
Abstract
This cross-sectional and correlational study was performed in order to determine the relationships between the perceived loneliness and social support levels of Turkish oncology patients, as well as their quality of life and symptom management. A total of 370 oncology inpatients participated in this study. Data were collected using, the FACT-G Quality of Life Scale, the Multi-Dimensional Scale of Perceived Social Support (MSPSS), the UCLA-Loneliness Scale (UCLA-LS), and the Edmonton Symptom Assessment Scale. A negative advanced significant relationship was found between the MSPSS total scores (r = −0.754, p < 0.01) and the UCLA-LS total scores. As the social support levels of the patients increased, their loneliness levels were seen to decrease and their quality of life was seen to increase. The patients were found to experience the symptoms of fatigue, worry, and feeling unwell more often as their loneliness levels increased and social support levels decreased.
Introduction
Cancer, which is one of the most significant health problems worldwide today, is a disease that threatens human life in biological, psychological, social, spiritual, and economic dimensions. Being diagnosed with cancer is a very traumatic experience and can affect both the patient and his/her family. Cancer affects one’s life, self-esteem, body image, personal and social roles, and relations with family and the environment, and may increase the need for social support (Pehlivan et al., 2012; Şahin & Tan, 2012; Yıldırım & Kocabiyik, 2010).
Social support can be defined as emotional, material, and cognitive assistance that is provided to an individual by a network of people around him/her to cope with his/her emotional problems and strengthens his/her psychological dynamics under stressful and difficult conditions (Langford et al., 1997; Thoits, 1986). Social support may be provided by a social network that consists of family, friends, neighbors, or community members (National Institutes of Health National Cancer Instutite, 2021). An individual can feel cared for, loved, respected, and valued with social support
Perceived social support, on the other hand, is defined as an individual’s subjective opinions and satisfaction about the level and quality of social support provided (Pierce et al., 1996; Sarason et al., 1990). An individual’s perception of the support provided to him/her can be measured and evaluated. People can attribute different meanings to the events they are living through, depending on their past experiences and upbringing
The need of an oncology patient for social support increases because of the treatments, recurring disease, bodily changes, and pain. In certain studies on the subject, it has been reported that emotional loneliness increased in younger oncology patients, that the risk of loneliness was higher in patients who were constantly fatigued or had disrupted cognitive functions (Deckx et al., 2015). It also stated that high levels of loneliness were related to poor immune function, fatigue, pain, mortality, and poor health outcomes (Adams et al., 2016). Additionally, a lack of social support and high levels of loneliness have both been reported to possibly affect endocrine and immune systems by transforming into psychosocial stress (Nausheen et al., 2010) and increasing the production of proinflammatory cytokines following acute stress (Jaremka, Fagundes, Glaser et al., 2013).
In a study on the subject, cancer has been reported to cause significant emotional and social loads, and it showed that patients diagnosed with cancer experienced emotional distress, social isolation, loneliness, and anxiety because of the side effects of treatments (Ettridge et al., 2018). In particular, loneliness, which is a subjective, disturbing, and sad experience caused by a lack of social relations (Perlman & Peplau, 1984), has been reported to be an important psychosocial factor related to the severity of cancer (Nausheen et al., 2010), and both social and emotional loneliness has been highlighted to be prevalent among oncology patients (Deckx et al., 2015).
The symptoms arising from the disease process or the side effects of treatments can have a negative impact on the quality of life in oncology patients. On the other hand, loneliness and a lack of social support can also affect the quality of life of oncology patients and the symptoms they experience (Jaremka et al., 2013; Jaremka, Fagundes, Peng et al., 2013; Jaremka et al., 2014; Li et al., 2015; Queenan et al., 2010). In certain studies on the subject, it has been reported that lonely patients experienced more pain, fatigue, and depression, that loneliness increased the risk of immune irregularity, pain, depression, and fatigue clustering symptoms, and that loneliness affected physical and mental wellbeing (Jaremka et al., 2013, 2013, 2014).
In a meta-analysis study, it has been reported that loneliness was more prevalent among patients who suffered from a lack of psychological or social support, that loneliness had an inclination to rise along with the time that had passed after the cancer diagnosis, and that there was a negative relationship between a lack of social support, social function, and loneliness (Deckx et al., 2014). Alongside this, the risks of recurring cancer and breast cancer-related mortality were reported to be higher in socially isolated women, and it has been stressed that social networking, friendly relations, and family relations are thus important (Kroenke et al., 2017). In this context, it is very important to prevent temporary loneliness before it transforms into the condition of severe and chronic loneliness. Chronic loneliness can form the basis for depression, increase the risk of suicide, and endanger psychological wellbeing (Perlman & Peplau, 1984). On the other hand, social support can decrease the loneliness experienced by oncology patients and increase their treatment adherence, speeding up the healing process and increasing their quality of life (Li et al., 2015).
Social support is such an important resource that it can have effects that prolong the lives of oncology patients. It is thought that it is very important to examine the relationship between the perceived loneliness of the patients, their social support levels, and symptom control in order to understand the patients, make their adaptation to the disease easier, ensure symptom management, increase their quality of life, and make the correct interventions according to the problems at hand. On the other hand, the psychological, emotional, and social dimension of oncology patients is a neglected and disregarded issue in the Turkish health care system. Health professionals can usually only focus on the treatment and care of the patients, and the loneliness and social support levels of the patients, as well as their quality of life, can sometimes be disregarded.
Determining perceptions of loneliness and social support among oncology patients can help health professionals tackle these issues and make the appropriate interventions. Alongside this, international and cross-cultural studies on the subject, which can exhibit differences, could contribute to the current mass of knowledge. This cross-sectional and correlational study was performed in order to determine the relationships between the perceived loneliness and social support levels of oncology patients, their quality of life, and symptom management. Study questions were: • What are the levels of the quality of life of oncology patients and their perceived social support? • Is there a relationship between the perceived social support levels of oncology patients and their quality of life and symptom management? • Do the sociodemographic or clinical characteristics of oncology patients affect their loneliness and perceived levels of social support or their quality of life and symptom management?
Method
Sample
The study was performed with the participation of oncology inpatients being treated at the University hospital between June 15th, 2017 and December 15th, 2017. In the sample size selection, the formula used for sampling in a known universe simply random sampling was used. While the size of the sample was determined sufficient to represent the universe, a total of 870 inpatients being treated in the oncology and hematology clinics where the study would be conducted were taken as reference. The sample size for a known universe was calculated to be 355 with a 95% confidence interval and 4% error rate. Considering data losses, the data collection process was completed when 370 patients were reached (83.3%). Male or female patients of 18 years of age and above, who volunteered to participate in the study, had no cognitive disorders, could communicate with us, and could answer the questions, were included in the study. Patients who did not agree to participate in the study (n = 7), and patients who could not communicate because of poor disease prognosis (n = 32) were excluded from the study.
Data Collection
Data were collected using a patient identification form, the FACT-G Quality of Life Scale (Version 4), the Multi-Dimensional Scale of Perceived Social Support (MSPSS), the UCLA-Loneliness Scale (UCLA-LS), and the Edmonton Symptom Assessment Scale. The questionnaire was checked by pretesting it in a group of 12 individuals. After the pilot study, no questions that could not be understood or filled out could be detected. Patients who participated in the pilot study were not included in the sample of the study. The questionnaire and the scales were then applied through face-to-face interviews. Data collection was completed in approximately 18–20 minutes per participant.
Data Collection Tools
The Patient Identification Form
The patient identification form prepared by the researcher included questions on the sociodemographic and clinical characteristics. Patient identification form information was obtained from medical records.
The Multi-Dimensional Scale of Perceived Social Support
The MSPSS was developed in 1988 by Zimmet, Dahlem, Zimet, and Farley. The Turkish validity and reliability study of the scale was performed in 1995 by Eker and Arkar. The scale was revised in 2000 by Eker, Arkar, and Yaldız. The MSPSS is an easy-to-use short scale, which subjectively evaluates the sufficiency of social support received from three different sources, namely family, friends, and significant others (Eker et al., 2000). In this Likert-type scale, there are 12 items varying between “Absolutely no” and “Absolutely yes” regarding perceived social support. The scale has three subdimensions of four items each, namely the family support subdimension, the friend support subdimension, and the significant other support subdimension.
The family support subdimension: In this subdimension, the level of the support received from family members as perceived by individuals is measured. The family support subdimension consists of items 3, 4, 8, and 11. The friend support subdimension: In this subdimension, the level of the support received from people considered as friends as perceived by the individuals is measured. The friend support subdimension consists of items 6, 7, 9, and 12. The significant other support subdimension: In this subdimension, the level of the support received from spouses, lovers, or other significant others as perceived by the individuals is measured. The significant other support subdimension consists of items 1, 2, 5, and 10.
In this scale, subdimension scores are obtained by totaling the scores of all four items in a subdimension. The lowest score that can be attained from each subdimension is 4, while the highest is 28. The lowest score that can be attained from the total scale is 12, while the highest is 84. Higher scores indicate higher perceived social support whereas lower scores indicate that social support is not being perceived or that the individual is lacking social support. In this study, the Cronbach’s alpha reliability coefficient of the scale was found to be 0.94, and the Cronbach’s alpha reliability coefficients of the family support subdimension, the friend support subdimension, and the significant other support subdimension were found to be 0.93, 0.96, and 0.99, respectively.
The UCLA-Loneliness Scale
The UCLA-LS is a scale developed by Russell et al. to evaluate the loneliness perceptions of individuals. The scale was revised in 1996 by Russell. As a result of the revision efforts, Russell reported the third version of the UCLA-LS to be very reliable. The Turkish validity and reliability study of the scale was first conducted in 1984 by Yaparel. The 10-item form of the UCLA-LS Version 3 consists of 5 normal and 5 inverse coded items reflecting how individuals define their own experiences. The lowest score that can be attained from the whole scale is 10, while the highest is 40. Higher scores indicate increasing feelings of loneliness, whereas lower scores indicate lower levels of loneliness. In this study, the Cronbach’s alpha reliability coefficient of the scale was found to be 0.877.
The FACT-G Quality of Life Scale
The FACT-G Quality of Life Scale (Version 4) was developed by Cella (1992) to evaluate the quality of life of oncology patients. The Turkish validity and reliability study of the scale was performed by Çetiner et al. in 2004. The scale is a 5-way Likert-type scale that consists of 27 items and 4 subdimensions, namely bodily status, social life and family status, emotional status, and activity status. The total score that can be attained from the scale varies between 0 and 108. Higher scores indicate a higher quality of life. In this study, the Cronbach’s alpha reliability coefficient of the FACT-G Quality of Life Scale was found to be 0.90, and the Cronbach’s alpha reliability coefficients of the bodily status, social life and family status, emotional status, and activity status subdimensions were found to be 0.88, 0.67, 0.88, and 0.81, respectively.
The Edmonton Symptom Assessment Scale
The Edmonton Symptom Assessment Scale was developed by Bruera et al. (1991) to increase the quality of care provided to patients, and it includes the symptoms most commonly seen in all patients (pain, fatigue, nausea, worry, sleeplessness, loss of appetite, feeling unwell, shortness of breath, and other problems). The Turkish validity and reliability study of the scale was performed by Kurt and Unsar (2011). Patients are expected to self-report their symptoms and evaluate the severity of each symptom from 0 to 10 points. Each item in the scale is a subdimension on its own, and 0 points indicate the absence of a symptom, while 10 points indicate a very severe symptom (Kurt & Unsar, 2011). In this study, the Cronbach’s alpha reliability coefficient of the Edmonton Symptom Assessment Scale was found to be 0.81.
Data Analysis
Study data were analyzed using the IBM SPSS V23 package program. The compliance of data with normal distribution was examined using the Kolmogorov Smirnov test. In comparisons between data that did not comply with normal distribution, the Kruskal Wallis, Mann Whitney U, and Pearson’s chi-squared tests were used. Spearman correlation analysis was used in the examination of the relationships between subdimensions. Reliability analysis efforts were examined using Cronbach’s alpha coefficients. Multiple regression analysis was used to measure the magnitude of the relationships between variables. Quantitative data were given as means (minimum-maximum), while qualitative data were given as frequencies (percentages). The level of significance was taken as p < 0.05.
Ethical Considerations
The study was started after obtaining permission from the University Clinical Studies Board of Ethics (05.05.2017/number: B.30.2.ODM.0.20.08/924). Informed consent was obtained from all individual participants included in the study.
Results
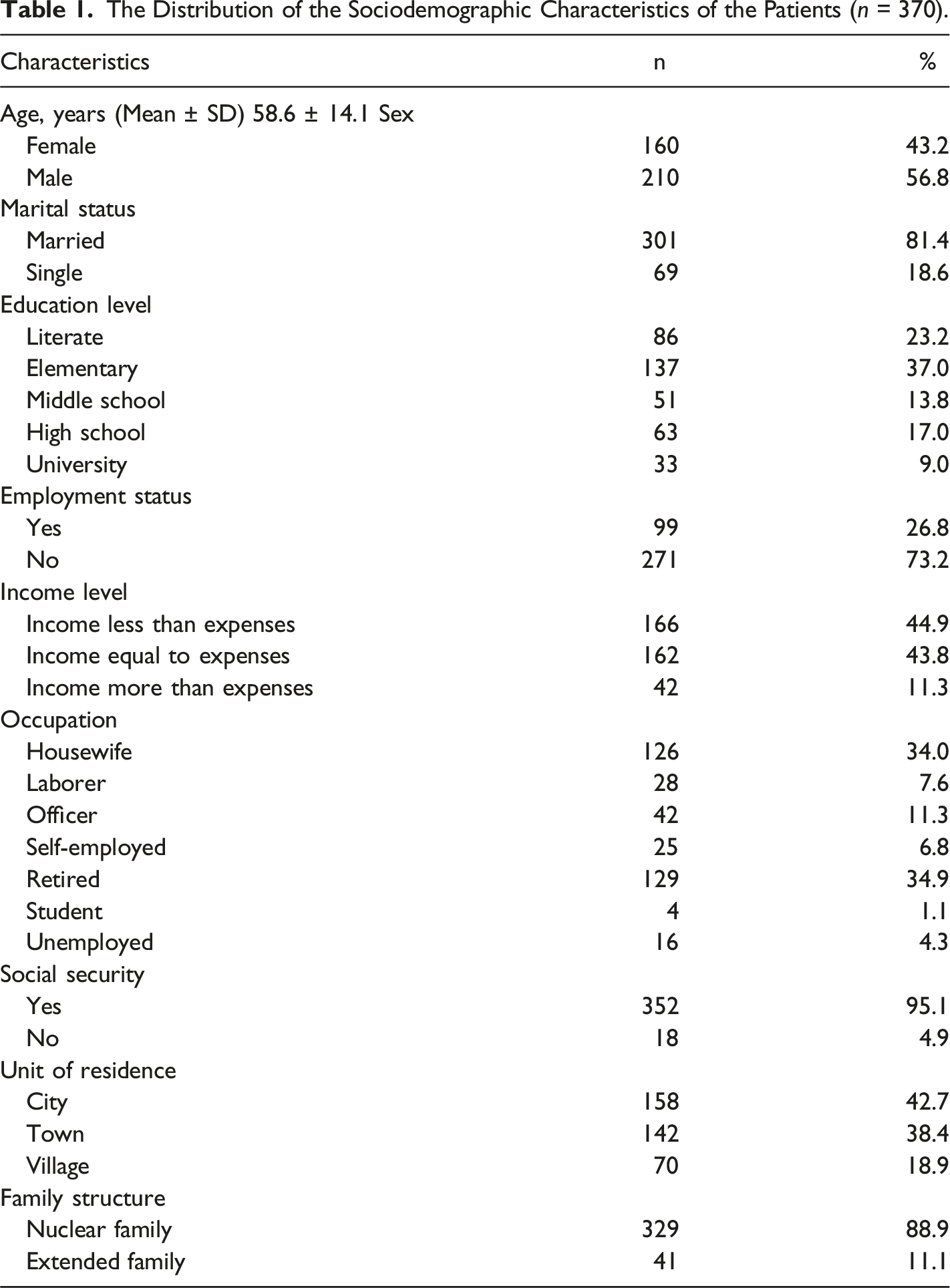
The Distribution of the Sociodemographic Characteristics of the Patients (n = 370).
The Distribution of the Clinical Characteristics of the Patients (n = 370).
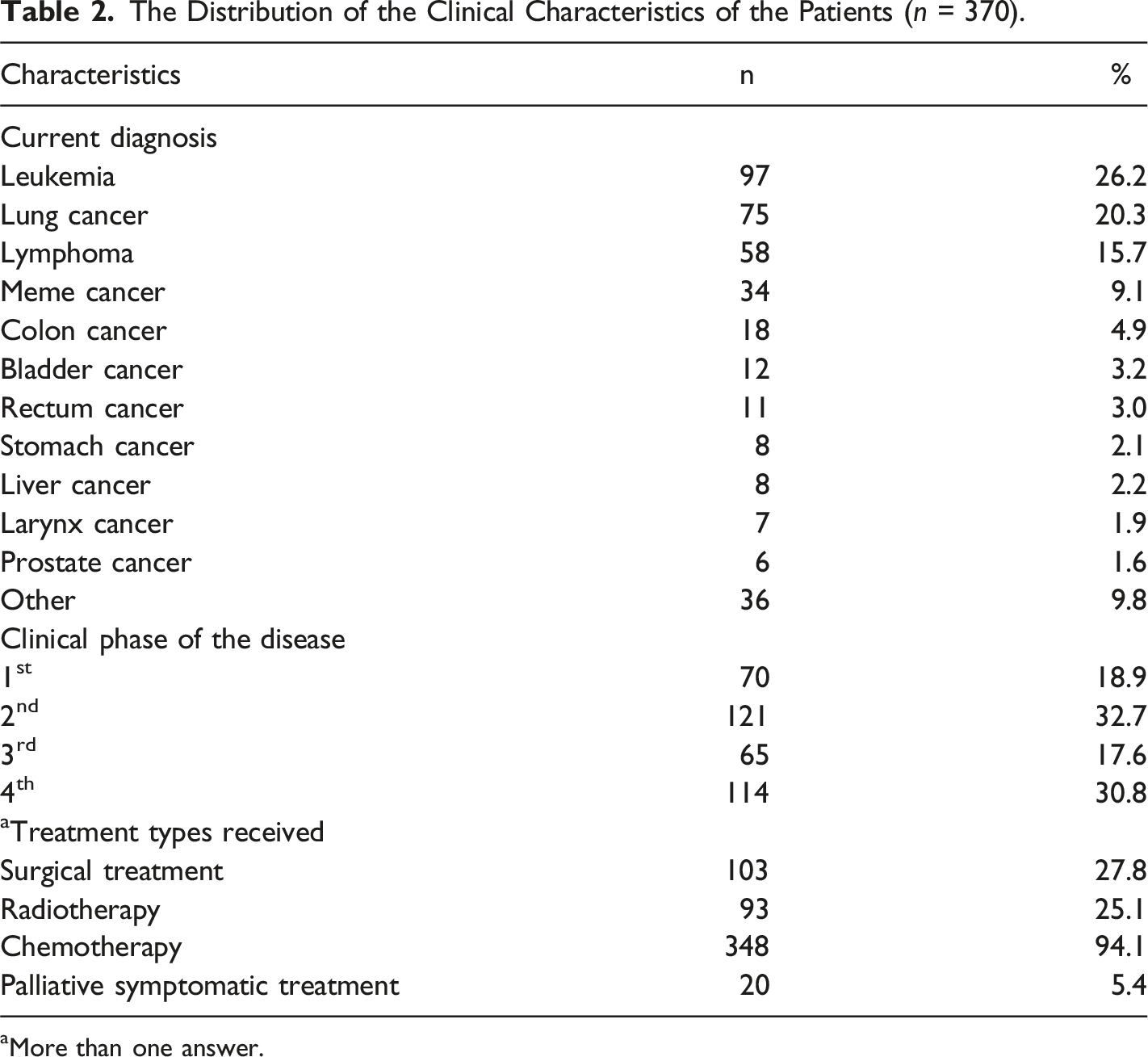
aMore than one answer.
Multi-Dimensional Scale of Perceived Social Support, UCLA-Loneliness Scale, FACT-G Quality of Life Scale, and Edmonton Symptom Assessment Scale Scores.
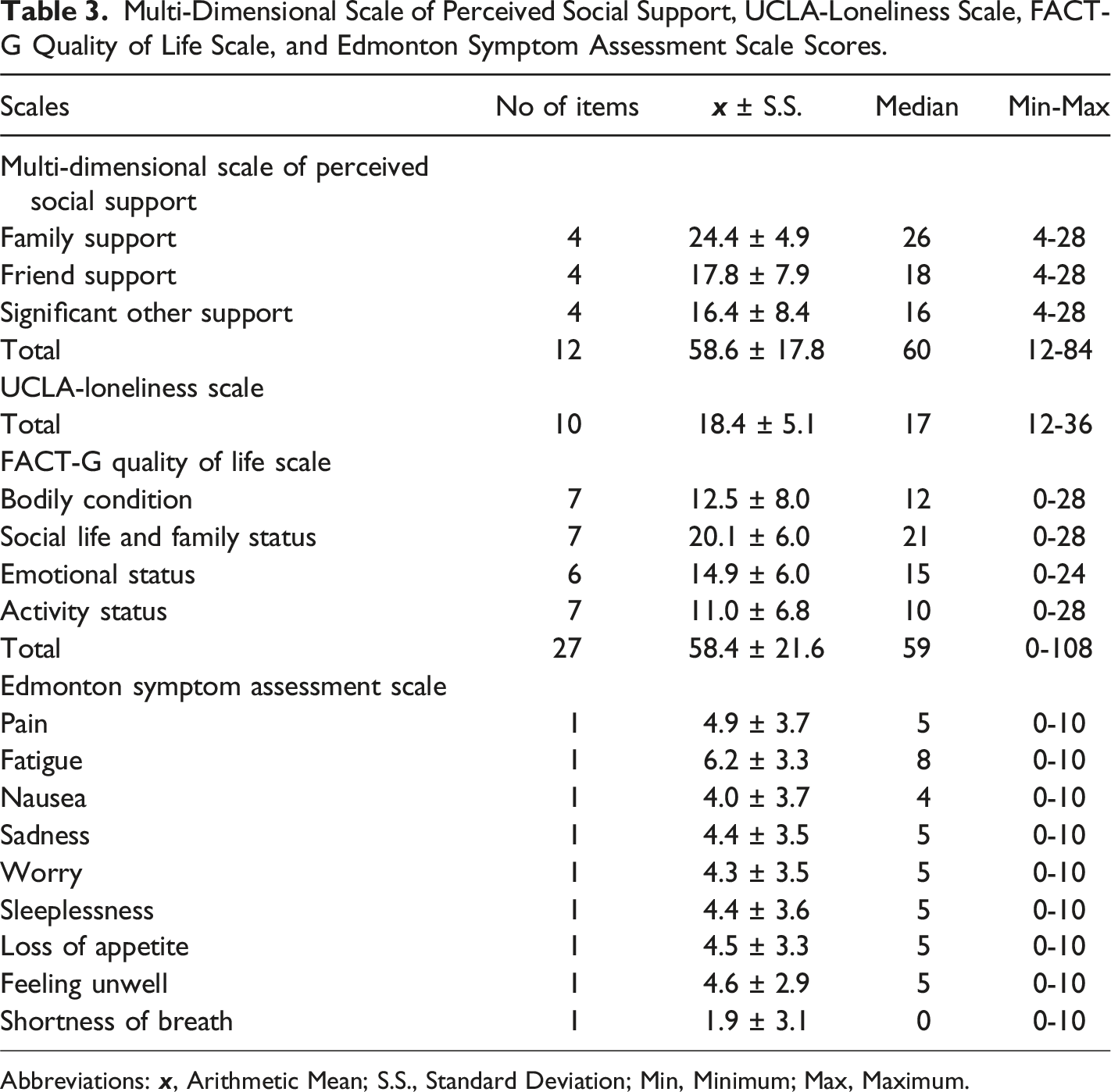
Abbreviations: x, Arithmetic Mean; S.S., Standard Deviation; Min, Minimum; Max, Maximum.
The Relationship Between the Multi-Dimensional Scale of Perceived Social Support, UCLA-Loneliness Scale, FACT-G Quality of Life Scale, and the Edmonton Symptom Assessment Scale.
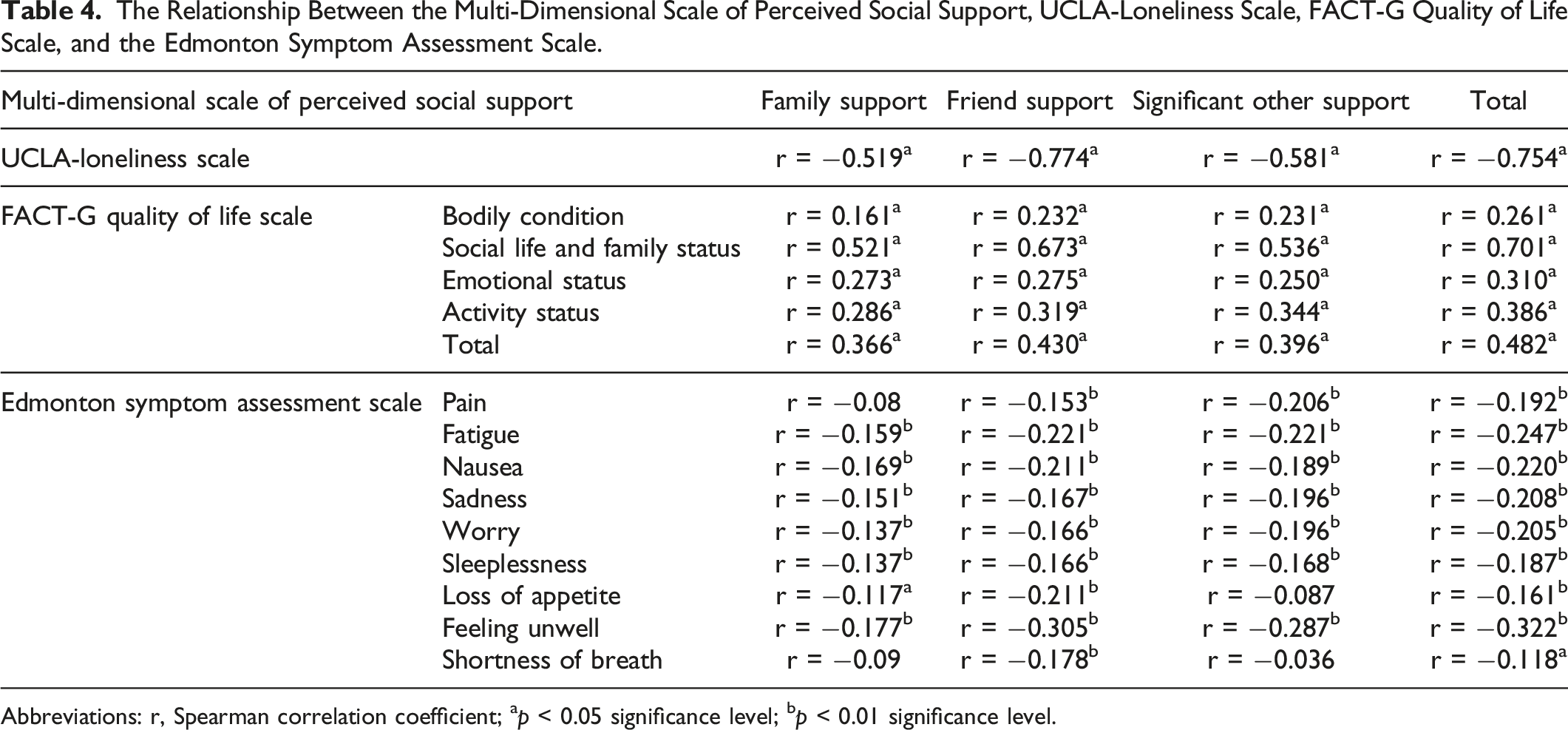
Abbreviations: r, Spearman correlation coefficient; ap < 0.05 significance level; bp < 0.01 significance level.
The Relationship Between the UCLA-Loneliness Scale and the FACT-G Quality of Life Scale and the Edmonton Symptom Assessment Scale.
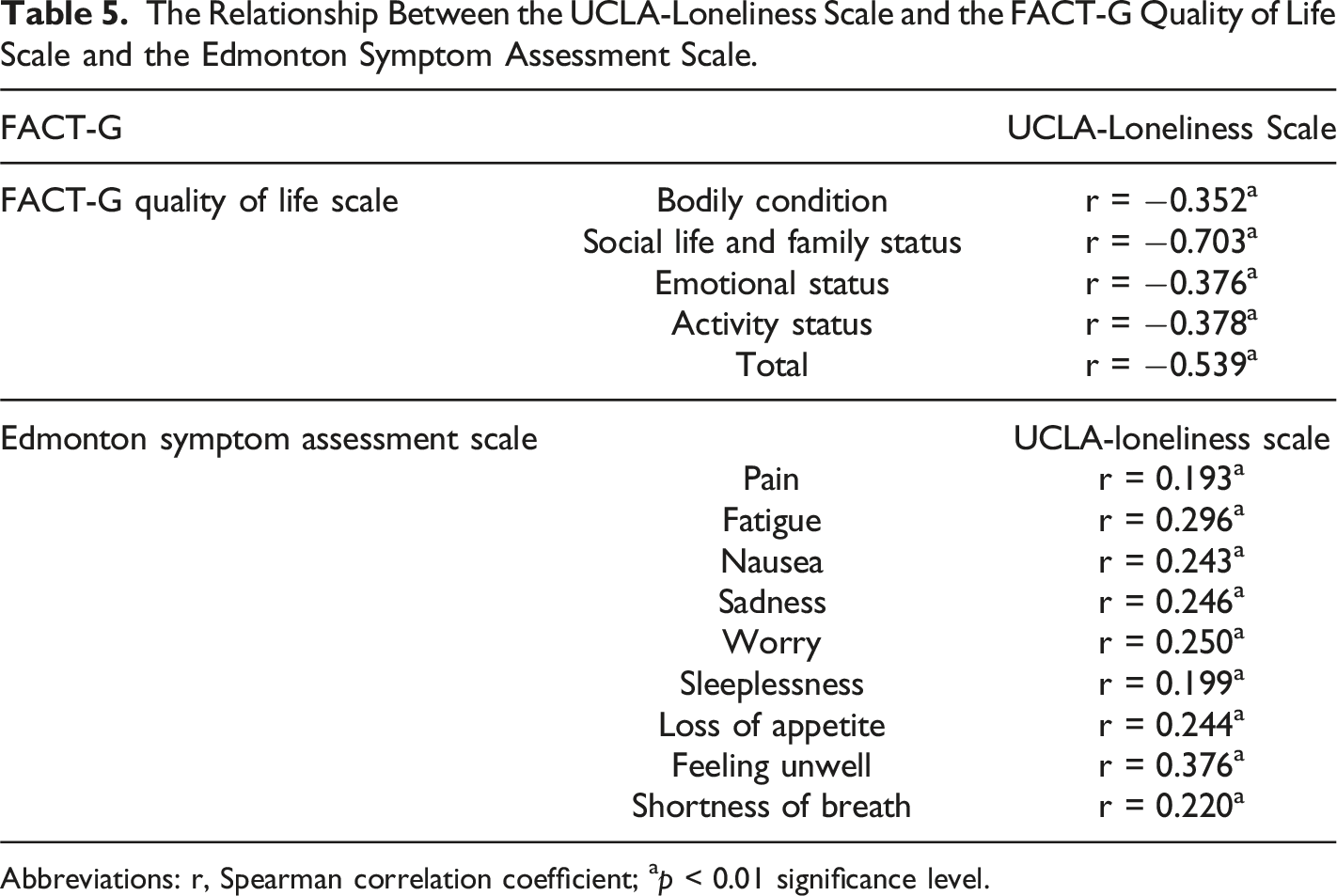
Abbreviations: r, Spearman correlation coefficient; ap < 0.01 significance level.
The Sociodemographic and Clinical Characteristics Affecting the Loneliness Levels of the Patients According to the Multiple Regression Analysis Performed.

F = 4943; p < 0.001; R2 (adj) = 0.197; VIF, variance inflation factor.
The Sociodemographic and Clinical Characteristics Affecting the Social Support Levels of The Patients According to the Multiple Regression Analysis Performed.
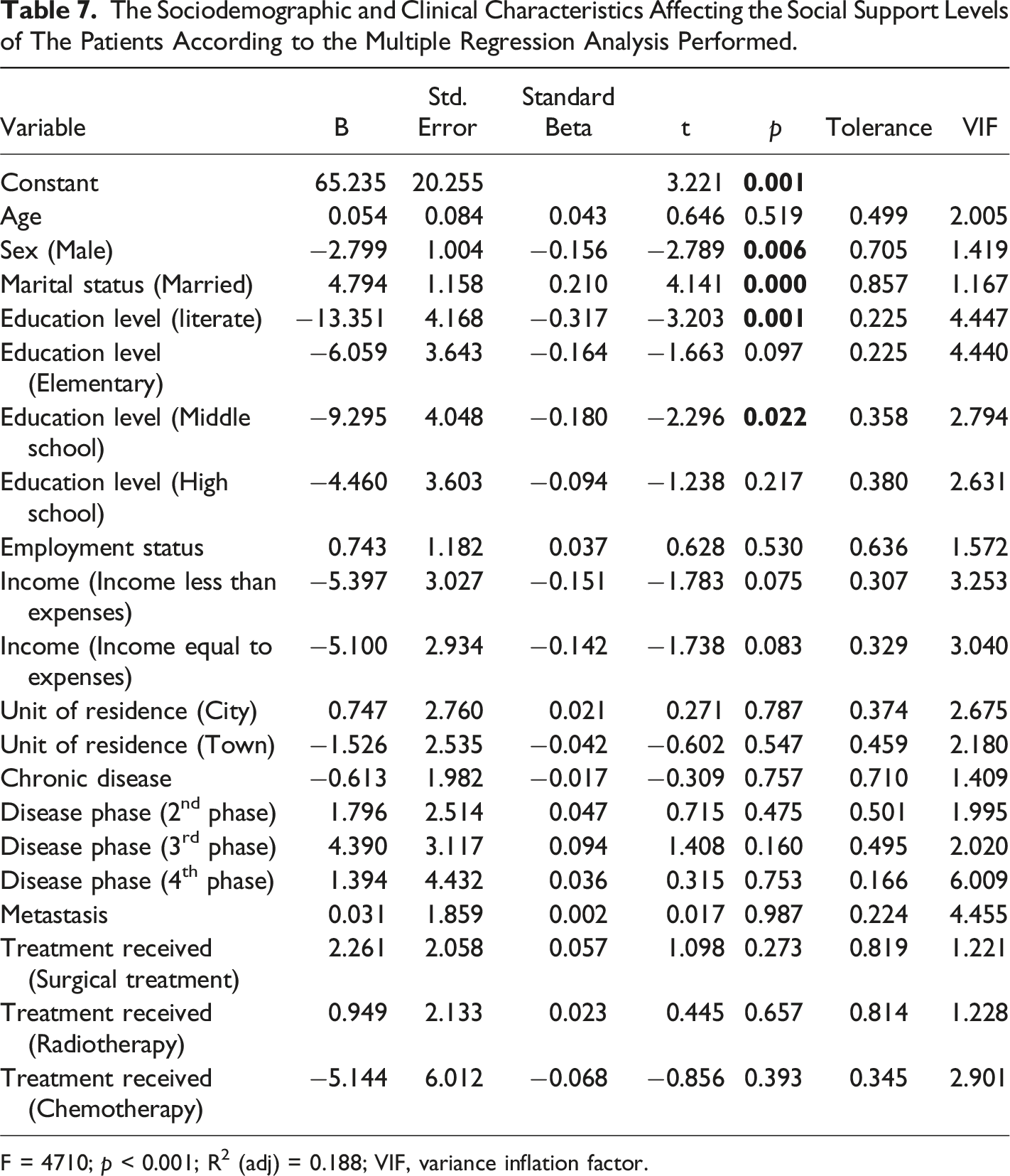
F = 4710; p < 0.001; R2 (adj) = 0.188; VIF, variance inflation factor.
The Sociodemographic and Clinical Characteristics Affecting the Quality of Life Levels of the Patients According to the Multiple Regression Analysis Performed.
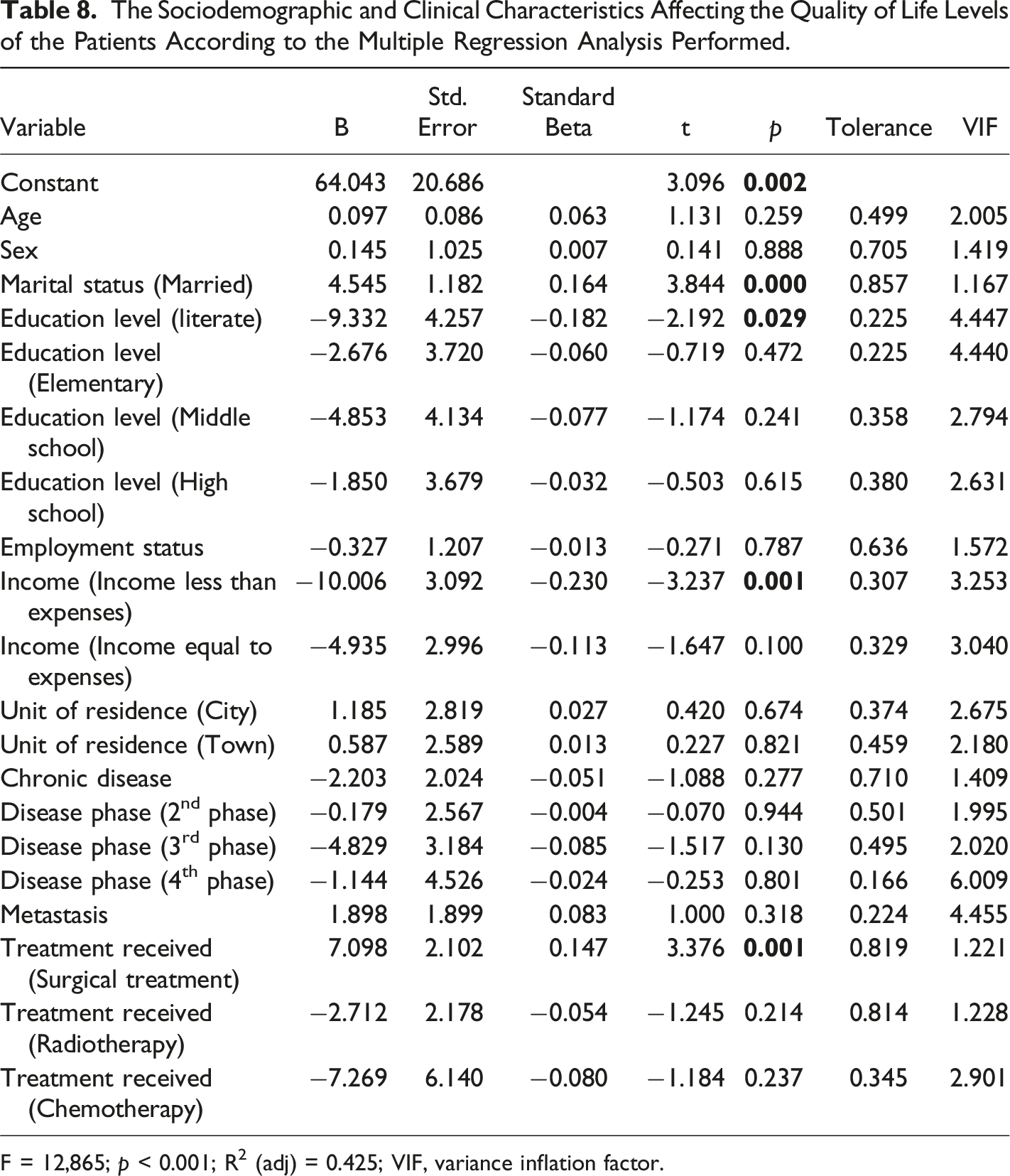
F = 12,865; p < 0.001; R2 (adj) = 0.425; VIF, variance inflation factor.
Discussion
The mean total score from the MSPSS was 58.6 ± 17.8. Given that the total score that can be obtained from the MSPSS ranges from 12 to 84 and that the higher the score, the higher the level of perceived social support, it can be stated that patients perceived themselves to have above average levels of social support and a high level of family support. For Turkish people, family is very significant factor in their lives, embodying social and cultural values, and the spiritual bonds that exist between relatives are very strong. In Turkey, family members generally take on the responsibility of caring for patients (Kuscu et al., 2009). In Turkish families, looking after a sick individual is seen as a duty that has to be fulfilled by his/her family members in line with cultural and religious values (Danacı & Koç, 2018).
In Turkey, the patient’s relatives thus try to manage all his/her problems, and provide physical, psychological, social and economic support. In particular, family members of advanced cancer patients often leave their jobs or reduce the time they spend working in order to meet these patients’ needs. They thus have less time than before to engage in social activities, and may even experience difficulty caring for themselves. The successful management of this situation necessitates that patients and their families become adapted to major changes in lifestyle (Danacı & Koç, 2018; Erdoğan & Koç, 1921).
Social support encompasses the support received from relatives, friends, and other relationships and positively affects health and well-being (Finfgeld-Connet, 2005). In Turkey, family ties tends to increase when the situation of the patient gets worse. This is particularly the case in highly traumatic diseases like cancer. In this regard, as support from family members and relatives increases, this helps the patient to cope better, to experience an increased sense of control over the cancer, to find it easier to adapt to and accept the disease, and, depending on the intensity and frequency of the support, perhaps even to be able to think about the disease in a more positive way.
The mean total score from the UCLA-LS was 18.4 ± 5.1. Given that the total score that can be obtained from the UCLA-LS ranges from 10 to 40, and that the higher the score, the greater the feeling of loneliness, the patients can be said to have felt moderately lonely. In the regression model using the UCLA-LS total scores of the patients as a dependent variable, loneliness was higher among male patients who were only literate or who had only attended elementary school, while they were lower among patients who were married. Being married carries with it the responsibility to look after the spouse and the children. Turkish society expects spouses to take on the responsibility of caring for someone who has cancer, however serious the prognosis. Cancer thus becomes an issue concerning the whole family, especially the husband or wife and the children, rather than being seen as the patient’s problem alone. Spouses become vital in ensuring that daily life and family routines continue as usual. Spousal support also decreases the patient’s sense of being alone (Danacı & Koç, 2018). The low loneliness levels of the married patients in the present study implies that their spouses were providing them with psychosocial support.
A meta-analysis on this topic found that loneliness was more frequent in those who had never married, were widowed, or were divorced, as well as among those who lacked psychological or social support, and that loneliness was not linked to factors such as the site of the cancer, the type of treatment, or the disease phase (Deckx et al., 2014). Howden et al. (2021) noted that patients residing in distant and rural areas were less likely to feel lonely than those residing in urban regions. In Dahill et al. (2020) study, the level of loneliness was higher in younger patients, in those whose disease was at an advanced stage, and those who had received radiotherapy or chemotherapy. Kraav et al. (2021) determined that there was a higher incidence of cancer in socially isolated men who felt alone.
The factors said to affect oncology patients’ levels of loneliness and social support vary in different studies; however, these variations may arise from the different social, clinical and sociodemographic characteristics of different patients (Deckx et al., 2014, 2015). The present study found that male patients had high levels of loneliness levels. With regard to upbringing and gender roles, men in Turkish society generally tend to feel they have to suppress their emotions, while women commonly share them with each other; women thus experience less loneliness because they communicate their feelings, while men do not seek other people’s help for psychosocial issues and stress. These factors may have played a part in the high levels of loneliness seen in the male patients. The traditional expectation that men will be “brave”, and the related prohibition on men from demonstrating any weakness or crying in the face of illness may also have had an influence on this situation.
Contrary to the present findings, Cramer and Neyedley (1998) found that men were reluctant to acknowledge that they felt lonely. The negative meanings ascribed to loneliness, and the effects that being lonely can have, may prevent individuals from discussing how they really feel. In terms of gender, this reticence is more prevalent in men. Men deny their loneliness because they believe they have to “act masculine”, and they remain silent even when they are in considerable distress (Cramer & Neyedley, 1998). Another study on this subject determined that, although the difference was not statistically significant, loneliness was higher in men, that social factors had an effect on this, and that women were less likely to have negative results in terms of accepting loneliness (Borys & Perlman, 1985).
The present study found a relationship between the perceived social support, quality of life, loneliness, and symptom management of the patients who took part in the research. In accordance with these findings, it can be said that the quality of life of patients improves, their loneliness levels are reduced, and the perceived severity of the disease changes as they perceive themselves to have a higher level of social support. Various studies on this topic have reported that high levels of loneliness in oncology patients are related to pain, fatigue, and a sense of mortality (Adams et al., 2016), as well as quality of life (Fanakidou et al., 2018; Theeke et al., 2012). Moreover, the risk of loneliness may be greater for patients who suffer from constant fatigue, or who have experienced cognitive disruptions; patients who felt lonely suffered higher levels of fatigue, pain, and depression (Jaremka et al., 2013, 2014).
Loneliness and perceived lack of social support may reduce an individual’s compliance with treatment. However, perceived social support can provide a cushion against disease, contributing to wellbeing and decreasing or balancing out the negative impacts of stress. Diagnosing fatigue and other symptoms in oncology patients may help to improve their quality of life. The emotional and behavioral responses that patients have to cancer can have a direct effect on the diagnosis, treatment, and prognosis of their disease.
Limitations of the Study
This study has certain limitations. Until comparable studies are conducted with patients with different sociocultural characteristics, the findings of this study cannot be generalized for all oncology patients. Since the population of the study consisted of patients with different types of cancer, the sample was not homogeneous. Evaluations, follow-ups, and monitoring regarding the loneliness, social support levels, and quality of life of the patients before and after the study were not performed. It is suggested that in further studies on the subject, both qualitative and quantitative methods should be used, and patients should be interviewed simultaneously.
Conclusion
A negative advanced significant relationship between the MSPSS and UCLA-LS total scores was found, where the loneliness levels of the patients decreased with increasing perceived social support levels. A negative, moderate strength significant relationship between the UCLA-LS and FACT-G Quality of Life Scale total scores was also found, where the quality of life of the patients increased with decreasing levels of loneliness. The regression model where the sociodemographic and clinical characteristics of the patients were taken as independent variables and their UCLA-LS, MSPSS, and FACT-G Quality of Life Scale scores were taken as dependent variables was found to be statistically significant. According to the findings of the study, loneliness levels were found to be higher among male patients who were only literate or elementary school graduates and lower among married patients, and perceived social support and quality of life were found to be higher among married patients.
Footnotes
Acknowledgments
We sincerely thank all of the oncology patients who participated in this study
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ondokuz Mayıs University Commission of Scientific Research Projects with the project number PYO.SBF.1904.17.004.