
Abstract
The Stigma of Suicide Scale (SOSS) is a measure of public attitudes toward suicide decedents, which makes it unique from other scales that measure more general attitudes toward suicide. The aim of this study was to further replicate and extend the reliability and factor structure of the SOSS (both long- and short form) in a sample of individuals directly impacted by suicide. This study also sought to identify factors that impact suicide attitudes unique to this sample. The sample included 312 participants who had personal experience with suicide. Results provided support for the oblique three-factor structure of the SOSS (stigma, isolation/depression, and glorification/normalization), with a superior model fit for the 16-item short form version. Correlates of suicide attitudes among individuals exposed to suicide included perceived relationship closeness to a suicide decedent, experience with both loss and attempt, and the sex of the suicide decedent.
Introduction
There remain many barriers to appropriate mental health and suicide prevention services for individuals affected by suicide (Batterham et al., 2013a; Tal-Young et al., 2012). One such barrier is social stigma. Stigma is defined as a label of social disgrace that is attributed to an individual (Arboleda-Flórez, 2002). Attitudes and stigma toward suicide can significantly impact behavior, whether it be the behavior of others toward individuals affected by suicide or the behavior of affected individuals. For individuals who struggle with suicidal ideation or who have been bereaved by a suicide loss, stigma can complicate feelings of social isolation and burdensomeness (Kodaka et al., 2011). Unfortunately, suicide stigma and its consequences on affected individuals have received less attention in suicide research compared to prevention and treatment topics. In addition, there are fewer studies examining measurements of attitudes toward suicide and their psychometric properties (Williams et al., 2018).
To understand social attitudes and stigma toward suicide, Batterham et al. (2013a, 2013b) developed the Stigma of Suicide Scale (SOSS), which is available in both a short- (16 items; SOSS-SF) and long form (58 items; SOSS-LF) version. The SOSS is the first questionnaire intended to measure social attitudes toward individuals who die by suicide from a community perspective. Using a principal component analysis (PCA) with orthogonal rotation, Batterham et al. (2013a) identified a three-factor structure of the SOSS: stigma, isolation/depression, and glorification/normalization. These factors represent stigmatizing views of suicide decedents, beliefs about suicide being associated with isolation and depression, and attitudes that reflect a normalized or glorified view of suicide. While these initial studies have added to the knowledge base about suicide attitudes in a novel way, they did not include diverse samples of individuals with varying experiences with suicide. The community sample from Batterham et al.’s (2013a) first study only included 10% who had personal exposure to suicide. While Batterham et al.’s (2013b) second study included a greater number of participants with a history of suicide ideation, there was no indication of whether participants had prior history of exposure to suicide loss. Furthermore, Batterham et al.’s (2013a, 2013b) use of a PCA with orthogonal rotation for factors that were correlated may have presented a limitation in data interpretation.
To gain a more well-rounded understanding of suicide attitudes, more research on attitudes from the perspective of those directly impacted by suicide (i.e., suicide loss and attempt survivors) is needed. To date, only a few known studies have investigated the psychometric properties of the SOSS, and even fewer have included participants with personal exposure to suicide. In three recent studies examining the psychometric properties of the 16-item SOSS-SF, the same three factor structure identified by Batterham et al. (2013a) was found (Aldalaykeh et al., 2020; Han et al., 2017; Williams et al., 2018). However, Han et al. (2017) found only 12 out of the 16 items to have significant factor loadings (excluded items were irresponsible, disconnected, pathetic, and cowardly). Regarding sample composition, Williams et al. (2018) had the highest percentage (35.4%) of participants with personal exposure to suicidality in another person, with 5.5% reporting a personal history of suicidality; while the other two studies had 11.3% and 7.1% of participants who had personal experience with suicide ideation (Aldalaykeh et al., 2020; Han et al., 2017 respectively). Two of these studies identified an association between personal exposure and suicide attitudes, such that personal experience with suicide ideation/attempt was associated with less stigma (Williams et al., 2018) and positively associated with greater glorification and normalization of suicide (Han et al., 2017).
Not only is it important to further validate the instruments used to measure public attitudes toward suicide, but it is also necessary to explore how suicide loss and attempt survivors perceive suicide for a more nuanced understanding on how personal experience can impact perceptions of suicide. Perspectives from those directly impacted by suicide can also inform our approach to changing negative or stigmatized attitudes that may act as a social barrier to help-seeking behavior.
The Present Study
This study sought to further explore the psychometric properties of the long- and short form versions of the Stigma of Suicide Scale (SOSS-LF and SOSS-SF, Batterham et al., 2013a) using a sample of suicide loss survivors and attempt survivors. Both versions of the SOSS were examined because this is the first study to use a sample exclusively consisting of suicide loss and attempt survivors. A secondary aim was to identify correlates of these attitudes. Special attention was paid to three domains of sample characteristics to examine their association with attitudes: (1) general demographic/background characteristics of the participants, (2) characteristics of suicide loss when applicable, and (3) characteristics of the participant’s suicide attempt when applicable.
Method
Procedure
A snowball sampling technique was employed to recruit suicide loss survivors and attempt survivors to complete an anonymous, online Qualtrics survey. Email listservs maintained by the American Association of Suicidology (AAS) were utilized to contact potential participants. Listserv members were sent an introductory email recruitment letter that directed them to the online survey site. Participants were also invited through word-of-mouth recruitment and online social media sites, such as Facebook and Twitter. Criteria for eligibility in the study included being at least 18 years old, ability to provide voluntary consent, and having experience with either a suicide attempt or loss in another person or personal ideation/attempt. No personal identifiers of the participants were collected. The study was approved by the appropriate institutional review board.
Measures
Stigma of Suicide Scale
The Stigma of Suicide Scale (SOSS; Batterham et al., 2013a) was developed to measure public attitudes towards a “prototypical” person who dies by suicide. The full-length version of the SOSS includes 58-items comprised of one- or two-word descriptors of a “typical” suicide decedent. The short form of the SOSS include 16-items from the full-length version. Examples of these descriptor words are stupid, isolated, brave, and irrational. Batterham et al.’s (2013a) original study revealed a three-factor structure with strong internal consistency overall (α = .90) and for each subscale: stigma (α = .95), isolation/depression (α = .88), and glorification/normalization (α = .86), with 31, 16, and 11 items respectively. Each item is rated independently using a 5-point Likert scale ranging from 1, strongly agree, to 5, strongly disagree, and scores are totaled for each subscale with higher scores reflecting greater endorsement of the isolation/depression and glorification/normalization factor, and higher scores reflecting less endorsement of the stigma factor. The SOSS has produced robust psychometric properties in previous studies (Aldalaykeh et al., 2020; Batterham et al., 2013a, 2013b; Han et al., 2017; Williams et al., 2018).
Demographic Variables
Demographic or background variables included in the analysis as independent variables were (1) participant age, (2) sex, (3) education level, (4) race, (5) country of residence, and (6) suicide exposure group identification (loss survivor, attempt survivor, both loss and attempt survivor). Participant age (in years) was measured continuously. Participant’s race (White vs. non-White) and country of residence (U.S. vs. non-U.S.) were measured dichotomously. The data for participant’s race originally captured a greater variety of categories (e.g., Asian-American, Native American, Latino/Hispanic), however, the variable was recoded to collapse race categories into White versus non-White due to having too few participants in the non-White categories. This presented the problem of having limited ability to perform meaningful data analysis to compare all race categories. Response options for participant’s education level included 0 = high school or less, 1 = some college, 2 = Associates/Bachelor’s degree, and 3 = graduate/professional degree.
Characteristics of Suicide Loss
Apart from the variable measuring the number of suicide deaths, participants who had experienced more than one suicide loss were asked to answer the remaining loss-specific questions in reference to the loss which was most significant to him/her. Suicide loss variables included in the analysis as independent variables were the (1) number of suicide deaths, (2) sex of the suicide decedent, (3) participant’s age at the time of loss, (4) number of years since loss, (5) relationship to suicide decedent, (6) perceived relationship closeness, and (7) perceived emotional impact. Participant’s age at the time of loss and number of years since loss were measured continuously in years. The number of suicide deaths was measured categorically (1 = one death, 2 = two deaths, and 3 = three or more deaths) because the variable was heavily skewed as evident in the preliminary screening of the data. Relationship to suicide decedent categories included immediate family member, extended family member, and other. Participants were asked to respond to statements about perceived relationship closeness and perceived emotional impact of loss using a 5-point Likert scale ranging from 1, “not close/little effect on my life,” to 5, “very close/significant effect on my life that I still feel.” For the purposes of this study, perceived relationship closeness and perceived emotional impact of loss responses were collapsed from five categories to three (1 = not close, 2 = somewhat close, and 3 = very close) due to data distribution problems identified in the preliminary screenings.
Characteristics of Participant’s Suicide Attempt
Characteristics of participant’s suicide attempt included the (1) number of previous suicide attempts and (2) age at the time of most recent attempt. The number of previous suicide attempts was measured categorically (1 = once, 2 = twice, and 3 = three or more attempts) due to the variable being highly skewed. Participant age at the time of most recent attempt was measured continuously in years.
Data Analysis
Given the study aim of examining the psychometric properties of the SOSS with a different sample (those who have survived suicide and/or experienced suicide loss) a confirmatory factor analysis (CFA) of the long form of the SOSS was first conducted to confirm the factor structure of Batterham et al. (2013a). For this study, all CFA were performed using R version 4.0.3 and the lavaan R package. Items were examined for R2 values above .30 and factor loadings above .40, and as items were removed significant chi-square changes were monitored along with model fit indices (Kline, 2016).
Following initial CFA and the resulting poor model fit indices, exploratory factor analysis (EFA) was conducted again to confirm the three-factor structure identified by Batterham et al. (2013a). The SOSS was expected to reflect three latent factors – stigma, isolation/depression, and glorification/normalization (Batterham et al., 2013a, 2013b). An EFA using principal axis factoring was conducted on the 58 items of the SOSS, using SPSS version 27 (SPSS Inc., Chicago, IL), with a Direct Oblimin rotation for potentially correlated factors. In order for an item to be considered meaningful, the factor loading had to be above a threshold level of 0.35 on the factor on which it loaded strongest (i.e., loading on other factors could not exceed 0.30), as recommended for a sample size of 250 (Hair et al., 1998). The number of factors to be retained was determined by examining Kaiser’s criterion (eigenvalues ≥1), scree plot, and interpretability of factors.
Following results of the EFA the items were further examined using confirmatory factor analysis (CFA) including examination of R2 (variance explained) values for each item and model fit indices. A CFA was also conducted with the 16-item short form of the SOSS.
Preceding further analyses, data were screened for univariate normality by examining values for skewness and kurtosis. To identify correlates of suicide attitudes, a series of one-way analyses of variance (ANOVA) tests, correlations, and independent sample t-tests were conducted between the aforenoted independent variables (e.g., age, education level, suicide exposure group) and each emergent SOSS-SF factor. All ANOVA tests were followed by either Tukey HSD and Bonferroni, or Games-Howell post-hoc comparisons, dependent on the outcome of Levene’s statistics tests of homogeneity of variance (Field, 2017). Following results of the bivariate analysis simultaneous multiple regression analysis were conducted to predict scores on each of the SOSS-SF subscales.
Results
Participants
A total of 312 participants completed the online survey, of which 79 (25.3%) identified as suicide loss survivors, 87 (27.9%) identified as attempt survivors, and 146 (46.8%) identified as having experienced both a loss and an attempt. The sample was predominately female (n = 271, 88%) and participant age ranged from 18–83 years of age, (M = 44.16, SD = 13.92). Regarding education level, 121 (38.8%) reported having less than a college degree. Eighty-one percent of the sample resided in the United States and represented 41 states.
Missing Data Analysis
Prior to EFA and CFA, the SOSS and PHQ-9 were examined for missing data patterns. The long form of the SOSS had missing data on items spread across 17% of cases with most missing only one or two items. Results from Little’s MCAR test were significant (χ2 = 2758.50, df = 2,575, p = .006). We therefore could not assume that data is missing completely at random and should assumed potential bias. Multiple imputation was done with the SOSS data, and the iterations chosen were an optimal match with the distribution of the original data. The PHQ-9 had missing data on items spread across 13% of cases and a non-significant Little’s MCAR test (χ2 = 25.60, df = 29, p = .65). However, 35 cases had missing data on all nine items of the PHQ9 and therefore could not be imputed.
Exploratory and Confirmatory Factor Analysis of SOSS Short and Long Form
Initial model fit was very poor for the CFA conducted on the long form of the SOSS with the 58 items and three-factor structure proposed by Batterham et al. (2013a) (χ2 = 3475.76, df = 1,592, CFI = .763, TLI = .753, RMSEA = .064, SRMR = .079). Given the results of the CFA, an EFA was conducted to explore the factor structure with this study’s sample. Initial examination of eigenvalues and the scree plot for the 58 items of the SOSS long form suggested the presence of four factors. Values of Bartlett’s test and the Kaiser-Meyer-Oklin (KMO) value indicated that the data were appropriate for factor analysis. The initial four factor EFA confirmed the presence of correlated factors and explained only 43.5% of the variance. Individual items were examined for low communalities values, factor loadings below .35 and significant cross loadings between factors. An iterative process of removing six poorly performing items resulted in the fourth factor consisting of substantially cross loaded items. Forcing the EFA to three factors resulted in a simpler and more conceptually intuitive factor structure explaining approximately 41% of the variance, with factors consistent with Batterham et al. (2013a), and corresponding to the labels stigma, isolation/depression and glorification/normalization.
Given confirmation of the three-factor structure, the analysis proceeded to a CFA with the 52 remaining items. The initial model fit for the three factor 52 item measurement model was very poor (χ2 = 2798.90, df = 1,271, CFI = .798, TLI = .780, RMSEA = .062, SRMR = .075). Several items were removed through an iterative process of examining item factor loadings, R2 values of items and significant changes in Chi-Square upon re-running the model. Final adequate model fit was achieved with 28 items remaining (χ2 = 694.4, df = 347, CFI = .909, TLI = .901, RMSEA = .057, SRMR = .053). The latent factors of isolation/depression and stigma were significantly correlated (r = .28, p < .001). Reliability was satisfactory for the resulting stigma (α = .91), isolation/depression (α = .92) and glorification/normalization scales (α = .82).
Summary of Confirmatory Factor Analysis Results for the SOSS-SF Subscales.
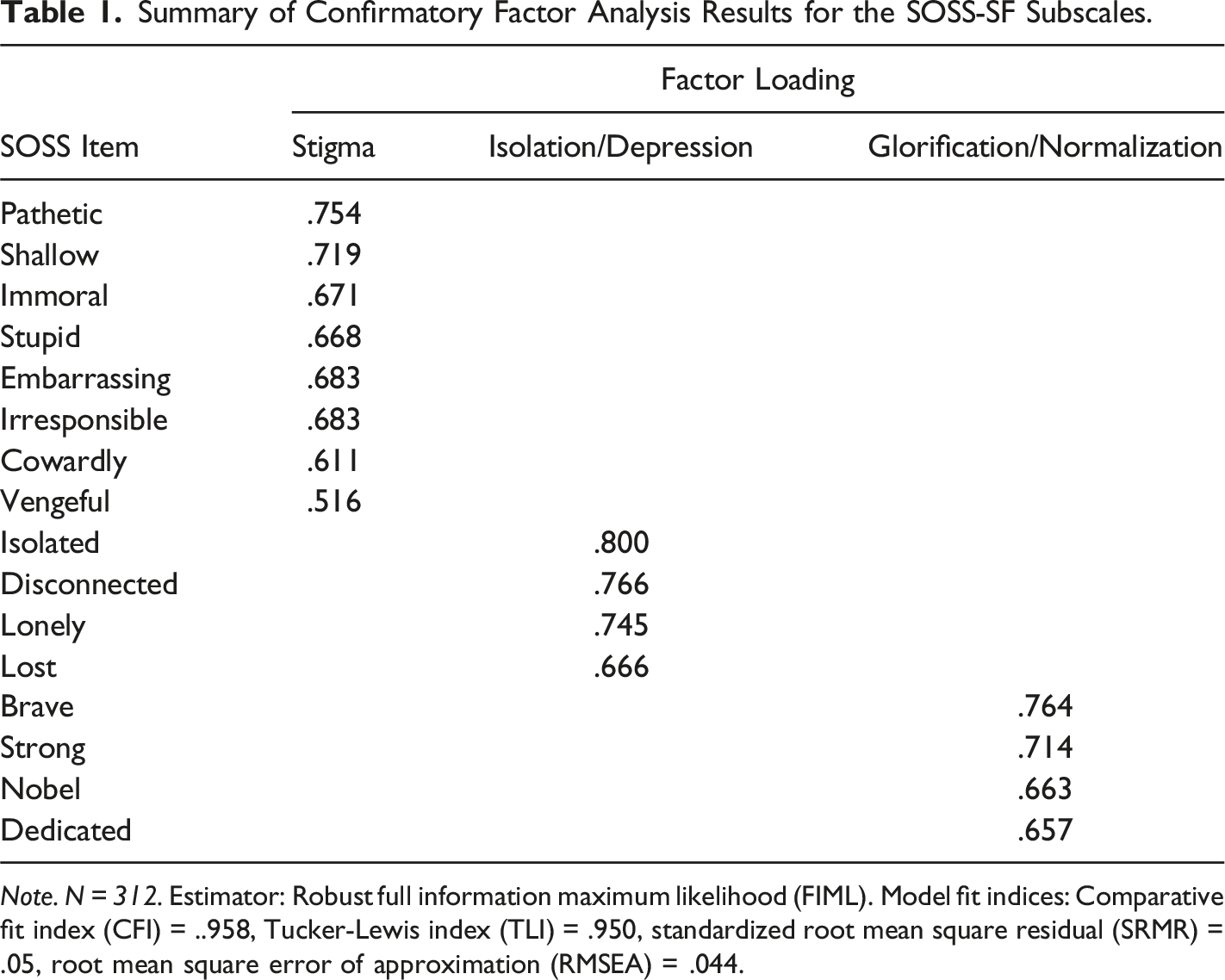
Note. N = 312. Estimator: Robust full information maximum likelihood (FIML). Model fit indices: Comparative fit index (CFI) = ..958, Tucker-Lewis index (TLI) = .950, standardized root mean square residual (SRMR) = .05, root mean square error of approximation (RMSEA) = .044.
Sample Characteristics as Predictors of Attitudes for SOSS-SF Subscales
Bivariate Relationships With the SOSS-SF Subscales.
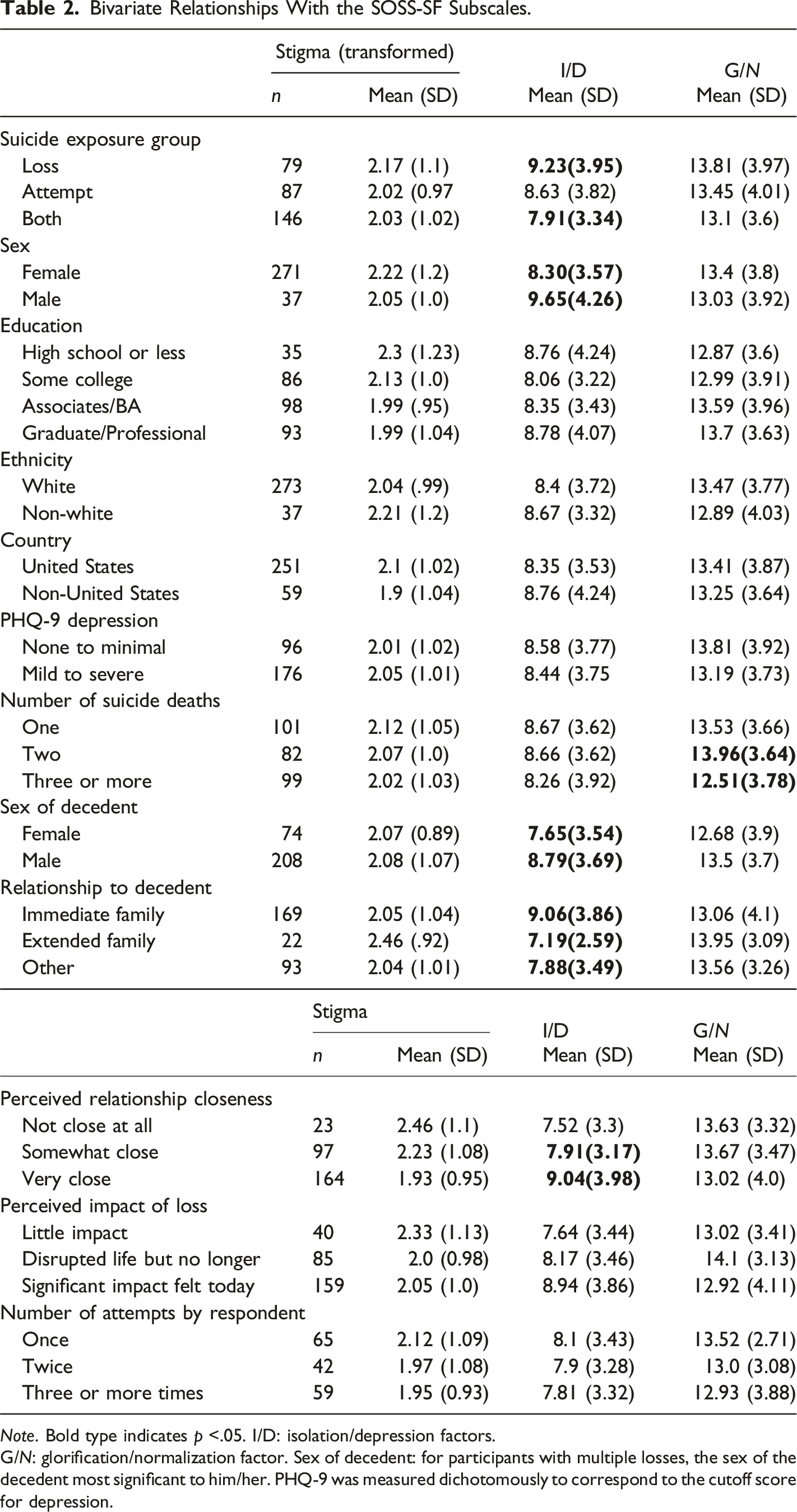
Note. Bold type indicates p <.05. I/D: isolation/depression factors.
G/N: glorification/normalization factor. Sex of decedent: for participants with multiple losses, the sex of the decedent most significant to him/her. PHQ-9 was measured dichotomously to correspond to the cutoff score for depression.
Covariates of SOSS Short Form Scales.
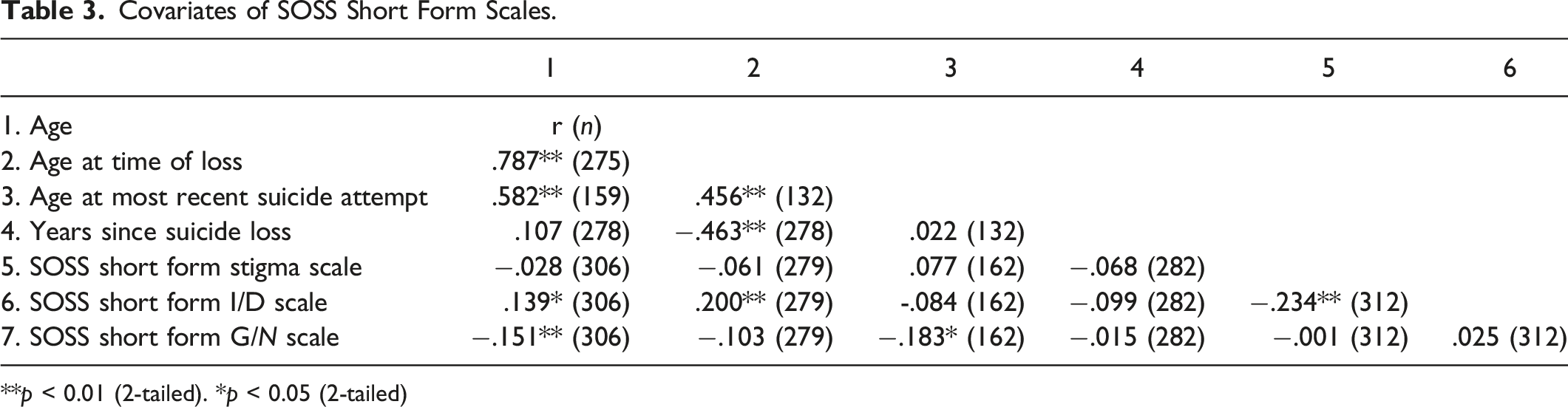
**p < 0.01 (2-tailed). *p < 0.05 (2-tailed)
In the present sample, females were significantly more likely to view suicide as resulting from isolation or depression (M = 8.3, SD = 3.57) than males (M = 9.65, SD = 4.26), t (296) = −2.34, p = .02. Participant age was significantly correlated with scores on the isolation/depression factor (r = .14, p < .05), such that younger participants were associated with more agreement that suicide is attributed to isolation/depression. Participant age was also significantly inversely correlated with scores on the glorification/normalized factor (r = −.15, p < .01), with greater agreement with glorification/normalization associated with older participants.
Regarding suicide exposure groups, there were statistically significant differences between loss survivors and both loss and attempt survivors on perceptions of suicide being attributed to isolation or depression, F (2, 309) = 3.51, p =.031. Suicide loss survivors (M = 9.23, SD = 3.95) were less likely to attribute suicide to isolation or depression as compared to participants who reported having experienced both a loss and an attempt (M = 7.91, SD = 3.34) (p = .04, Games Howell Post Hoc Test for violation of homogeneity of variance assumption). There were no statistically significant differences among suicide exposure groups on stigmatized and glorification/normalization suicide attitudes (p = .59 and p = .40 respectively).
The only characteristic of suicide attempt as a significant predictor for suicide attitudes was participant’s age at the time of attempt. For participants who had a history of suicide attempt(s), their age at the time of attempt was inversely significantly correlated with the glorification/normalization scale scores (r = −.18, p < .05). The older the participant at the time of their suicide attempt the more likely they were to agree with the glorification/normalization of suicide scale items.
Characteristics of Loss as Predictors of Attitudes for SOSS-SF Subscales
Significant differences were observed for suicide loss survivors who had different experiences with loss. Participant age at the time of suicide loss was significantly correlated with isolation/depression scores (r = .2, p < .01), with younger age at the time of loss being associated with greater agreement. A significant one-way ANOVA was found for a subset of the sample that experienced a suicide loss (F (2,279) = 3.65, p = .03). Participants who experienced three or more suicide losses (M = 12.51, SD = 3.78) had more agreement (significantly lower scores) on the glorification/normalization scale than those that experienced two losses (M = 13.96, SD = 3.64), although neither was significantly different for those who experienced only one death (M = 13.53, SD = 3.66) (Tukey HSD and Bonferroni post hoc tests).
Scores on the isolation/depression factor were significantly higher (indicating less agreement) when the suicide decedent was male (M = 8.79, SD = 3.69) as compared to when the suicide decedent was female (M = 7.65, SD = 3.54), t (280) = 2.32, p = .021. In other words, participants who experienced a suicide loss of a female attributed isolation or depression more strongly. There were statistically significant differences between suicide decedent relationship categories (i.e., immediate family, extended family, and other) on the isolation/depression factor, F (2, 281) = 4.71, p = .01. Suicide loss survivors who had experienced a death of an immediate family member (M = 9.06, SD = 3.86) were less likely to attribute suicide to isolation or depression as compared to participants who had lost an extended family member (M = 7.19, SD = 2.59) or other person (M = 7.88, SD = 3.49) (Games-Howell post hoc tests for violation of homogeneity of variance). There were no statistically significant differences among decedent relationship groups on stigmatized and glorification/normalization suicide attitudes (p = .19 and p = .41 respectively).
There was a significant effect of perceived relationship closeness on the isolation/depression attitudes scores, F (2, 134.69) = 5.45, p = .01. The Games-Howell post hoc tests (for violation of homogeneity of variance) revealed less agreement (significantly greater scores) on isolation/depression attitudes for participants who indicated having had a “very close” relationship (M = 9.04, SD = 3.98), than participants who indicated “somewhat close” (M = 7.91, SD = 3.17) but neither was significantly different from “not close at all” (M = 7.52, SD = 3.3).
The initial one-way ANOVA results were statistically significant for the stigma subscale scores but post hoc tests (Tukey HSD and Bonferroni) indicated differences between the means of the scores of participants who endorsed “very close,” “somewhat close,” or “not close at all,” be approaching but not achieving statistical significance (p = .057 for “somewhat close” and “very close”, p = .051 for “very close” and “not close at all”). There were no statistically significant differences among perceived closeness groups on the glorification/normalization suicide attitudes (p = .36).
Multiple Regressions Examining Combined Predictors of SOSS-SF Subscales
Upon examination of significant bivariate relationships, the following predictors related to suicide loss characteristics were added to multiple regressions with the stigma, isolation/depression and glorification/normalization scales as dependent variables: Participant age and sex, decedent sex, suicide exposure group, relationship to decedent, and perceived closeness to decedent. Regressions were examined for independence of errors, normality assumptions and multicollinearity. The participant’s age at time of loss could not be included in the analysis due to multicollinearity with the age variable, and number of suicide deaths could not be included due to perfect prediction between dummy variables. Separate multiple regression analyses were not performed for variables related to characteristics of the participant’s suicide attempt because only one predictor (i.e., age at time of attempt) was significant at the bivariate level.
Multiple Linear Regression: Examining Predictors of the SOSS Stigma Scale.
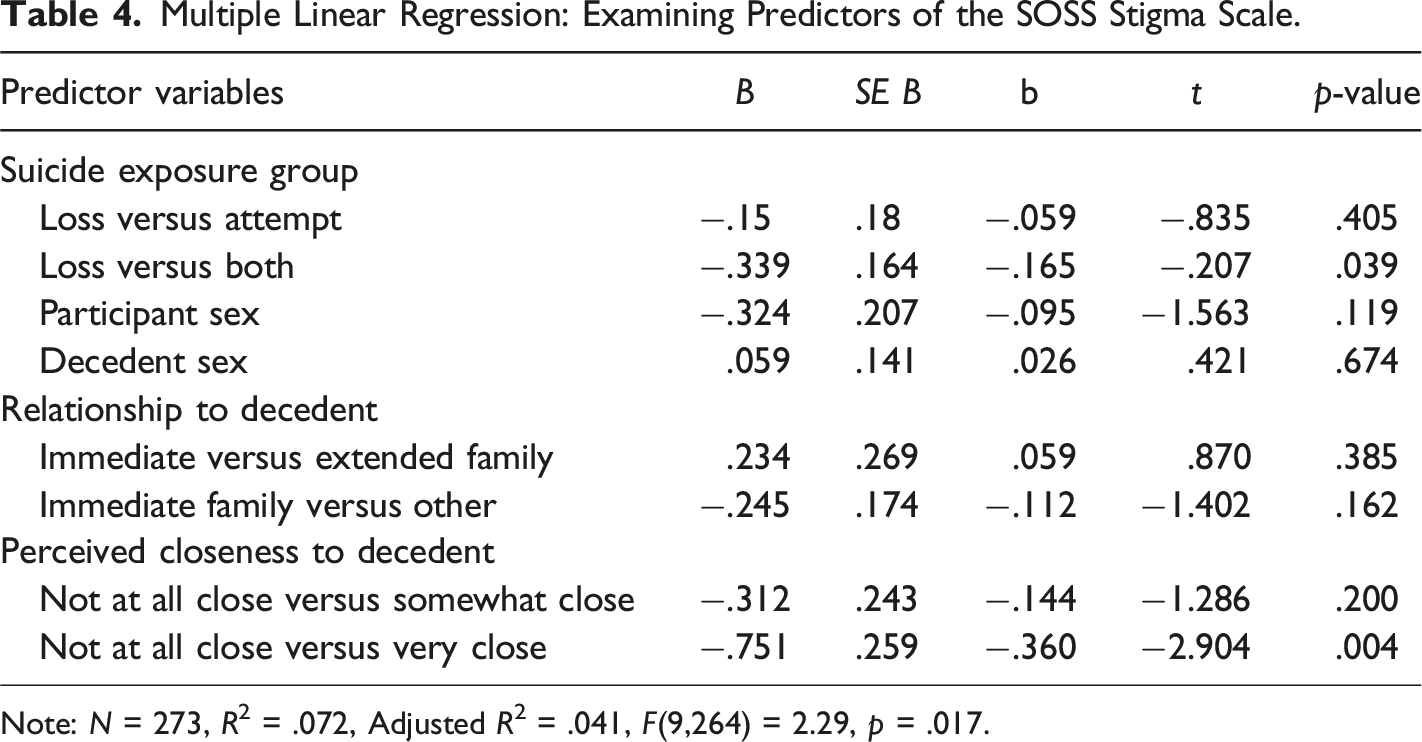
Note: N = 273, R2 = .072, Adjusted R2 = .041, F(9,264) = 2.29, p = .017.
Multiple Linear Regression: Examining Predictors of the SOSS Isolation/Depression Scale.
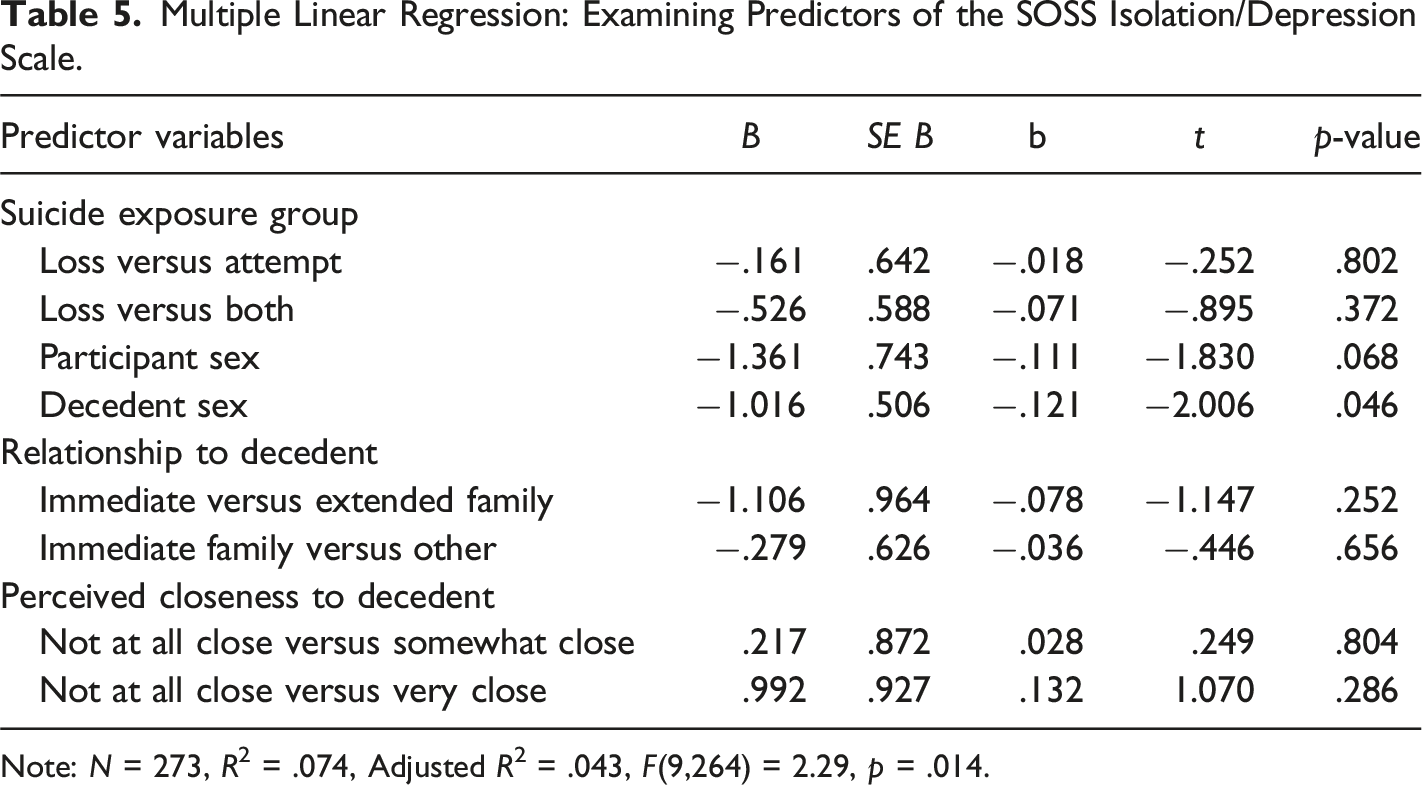
Note: N = 273, R2 = .074, Adjusted R2 = .043, F(9,264) = 2.29, p = .014.
Discussion
The present study is the first to use a sample composed exclusively of suicide loss and attempt survivors to examine the factor structure of both forms of the SOSS (i.e., 58-item and 16-item) and report their outcomes. Our results indicated support for the oblique three-factor solution of the SOSS-SF and SOSS-LF for this sample. That is, our results suggest that individuals who have had exposure to suicide (i.e., loss and attempt) tended to interpret the SOSS items similar to community-based participants from previous research (Batterham, et al., 2013a, 2013b).
SOSS-LF Items Retained and Excluded.
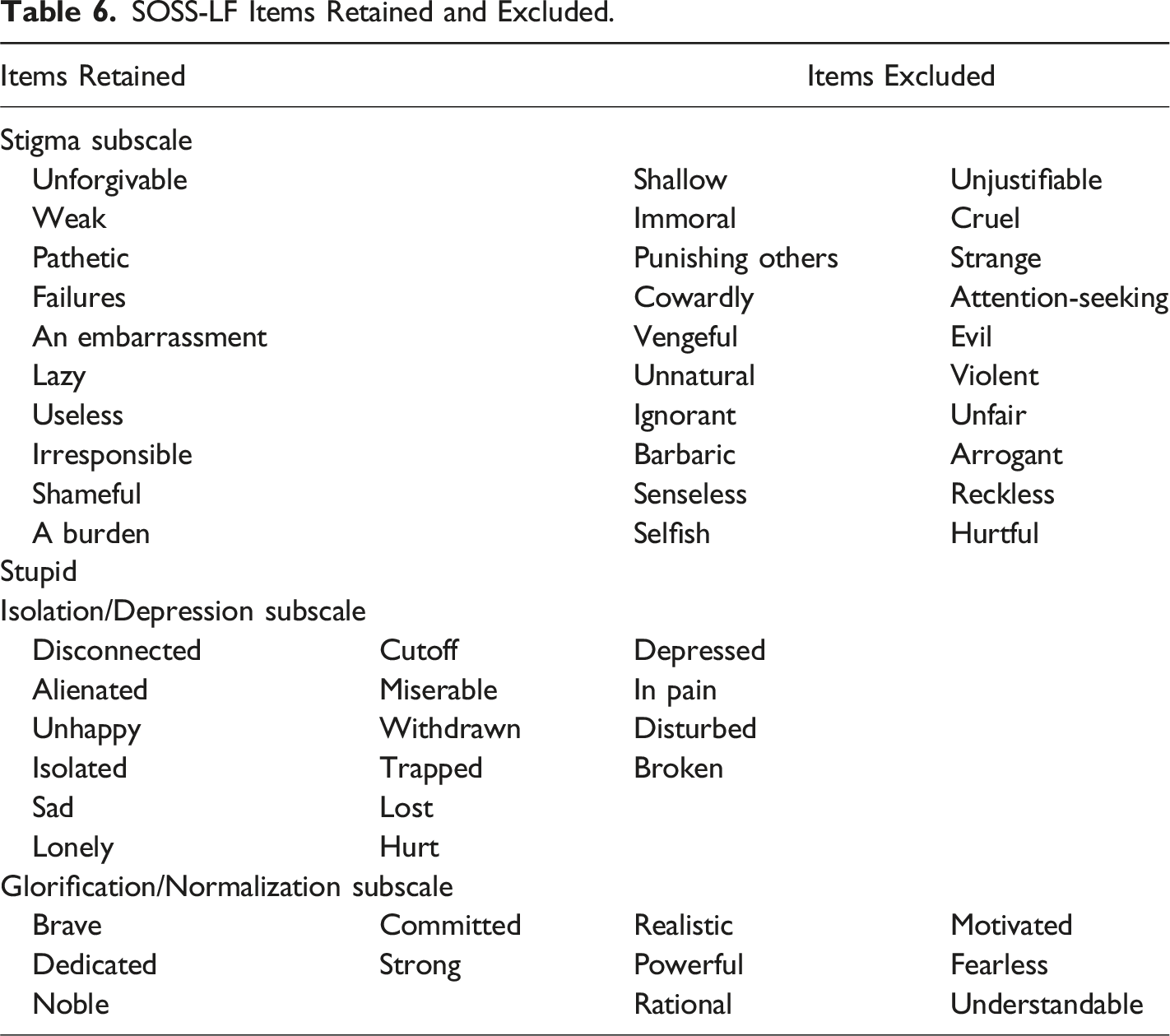
More recent studies using the SOSS have elected to use the short form version (Aldalaykeh et al., 2020; Han et al., 2017; Murphy et al., 2019; Williams et al., 2018), which may be due to the convenience of using a more time-efficient measure and/or the more robust psychometric properties as compared to the long form. However, Han et al.’s (2017) study examining the psychometric properties of the SOSS-SF (translated to for Chinese participants) still found that four of the 16-items (irresponsible, disconnected, pathetic, and cowardly) did not meet the factor loading criteria. The authors suggest that this may be due to different Chinese social norms that emphasize interpersonal relationships, as opposed to specific character traits. Therefore, it appears that how individuals interpret the SOSS items is at least partially dependent on the cultural norms and values of the population being tested. This not only applies to differences based on varied ethnic cultures but also to subcultures revolving around “survivorship” and suicide. Experiencing a suicide attempt or loss, much like other traumatic experiences, has the potential change someone’s worldview, beliefs about acceptable norms, and values. Due to these cultural and subcultural differences, it is necessary for future studies using the SOSS-SF to continue exploring its psychometric properties to ensure that nuances are identified for different types of populations.
This study also explored the associations between the SOSS-SF factors and sample characteristics to identify correlates of suicide attitudes. Notable findings include females being less likely than males and older participants more likely than younger ones to view suicide as resulting from isolation or depression. Suicide loss survivors were less likely to attribute suicide to isolation or depression as compared to participants who reported having experienced both a loss and an attempt. Older age of responders was also related to greater agreement with glorification/normalization. For attempt survivors, the older age at the time of participant’s attempt (most recent if more than one attempt) was associated with stronger glorification/normalization views.
Suicide attempt survivors who had also experienced a suicide loss were more likely than suicide loss survivors without an attempt history to have hold less stigmatized attitudes toward suicide. This was also true for loss survivors with a closer relationship to the decedent. This finding suggests that loss survivors without their own lived experience and/or without having lost someone close still hold and might perpetuate stigmatized views about suicide. It might be concluded then that naturally reducing stigma about suicide occurs when an individual has made an attempt themselves and/or when they lost someone close to them. We can only speculate possible rationale for this phenomenon. For example, having made a suicide attempt, an individual gains a more comprehensive insight into the factors that contributed to making the attempt. Similarly, an individual who lost someone they were close to, might better understand the nuances of the decedent’s life and hold less stigmatized views about their suicide death. Clearly, more research is warranted to determine the mechanisms of change in suicide stigma. This finding also has implications for intervention strategies targeting suicide stigma. Given that stigma about suicide still precludes individuals (i.e., both suicide loss survivors and attempters) from seeking and accessing psychiatric help, it is important to implement strategies, such as psychoeducation, to reduce these negative attitudes. In the light of this finding, extra attention should be paid to those who lost someone to suicide they weren’t close to (e.g., acquaintances) and address any unhelpful views around suicide that might be held by the loss survivor in order to alleviate some of the negative consequences for other affected individuals.
Strengthens, Limitations, and Future Directions
This study has some notable strengths and weaknesses. First, it is the first to explore psychometric properties of both the long- and short-form Stigma of Suicide Scale (SOSS) in a sample of suicide loss and attempt survivors and people who have both experiences. Results indicated that short form of the SOSS has acceptable psychometric properties for future research. When selecting which form of the SOSS is most advantageous, researchers should consider two points: (1) the target population for the study and (2) the overall aim of the study. Studies that target specific populations not yet included in previous studies using the SOSS would do well to administer the long-form version and perform a factor analysis because, as was true in this study, certain nuances would be captured regarding which items (i.e., character descriptions) are perceived as applicable for that particular population. However, for studies that are not focused on groups that have not been previously studies, the SOSS short-form is recommended. This recommendation is based on the fact that the short-form has acceptable psychometric properties and is less time intensive to complete. Without more research using the SOSS long-form to demonstrate unacceptable psychometric properties, it would be premature to discount the utility of the long-form entirely.
Given that exposure to suicide has been shown to be a risk factor for depression and suicidal ideation (Cerel et al., 2016), it is important to understand how attitudes in people with different types of lived experience or a combination of the two might relate to their development of symptoms. This study adds to our understanding of factors that impact attitudes and how these attitudes different between suicide exposure groups. Additional research is needed to determine how suicide attitudes are related to risk in these populations. It might be that changing attitudes about suicide can lead to better outcomes for people with lived experience.
However, this study is limited in that it utilized a self-selected convenience sample which might not be representative of all loss and attempt survivors. The sample size was relatively small and limited the ability to perform a wide range of comparisons. Furthermore, the sample was predominately White and female, which limited the ability to compare a greater variety of groups. Previous findings indicate that females more frequently attempt suicide but have less fatal attempts as compared to men (Drapeau & McIntosh, 2021). Additionally, research also shows that females engage in research more often than males (Covell et al., 2003; Hill et al., 1979). These factors could account for the fact that there are a greater number of female loss survivors.
Future research is needed to address the shortcomings of the sampling procedures. Recommendations for sampling techniques to improve sample size include, but not limited to, partnering with funeral homes to identify suicide loss survivors, utilizing emergency department records to identify suicide attempt survivors, and using survey platforms that have large, pre-existing databases of audiences (e.g., Survey Monkey, Qualtrics). These survey platforms have features that allow researchers to reach a global and national audience; thus, providing an increased chance of recruiting participants that meet the eligibility criteria. To obtain a more representative sample, stratified random sampling methods to recruit participants with suicide loss or attempt as the pre-determined characteristic. Potential participants identified through funeral homes, emergency departments, and survey platforms should be randomly selected and recruited for participation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.