
Abstract
The management and delivery of bereavement care and support services present practical challenges. A national-level, qualitative study was conducted to examine the current practices in Singapore. The study’s purpose was to inform bereavement care practices by drawing from perspectives of service providers offering death, dying and bereavement-related services. This qualitative study was undertaken using focused group discussion (FGD) with service providers from the health, social and death-related sectors. Ten FGDs were conducted with a total of 69 participants. Thematic analysis yield two themes – identifying challenging circumstances to provide bereavement care and strategies for dealing with the gaps in service delivery. The service providers’ experiential knowledge could be borrowed to strengthen the current bereavement care practices for the good of the community. The findings have informed the reconceptualization of a local bereavement care and support service model, with the public health model as the recommended underpinning conceptual framework.
Introduction
Bereavement is defined as the experience of having lost a loved one to death of which the person is trying to adapt and it is a common experience for many at some point in their lives. Grief is a natural response to such a loss and it comprises ‘thoughts, feelings, behaviors, and physiological changes that vary in pattern and intensity over time’ (Worden, 2018, p. 18). Each loss is unique – whether it is the death of a family member, friend, colleague or loved one – and the need for bereavement support varies according to the personal needs and resilience of the individuals and families affected.
Majority of the bereaved individuals are reported to be resilient and able to employ their own inner and informal resources to cope and adapt to the loss (Bonnano et al., 2004). However, some are more at risk of developing long-term physical or mental disorders (Stroebe et al., 2001). One such vulnerable group is those who are affected by sudden and traumatic death, such as suicide and accident. These bereaved individuals are exposed to both trauma and grief (Doka, 1996), and thus are at greater risk of developing complicated grief reactions, such as suicide ideation, engagement in self-destructive behaviours or symptoms of major depression (Worden, 2018).
In addition to personal predisposing characteristics (such as attitudes, values, and beliefs) and relational factors (such as nature and strength of the bereaved-deceased relationship), review of risk factors that influence grief suggested that circumstantial factors may determine a bereaved individual’s vulnerability to loss and their adjustment to bereavement (Aranda & Milne, 2000; Stroebe et al., 2001). For example, the way terminally ill or dying patients are being cared for, the approach used to communicate the death of a person especially if it is a traumatic death, and the bereavement rituals performed may impact the bereaved individuals and families’ grief experiences (Becker et al., 2020; De Leo et al., 2020; Grande et al., 2009). Other bereaved individuals and families were found to be impacted on practical and financial matters that accompany the loss (Lancaster & Johnson, 2020). Grieving could be further encumbered by cascading life stressors (e.g. taking on new roles, daily life changes) particularly for those who are younger and those who lost a parent, partner or child (Eisma et al., 2021).
International Grief and Bereavement Practices
It has been widely argued that a universal bereavement service is unnecessary; bereavement support service should be offered in response to individually identified needs and risks through appropriate levels of service provision (Department of Health, UK, 2005). A quantitative review of outcome studies had also concluded that offering psychotherapeutic interventions to resilient individuals is unnecessary, unhelpful, or even harmful (Currier et al., 2008). One emerging approach to bereavement care provision is the public health model of bereavement support, such as that recommended by the National Institute of Clinical Excellence in the United Kingdom (NICE, 2004). NICE had recommended a three-component model of bereavement support. The first component recommends that information on the bereavement experience should be offered to all bereaved people who are encouraged to utilize their informal support network for support. The second component is catered to those who are assessed and identified as those that require a more formal opportunity to review and reflect on their loss experience, with the support of non-specialist service providers such as volunteer bereavement workers, befrienders, faith-based and other community groups. However, an onward referral must be established if more complicated grief reactions emerge. The third component recognizes a minority group of bereaved persons who require specialist bereavement support for complicated grief reactions (NICE, 2004). Similar advocacy was made in Australia, where a public health model to bereavement in palliative care was proposed as a systematic and evidence-based framework to meeting the needs of bereaved persons and families (Aoun et al., 2012).
Grief and Bereavement Support Service Landscape in Singapore
Currently, grief and bereavement care and support are available via the psychosocial services in individual hospitals, home care services, inpatient hospices, and some community social service organizations. However, the situation is complex as there is a lack of understanding of the service model and approach adopted by the various organizations. There is also no consensus amongst organizations on possible service outcome measures that may define good care. Some of the common one-time or ‘touch-and-go’ bereavement support services provided include attending wake, sending condolence card, conducting a follow-up telephone call or home visit, and making referral for bereaved individuals who need grief counselling. Some other ongoing programs include financial assistance, support groups, counselling, memorial services, talks or workshops, and befriending program. Organically, in the community, faith groups and grassroots volunteers also provide services such as prayers, funeral services, support groups and/or spiritual counselling for their members.
While most caregivers can cope with grief and bereavement, unpublished local surveys of bereaved families amongst palliative care services showed that about 10% of them suffer from bereavement-related morbidity. Less is known for deaths not seen in palliative care services or when death is unexpected. It is truly a challenge for the health and social care sectors to identify individuals who are at risk of complicated grief and to offer bereavement care and support that address individual needs through appropriate levels of service provision.
Recognizing these challenges, we embarked on an exploratory study of bereavement experiences and supports needs of the bereaved individuals, and the service delivery experiences of local, current bereavement-service providers. The aim is to inform bereavement care practices and develop a model of care that could be applicable to the whole of community, or even at the national level. This present paper focuses mainly on the gaps and challenges in the current provision of bereavement care, as well as the hope for bereavement support services in the future, from the perspectives of service providers.
Methods
With the approval from the Singhealth Centralised Institutional Review Board approval (CIRB ref: 2017/2807), a qualitative approach using focused group discussion (FGD) was used to examine the provision of bereavement care and support by the various service providers. The practical guide developed by Wilkinson (2008) was applied as a guide in planning and executing the FGDs. This included the design issues, ethical issues, planning of focus group schedule and preparation of a typical FGD session. Using a standard semi-structured discussion topic guide, we engaged in in-depth discussions with the participants who related their experiences, through which the challenges, gaps and hopes for supporting bereaved persons were articulated in the participants’ own words.
Identification of Participants
The participants were selected and included in the FGDs by invitation only; stratified and purposive sampling techniques were used to ensure presence of participants from diverse professional disciplines and from multiple healthcare/social service settings. The identified potential participants were those whose vocation required them to address issues related to death, dying and/or bereavement with their patients or clients, and their families. This included service providers in various healthcare settings (e.g. hospitals, hospices) and community agencies (e.g. eldercare centres, social service agencies) who come into contact with bereaved individuals and families.
To be eligible, the participant had to be involved in direct care of patients and/or bereaved family caregivers (e.g. doctors, nurses, medical social workers, and other allied health professionals) or provided bereavement support services in the community (e.g. counsellors, psychologist, social workers and therapists) or worked in death-related services (e.g. funeral directors and insurance agents), and had at least 2 years of professional experiences. In addition, we also recruited faith leaders and grassroots volunteers who had been serving the community on death-related issues for at least 2 years.
In our invitation emails, we included the participation information sheet to provide the potential participants with information about the study and opportunity for clarification. On the day of the FGD, the study was explained face-to-face using the participation information sheet again and a written consent was sought before the FGD commenced.
We targeted to recruit 80 participants. A total of 127 invitations were sent out to the service providers and 69 were recruited successfully. Among the 58 who declined the invitation, 32 of them gave the reasons for declination, of which, unavailability to attend the scheduled session was the main reason (36.2%), followed by those who perceived themselves as having insufficient experience serving the bereaved persons to provide contribution to the FGD (6.9%).
Data Collection
A total of 10 FGDs with 69 participants from different work settings and professions were conducted, with participants assigned to focus groups that were closest to their work industry or profession. The groups formed included service providers from health care sector, social care sector, funeral industry, insurance industry, children and young persons’ specialists, grassroots organizations, and faith groups. The FGD was held at one of the research sites, with convenience to the participants and neutrality as two key considerations when deciding on the setting. The average length of a FGD was 120 minutes (range, 110–129 minutes). FGD guide was used to focus the discussion on topics such as current service provision, vulnerable clients, service gaps and challenges, and hopes for better future bereavement support services for the bereaved. The participants completed a demographic sheet, which inquired of information such as the practice setting, occupation, and number of years of relevant working experiences at the end of the FGD. Each FGD was facilitated by at least one facilitator and had a note taker; bigger groups had a co-facilitator. All the facilitators had experience facilitating a FGD and were briefed on the FGD guide to achieve a common understanding. All the FGDs were conducted in English language, audio-recorded with permission, transcribed as verbatim and analysed using NVivo.
Data Analysis
All the transcripts were checked against the audio file for accuracy before the data were coded and analysed by the first author and second author, who were the main researchers for the study, and were trained in social work and qualitative research methods. To enhance credibility of analysis, each of the 10 transcripts was analysed and coded independently by the first author and second author (Nowell et al., 2017). The rationale for involving only two researchers in the coding and analytical process were also for practical reasons: active involvement of the two researchers in data collection, ability to maintain a consistent analytical approach, and the small number of transcripts.
Using Braun and Clarke’s thematic analytical method, codes revolving around the experience of providing bereavement care and support were organized and categorized into sub-themes and themes through the process of initial coding, focused coding and axial coding (Braun & Clarke, 2006). The transcripts were read and re-read to search for meanings and patterns, iterative coding was performed with additional themes identified, codes re-categorized and themes revised. Once all the themes and sub-themes were identified, these were reviewed and compared between the two authors. In the peer debriefing, there was an exchange and examination of how their thoughts and ideas evolved as they were engaged deeply with the data. Differences in interpretation – mainly in the categorization of sub-themes and choice of words – were discussed and resolved to reach a consensus. The preliminary findings were also presented and discussed across different platforms to test the findings and interpretations with the research team, participants and other service providers. Finalized themes with verbatim that encapsulated the semantics of the themes were selected and presented in this paper.
Results
Demographics
Socio-Demographics of Focused Group Discussion Participants.
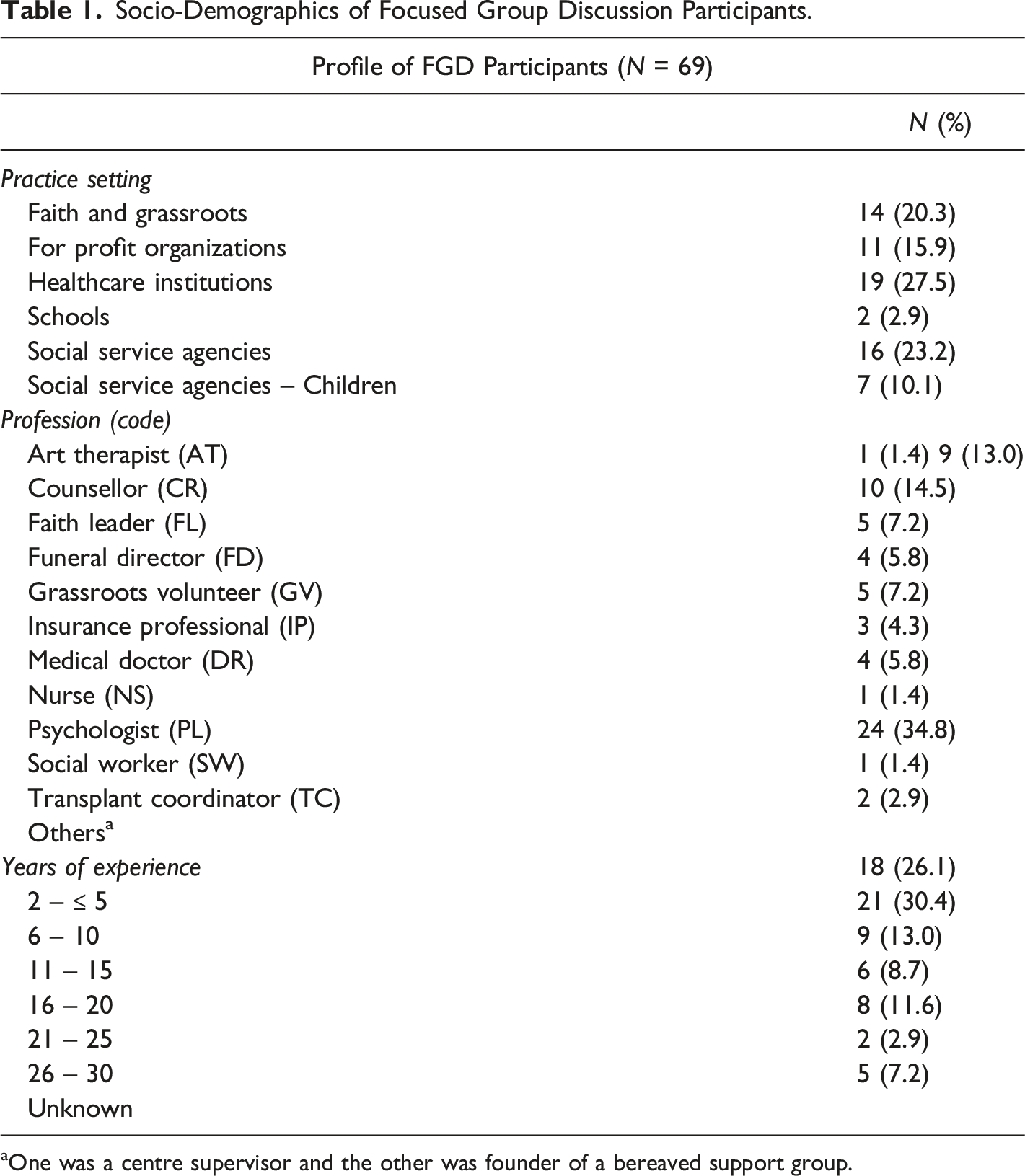
aOne was a centre supervisor and the other was founder of a bereaved support group.
Themes
Themes and Sub-Themes.
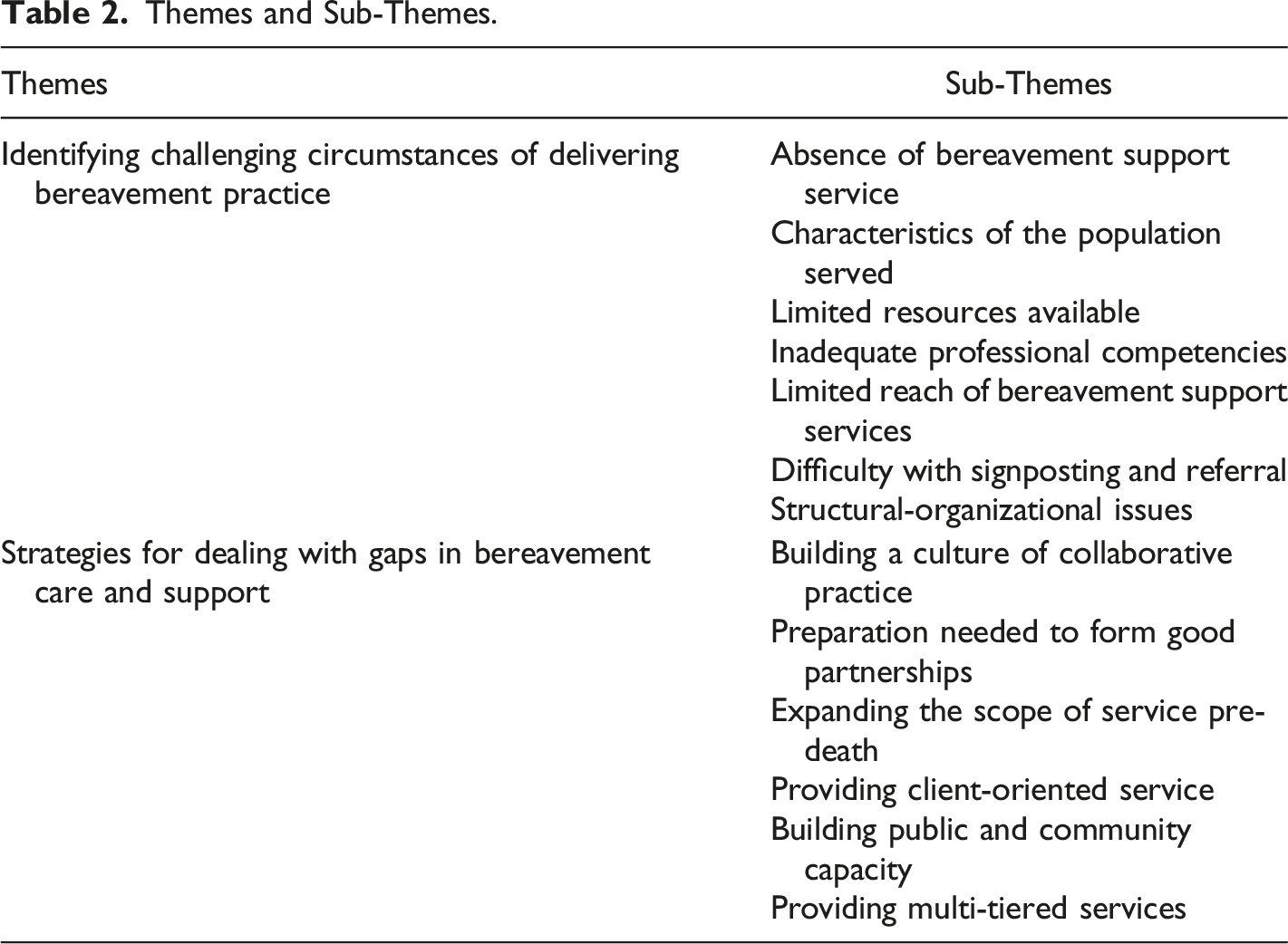
Theme 1: Identifying challenging circumstances of delivering bereavement care
Subtheme 1: Absence of bereavement support service. The need to process with a bereaved individual his/her grieving experience post-death was mentioned by the FGD participants. Yet, the service was said to be ‘lacking’ or ‘minimum to none’. One doctor expressed this view as follows: ‘… when [patients] die, most of the time [the service] ends. Sometimes we call them [bereaved family] one or two weeks later, sometimes maybe a few months later, but there isn’t really any follow up … most of the service is pre-death. Death sort of ends the service’. (FGD02-01-DR)
One social worker also highlighted the absence of an organization that specializes in grief and bereavement services as a salient service gap: ‘… it really hit me, the question that she [patient’s family member] pops to me is like, “Here in Singapore, we have family service centres serving families; we have other centres serving other people suffering from diseases, [why] we don’t have a bereavement centre? … like, upfront [one] knows it is the place that [one] can go and is open to all. No matter which stage of grief [one] is in – maybe memorial, anniversary, or very acute stage, [one] can still choose to come and go whenever I need”’. (FGD08-07-SW)
Subtheme 2: Characteristics of the population served. The nature of the population served was mentioned as one of the challenges faced in the delivery of bereavement care services. For example, it was said that nothing much could be initiated if the bereaved chose to withdraw into their own grief or were not ‘willing’, ‘ready’ or ‘open’ to receive help. One of the social workers in this regard said:
‘Sometimes [it] is not that we do not [do the preparation work] (i.e. with death in view in the treatment discussion); I think no matter how much we prepare, it also depends on the receiving end, what they select to listen to and not listen to, at times. I think that is also another challenge’. (FGD08-06-SW)
Trust issue was highlighted by some participants as one of the important factors for an effective helping relationship. In this regard, the lack of opportunity to engage the caregivers prior to the death was highlighted by one social worker as one key reason for the lack of trust: ‘… for patients who we [had little contact time or] don’t have a lot of rapport with, but we know that they passed away, we will follow a phone call to the family in a few days’ time after they’ve settled down [to] see how they are coping. Most of the time because there is no relationship, they also won’t tell us’. (FGD08-03-SW)
Another social worker stated that religion was also a factor that could influence the helping relationship: ‘…. [religion] is a way we call them and get them to share but it does take time. We go slow with them because it’s very, very hard for them to express that they are angry for what happened because that’s frowned upon in the religion, that you are blaming God’. (FGD07-02-SW)
Added to the challenges were the presence of complex family dynamics, such as families with pre-existing conflicts or family secrets. Working with a bereaved person who was a minor was also recognized as an added barrier by one doctor: ‘… when you’re working with a young client, there are always concerns around consent, access, the ethics of speaking with a young person. Therefore, much as you realized there is a lot of work to do, you often have to negotiate a portal of entry to even gain that conversation with the child … Somebody who just needs to give us permission to even talk to him or her. So, that’s something that is an inherent challenge’. (FGD03-07-DR)
Subtheme 3: Limited resources available. Lack of manpower was an issue commonly reported by the participants when they verbalized the struggles with performing multiple roles – to provide bereavement support in addition to their usual duties of managing the care of new and existing patients and their families. Closely related to the lack of manpower was the lack of funding and lack of time as expressed by one social worker: ‘… working at hospital is that you always have new admissions, so you are always caught up with the new cases and the cases who have been discharged or passed on, probably will take a second seat, so I think that is a difficulty …. how are you going to juggle with active cases [and] who have passed on? ... one phone call is definitely not enough. If you work at the setting long enough, you will have seen many deaths, [and] you will never be able to catch up with the calls’. (FGD-080-09-SW)
Subtheme 4: Inadequate professional competencies. Although the participants said that they had some knowledge on grief and bereavement, they highlighted that they were still ‘at a loss of what to say’ when they were with the bereaved client. One such view expressed by a social worker was as follows: ‘I think all of us went through grief and bereavement classes, we know in general what is all about but somehow sometimes [when] we deal with patient and family [who are] going through grief and bereavement, we are at a loss of what to say. Most of the time we actually do not say anything because we all know that sometimes silence may just do the work itself …’ (FGD08-10-SW)
The importance and readiness of ‘self’ noted by another social worker was as follows:
‘I actually feel that it takes more than training; it is not about knowledge, it’s not about knowing what to say, [not about] knowing some Victor Frankl’s [work], but it’s really a lot about the being of the worker: am I able to sit in this? ... having examined my own values about loss, my values about life, my own values about all these things, like meaning-making and I think that is the challenging part for me ...’ (FGD08-11-SW)
Subtheme 5: Limited reach of bereavement support services. The low participation rate in purposefully developed services for the bereaved individuals and families was highlighted by the participants. One such under-utilized service was the annual memorial service mentioned by a nurse: ‘Per month we have about 150 deaths … we do this [memorial service] like every four months, so we should easily have at least 600 families right? But we are getting about 20 families each time to come back’. (FGD02-03-NS)
One social worker also mentioned that the place of service provision was a potential barrier although the bereaved families needed help: ‘… I am trying to invite them [the deceased patient’s family] for the remembrance service and subsequently the patient’s daughter got back to me and told me that she finds it very hard for her to talk to anyone right now. She knows she has a need, yet at the same time she wants to be detached from the hospice team. She finds that we are very caring and the care also kind of gives her pressure’. (FGD02-06-SW)
Subtheme 6: Difficulty with signposting and referral. The questions about where to refer the bereaved individuals to get help or even if such grief and bereavement services existed were commonly raised by the participants. One funeral director opined that the lack of clarity of services available was one critical factor: ‘… as a funeral professional, I can even spot which family needs help, and this sort of help is not like financial or in terms of service that is required, it’s actually more of the grieving process itself... But I don’t think there is a very clear-cut or informative platform that tells the industry players or anyone ... “oh, there is this agency … that’s actually specialized in grief counselling.” So, I don’t know how they can support themselves after the funeral is over’. (FGD04-02-FD)
Subtheme 7: Structural-organizational issues. Structural-organizational issues were frequently raised by the participants. One such key issue raised by a doctor concerned the funding model, for which follow-up bereavement support was time-limited: ‘… the way we are funded, the healthcare model, is such that after a patient dies, for example an adult with two children, we are expected to wrap up the case a month after and we will not be funded for any care that happens afterwards’. (FGD03-07-DR)
Organizational barriers were also mentioned by some participants. These included the organizational mission which determined the types of clients served and length of service, the lack of protocol for timely referral to appropriate bereavement support services and the practice model. In this regard, drawing of the service boundary was emphasized by one social worker as a major barrier to meeting the needs of the bereaved persons seamlessly: ‘… we tend to box up and draw boundary and we forget that whatever we are providing should be for the betterment of the client. We should look at the needs of the clients, wanting seamless care rather than … they [having] to move on to different agencies for different type of resources’. (FGD01-06-SW)
Theme 2: Strategies for dealing with the gaps in bereavement care and support
Subtheme 1: Building a culture of collaborative practice. Some participants advocated for a culture of collaborative practice so that services could be better coordinated and delivered to meet the needs of the bereaved families. Connections and conversations with the relevant service providers was recognized by one social worker as one of the prerequisites: ‘… collaborative practice is not something new with [Organization A], … there are platforms created where all the agencies come together and [Organization A] actually opens doors to share information. The idea is we [service provider] connect with the right person [agency counterpart] and the person saw the issues that we were facing, and they helped to open the door. So, I think, to build the culture of collaborative practice is where we really start to have conversations; we recognize what the challenges are’. (FGD02-05-SW).
It was emphasized by the participants that communication between service providers about a common case seen would need to be purposeful, with an open attitude towards practice, as well as sharing of experience and necessary information. However, this was currently seen by a nurse as lacking in practice: ‘I must add that [Organization B] is a really very protected place, because I also encounter a lot of difficulty working with the professionals in [Organization B]. Even the social workers are very reluctant to share their story with us [about] the same patient that they’re seeing and I’m seeing. They are very reluctant’. (FGD02-03-NS)
The importance of establishing forms of partnership, at institutional level or case-by-case basis, was also pointed out by a counsellor: ‘In terms of support for people who lost family members … Sometimes they need to repeat their story many times to different service providers. It’s such a struggle for them sometimes. So, can we make this process more person-centred? To become easier and more accessible? ...’ (FGD07-04-CR)
Subtheme 2: Preparation needed to form good partnerships. The need for preparation was highlighted by the participants to establish a good partnership with external agencies for the best interest of the clients they serve. For example, one medical social worker stated the importance of making efforts to engage other partnering agencies early enough so that the relevant workers were able to engage and establish a relationship with the surviving family: ‘… we realized that when the partners come alongside us before death, they are introduced at the hospice before death, the success rate of continuing bereavement [support] is a lot higher. Some of the FSCs [family service centres] that already see the family before death, we also ask them to come …. Then, we realized the success rate is higher’. (FGD02-07-SW)
Subtheme 3: Expanding the scope of service pre-death. Some participants highlighted that bereavement care did not happen only after death. Rather, essence of the care should be incorporated in the patient care phase so that the healing process could begin when death occurs. As expressed by one social worker, it included acknowledging the loss, looking into anticipatory grief, conducting ACP conversations, and making sense and reconciling their losses: ‘… we see the need to look at end-of-life care or even aging issues in which there are a lot of losses, both for the elderly as well as for their family members; [end-of-life care] must be developed, but I think [we are] not quite there. We have seen some of our home care cases deteriorate at home and when that happens the social worker is activated to go in and provide emotional support. I think part of that broad stroke is also to prepare for the loss and to see how they are journeying those final days with the loved one … so you just walk, because you already know them for a while already’. (FGD08-11-SW)
The importance of work near the point of death was also emphasized by the participants. For instance, one social worker mentioned the importance of guiding and preparing the family for the death, especially if the surviving family includes a young person: ‘It’s the preparation work that is very crucial in preparing children for the last moment … even if the case is referred last minute, and you know that the patient is dying, we still make sure that we prepare the child first, with regards to what he/she will see in the room later on. And then we cushion the child in bringing [him/her] in, or whether if he/she wants to go in’. (FGD06-03-SW)
Subtheme 4: Providing client-oriented service. The need to provide bereavement support services, even beyond organization boundary to enhance continuity of care, was recognized by the participants as they realized that death might not happen within their services. One social worker acknowledged that even if death happened in her organization, she could not support the bereaved family forever: ‘… we are always talking about organization, can we break this barrier? Like okay I belong to [Organization C] but because of certain [exceptional] case, can I be sent to the bereavement counselling centre so that that patient family doesn’t have to travel back to [Organization C]? … I am very willing to just go over there to see that family because it is like really cross organizations, but I still get my pay from [Organization C]’. (FGD02-06-SW)
Client-oriented services also included forms of practice that are culturally appropriate. One counsellor highlighted the need for service providers to be flexible, and tailor-made their services to address the needs of the bereaved family: ‘Sometimes when the [patient] passed on, the clients might be alone, and children in prison. They looked to us as their own children, their own families, so our case officers actually did go and there were some instances where the [Muslim] family … allowed us to help wash the deceased. We also accompanied families to the burial site. I think that is very important and … I feel that I am able to do the utmost for my client. It’s not just centre-based when the families come [to the centre]’. (FGD07-03-CR)
Subtheme 5: Building public and community capacity. The participants advocated for greater public and community awareness and sensitivity towards the needs of the patients, caregivers and bereaved families. One such view expressed by a faith leader was as follows: ‘… the community [public] might be confused sometimes. Emotional challenges and spiritual challenges are different although they look the same and seem the same. But [it’s] really to create awareness in the community [public] to not treat them on the same note. So, I guess this awareness is critical, in my opinion, to the success of helping more bereaved families or people involved, and I guess education at large definitely will help …’ (FGD09-04-FL)
Public education was said to be one key approach to not only increase greater awareness in the public and community, but also to promote grief literacy and hence promote the readiness to talk about death. This was elaborated by one counsellor: ‘… one of the struggles of the bereaved is actually the need to be understood and the respect for the way which they grieve and there is no time limit. Some of the bereaved are told: “Two years already, you should get on with life”, or “Six months already, why are you still crying?”… “Daddy died [three weeks] already, what’s wrong with you?” …. I think that education for that respect and that understanding; different people do grieve differently and children too, [is important]’. (FGD07-01-CR)
One faith leader highlighted the need to create networks in the public and community with the aim for the community to support the community: ‘I think for me, it is helping our own community to be a little bit more accepting of some of the difficulties and losses in life, that we also want to look at this as an opportunity to help one another, recognizing that it’s very personal, it’s very painful, but we need to help one another because we are family; because we are a community’. (FGD09-09-FL)
Subtheme 6: Providing multi-tiered services. Different people needing different levels of intervention and care were recognized by the participants. For example, help could be made available in the form of public education booklet or website. To one of the faith leaders, help could also be provided organically by non-professionals, faith leaders or even volunteers who are trained with some level of knowledge and skills: ‘… when we plan the funeral service, we know how dearly this person relates to the person that is passing away. We can identify whether this person needs any more help. Funeral directors can refer to the religious leaders to give them extra comfort and support. So, I think not only religious leaders, but funeral directors must also identify and see [if there is a need for bereavement support]’. (FGD09-07-FL)
Specialist services may be needed for bereaved families that are vulnerable, such as those who encounter complex situations surrounding the death event. This include surviving families who are bereaved by suicide, who experience multiple losses, who have pre-existing health issues, who were dependent on the deceased, or who caused the death unintentionally. One such opinion stated by a transplant coordinator was as follows: ‘Where the family member contributes to the death … for example, our motorcyclist and the pillion rider was the mother, you know, so … that gets very complicated, having to resolve that issue and then having to deal with [organ] donation on top of that’. (FGD08-01-TC)
Targeted services could also be required for bereaved individuals at different life stages, such as bereaved adult child caregivers who had been taking care of the elderly deceased for many years, bereaved young children who lack a voice for themselves, bereaved elderly who are socially isolated, bereaved parents whose only child died, and bereaved spouse with young children. One such view expressed by a social worker was as follows: ‘Some of them will actually tell us that “I don’t actually know how to handle a bank account.” “I don't actually know how to handle HDB [Housing Development Board] ownership.” “I don't actually know where his CPF [Central Provident Fund] statement is.” All these, the remaining spouse needs to take over the decision making and to run the family as per normal because they still have young children. The remaining spouse will take on all the stress’. (FGD08-07-SW)
Discussion
This is the first Singapore study to report on the bereavement care practices and service delivery, to understand how the needs of the bereaved persons are met and to examine gaps in the current provision landscape of grief and bereavement care. Thus, service providers from health and community sectors, as well as potential providers of bereavement support from the funeral industry, financial industry, faith groups, and non-professional volunteers were recruited as FGD participants. The management and delivery of bereavement support services present practical challenges, and these are well supported by our findings. The FGD participants also acknowledged that not all bereaved individuals require bereavement counselling. However, there was a general concern about the challenge to identify and refer those who may be at risk of complicated grief for timely and relevant help. Particularly, the funeral directors highlighted a lack of clarity of where to refer to, the social workers emphasized on a lack of collaborative practice among the service providers with the clients as the centerstage, and a lack of clarity and consistency in practice regarding follow-up procedures within their respective organizations.
The findings highlighted three key areas that are elaborated below and synthesized into a three-tiered model of bereavement support with the public health approach as the underlying conceptual framework. The three areas include the need to develop a national framework for bereavement care and support, increase grief literacy among the public and community for self-care and mutual support, and promote a culture of collaborative practice and partnerships so that bereavement care and support can be seamless across services (see Figure 1). Three-tiered public health model to grief and bereavement service provision. (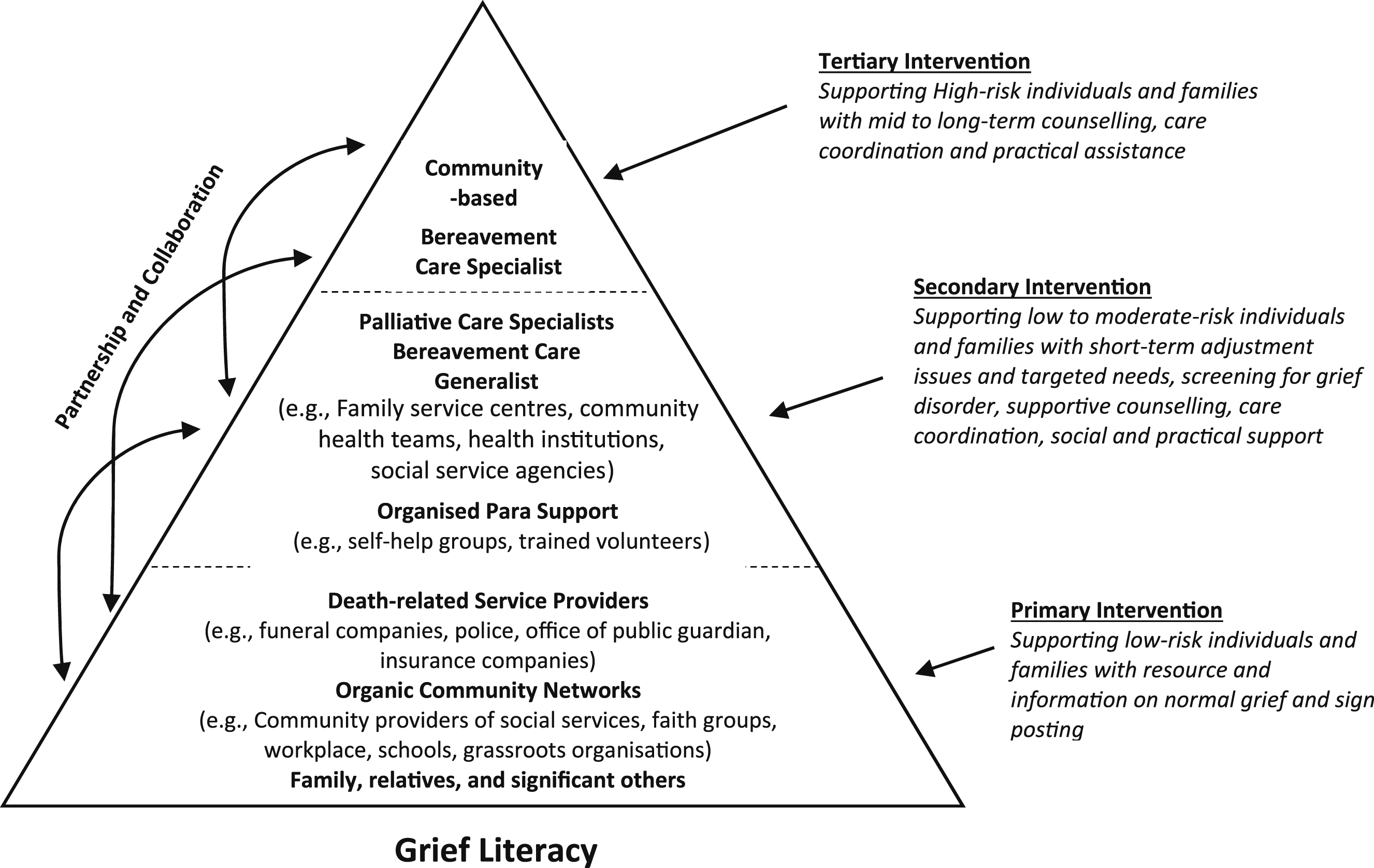
Developing a national framework for bereavement care using a public health approach
The proposed national framework takes reference to the multi-tiered public health model to bereavement support recommended in UK (NICE, 2004) and Australia (Aoun et al., 2012).
At the universal level, the bereaved-friendly practices could be the main service delivery environment. Bereavement-friendly practices refer to any service providers (e.g. health sector, community sector, death-related industry like funeral companies, police, and insurance companies), organic community networks (e.g. faith groups, workplace and grassroots organizations) or even public and community (e.g. families, relatives and neighbours) who adopt practices that support the bereaved individuals in the community, such as providing relevant information and resources, and linking up with services. The aim is to reduce the impact of the loss on the bereaved and enhance the overall well-being.
At the intermediate level, bereavement-informed practices may be the key, where organizations with professionals (e.g. palliative care specialists and bereavement care generalists) and organized para-support (e.g. self-help groups and trained volunteers) provide some aspects of targeted bereavement care. They are the professionals who received adequate training to support those requiring targeted, short-term bereavement support (e.g. adjustment issues and practical needs), screen for grief disorder, and provide supportive counselling. An onward referral for tertiary level of indicated care together with a proper triage assessment will be established, if needed.
Finally, at the tertiary level, a designated bereavement care program can be established with the primary aim to provide bereavement care for high-risk individuals and families, such as assessment and intervention for grief disorders, long-term grief counselling, as well as care coordination and practice support. They are the bereavement care specialists who are specially trained in, for example, grief therapy, trauma work and mental health to work with the bereaved individuals at the tertiary level.
Increasing grief literacy among the public, para-support and professional communities
The findings from this study confirm earlier studies that not all bereaved individuals and families require professional support. Rather, many of the bereaved persons can cope with the grief by utilizing their networks of social support and seeking self-help materials. Yet, advancing the community’s capacity to provide bereavement care remains underdeveloped (Rumbold & Aoun, 2014). Thus, community capacity building is required.
Corresponding to the level of care required, training pathways for community lay helpers, bereavement care generalists and bereavement care specialists can be established to ensure a match between needs and services availability. For example, professionals and lay people with high touch points could be equipped with skills to better identify and support the bereaved. The funeral directors are one such key player, who were found to have significant effect on the grief in their interactions with the family survivors (Rando, 1993). Other death-related service providers such as the police, insurance agents and religious ministries could also have their capability raised to look out for bereaved persons and link them up to services so that an improved bereavement outcome could be achieved.
Promoting a culture of collaborative practice and pro-active partnerships
As shown in the findings, the healthcare sector, such as the palliative care services emphasized care of the patients and the family caregivers during the pre-death phase and immediate post-death phase. Bereavement support tend to be followed up in the community. The findings also indicated that healthcare teams who screened and identified family caregivers who may have higher bereavement needs and introduced a bereavement care provider from the community before the death occurred saw better bereavement outcomes subsequently. This implies that before a death occurs, intervention for grief that accompanies cumulative losses and anticipatory losses can have positive impact on bereavement outcomes. As such, timeliness in developing referral pathways is crucial to building rapport and trust in the service’s ability to help at post-death phase. For example, the palliative care services may take the lead in pre-death work, while introducing their partners – community networks or the social networks of the family caregivers, bereavement care generalists or specialists in response to the needs of the family caregivers – early enough to ensure smooth transition of care. A through-care collaboration involving the palliative care team, social care agencies as well as community helpers across the pathways from pre-death to post-death care can ensure that services are wrapped around the clients so that they are well supported and not be lost to follow-up.
In addition to the importance of continuity of service, our findings also suggest the importance of continuity of relationship. That is, the importance of involving someone who was involved in the care of the deceased in the bereavement team or involving someone from the bereavement team in the care of the family caregivers before the death cannot be underestimated. This is similarly recommended in Aoun et al. (2017).
Limitations
This study was not conducted using a random sample of service providers relevant to the study. However, this sample consisted of a large sample representing a wide spectrum of service providers from different sectors and professions. We also recognized that those who declined or could not participate in the focus group discussions might have had different experiences. However, the findings compared favourably to studies undertaken internationally.
In addition, we acknowledged that potentially, there might be researcher biases since the transcripts were coded and analysed only by two researchers. However, efforts were made to discuss the findings with the research team, in different platforms with participants and other service providers, and with reference to international empirical studies.
Conclusion
Participation in the FGD offered a platform for service providers from different sectors to reflect critically on the current bereavement care practices. The findings have suggested a public health approach to bereavement care practice as a way forward to better meet the needs of bereaved individuals and families; as a foundation for determining the types of bereavement support services to be offered to bereaved individuals and families, subject to their needs and risk factors. From the public health perspective, bereavement services should be developed and provided for the whole population of bereaved people, giving priority to community capacity building so that bereaved people can be supported by their existing social networks, and the professional care supplements rather than replaces the social networks. To bring the public health model of bereavement care to the fullest benefits to the whole population of bereaved, there is also a need to complement our medical and psychosocial understanding with the cultural and spiritual strategies.
Footnotes
Acknowledgments
Authors would like to thank Alison Chew, the research assistant for assistance with the research project, Grace Yong for assistance in note taking the FGDs, and all the FGD facilitators. Authors would also like to thank all the FGD participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Temasek Foundation Cares.
Author’s Note
An earlier version of this work was presented as part of a report to Ministry of Health, Singapore and Temasek Foundation Cares.
The Bereavement Workgroup Members consisted of Ms Wai Yee CHEE (Singapore Hospice Council), Dr Ivan WOO (Tan Tock Seng Hospital), Dr Geok Ling LEE (National University of Singapore), Dr Mansha KHEMLANI (Khoo Teck Puat Hospital), Ms Kwai Theng LEONG (St Andrew’s Community Hospital), Ms Candice TAN (Tan Tock Seng Hospital), Dr Gilbert FAN (Nation Cancer Centre Singapore), Dr Carolyn NG (Children’s Cancer Foundation till July 15th, 2018), Ms Hwee Chin NG (Children’s Cancer Foundation), Ms Susan CHAN (Dover Park Hospice), Mrs Lay Beng LEE (Tan Tock Seng Hospital), Ms Grace ONG (Assisi Hospice till April 30th, 2018), Ms Cheng Wan PEH (Assisi Hospice), Ms Terina TAN (National University Hospital Systems), Mrs Yee Pin TAN (National Cancer Centre Singapore), Mr Andy SIM (Singapore General Hospital).