
Abstract
In order to achieve an in-depth understanding of professional caregivers’ experiences of bereavement after patient deaths in Mainland China, qualitative description was employed. 24 physicians and nurses from hospitals in Nanjing, China, participated in one-to-one, semi-structured interviews. Thematic analysis was adopted for data analysis. Five themes were generated: the nature of professional bereavement experiences, the meaning of patient deaths, immediate bereavement reactions, long-term changes, and coping strategies. Each theme included personal and professional dimensions. Professional bereavement experiences in Mainland China were found to be influenced by workplace violence against professional caregivers, traditional Chinese medical ethics, the strong death taboo, and inadequacies of the healthcare system. Professional bereavement experiences are meaning-driven, comprehensive, and usually disenfranchised. They involve multidimensional reactions and have both short-term and long-lasting, both event-specific and accumulated impacts. Cultural and systemic factors could shape professional bereavement experiences.
Introduction
Patient deaths are impactful events for professional caregivers (Granek et al., 2017).As physicians and nurses build both professional-client relationships and personal bonds with their patients, patient deaths can trigger bereavement experiences among professional caregivers; such experiences are referred to as professional bereavement (Wenzel et al., 2011).
Physicians and nurses experience professional bereavement as both a member of the medical staff who is responsible for the treatment outcome and an individual who knows the deceased personally (Chen et al., 2018). Shortly after a patient’s death, professional caregivers may experience physical (e.g., insomnia (Jackson et al., 2005), emotional (e.g., grief and guilt (Granek et al., 2017), cognitive (e.g., intruding thoughts about the death (Wilson, 2014), relational (e.g., disconnections from friends and family (Granek et al., 2015), existential (e.g., death anxiety (Shorter & Stayt, 2010), and spiritual (e.g., questioning of one’s religion (Masia et al., 2010) reactions. Moreover, repeated experiences of patient deaths can lead to fundamental changes in both the professional and personal lives of professional caregivers (Chen et al., 2018). For instance, in daily work, healthcare professionals would deliberately involve less in caregiving to avoid getting hurt when patients die (Gerow et al., 2010). Personally, they set new priorities in life after witnessing many lives passing (Conte, 2014).
Until now, the majority of studies on professional bereavement were conducted in developed countries and regions in the world, particularly Europe and North America, and experiences from non-Western and underdeveloped regions are underrepresented (Chen et al., 2018). Between these regions, huge differences exist in cultural backgrounds, healthcare systems, and healthcare resources. As all these aspects are vital in shaping professional bereavement experiences (Papadatou, 2009; Rosenblatt, 2008), direct generalizations are problematic.
Professional Bereavement in Mainland China
In Mainland China, at least 1.11 million deaths occurred in hospitals in 2017 (National Health Commission of the People's Republic of China, 2018), accounting for more than 90% of deaths in all healthcare institutions. These events exposed 1.80 million practising physicians and 2.82 million registered nurses in hospitals to professional bereavement experiences (National Health Commission of the People's Republic of China, 2018). Nevertheless, few studies have explored the topic of professional bereavement in China.
A series of unique cultural and systemic factors in Mainland China may make professional bereavement experiences particularly challenging and complicated there.
In terms of culture, death is a taboo subject in China (Hsu et al., 2009), and related topics are avoided not only in daily conversations but also in professional-patient discussions in medical contexts (Chan & Chow, 2006; Mak, 2006). Moreover, owing to the Confucian familism tradition, patients’ families play quite important roles in “doctor-family-patient relationships” in medical processes in China (Cong, 2004), which may also complicate professional bereavement.
Currently, the healthcare system in Mainland China is underdeveloped: the density of healthcare professionals is relatively low (World Health Organization, 2015), staff workload is inevitably heavy (Wen et al., 2016), and patients’ quality of death is far from satisfactory (The Economist Intelligence Unit, 2015). In other words, compared with more developed countries, in China, professional caregivers experience more patient deaths in their careers, those deaths are more likely to be unsettling rather than peaceful, and there is less time for professional caregivers to deal with those deaths.
In addition, in contemporary society, Chinese professional caregivers suffer terribly from severe mistrust and even violence from patients and their families (An, 2013; Hesketh et al., 2012). As families hold high expectations of medical outcomes (Yan, 2018), they tend to feel disappointed when a patient dies and then blame professional caregivers, hurt them, or even create chaos in the department (Pan et al., 2015). Such incidents have led to the injury, or even death, of professional caregivers (Pan et al., 2015), and they may cast a shadow on professional bereavement experiences in Mainland China.
The Present Study
The present study aims to achieve an in-depth understanding of professional bereavement experiences in Mainland China based on first-hand qualitative data.
Methods
Design
The authors adopted a constructivist epistemology and the tenets of naturalistic inquiry. Qualitative description, a method for the low-inference description of a phenomenon (Sandelowski, 2000), was applied. The authors followed the reporting guidelines of the Standards for Reporting Qualitative Research (SRQR) (O’Brien et al., 2014).
Participants
Physicians and nurses working in hospitals in Nanjing, China, who had experienced at least one death of a patient under their care were included in the study, but those who knew their latest deceased patient personally before providing healthcare services were excluded.
Nanjing is the capital city of Jiangsu Province, where the total GDP and GDP per capita rank 2nd and 4th highest, respectively, among those of the 31 administrative divisions in China (China Statistical Bureau, 2016) and where healthcare resources are abundant (Liu et al., 2016). In 2017, 19,324 practising physicians and 28,707 registered nurses were working in hospitals in Nanjing (Nanjing Health and Family Planning Commission).
Purposive sampling, convenient sampling, and theoretical sampling strategies were jointly employed in participant recruitment. The first few participants were recruited via advertisements in several hospitals in Nanjing, and these participants in turn invited more people to participate. During recruitment, maximum variation was pursued in terms of participants’ sex, position, department, length of service, and recent personal bereavement experience, as well as the accreditation level and ownership of the hospital they worked in. Because several interviewees mentioned that patient deaths at the beginning of their careers had enormous impacts, the authors purposefully recruited several interns. The recruitment was complete when satisfactory diversity among participants had been achieved and no new participants were required for theoretical considerations.
A total of 24 participants (13 females, Table 1) were included in the study, and their average age was 29.3 years (SD = 4.93, range: 25‒42). Among them, 22 were from tertiary-level hospitals, while two were from secondary-level hospitals. All except one worked in public hospitals. The interviews lasted between 6 minutes (due to interruption for one participant to perform an emergency resuscitation) and 1 hour and 14 minutes, with an average duration of 23 minutes.
Information of Interviewees.
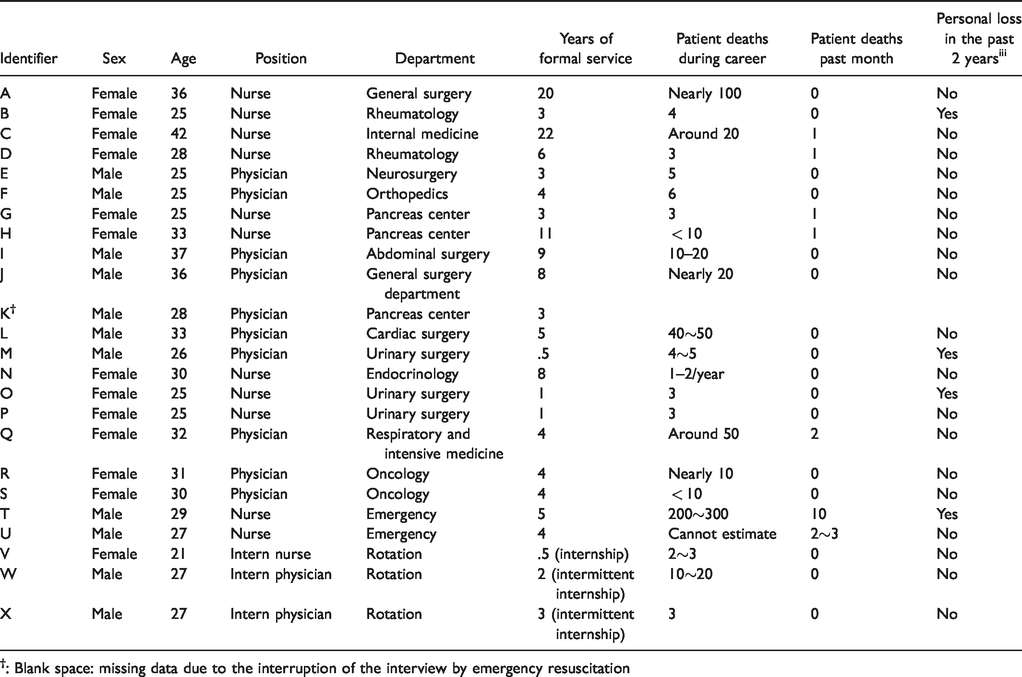
†: Blank space: missing data due to the interruption of the interview by emergency resuscitation
Data Collection
Data were collected by C.Q.C. between September and November 2017 via individual face-to-face semi-structured interviews. An interview guide developed based on a literature review and discussions between the authors was followed, and the major questions were as follows: “Can you please tell me about one impactful or typical patient death in your career/can you please tell me about your most recent patient loss? What were your feelings? How did it influence you?”
Ethical Considerations
The present study was approved by the Human Research Ethics Committee of The University of Hong Kong (reference number: EA1707005). All participants gave written consent before data collection began. Participants could drop out of the study at any time and would be provided with the contact information for free mental health hotlines if they felt uncomfortable during the interviews.
Data Analysis
All interviews were audio-recorded and later transcribed, and participants were identified by codes instead of their names. The audio recordings and documents containing personal identifiers were kept strictly confidential: The audio recordings were saved on an encrypted USB stick, and the documents were locked in a file cabinet.
Data were analysed in NVivo 11 (QSR International Pty Ltd, 2015) following the steps of thematic analysis (Braun & Clarke, 2006). For interview data, the main coder, C.Q.C., first read the text many times to familiarize herself with it. Then, she freely coded the text and identified as many initial codes as possible. Afterward, initial codes were grouped together as themes. Those themes were reviewed and named accordingly, and they were then summarized in a table.
Rigour
Several actions were taken to enhance the trustworthiness and credibility of the data analysis. The authors rigorously adhered to the research steps, and the main coder maintained reflexivity throughout the coding process and recorded notes on her reflections. Research meetings between C.Q.C. and A.Y.M.C were held regularly to discuss their interpretations, and four additional experts in the field of bereavement and grief were invited to give comments on the generated themes.
Results
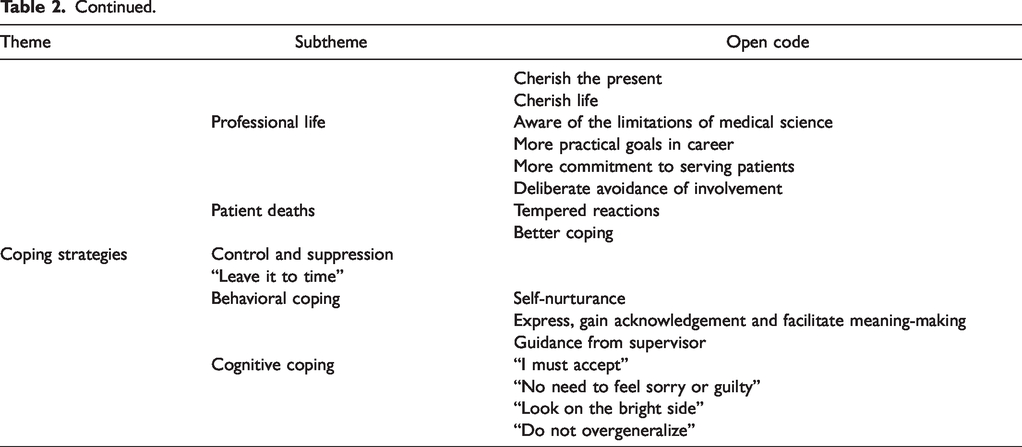
Authors identified 73 open codes from the transcripts, which were then grouped under 17 subthemes. Eventually, based on the aspects of professional bereavement experiences they covered, the subthemes were categorized into five themes (Table 2): the nature of professional bereavement experiences, the meaning of patient deaths, immediate bereavement reactions, long-term changes, and coping strategies. Examples for each open code are shown in the Appendix.
Generated Themes From the Interview Data.
Nature of Professional Bereavement Experiences
With regard to the nature of professional bereavement experiences, three subthemes were revealed.
Professional bereavement is an experience for which school education fails to prepare professional caregivers. As feelings after encountering a patient death in real life are totally different from those when seeing a body in an anatomy lesson or reading a case in a book, the overall reactions generated by a real death often take professional caregivers by surprise. At those moments, some caregivers may wonder, “Why hasn’t anybody warned me about this?” Moreover, no relevant values or coping methods are taught ahead of time to prepare professional caregivers psychologically or spiritually for these encounters.
Moreover, professional caregivers’ grief after patient deaths is often disenfranchised: it often goes unnoticed and is not recognized by other people. Interviewees mentioned that people around them usually believe that medical staff are too calloused and numbed from their past training and day-to-day dealings with death to feel anything after patients die. Further intensifying professional bereavement experiences is the phenomenon of self-stigmatization: interviewees said that they believed they should not talk about death-related feelings, that they should not reveal those feelings at home, and that they should not even have those emotions in the first place because they were a sign of being “too vulnerable.”
In addition, professional caregivers have almost no resources to deal with professional bereavement experiences. On the one hand, physicians and nurses in Chinese urban hospitals are extremely busy. They barely have time for a short break after a patient death, let alone time to attend to their grief. On the other hand, there is no psychological support available in hospitals for professional bereavement.
Meaning of Patient Deaths
Professional caregivers attribute both personal meanings and professional meanings to patient deaths.
From a personal perspective, a patient’s death is first and foremost the loss of a valuable life, which is a great pity. Some interviewees reported viewing death as the loss of a friend or an acquaintance. Sometimes, a patient’s death causes great pain for family members, and empathy for families can make physicians and nurses suffer as well. In certain cases, the deceased patient or the scene of the patient’s death reminds professional caregivers of their own late loved ones, and thus, witnessing the death makes them relive a past personal loss. A patient’s death may also sound a warning bell for professional caregivers, making them think about the possibility of losing loved ones in the future. Similarly, professional caregivers may be reminded of and forced to confront their own mortality when witnessing patient deaths. In extreme circumstances, a patient’s death can be a terrifying and even traumatic event for professional caregivers due to the horrific scenes involved.
From a professional perspective, physicians and nurses may interpret patient deaths as their own job failure and incapability. Moreover, some professional caregivers view patient deaths, especially those that still happen after all possible efforts have been made, as reminders of the limitations of medical science. For some, these deaths even signify the “death” of their idealized professional identity as an omnipotent physician or nurse who is always the “saviour” for patients. In addition, as some professional caregivers wish to have a safe shift without emergencies or bad news, a patient death on their shift can be viewed as bad luck. Moreover, patient deaths are perceived as triggers of potential professional-family conflicts. Nevertheless, patient deaths are not necessarily negative events: several interviewees viewed each case of a patient’s death as a precious opportunity to reflect and “learn from mistakes.”
Immediate Bereavement Reactions
Professional caregivers may have multidimensional reactions after each specific patient death, including behavioural & physical, emotional, cognitive, and philosophical ones.
Behavioral reactions involve crying and hypervigilance, and the latter usually manifest after professional caregivers are traumatized by horrific death scenes. Interviewees also reported insomnia.
The most commonly mentioned reactions are emotional ones. Professional caregivers experience grief after patient deaths, and they sometimes feel sorry and regret for the loss of a valuable, and in particular young, life. They will also feel pity for the patient and the bereaved family. Moreover, interpreting a patient death as failure in work, professional caregivers may feel frustrated, disappointed, and helpless. They may also feel guilty and blame themselves when they believe that they could have done a better job in preventing the death, delaying it, or making it easier for the patient. Sometimes, the cause of death cannot be fully understood, and professional caregivers suffer from feelings of perplexity. Moreover, being afraid for getting blamed or even hurt by the family, interviewees feel nervous after a patient dies. When conflicts do take place, physicians and nurses feel angry, wronged, and hurt as they cannot be trusted even after trying their utmost to save a patient. In contrast, when they are trusted and thanked by families, they feel moved. When death scenes are awful, physicians and nurses feel frightened. Interviewees also mentioned feelings of relief and peace when a patient dies a “good death.”
Cognitive reactions are mainly related to reasoning, evaluation, belief, and memory. Professional caregivers can go through a repetitive chronological recall of the case to try to figure out “when things went wrong.” At the same time, some experience counterfactual thinking and keep asking “what if.” Meanwhile, physicians and nurses try to evaluate their own performances and their responsibility for the death. They will also undergo self-reflections to learn from the case. In order to estimate the risk of work-place violence, professional caregivers also conduct self-censorship to look for anything that could be used against them. Accompanying a sense of failure, professional caregivers may have beliefs like “I am not a good physician/nurse yet,” or even “I am not a good physician/nurse at all.” For deaths that are especially meaningful or traumatic, their vivid memory will last for quite a long time and sometimes even for decades.
Regarding philosophical reactions, some professional caregivers realize the senselessness and uncertainty of death, and their death anxiety arouses.
Long-Term Accumulated Changes
After all the patient deaths in career, professional caregivers gradually achieve changes in their personal life and professional life, as well as their attitudes toward, and reactions after, patient deaths.
In their personal lives, physicians and nurses realize that life is short, uncertain, and valuable. They also gain deeper insights into the fact that “death is unavoidable.” As a result, they become more at ease with life, and they cherish life, the present, and time spent with their loved ones all the more. Moreover, professional caregivers become more sensitive to the signs of ageing in people around them, especially their loved ones, which often elicits sadness and nostalgia. In addition, some become more anxious about their own death and that of their loved ones in the future. On the other hand, some interviewees reported accepting death as a part of the natural law and being more eager to avoid over-treatment at the end of their own lives.
In their professional lives, physicians and nurses learn the limitations of medical science after experiencing many patient deaths. In this way, they set more practical goals for their careers: instead of striving to “heal the wounded and rescue the dying,” professional caregivers learn to “exert the utmost of their human abilities, and then resign the rest to the decree of Heaven.” Additionally, after witnessing the prices that patients and families pay when professional caregivers have not done their best, physicians and nurses become more committed to serving patients and eager to improve their knowledge and skills. However, some deliberately avoid becoming too involved to protect themselves from the pain of witnessing the suffering of a person whom they connect to.
After experiencing many patient deaths, new cases of patient deaths become less impactful for professional caregivers, and physicians and nurses become better at coping with those events.
Coping Strategies
Many interviewees mentioned that at the moment of a patient’s death, professional caregivers must control and suppress their feelings and reactions. In the face of the work to be done and the bereaved family to be supported, they must remain “calm and rational.” Moreover, some caregivers do not take deliberate action to deal with patient deaths, as they believe in the healing power of time.
For those professional caregivers who actively cope with patient deaths, behavioural coping and cognitive coping are major strategies.
Regarding behavioural coping, physicians and nurses may nurture themselves after patient deaths by exercising, reading jokes, resting, and spending time with loved ones. Moreover, some seek opportunities to express their feelings, gain acknowledgement and facilitate meaning-making during story telling. Most of the time, they turn to colleagues for mutual support. Some also share their feelings with families, but others choose not to do so to avoid burdening their loved ones with “negative energy.” In addition, guidance from supervisors is helpful, as experienced staff usually have more wisdom and resources in dealing with patient deaths.
In terms of cognitive coping, some professional caregivers tell themselves to accept patient deaths as a part of their job and a part of the natural law. When physicians and nurses feel guilty and sorry about a death, they try to remind themselves that they have tried their best, and even if they could have done better, sometimes, there is no way to avoid a patient’s death, as the patient was too sick to recover. Sometimes, professional caregivers adjust their mindsets and try to look on the bright side: “This has taught me something, in the end.” Additionally, physicians and nurses remind themselves that drawing the conclusion that medical science is disappointing and hopeless after just one patient death risks overgeneralization. On the one hand, more patients have benefitted and survived than have died after medical treatments; on the other hand, medical science is progressing, so certain diseases that are terminal today might become curable in the future.
Discussion
Professional Bereavement Experiences: Shared Key Features Across Regions
From the themes identified in interviews with 24 Chinese hospital physicians and nurses, several key features of professional bereavement experiences in Mainland China are revealed. Professional bereavement is a comprehensive process, as it involves multidimensional reactions and has both short-term and long-lasting impacts and both event-specific and accumulated impacts. Professional bereavement is also an experience that cuts across one’s professional life and personal life, as both dimensions were identified in each of the five themes. Moreover, professional bereavement experience is meaning-driven, as participants’ immediate bereavement reactions, long-term changes, and coping strategies were all based on the meanings they attribute to patient deaths. These features are consistent with findings of qualitative studies from other regions of the world (Katz & Johnson, 2016; Papadatou, 2009), which indicates the shared features of professional bereavement experiences regardless of culture, healthcare system, institution, and position.
Moreover, a low level of preparedness for patient deaths, the absence of support, disenfranchisement, and self-stigmatization have also been mentioned by healthcare professionals around the world, although no previous study has explicitly generated and emphasized the relevant themes. For instance, in South Africa, a doctor in the study by Masia et al. (2010, p. 300) mentioned “Because medical school does not prepare us for such things [patients’ deaths], when you lose patients, you always feel incompetent, inadequate and ashamed.” In the UK, a registered nurse in the study by Wilson (2014, p. 42) said “It was over quite quickly for him [the deceased patient], it was traumatic all round for everybody. Everybody wanted to talk about what happened, but that day there was no time, we just carried on.” In the U.S., Conte (2014, p. 42) unveiled pediatric oncology nurses’ “frustration regarding their loved ones’ lack of understanding of pediatric oncology and the misnomers that their jobs were sad and depressing a majority of the time”, and Gerow et al. (2010, p. 126) recorded a nurse saying “I never really believed that I deserved to get upset … I mean, this is your job; you’re supposed to deal with this stuff.” Disenfranchised grief, which has been widely studied regarding familial bereavement (Doka, 2002), is also a key feature of professional bereavement experiences.
New Discoveries With “Chinese Characteristics”
Several new open codes in the present study have not been mentioned by the existing literature, which are closely related in the cultural and systemic context of Mainland China.
Shadow of Workplace Violence on Professional Caregivers
As reflected in the findings, workplace violence casts a heavy shadow on professional bereavement experiences in Mainland China: professional caregivers may interpret a patient’s death as a trigger for potential professional-patient conflict and therefore feel nervous and perform self-censorship. When they are blamed by the bereaved family after having tried their best to save the patient, they feel wronged, hurt, and angry. In contrast, when families express appreciation despite patient death, professional caregivers are deeply moved, as such cases are quite rare and extremely precious in contemporary China.
Moreover, the aforementioned themes, together with the interviewees’ empathy with bereaved families, show that patients’ families have a profound influence on professional bereavement experiences in Mainland China. This influence could be traced back to the emphasis on families in Confucian tradition (Cong, 2004), which is reflected in so-called Confucian familism in health care activities in Mainland China (Fan & Wang, 2015): According to Confucian familism, “Families, not individuals, have ontological priority. It is not just that individuals only flourish within families. It is rather that families are the grounding reality within which individuals must be understood” (Fan, 2007, p. 16). Under such circumstances, families rather than patients are recognised as holding the authority to make medical decisions (Fan, 2007). Therefore, families play vital roles in medical processes in Mainland China, and so do their voices and experiences.
Influence of Traditional Chinese Medical Ethics
Healthcare professionals’ doubts about the value of their profession after patient deaths have been mentioned by studies in other countries (Masia et al., 2010), but those doubts are mainly based on healthcare professionals’ confusion and frustration (Honkavuo & Lindström, 2014) rather than their grief over the loss of an imagined identity. The latter may derive from traditional Chinese medical ethics, which presents the image of doctors as “heroic and benevolent saviours” who “study medical skills painstakingly” and “do their best to rescue the dying and to heal the wounded” (Guo, 1995; Yan, 2018). These ideals may have shaped the vision of many Chinese medical students. As a result, when professional caregivers realize that many lives cannot be saved by doctors regardless of how hard they try to improve their skills, it is a dream or an idealized identity rather than a goal that is destroyed.
Extreme Difficulties Due to the Strong Death Taboo and Inadequacies of the Healthcare System
Chinese professional caregivers interpret patient deaths on their shifts as bad luck and therefore feel uncomfortable. Although negative views about encountering death in daily life have been widely reported across the globe (Colclough, 2017; Georgijev, 2015), such beliefs among medical staff have rarely been observed outside of China. This illustrates the extremely strong death-related taboos in Chinese culture (Chan & Chow, 2006; Hsu et al., 2009).
After patient deaths, Chinese physicians and nurses have very little time, space, or energy to deal with their loss-related reactions, and they very often have to suppress their feelings. This is due to the inadequacy of the healthcare system and the heavy workload (Song et al., 2017; Zhou et al., 2017). For the same reason, access to professional support following patient deaths, which is criticized as “insufficient” or “not qualified enough” in other regions of the world (Strote et al., 2011; Wilson, 2014), rarely exists in Mainland China.
Contributions
As the first qualitative exploration of professional bereavement in Mainland China, the present study greatly deepens the understanding of this phenomenon in the Chinese context. Several major findings echo those from other parts of the world and reinforce the shared key features of professional bereavement experiences across regions: Lying across both personal and professional domains, the experience of professional bereavement involves a meaning-driven, comprehensive, multi-dimensional, and often disenfranchised process with both immediate and long-term influences. Moreover, the present study expands the findings of previous studies by revealing elements with “Chinese characteristics”: Professional bereavement in Mainland China is influenced by traditional Chinese medical ethics, Confucian familism beliefs, the strong death taboo, workplace violence against professional caregivers and inadequacies of the healthcare system there. These findings, on the one hand, illustrate how cultural and systemic factors can shape professional bereavement experiences and, on the other hand, contribute a valuable, unique piece to the theoretical puzzle of the phenomenon.
Limitations
Due to feasibility concerns, the data in the present study were collected exclusively from physicians and nurses in urban hospitals in one of the most well-developed provinces in Mainland China, which limited the generalizability of the findings. Moreover, constrained by the busy schedule of interviewees, the average duration of interviews was not long. However, the comparisons between the present results and those presented in previous literature indicated no detrimental influence on the depth of the findings in this study.
Reflexivity
Although the researchers tried their best to increase the trustworthiness of the study, the identities and experiences of the researchers inevitably influenced the research. C.Q.C., the sole interviewer and main coder, personally witnessed a physician’s grief after her loved one passed away in hospital; this event inspired her to conduct the present study but could have introduced confirmation bias. Moreover, C.Q.C. experienced slight death anxiety during the interviews and data analysis, so the participants’ negative feelings after patient deaths might have been mildly exaggerated due to her projections of her own feelings. In addition, because C.Q.C. and A.Y.M.C. reviewed related studies on professional bereavement before starting the present study, they may have brought preconceived ideas to the study. K.X., a cardiologist, was included on the research team in an effort to partially mitigate the biases induced by the other two authors’ lack of clinical experience.
Practical Applications
This study provides insights into how to prepare Chinese professional caregivers for and support them after a patient’s death. First, it is critical to introduce curriculums for medical and nursing students in which work-related grief is comprehensively discussed. Education is also necessary for the general public and managers of healthcare institutions to ensure that they do not ignore or even stigmatize professional caregivers’ grief after patient deaths. After professional caregivers experience patient deaths, it is imperative that they are provided with acknowledgement, time, space, and professional support. At the national level, more efforts are needed to build a stronger healthcare system, to prevent workplace violence against professional caregivers and to disrupt death taboos so that additional burdens during professional bereavement can be alleviated.
Future Studies
For future studies, investigating professional bereavement in contexts other than urban hospitals is imperative for a more comprehensive understanding of the phenomenon in China. Moreover, the issue of how interventions at the individual, institutional, and even national levels can benefit professional caregivers when they experience patient deaths is worth studying. To achieve such a goal, the development of a specific assessment tool for professional bereavement is necessary.
Conclusions
Professional bereavement experiences are meaning-driven, comprehensive, and usually disenfranchised. They involve multidimensional reactions and have both short-term and long-lasting impacts and both event-specific and accumulated impacts. Cultural and systemic factors can shape professional bereavement experiences. Professional bereavement in Mainland China is influenced by traditional Chinese medical ethics, Confucian familism beliefs, the strong death taboo, workplace violence against professional caregivers and inadequacies of the healthcare system.
Supplemental Material
sj-pdf-1-ome-10.1177_0030222821992194 - Supplemental material for Bereavement After Patient Deaths Among Chinese Physicians and Nurses: A Qualitative Description Study
Supplemental material, sj-pdf-1-ome-10.1177_0030222821992194 for Bereavement After Patient Deaths Among Chinese Physicians and Nurses: A Qualitative Description Study by Chuqian Chen, Amy Yin Man Chow and Ke XU in OMEGA—Journal of Death and Dying
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.