
Abstract
The current study was conducted to adapt the Grief and Meaning Reconstruction Inventory (GMRI) into Spanish and to establish its psychometric properties in a group of 202 mourners seeking treatment in Spain. A confirmatory factor analysis established that the Spanish GMRI yielded eight factors, displaying strong reliability and convergent validity, through the scale’s inverse correlation with the Inventory of Complicated Grief and various measures of psychological distress, explaining a 48% of the variance of the former measure. A network analysis suggested that sense-making could play a central role in meaning-making during bereavement.
The loss of a loved one represents a rupture of the relational bond with the deceased, which can produce emotional suffering, loss of purpose, and feelings of meaninglessness about self and life for survivors (Rando, 1986; Riches & Dawson, 2000). During the grief process, a progressive modification of the beliefs and values used to organize the experience and the symbolic bonds occurs, resulting in the gradual revision of the relationship of the deceased and the emergence of new meanings in life (Neimeyer, 2019).
In other cases, however, the grief process is characterized by intense psychological distress and sustained symptoms over several months or years. This phenomenon has been conceptualized as complicated grief (CG; Shear et al., 2014) or prolonged grief disorder (American Psychiatric Association, 2013, World Health Organization, 2018). Therefore it is important to differentiate between an adaptive grief versus one that needs specialized care (Prigerson et al., 2021). Finding a meaning in loss and in life differentiates adaptative and maladaptive grief, and is a process that can be assessed by the Grief and Meaning Reconstruction Inventory or GMRI (Gillies et al., 2015). The goal of the present study was to adapt the GMRI in a Spanish language context and to conduct a network analysis (NA) of its constituent elements in order to contribute to both the practical armamentarium of clinicians and researchers in Spanish-speaking countries and communities, and to advance theory regarding the meaning-making process in the wake of loss.
The Meaning Reconstruction Approach
A constructivist conceptualization of grief (Neimeyer, 2000; 2019) offers a meaning-oriented perspective, considering grief as an intimate process that nonetheless occurs in an intricate social context (Neimeyer et al., 2014). Loss may invalidate the core constructions of the bereaved about self and reality, as they face a series of idiosyncratic challenges to reconstruct their identity and reestablish a sense of continuity in their lives. A large body of research supports the role of meaning-making in predicting and even mediating the impact of various risk factors for poor bereavement outcomes, including complicated or prolonged grief symptomatology (Currier et al., 2012; Milman et al., 2019; Neimeyer, 2019).
Meaning oriented theorists and researchers (Gillies et al., 2014; MacKinnon et al., 2013; Neimeyer, 2011, 2012; Park, 2010) have posited the influence of sense-making, identity re-construction and reaffirmation of a security-enhancing continuing bond with the deceased as predictors of adaptive grief and wellbeing following loss. To assess these constructs, Gillies et al. (2015) developed the Grief and Meaning Reconstruction Inventory (GMRI), a 29-item self-report measure encompassing various expressions of meaning making in loss. Gillies and Neimeyer (2006) identified three activities of meaning reconstruction involved in the grieving process: sense making (striving to comprehend what happened), benefit finding (embracing valued life lessons or positive reappraisals of the experience), and identity change (revising or developing a clearer and valued sense of self and social relationships). In a mixed methods study of these processes in a diverse sample of 332 bereaved adults, Gillies et al. (2014) conducted a thematic analysis of participant narratives and then formulated numerous items to comprise a multi-factorial scale of meaning making in loss. The final scale, dubbed the GMRI and its factors showed good internal consistency and strong convergent validity with measures of grief-related personal growth; and strong negative correlations with measures of complicated grief, bereavement-related negative emotions, psychological distress and mental health symptoms.
One goal of the current study was to adapt the GMRI to Spanish and examine its psychometric properties. The GMRI could serve as a useful tool for screening whether the bereaved are following a maladaptive grief process, an adaptive integration of the loss, or even one leading toward posttraumatic growth (PTG) through adversity (Tedeschi & Calhoun, 1996). Furthermore, the factors measured by the GMRI could suggest specific treatment and prevention programs to support the bereaved. The validation of a Spanish version of the GMRI could allow clinicians to address practical needs that emerge in the therapeutic context with Spanish-speaking mourners.
As a second goal of the study, inspired by the work of Bellet et al. (2018), we sought to determine whether the factors of the Spanish GMRI could alternatively be conceptualized as a set of interacting features of meaning-making through the adoption of NA (Epskamp et al., 2018). Development of a network model of the GMRI could contribute to meaning reconstruction theory by suggesting which aspects of meaning making assessed by the instrument are likely to play a pivotal role in activating changes in the network of elements representing constituent features of meaning reconstruction, as assessed by the measure.
Methods
Translation Protocol
Following best practices in professional translation of psychometric scales (International Test Commission, 2017), translation of the original English version of the GMRI (Gillies et al., 2015) was carried out independently by two healthcare professionals specialized in grief, both native Spanish speakers with a high level of English language proficiency. Minor discrepancies between the two versions were resolved by consensus to obtain a synthesized version. This synthesized version was back-translated to English by a native English speaker, a healthcare professional familiar with grief theories. The back-translated version was compared with the original, and the discrepancies were, again, analyzed and resolved by consensus.
Participants
The sample was recruited from [the Hospital Infantil Universitario “Niño Jesús”, Hospital General Universitario Gregorio Marañón, Hospital La Paz, Madrid; Fundació Hospital de Sant Jaume i Santa Magdalena, Hospital de Calella, Catalunya; and the Hospital Universitario Miguel Servet, Aragon, Spain.]. The participants were patients of the grief therapy programs of the services of oncology, palliative care and/or health psychology. The inclusion criteria were: to be experiencing a grief process due to the death of a close relationship, the death having occurred a month before or more. The exclusion criteria were: being in a grief process for 3 years or more, and having had a legal problem with the healthcare team.
Procedures
The research project was approved by the ethical committee of [the Hospital Infantil Universitario Niño Jesús of Madrid, Spain (R-0021/16)]. To collect socio-demographic data and previous history of losses and grief an ad hoc questionnaire was designed.
The potential participants were contacted telephonically or in person. First, the project, its research objectives and its relevance to the field were explained. Those interested in participating received an information sheet about the project and signed informed consent and a confidentiality agreement. The administration of the questionnaires was carried out through in-person or telephonic interviews, email, or postal mail.
Instruments
Grief and Meaning Reconstruction Inventory (Gillies et al., 2015)
The GMRI is a 29-item self-report questionnaire that assesses meaning reconstruction after the loss of a beloved one. The items are answered on a Likert scale ranging from 1 (“totally disagree”) to 5 (“totally agree”). In the originally validated measure, the items are grouped into five factors: Valuing Life, Emptiness and Meaninglessness, Personal Growth, Sense of Peace and Continuing Bonds. The score for each factor is computed by summing up its items’ ratings, with those on the Emptiness and Meaninglessness factor being reverse scored. The GMRI has good psychometric properties including convergent validity, factorial validity and reliability (Cronbach’s alpha internal consistency α = .86; ranging from .85 to .76 for the subscales). The higher the scores, the higher the level of adaptive grief and meaning reconstruction.
Inventory of Complicated Grief (Prigerson et al., 1995)
The Inventory of Complicated Grief (ICG) comprises 19 self-report items designed to assess CG. The items evaluate the frequency of different symptoms at the behavioral, cognitive and emotional levels. They are answered on a 5-point Likert scale that ranges from 0 (“never”) to 4 (“always”). We used the Spanish adaptation (Limonero García et al., 2009), with similar psychometric properties to the original (Cronbach’s alpha internal consistency α = .88). To compute the total score, the items ratings are summed. According to Prigerson et al., (1995) a score of 25 or more represents the probable presence of complicated grief.
Hospital Depression and Anxiety Scale (Zigmond & Snaith, 1983)
The Hospital Depression and Anxiety Scale (HADS) consists of 14 self-report items developed to assess the behavioral and cognitive symptoms associated with depression and anxiety. The HADS comprises two 7-items subscales, focused on depression (HADS-D) and anxiety (HADS-A). Items are answered on a 5-point Likert’s scale (0–4) with different answer options. Two subscores are computed by summing the item ratings of each subscale. A total score is computed by averaging the two subscores. We applied the Spanish version (Herrero et al., 2003; Quintana et al., 2003), which has good psychometric properties (Cronbach’s alpha internal consistency α = .86 for each subscale). A cut-off of 11 has been reported, and a threshold range of 8–10 defines a probable case of clinically significant anxiety and/or depression, with scores below eight representing subclinical levels of both sets of symptoms.
Data Analyses
To assess whether there were differences between type of relationship of the deceased and cause of death in the scores of the instruments applied, we performed a multivariate analysis of variance (MANOVA). With correlations we explored the relationship between age, time since loss and the instrument scores. The reliability of the GMRI was estimated with Cronbach’s alpha and McDonald’s omega indexes. The 95% confidence intervals (CI) for these indexes were computed with bootstrapping. McDonald’s omega was calculated with the method proposed by Hancock and An (2020).
Construct validity was assessed with exploratory (EFA) and confirmatory factor analyses (CFA). Exploratory factor analysis was performed with maximum likelihood estimation applying orthogonal varimax rotation. For CFA the maximum likelihood estimator was also used. The different models tested with CFA were compared with the goodness of fit (GoF) indexes. Based on the best fit model obtained with CFA, scores for the subscales of the GMRI were computed. These scores were correlated with the scores of the other instruments to establish convergent validity. Two linear regression models were computed to estimate the predictive validity of the GMRI for the ICG total score. In the first model, the GMRI total score was used. In the second model, with the forward stepwise procedure, the GMRI subscale scores were introduced to the model.
The NA was computed with EBICglasso (Extended Bayesian Information Criterion Graphical Least Absolute Shrinkage Selection Operator) estimation. Exploratory factor analysis, MANOVAs, correlations and linear regression were estimated using IBM SPSS 26 (IBM Corp, 2020). Reliability indexes were calculated with the package OMEGA (Hayes & Coutts, 2020) on IBM SPSS 26. Confirmatory factor analyses was performed using Mplus 8 (Muthén & Muthén, 1998-2017). Network analysis and its centrality measures were computed with JASP (JASP Team, 2020) and their GoF indexes were calculated with the R package Psychonetrics (Epskamp, 2021) on R (R Core Team, 2021) using RStudio (RStudio Team, 2021).
Results
Characteristics of the Sample
Mean and standard deviation (SD) for the Grief and Meaning Reconstruction Inventory (GMRI) total score, Inventory of Complicated Grief and Hospital Depression and Anxiety Scale (HADS) scores for the total sample, men and women, relationship of the deceased, cause of death and previous losses.
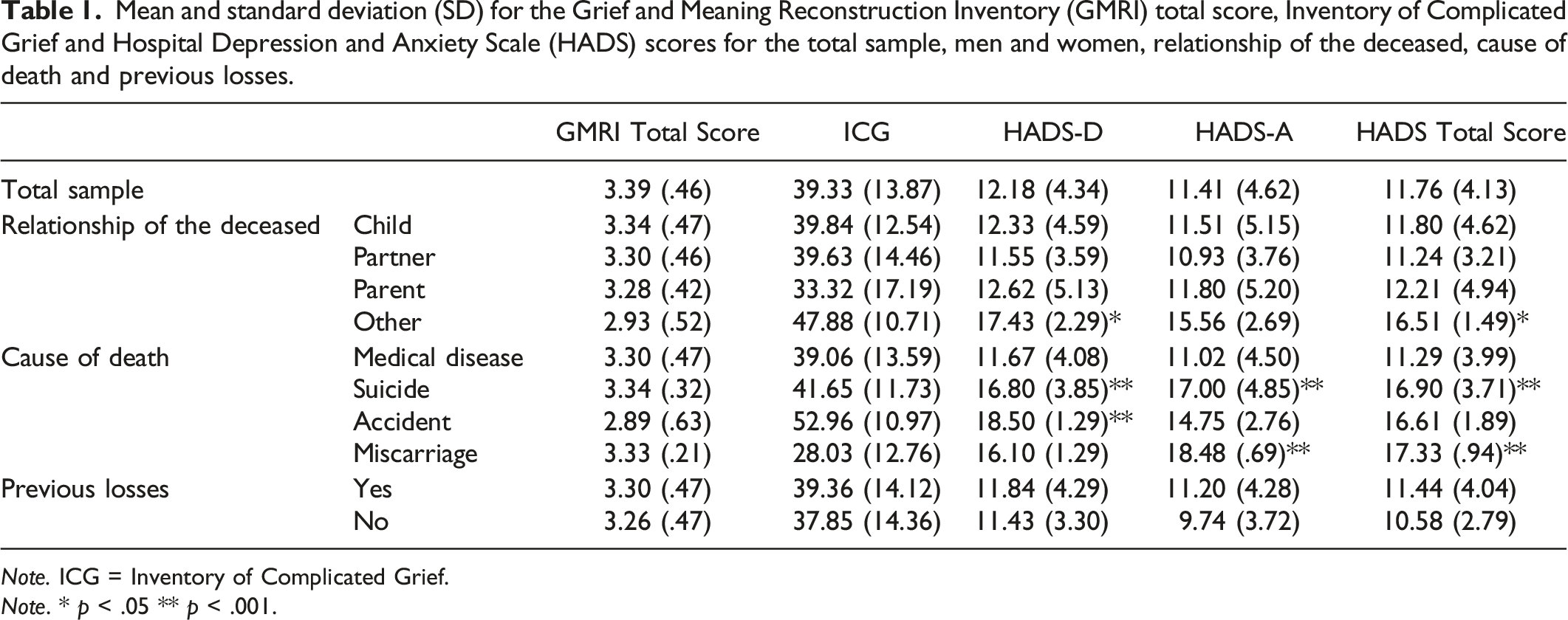
Note. ICG = Inventory of Complicated Grief.
Note. * p < .05 ** p < .001.
Background Factors
In terms of differences in the type of relationship of the deceased on the HADS, with Pillai’s trace, there was a significant effect of the relationship of the deceased on the HADS-D and HADS-A, V = .10, F(9, 546) = 2.03, p = .034 and on the HADS total score, V = .090, F(6, 366) = 2.79, p = .011. Again, in these two models, the ICG score was included as a control variable to separate the effect of grief on depression and anxiety levels. Post-hoc univariate tests revealed statistically significant differences between the type of relationship of the deceased in the HADS-D, F(3, 182) = 4.13, p = .007, η 2 p = .06, and HADS total score, F(3, 183) = 3.52, p = .016, η 2 p = .06, with those who had another type of relationship of the deceased experimenting higher symptoms than those who had lost a child, a partner or a parent (see Table 1). No differences between the type of relationship of the deceased were found in the ICG and GMRI total score.
Similarly, when controlling for the ICG total score, there was a significant effect of the cause of death (using Pillai’s trace) on the HADS-D and HADS-A, V = .16, F(9, 543) = 3.32, p = .001 and on the HADS total score, V = .13, F(6, 364) = 4.29, p < .001. According to post-hoc univariate tests, patients who lost someone due to suicide and an accident presented higher levels of depression (HADS-D) than patients who lost someone because of a medical disease, F(3, 181) = 6.89, p < .001, η 2 p = .10. Likewise, patients who lost someone due to suicide and miscarriage presented higher levels of anxiety (HADS-A), F(3, 181) = 5.43, p = .001, η 2 p = .08, and general psychological distress (HADS total score) than patients who lost someone due to a medical disease, F(3, 182) = 6.90, p < .001, η 2 p = .10. No differences in the HADS, ICG and GMRI total scores were found between those who had experienced previous losses and those who did not.
The age of the participants was negative statistically significant correlated with HADS-D, r = −.21, p < .01, and HADS total score, r = −.16, p < .05. The variable time since loss obtained statistically significant positive correlations with HADS-A, r = .23, p < .01, and HADS total score, r = .20, p < .05. These variables did not obtain statistically significant correlations with the ICG and GMRI total score.
Reliability
Cronbach’s alpha and McDonald’s omega resulted in α = .78 [.73, .81] and ω = .77 [.72, .81], respectively, for the Spanish GMRI, indicating a good reliability.
Construct Validity
Exploratory factor analysis
The Kaiser–Meyer–Olkin (KMO) measure verified the sampling adequacy for the analysis, KMO = .72 (‘middling’ according to Kaiser and Rice [1974]), and all KMO values for individual items were greater than the acceptable limit of .5 (Kaiser & Rice, 1974). Bartlett’s test of sphericity, x 2 (406) = 1313.48, p < .001, indicated the adequacy of the correlation matrix for the estimations. An initial analysis was run to obtain eigenvalues for each factor in the data. Nine factors had eigenvalues over Kaiser’s criterion of one and in combination explained 62.02% of the variance. The nine-factor solution was retained as is shown in Supplementary Table 1. These nine factors were called: I. Personal Growth; II. Identity Change; III. Preparation for the Death; IV. Death as Relief; V. Belief in Afterlife; VI. Valuing Others; VII. Validation of Deceased; VIII. Senselessness; IX. Negative Changes From Loss.
Confirmatory Factor Analysis
Three factorial structure models were tested with CFA: Gillies et al. (2015) original model, the nine-factor model previously obtained with EFA, and an eight-factor model (with the idea of reducing factors following Gillies et al., [2015] original structure to obtain a more parsimonious model). For the eight-factor model, the items belonging to factors VIII and IX from the EFA were grouped in one factor called Emptiness and Meaninglessness. Gillies et al. (2015) original model did not converge. The other two models were compared with the GoF indexes. The nine factor model resulted in a Log-likelihood = −8558.02, x 2 (341) = 552.21, p < .0001, RMSEA = .06, AIC = 17,914.24, BIC = 18,321.16, CFI = .81, TLI = .78. In contrast, the eight factor model obtained a Log-likelihood = −8558.02, x 2 (349) = 560.17, p < .0001, RMSEA = .06, AIC = 17, 906.20, BIC = 18,286.65, CFI = .81, TLI = .78. Based on the GoF indexes, the eight-factor model resulted in a better adjustment to the data. The factor loadings of this model are shown in Supplementary Table 2.
Convergent Validity
Correlations between Grief and Meaning Reconstruction Inventory (GMRI), Hospital Depression and Anxiety Scale (HADS) and Inventory of Complicated Grief (ICG) scores.
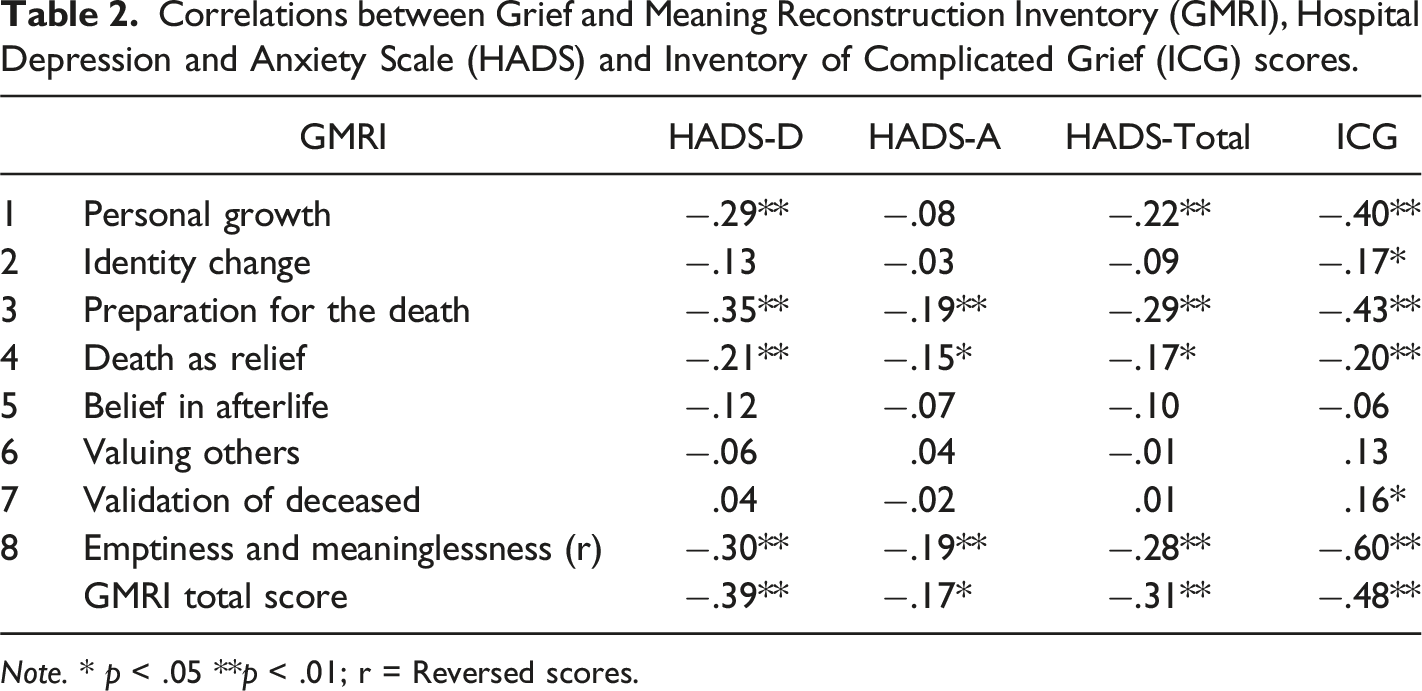
Note. * p < .05 **p < .01; r = Reversed scores.
Predictive Validity
Linear models of predictors of the Inventory of Complicated Grief (ICG) total score from the Grief Meaning Reconstruction Inventory (GMRI) Spanish subscales.
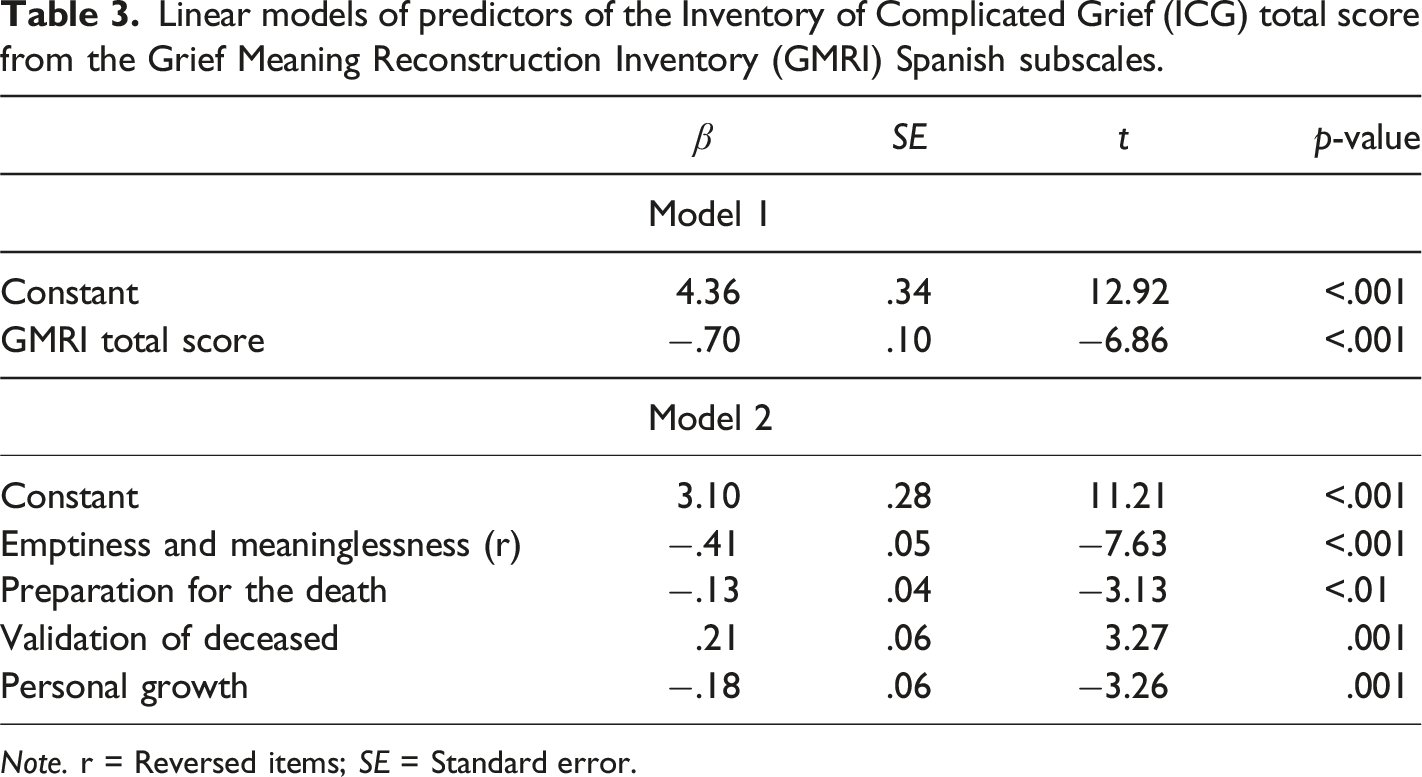
Note. r = Reversed items; SE = Standard error.
Relationship Between GMRI Subscales and Background Factors
There was a significant effect of relationship of the deceased on the GMRI subscales, V = .26, F(8, 175) = 2.14, p = .001, particularly on Preparation for the Death, F(3, 182) = 9.86, p = .035, η 2 p = .049, with post-hoc contrasts revealing a statistically significant difference between child (M = 2.11, SD = .91) and partner (M = 2.48, SD = 1.14), with those who had lost a partner obtaining a higher score; and Validation of Deceased, F(3, 182) = 6.72, p < .001, η 2 p = .10, with post-hoc contrasts revealing statistically significant differences between child (M = 4.82, SD = .31) and partner (M = 4.45, SD = .78), and child and parent (M = 4.43, SD = .65), with those who had lost a child obtaining higher scores. Additionally, no significant effect of cause of death on the GMRI subscales was found. No differences in the GMRI subscale scores were found between those who had experienced previous losses and those who did not. Time since the loss was not correlated with any of the GMRI subscales or GMRI total score. However, the age of the patients was statistical significantly correlated with Preparation for the Death, r = .27, p < .001, and Validation of Deceased, r = −.24, p < .001.
Network Analysis
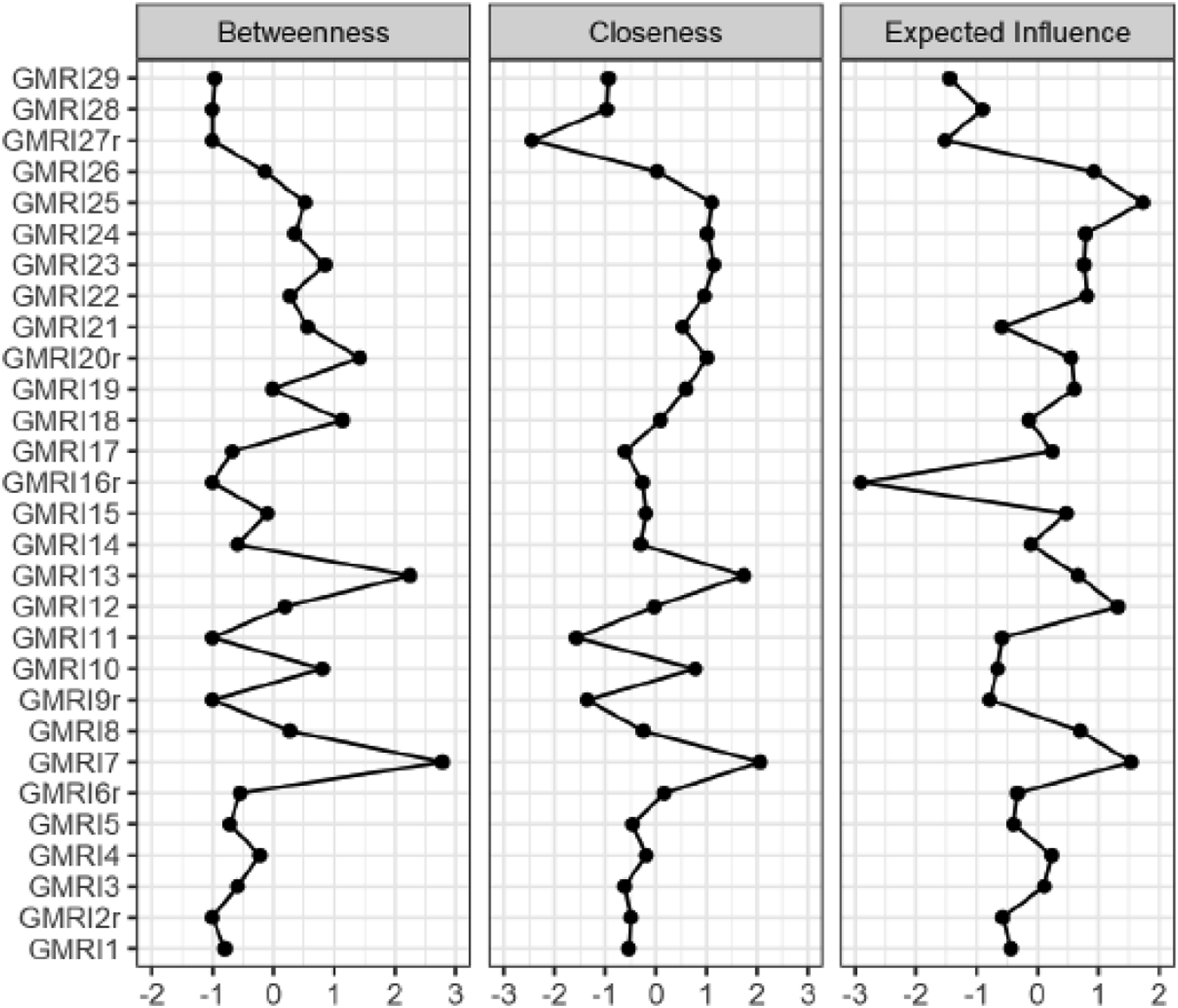
A network model using the EBICglasso estimation was computed including the 29 items. We obtained the network shown in Figure 1 with 106 non-zero edges (from 406) and a Sparsity degree of .74. The GoF indexes of the network model are the following: Log-likelihood = −8769.28, x
2
(352) = 398.90, p = .043, RMSEA = .03, AIC = 17,704.56, BIC = 17,979.14, CFI = .96, TLI = .95. Figure 2 shows three plots: two with the centrality measures of the network (betweenness and closeness) and one for expected influence. Of note, in keeping with meaning reconstruction theory, the sense-making node (item 7) emerged as the most central and theoretically most influential element of the meaning making network, followed by nodes related to valuing life and relationships (items 12 and 13) and identity change (item 13). The implications of these findings regarding node centrality will be discussed below. Network structure for the Spanish Grief and Meaning Reconstruction Inventory (GMRI). Centrality plots and expected influence. Note. GMRI = Grief and Meaning Reconstruction Inventory (and its item numbers [with r are those reverted]). Betweenness = The number of shortest paths that pass through the node of interest. Closeness = The inverse of the sum of all shortest paths from the node of interest to all other nodes. Expected influence = Probability of the node of interest to influence all other nodes.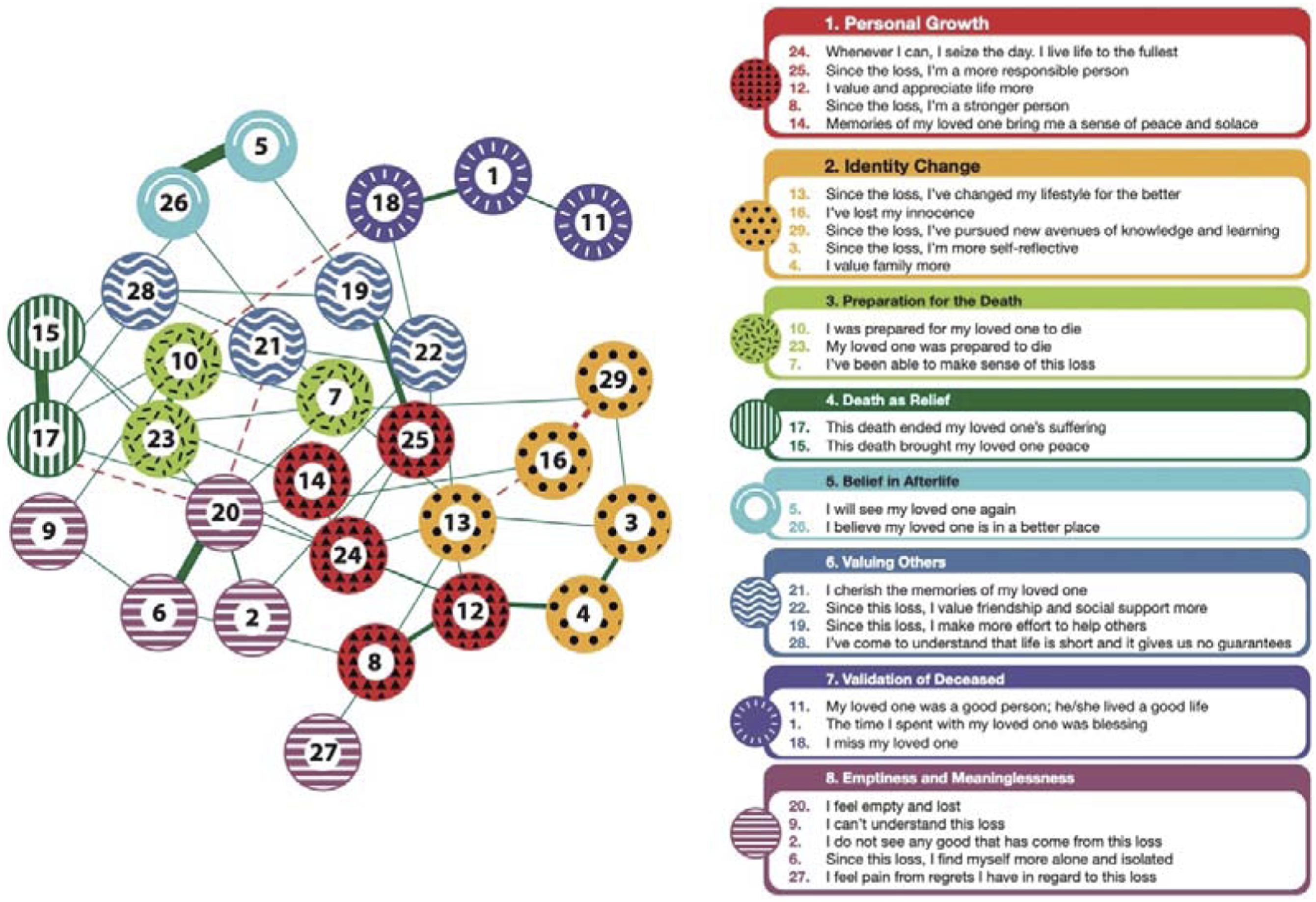
Discussion
Psychometric Properties of the Spanish GMRI
The study reported the psychometric properties of the Spanish version of the GMRI in a sample of Spanish mourners in grief therapy. The sample was comprised of bereaved patients seeking treatment and experiencing psychological distress associated with grief (ICG scores >25, suggesting CG according to Prigerson et al., [1995]). This is also shown in their HADS scores, which are slightly higher than 11 on average, indicating the presence of clinically significant depressive and anxious symptoms.
In terms of the Spanish GMRI total score, the participants showed medium levels of meaning reconstruction after the loss when considering the scores ranging from 1 to 5. These scores seem to be lower than the mean of Gillies et al.’s (2015) study (M = 3.82, SD = .42).
The Spanish GMRI showed good reliability (as estimated with Cronbach’s alpha and McDonald’s’ omega), indicating that its items are consistent and indicative of the same construct. In terms of construct validity, with EFA, we obtained a nine-factor solution in contrast to the original study in which they obtained five. This may be due to the differences in the sample characteristics between the two studies: bereaved students versus mourners in grief therapy. That is, our sample was obtained from treatment-seeking patients, so unsurprisingly the scores in the three instruments used (GMRI, ICG and HADS) suggested substantial distress across all measures. Moreover, the current patients were struggling with quite difficult losses: 44.6% had lost a child and 34.2% a partner.
Item 16 (“I’ve lost my innocence”) loaded negatively to Factor 2, Identity change. In English, losing innocence is understood as not trusting or losing faith in the goodness of life, world or people. In Spanish, although this item can be interpreted in that way, it may also be understood as gaining maturity and growing due to losing a naive understanding of life. Having this positive connotation in Spanish, the item is answered as a double negative statement; therefore, loading negatively when its scores are reversed.
Regarding CFA, Gillies et al. (2015) original model did not converge, stressing, even more, the differences in sample characteristics. The nine-factor model previously obtained with EFA, although it converged, did not show a good fit (Hooper et al., 2008): Chi-squared p-value < .05; CFI (Comparative Fit Index) < .90; TLI (Tucker-Lewis Index) < .95. However, the RMSEA (Root Mean Squared of Approximation) showed an acceptable adjustment (RMSEA <.08; Hooper et al., 2008). Following the factors obtained by Gillies et al. (2015), we tested an eight-factor model, grouping the last two into a single factor called, as by Gillies et al. (2015), Emptiness and meaninglessness. Even though some of the GoF indexes are under the threshold required to consider it a good fit, based on the AIC (Akaike Information Criterion) and BIC (Bayesian Information Criterion) used for comparison purposes (the lower the values, the better the model), the eight-factor model better explains the data structure than the nine-factor model. Therefore, the structure of this model was chosen to represent the subscales of the Spanish GMRI and perform further analyses. Considering the lack of fit reflected by some indexes, these results should be interpreted with caution (see limitations and future directions section for more details).
From a theoretical perspective, it should be noticed that the three activities of meaning reconstruction involved in the grieving process conceptualized by Gillies and Neimeyer (2006) can be associated with three of the factors we obtained: sense making with Factors 3 and 4 Preparation for the Death and Acceptance of the Death, benefit finding with Factor 1 and 2 Personal Growth, Identity Change. In this sense, the Spanish GMRI is capturing three core processes associated with meaning reconstruction after the loss. Other factors represent additional dimensions entailed in PTG, bearing on spirituality (Factor 5 Belief in Afterlife) and altruism regarding relationships (Factor 6 Valuing Others), as well as an affirming continuing bond (Factor 7 Validating the Deceased). With the final addition of Factor 8 Emptiness and Meaninglessness, the Spanish GMRI therefore provides a broad assessment of the various dimensions of meaning making in bereavement.
Regarding convergent validity, the GMRI total score was significantly negatively correlated with the scores of all other instruments. That is, it displayed medium correlations with the ICG, HADS-D and HADS-Total scores, and a more modest correlation with the HADS-A score. Thus, mourners reporting more meaning reconstruction reported fewer symptoms of depression and complicated grief, and to a lesser extent, anxiety. These results are similar to those reported by Gillies et al. (2015).
In terms of predictive validity, we obtained a model in which 48% of the ICG variance was explained by greater Emptiness and Meaninglessness and Validation of the Deceased, and less Preparation for the Death and Personal Growth. Thus, bereaved patients reporting more of the latter were less likely to endorse high levels of CG. In contrast, Emptiness and Meaninglessness, and Validation of the Deceased were positively associated with CG, suggesting a possible diminishment of the relative value of one’s own life in the present.
Network Analysis
The NA allows us to understand the construct of meaning reconstruction as an emergent phenomenon that involves the manifestation and potentiation of different changes in perceptions and attitudes towards loss, life and identity. Theoretically, these processes activate and suppress each other, allowing the emergence of a pattern that we call meaning reconstruction in loss.
When analyzing the centrality measures of the network (Figure 2), item 7 (I’ve been able to make sense of this loss) poses the highest betweenness, closeness, strength and expected influence. Thus, sense-making functions as the central item of the network, the one that establishes the most substantial connections with other items. Therefore, viewed conceptually in network terms, sense-making is fed and activated by the other elements of meaning reconstruction, but at the same time, it co-activates the others. This implies that there could be a virtuous cycle between the changes in perceptions and attitudes towards loss, life and identity measured by each item and the perception of being able to make sense of loss. Following the expected influence of the items, for instance, the perception of having changed life for the better since the loss (item 13), valuing and appreciating life more (item 12), and being a more responsible person (item 25) increase the perception of having been able to make sense of loss (item 7). At the same time, having this latter perception positively reinforces the previous ones.
Nonetheless, it is necessary to consider the criticism that the use of centrality measures in NA has received (Bringmann et al., 2019). That is, betweenness and closeness seem to be unsuitable as measures of node importance. It is not clear what they represent in psychological terms, and their consistency varies depending on the network structure and not necessarily on the item content. Therefore, the potentially central role of sense-making in the network should be posited with caution. Some authors in the grief research field have suggested using more precise measures like expected influence to interpret grief-related networks (Robinaugh et al., 2014; Robinaugh et al., 2016). As we noted above, the items with the highest probability of influencing others are 7, 13, 12 and 25, which accords with a large and growing body of evidence that sense making both contemporaneously (Currier et al., 2008; Lichtenthal et al., 2010) and longitudinally (Coleman & Neimeyer, 2010; Milman et al., 2017; 2019) predicts more adaptive grief outcomes in a wide range of bereaved populations. In light of the present NA, this might be explained in part by its role in activating and supporting other meaning enhancing processes in a network of interacting attitudes and behaviors that jointly comprise meaning making in the wake of loss.
Clinical Implications
The results of this study carry useful implications for psychological assessment and intervention with bereaved persons who are contending with intense, complicated or prolonged grief trajectories following profound losses. First, our findings regarding the demonstrated reliability and validity of the Spanish GMRI argue for its utility as a multidimensional measure of meaning-making in the wake of loss for speakers of that language, which can help identify both areas of vulnerabilities and strengths. Repetition of the same measure over time can also help track progress across the course of therapy and play a useful role in testing possible mechanisms of change in research on grief therapy.
Second, the link between several GMRI subscales—Personal Growth, Identity Change, Preparation for the Death and Acceptance of the Death—and more favorable grief outcomes suggests the utility of meaning-oriented therapeutic techniques and procedures in fostering adaptive coping for clients both as their loved one approaches death (Burke et al., 2015) and in the months that follow (Burke et al., 2017). A large and diverse clinical toolbox of such methods exists to support this effort (Neimeyer, 2012, 2016, 2022).
Limitations and Future Directions
Although the present study benefitted from the use of validated measures, state-of-the art translation protocols, and the recruitment of a large group of bereaved patients receiving grief therapy at major research hospitals, it nonetheless has some limitations. First, as a single-point assessment study, no test-retest reliability analyses were performed. Therefore, conclusions about the stability of the constructs assessed with the Spanish GMRI await further longitudinal study. Considering that our sample was constituted by mourners receiving grief therapy, it is highly probable that their scores would change over time, not only because the effects of therapy in their processes of grief-meaning reconstruction and symptoms, but also because patients may change the way they interpret the item content (i.e., response shift; Vanier et al., 2021).
Second, the GoF indexes we obtained when evaluating the factorial structure of the questionnaire are not completely accurate, specifically the Chi-squared test (p < .05), indicating that the model was not an optimal fit to the data. Some authors (Hu & Bentler, 1999; Sun, 2005) criticize the use of the Chi-squared test to assess structural equations models (SEM), recommending the use of other indexes, like the RMSEA, which in the present study suggested an acceptable fit (RMSEA <.08). However, based on the AIC and BIC, the eight-factor model outperformed the nine-factor model. While it is true that the network model also obtained a p-value under the threshold (p = .045) in the Chi-squared test, this value is closer to .05 than the value of the other models, and all other indexes (RMSEA, CFI, TLI) exceed the threshold, indicating a good fit of the model. Considering that the probability of Chi-squared p-value > .05 in SEM increases proportionally with the sample size (Muthén & Muthén, 2002; Wolf et al., 2013), it is probable that with higher sample size, the problems of lack of fit would resolve. Regarding the questionnaire content, the translation of item 16 presented problems in its interpretation as the EFA, CFA, and NA suggested. Considering these results, we suggest a different adapted translation: “Now I know that life does not have to be fair and kind.” This sentence in Spanish aligns more clearly with the meaning of the English sentence “I’ve lost my innocence.” In future research, this item should be added to the Spanish GMRI to test its accuracy and how it affects the psychometric properties of the instrument if substituted for the original more ambiguous item.
Conclusion
The Spanish GMRI displayed acceptable psychometric properties with good levels of internal consistency that support its use in both clinical and research settings. It presented a distributed network structure consistent with the theory, in which specific items related to sense-making, identity change and growing from loss (or benefit finding) theoretically have the highest probability of activating other nodes in the meaning-making network. That is, these highly central elements of meaning-making could trigger a ripple effect of changes in perceptions and attitudes towards loss, life and identity that fosters the emergence of meaning reconstruction. The processes that subserve this mechanism are inversely associated with CG and the psychological symptoms that accompany it. Therefore, several of the processes assessed by the Spanish GMRI could act as protective factors against the development of CG in the wake of serious loss. In this sense, the Spanish GMRI represents a potentially helpful tool in clinical practice, not only to assess clients experiencing grief in order to design and implement a treatment plan and monitor treatment progress, but also to design prevention programs. Future research should be aimed at corroborating our findings, contributing to a better understanding of grief processes and meaning reconstruction with Spanish-speaking mourners.
Supplemental Material
Supplemental Material - Adaptation of the Spanish Grief and Meaning Reconstruction Inventory: An Initial Validation and Network Analysis
Supplemental Material for Adaptation of the Spanish Grief and Meaning Reconstruction Inventory: An Initial Validation and Network Analysis by Valeria Moriconi, Amparo Menéndez, Robert A. Neimeyer, and Danilo Moggia in OMEGA - Journal of Death and Dying
Footnotes
Acknowledgments
The authors would like to thank Pilar Aguián Clemente y María Antonia Lacasta Reverte and the invaluable work of the Aladina Foundation and Funadació Hospital de Sant Jaume i Santa Magdalena in supporting families in grief. We would also like to thank the parents who have entrusted us with their stories of love and pain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.