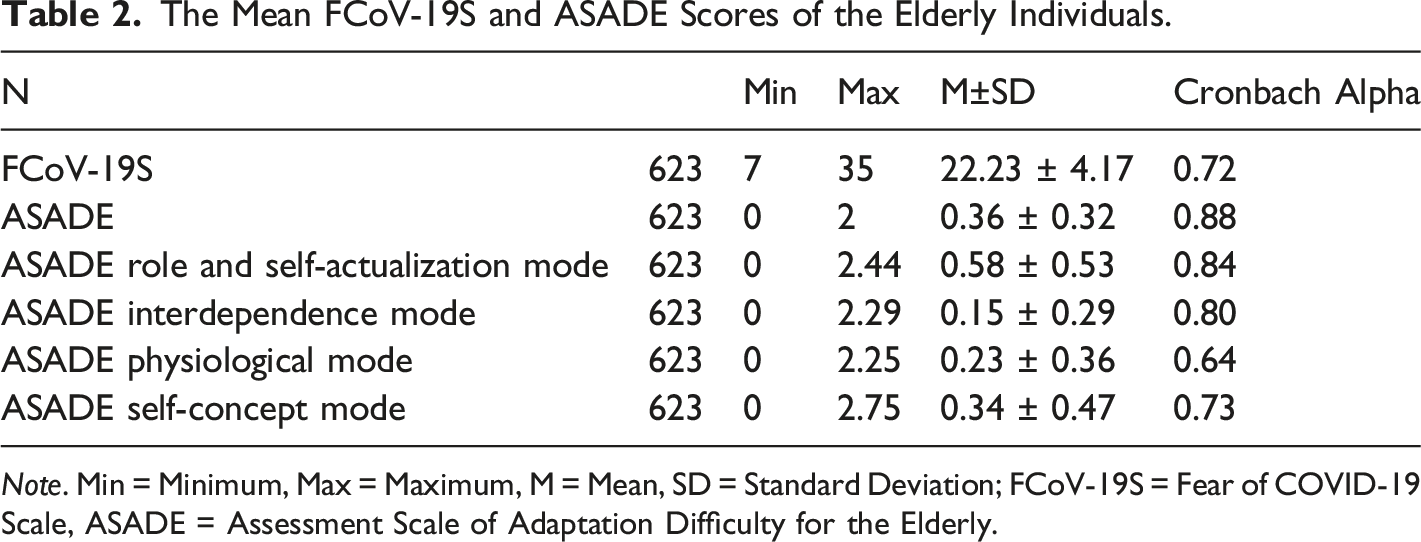
Note. Min = Minimum, Max = Maximum, M = Mean, SD = Standard Deviation; FCoV-19S = Fear of COVID-19 Scale, ASADE = Assessment Scale of Adaptation Difficulty for the Elderly.
Relationship between the Mean FCoV-19S and ASADE Scores of the Elderly Individuals.
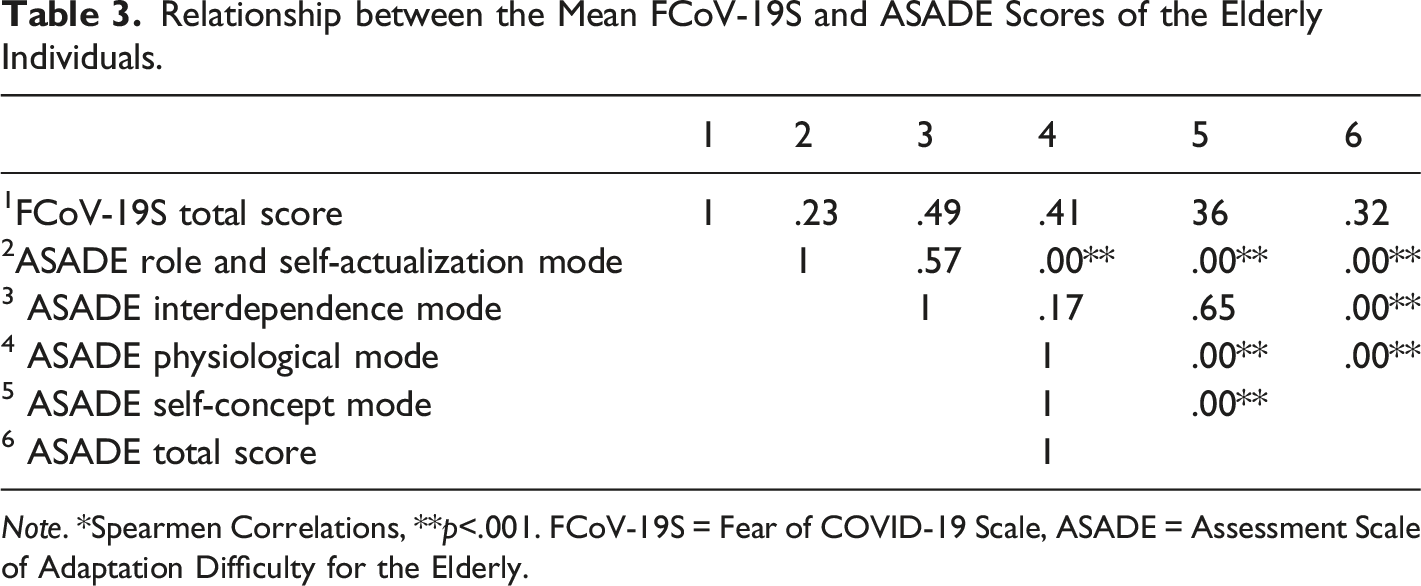
Note. *Spearmen Correlations, **p<.001. FCoV-19S = Fear of COVID-19 Scale, ASADE = Assessment Scale of Adaptation Difficulty for the Elderly.
Discussion
As COVID-19 became an increasing problem worldwide, owing to the uncertainty of the disease and treatment process, it caused stress, anxiety and fear, especially among elderly individuals with at least one chronic disease who had been quarantined (Ahorsu et al., 2020; Nicola et al., 2020). The literature emphasizes the relationship between the fear of COVID-19 of elderly individuals aged 65 and over and their levels of adaptation to the measures taken to establish a “new normal.”
It was determined that the mean FCoV-19S score of the elderly who participated in the study was slightly above the mid-level of 22.23 ± 4.17. In the literature, the study by Yadav et al. (2020) found a low score of 18.1 ± 5.2, the study by Hossain et al. (2020) stated that women and elderly individuals had moderate and high levels of fear, the studies by Gashi (2020) and Mertens et al. (2020) indicated that individuals had high levels of COVID-19 and anxiety, and, according to the study by Chee (2020), elderly individuals experienced uncertainty about COVID-19, and fear of transmission and death. Expert reports in the literature stated that the COVID-19 pandemic affected the psychology of elderly individuals and caused stress, fear, and death anxiety (Banerjee, 2020; Kımter, 2020; Wu, 2020). The findings of the current were similar to the results of others studies indicating fear and psychosocial effects arising from COVID-19. These results suggested that older individuals need to be psychologically supported to reduce their sense of fear.
It was determined that the average ASADE score of the elderly individuals who participated in the study was 0.36 ± 0.32. The literature reported that the average ADEAS score ranged from 1.00 ± 0.68–1.07 ± 0.73 (Kütmez Yılmaz, 2020; Kütmez Yılmaz & Kıl, 2020; Şişman & Kutlu, 2016). Considering that the scale is scored between 0 and 3 and that adaptation increases as the scores approaches 0, the elderly individuals in the current study were found to have high levels of adaptation levels. Adaptation to old age was interpreted as the acceptance of changes such as diseases caused by aging, physical, psychosocial, and economic losses, the limitations placed on one’s activities, and the adaptation to these issues through developing healthy coping skills (Kütmez Yılmaz & Kıl, 2020). The current study found that owing to the cultural characteristics and Islamic-dominated belief system where the research was carried out, the elderly individuals were valued, respected, and that their needs were met and social relations maintained with them. Hence, it can be said that this reflects a positive adaptation to old age.
It was determined that adaptation to old age decreased as age advanced. The results of the current study were in line with the literature (Aşiret & Yiğit, 2018; Kütmez Yılmaz, 2020; Kütmez Yılmaz & Kıl, 2020; Şişman & Kutlu, 2016). Decreased adaptation to old age as age advanced can be explained by the fact that, with increasing age, the number and severity of diseases and dependency increase.
The current study determined that single people had higher fear of COVID-19, while those who were married had high levels of adaptation to old age. The literature reported that single people experienced the fear of COVID-19 more than those who were married and had a lower level of psychological resilience (Kımter, 2020; Wang et al., 2020; Kunz & Minder, 2020; Yadav et al., 2020); it was determined that those who were married and lived with their spouse had higher levels of adaptation to old age (Kütmez Yılmaz, 2020; Kütmez Yılmaz & Kıl, 2020). These results tell us that the reason why the fear of COVID-19 is higher for the single elderly people than the married ones is because they do not have social support, and that living alone causes them to feel unsafe; the high level of adaptation of married elderly people to old age can be explained by the positive effect of social support provided by the spouse on the physical and psychosocial health of elderly individuals and their ability to cope with stressful life events. In this sense, single elderly people living alone, especially during the pandemic, should be supported socially, psychologically and physiologically.
It was determined that the elderly living in the cities had a higher fear of COVID-19 than the elderly living in the wider district or villages. Although there are studies in the literature showing that the fear of COVID-19 is high in individuals living in the province (Hossain et al., 2020; Özdin & Bayrak Özdin, 2020), there are also results that indicate high fear of COVID-19 among the elderly living in the countryside (Parmaksız, 2019; Yadav et al., 2020). This can perhaps be interpreted as individuals living in the cities after COVID-19 wanting to resettle in districts and villages because of the idea that urban areas are overcrowded and there is a greater risk of transmission of the disease, while, conversely, those living in the districts and villages want to live in the cities because they have difficulty accessing health services. The reason for the different results in the studies is thought to be due to the different sample numbers, education levels and age groups in each of them.
It was found that the elderly who defined their income as low had significantly higher total mean scores for the ASADE compared to those with a medium or high income; in other words, they had difficulty adapting. Studies in the literature have indicated that socio-economic and health inequalities affected the COVID-19 pandemic, so individuals whose incomes were lower had higher COVID-19 pandemic fear and anxiety scores (Kantamneni, 2020; Gashi, 2020). These results suggest that individuals whose incomes were low may also have decreased their health care benefits, may have failed to manage of their chronic diseases, and may have had difficulty adapting because they felt weak. Supporting elderly individuals socio-economically through government policies may make them feel more secure, thereby reducing their difficulties in adapting.
The study found that the fear of COVID-19 was significantly higher for the elderly individuals who smoked. Studies in the literature have reported that smoking is associated with the COVID-19 progression, that smokers are 1.91 times more likely to experience severe COVID-19 than those who had never smoked, and that smoking is a factor that increases the rate of hospitalization (Killerby et al., 2020; Patanavanich & Glantz, 2020). These results show us that the elderly had more the fear of COVID-19 due to the explanations given in media and scientific publications about the risk of infection and the high mortality in smokers.
It was determined that the fear of COVID-19 was significantly higher for the elderly who had themselves tested positive for COVID-19 and/or whose relatives had tested positive for COVID-19. Studies have indicated that those who had lost a relative to COVID-19 or whose relatives had had the disease had high levels of fear and anxiety of COVID-19 and had lower levels of psychological resilience (Cao et al., 2020; Çetin & Anuk, 2020; Duman, 2020; Özdin & Bayrak Özdin, 2020). These results suggested that when elderly people were worried about the deadly consequences of the pandemic, COVID-19 psychologically disturbed them, and these elderly individuals may have experienced fear of death and fear of losing their relatives. In this process, it is important to support the mental health of the elderly who have tested positive for COVID-19 and their relatives by providing psychological support.
In the current study, it was determined that the majority of the elderly individuals followed all official instructions, took the necessary precautionary measures against COVID-19 and adapted to the “new normal.” It was found that individuals who had adapted to old age also adapted to the “new normal,” but experienced a high degree of fear. Studies in the literature have reported that individuals applied a high rate of self-isolation and developed health behaviors by staying at home and wearing masks to prevent the spread of COVID-19 (Hossain et al., 2020). These results suggest that older individuals were more afraid of transmission of the disease and death, and, that, as a result, they were trying to adapt more quickly to the “new normal.” However, although they took the necessary measures and adapted, the fact that the situation is still uncertain and that mutations may occur even after vaccines have been developed, means that they are still afraid of COVID-19. In the “new normal,” elderly individuals who are in vulnerable groups should be protected until the pandemic is over and the government should develop policies specifically targeting the care of the elderly.
Conclusion and Recommendations
This study concluded that elderly individuals fear COVID-19 but have also adapted to the “new normal.” It could be said that because they had high levels of COVID-19 and fear of death, the elderly did not have difficulty adapting. The COVID-19 pandemic affected them psychologically, socially, and physically due to forced isolation, loneliness, disease, uncertainties about the treatment process, and fear of death. The severe fear experienced by elderly individuals about the pandemic can be reduced by providing them with sufficient correct information, and the necessary psychosocial support.
Limitations
This study consisted of elderly people aged 65 years and over who attended the Family Health Center at the time of the study and thus did not cover all elderly people in Turkey.
Implications for nursing practice
This study provides important clinical findings in understanding the fear of the elderly population, the first group to withdraw from normal social life due to COVID-19, and their adaptation to the “new normal.” It shows that elderly individuals need help to overcome their fears about COVID-19 and adapt. It is necessary to understand the difficulties arising from the fear of COVID-19 (especially in those elderly people who live alone, who smoke, who have tested positive, or who have relatives who have tested positive for COVID-19), and to determine appropriate strategies to deal with these challenges. During the pandemic, health professionals should determine at an early stage the psychological effects that the elderly may experience due to their fear of COVID-19. By taking measures to address these, they can help those of a more advanced age develop effective strategies and survive the pandemic with minimal damage.
Footnotes
Acknowledgments
The authors would like to thank all the participants.
Author Contributions
Concept – S.Ş., A.Y.K.; Ş.S.; Design - S.Ş., Ş.S; Supervision - S.Ş., Ş.S.; Resource - S.Ş., A.Y.K.; Materials - S.Ş., Ş.S.; Data Collection and/or Processing - S.Ş., Ş.S.; Analysis and/or Interpretation - S.Ş., A.Y.K.; Literature Search – S.Ş., A.Y.K.; Writing – S.Ş., A.Y.K.; Critical Reviews – S.Ş., A.Y.K.; Ş.S.; Other - S.Ş., A.Y.K.; Ş.S.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethics committee approval was gained from the Ethics Committee for Non-Interventional Clinical Studies at Burdur Mehmet Akif Ersoy University (Decision Number: GO 2020/240).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.