
Abstract
Introduction
This study aimed to determine the effect of an online psychoeducational support group on the perceived stress of caregivers of coronavirus disease 2019 (COVID-19) survivors.
Methods
This randomized clinical trial included 70 caregivers of COVID-19 survivors discharged from Imam Reza Hospital in Mashhad, Iran in 2021. The intervention group received a psychoeducational support training program for stress management through six online group sessions (each 35–45 minutes) in a week. An expert psychiatric nurse provided this program on WhatsApp immediately after the patient’s discharge from the hospital. The participants completed the Perceived Stress Scale (PSS-14) before starting the intervention and 1 week after that. Data analysis was conducted by descriptive and inferential statistics, including Chi-square, Fisher’s exact test, independent, and paired t-test.
Results
Both groups were homogeneous in terms of demographic variables of survivors and caregivers. In terms of the PSS, there was no significant difference between the two groups before the intervention (p=0.28). The pre- and post-intervention scores of PSS in the intervention group were 39.57 ± 5.89 and 35.48 ± 5.68, respectively, indicating a significant decrease (p<0.001). Also, the pre- and post-intervention differences between the intervention and control groups were −4.08 ± 3.52 and −0.11 ± 2.66, respectively, indicating a greater decrease in the total PSS of the intervention group (p < 0.001).
Conclusion
The family caregivers of COVID-19 survivors suffered from psychological distress during their patient care. It is recommended to perform online psychoeducational support group interventions for these individuals based on psychological and educational support program.
Introduction
The outbreak of coronavirus disease 2019 (COVID-19) and its high mortality has imposed a psychological burden on various communities. The results of studies conducted during the COVID-19 pandemic have reported moderate to severe levels of symptoms of psychological distress, including death anxiety, depression, stress, posttraumatic stress disorder (PTSD), and anxiety in individuals (Liu et al., 2020; Mirhosseini et al., 2021; Özgüç et al., 2021; Rehman et al., 2021). Fear of death, exposure to COVID-19 news, exposure of relatives to COVID-19, social stigma, uncertainty about the disease and its treatment, or staying at home quarantine during the COVID-19 pandemic are various factors that have been identified as causing or exacerbating psychological symptoms (Bakioğlu et al., 2021; Guo et al., 2020; Pradhan et al., 2022). COVID-19 patients and survivors experience the psychological distress of the disease (Ma et al., 2020; Cai et al., 2020). This disease not only disrupts their lives, social and family relationships of them but also affects the conditions of their family caregivers (Arnout et al., 2020; Bassi et al., 2021; Abbasi et al., 2020). In this regard, it should be noted that unlike family needs, which are often forgotten, the patients' needs are usually prioritized. Family caregivers face various challenges during the care period, including worsened quality of life, unmet needs, and physical, psychological, and social problems (Wu et al., 2020; Abbasi et al., 2020). In the context of COVID-19, such evidence is confirmed. For example, the results of the study by Jafari-Oori et al. (2021) showed that 77.75%, 75%, and 80% of family caregivers of COVID-19 patients experienced depression, anxiety, and stress in the post-discharge period, respectively (Jafari-Oori et al., 2021). Also, the results of Prakash et al. (2021) showed that 35–40% of family members of these patients suffered from severe symptoms of anxiety, stress, and depression (Prakash et al., 2021). According to the evidence, exposure to death anxiety, grief, and loss during caring for COVID-19 patients are major factors of psychological distress in family caregivers (Morris et al., 2020; Picardi et al., 2021). Previous studies attributed the distress and psychological burden in family members to anxiety and lack of awareness of the patient’s conditions and stress due to providing care for COVID-19 patients or survivors (Mirzaei et al., 2020; Rahimi et al., 2021; Kıssal et al., 2019). Caregivers incur the burden of care while shifting roles and taking responsibility for managing the needs of patients; thus, they need support (Delalibera et al., 2015). Due to limited training and insufficient resources, as well as their low awareness of the emerging disease and how to care for the patient, caregivers of COVID-19 patients face far more challenges than other caregivers (Mirzaei et al., 2020). As the frontline health care providers, nurses are in close contact with the patients and their families in clinical settings. They are known as ‘ideal individuals' to help family caregivers meet their needs and cope with stressful situations (Shorofi et al., 2016). Therefore, considering the important role of nurses in health care systems, multilateral nursing interventions such as online support sessions (LaCoursiere, 2001) are necessary to reduce stress in the family caregivers of COVID-19 survivors, increase their awareness, and address the educational and psychological needs.
One of the most effective psychosocial approaches is psycho-education support which addresses the concerns caused by psychological distress (Nolan & Petrakis, 2019). These interventions are time-limited and have structured methods, including stress management, education for health promotion, and psychiatric support (Ahmad & Meltem Meriç, 2021). Several studies have been performed on caregivers of patients such as stem cell transplantation, children suffering from cancer, and mentally disabled individuals. These studies showed that psycho-education support interventions had a significant effect on reducing distress and promoting mental health, quality of life, and problem-solving skills (Gonzalez-Fraile et al., 2019; Laudenslager et al., 2019; Tang et al., 2020). Since the beginning of the disease, limited studies have evaluated the mental health of caregivers of COVID-19 patients and survivors. However, most of these studies are descriptive and mainly focus on identifying the extent of psychological distress. As a result, few experimental studies with supportive interventions for these individuals have been conducted. For example, the results of Shariati et al. (2021) showed a decrease in the perceived stress of the family members of these patients through online support sessions and web-based communication between family members of COVID-19 patients and nurses (Shariati et al., 2021). Also, the results of a previous study by Nia et al. (2022) revealed that the online support based on family-centered empowerment model (FCEM) significantly reduced depression, anxiety and stress among caregivers of COVID-19 patients (Nia et al., 2022).
The major changes in lifestyles and new needs caused by the prevalence of COVID-19 have led family caregivers of COVID-19 survivors to experience excessive stress. It should be noted that the mental status of family caregivers plays an important role during the caring period. Therefore, the utilization of psycho-education support is necessary to alleviate psychiatric distress. Due to limited studies on perceived stress in family caregivers of COVID-19 survivors, this study aimed to determine the effect of online support groups on perceived stress of these people through using psychoeducational support programs.
Method
Study design
This randomized controlled trial had a pretest-posttest design. The study was registered in the Iranian Clinical Trial Registry system (code: IRCT20210109049978N1) in 2021.
Participants
This study included 70 family caregivers of COVID-19 survivors discharged from Imam Reza Hospital in Mashhad, Iran. The inclusion criteria were being at the age range of 18–60 years, being a member of the patient’s family, caring for a patient hospitalized due to COVID-19 and discharged within a maximum of 1 day, not suffering from disorders such as psychological disorders and addiction, having access to the internet and online social software, being able to utilize smartphones at least as a basic user, not participating in other supportive interventions concerning COVID-19, and not being employed in medical professions (such as a physician, nurse, midwife, etc.). The exclusion criteria were not participation in the posttest phase, not attending more than two sessions of online support groups, and unwillingness to continue participation in the study. Using quadruple random blocking allocation, the participants were divided into two groups of intervention and control (Figure 1). CONSORT flow diagram of the study.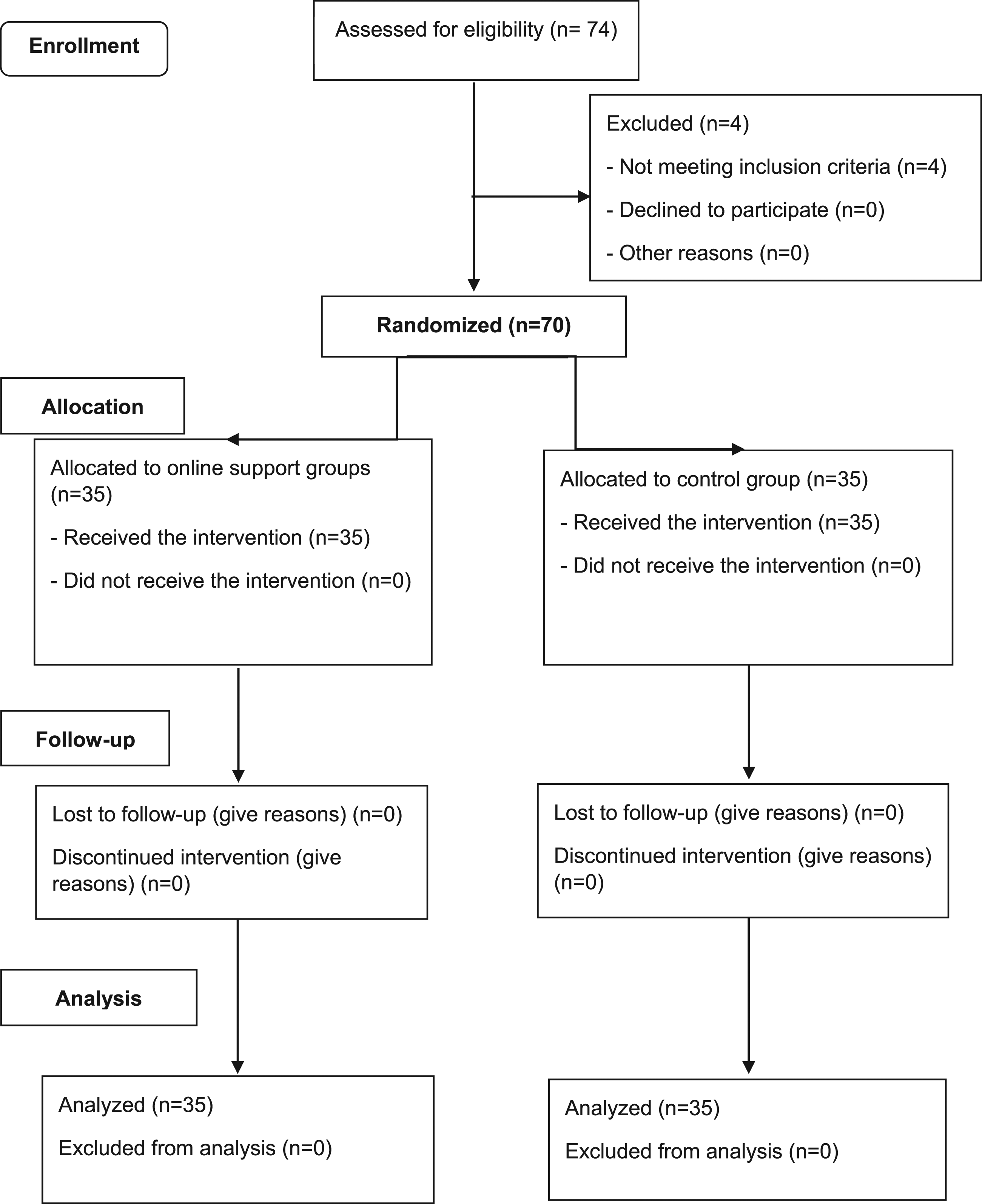
Measures
Demographic characteristics form
We recorded the demographic characteristics of the survivors and their caregivers, including age, gender, marital status, academic degree, and employment status. Also, we considered the following issues: the relationship and cohabitation status of the caregiver and survivor, the caregiver’s monthly income, the patient’s history of hospitalization in the intensive care unit (ICU) due to COVID-19, the caregiver’s history of COVID-19, and the history of COVID-19 induced infection or death in the caregiver’s relatives.
Checklist of COVID-19 educational needs
This checklist included 17 questions in seven areas (general education on COVID-19, infection control, nutrition, child protection, older adults protection, contact with a COVID-19 patient, and social stigma on the COVID-19 patients and their families). The response options were as follows: “no need, low, medium, and high”.
The perceived stress scale (PSS-14)
This 14-item scale was developed by Cohen et al. (1983) to measure perceived stress. Each question gets a score from 0 to 56 according to the individual’s answer (never = 0, rarely = 1, somewhat = 2, relatively high = 3, high = 4). Scoring the questions is inverse (4, 5, 6, 7, 9, 10, and 13), where a higher score indicates more perceived stress and vice versa (Cohen et al., 1983). The reliability of this scale was confirmed by Hosseini et al. (2016) using Cronbach’s alpha correlation coefficient of 0.85 (Hosseini et al., 2016). The reliability of the scale in our study was evaluated using the internal consistency method by calculating Cronbach’s alpha coefficient of 0.73.
The validity of the instruments of this study was confirmed by seven academic staff of the Mashhad School of Nursing and Midwifery. The online forms of data collection were prepared through Porsline web-based service (https://survey.porsline.ir) in the local language (Persian) and sent to the caregivers. The data collection form was completed twice (once before the intervention and again 1 week after the intervention).
Intervention
Six online psychoeducational group sessions were conducted by the first author (S. M.), who is an expert psychiatric nurse. To do so, we made live video calls in WhatsApp to a group of three to five individuals during 1 week. Each session lasted for 35–45 minutes. The reasons for selecting WhatsApp were its usability and availability features, as well as the possibility of making video calls in a group format and the option of broadcasting live images of the individuals for intervention. The intervention was planned and guided by the researcher. Considering the caregivers’ duty to care for the discharged individual, the first three sessions included topics related to COVID-19, and the second three sessions dealt with psychiatric support training according to stress management plan based on the transactional model of stress and coping by Lazarus (1984). According to the needs assessments, the required educational contents for each session were sent 1 day before that session in video clip formats to members in groups so that they could discuss content during the session.
Regarding the content of sessions, the first session included items such as general instruction about the supportive sessions, examining educational needs toward COVID-19, method of using protective equipment, and caring for COVID-19 survivors at home after discharge; the second session included nutrition management and the method of caring for the elderly and child survivors suffering from COVID-19; the third session included infection control and disinfection, warning signs of the disease, and education on how to use drugs; the fourth session included definition of stress (its process and consequences), examining the stressful situations during care, and COVID-19 stigmatization; the fifth session included identifying the stressful dysfunctional thoughts (challenges, replacing irrational thoughts with logical ones, and their reappraisal) and selecting a suitable problem-based or emotion-based coping strategy in stressful situations; and the sixth session included the summary of relaxation and problem-solving techniques, discussing the educational programs provided in previous sessions, and integration of these programs in daily life.
Meanwhile, participants in the control group received routine interventions of the medical center, such as benefiting from post-discharge training and COVID-19 telephone systems such as 4030 in Iran.
Sample size
According to a previous study by Khashouei et al. (2016), taking 95% confidence interval and 80% test power into account, and considering the probability of data loss, the sample size was calculated as 70 individuals.
Blinding
The statistical analyzer was blinded to all the group allocations.
Data analysis
Data were analyzed using descriptive statistics and inferential statistics, including Chi-square, Fisher’s exact test, independent t-test, and paired t-test. A p-value <0.05 was considered as significant for all statistical tests.
Ethical considerations
The study protocol was approved by the Ethics Council of Mashhad School of Nursing and Midwifery (code: IR. MUMS.NURSE.REC.1399.051). Prior to study, the procedure was explained to all participants, and they were assured that their information would be kept confidential. Furthermore, the online informed consent form was confirmed by all participants. They were also authorized to withdraw from the study at any point. Considering the online nature of the intervention, all the established groups were disaggregated based on gender. Also, the female caregivers were free to reject a video call and replace it with only voice call.
Results
Demographic Characteristics of Covid-19 Survivors
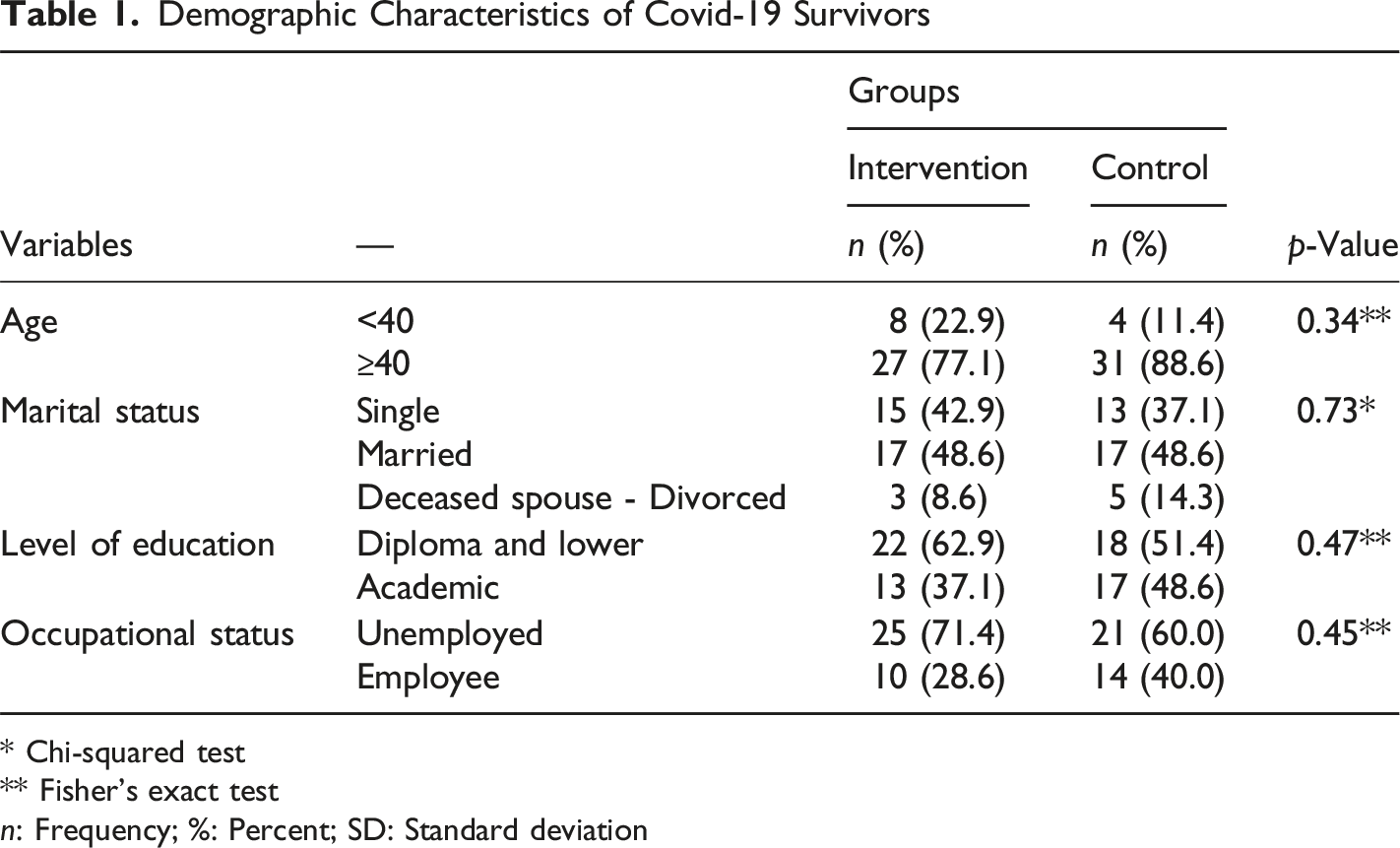
* Chi-squared test
** Fisher’s exact test
n: Frequency; %: Percent; SD: Standard deviation
Demographic Characteristics of Caregivers
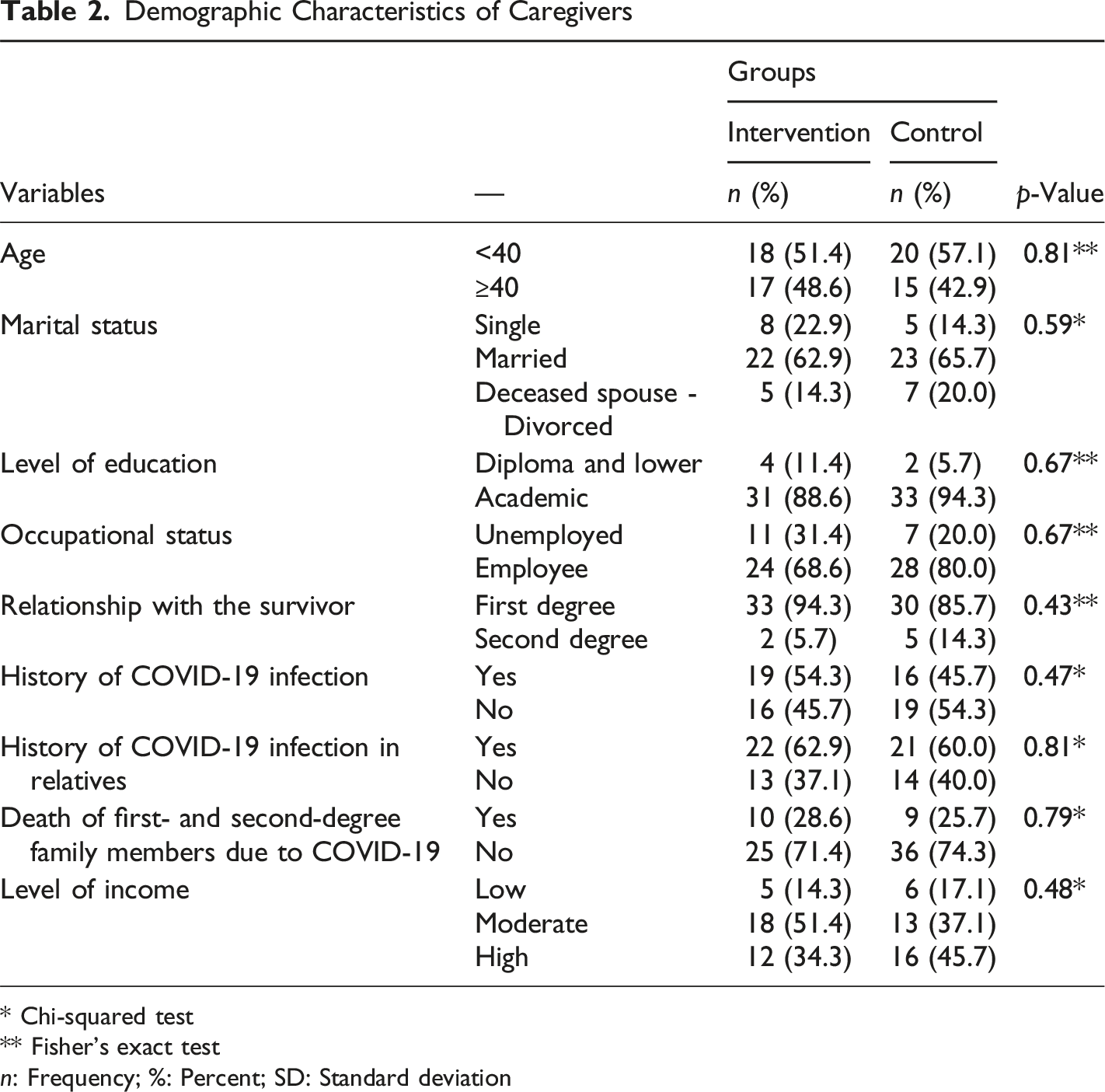
* Chi-squared test
** Fisher’s exact test
n: Frequency; %: Percent; SD: Standard deviation
Mean Score of Perceived Stress in Family Caregivers of COVID-19 Survivors before and after Intervention in Both Groups.
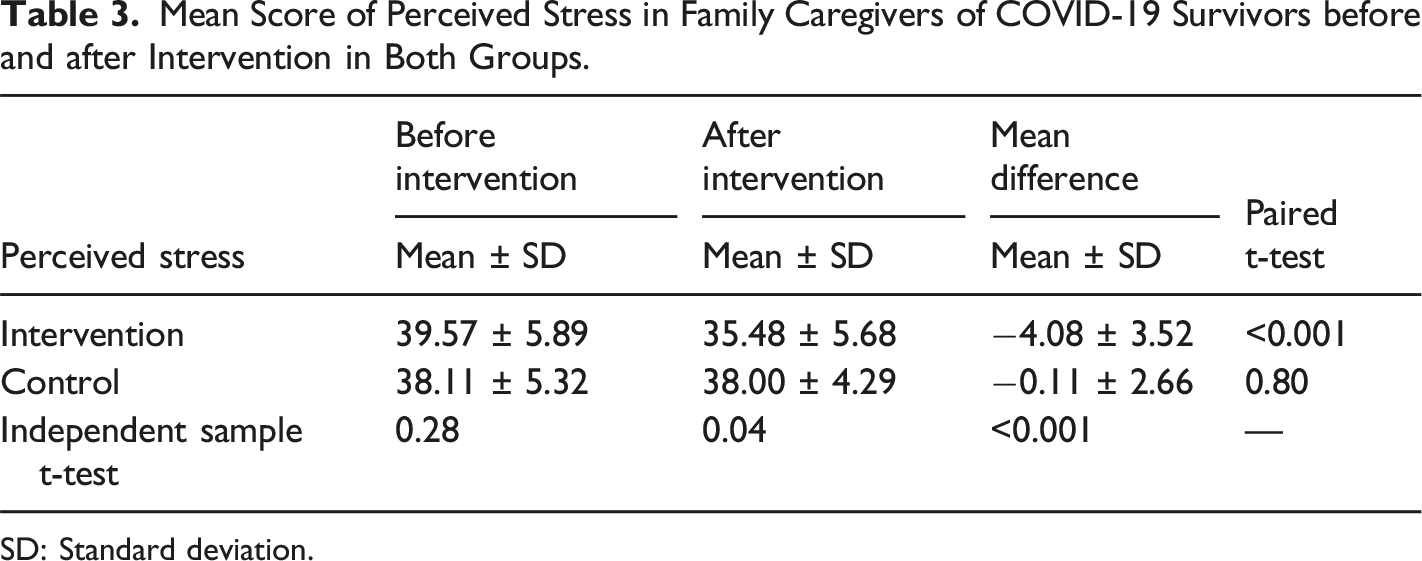
SD: Standard deviation.
Discussion
The findings of this study provided useful guidelines to implement psychoeducational interventions in the form of online support groups to reduce perceived stress in caregivers of COVID-19 survivors. The observed changes are very important because these caregivers are caring for patients who suffer from an unknown and emerging disease with a high prevalence and physical and mental complications (Dar et al., 2021; Fu et al., 2021). The negative physical and psychological consequences of COVID-19 are not limited to the duration of hospitalization, and will last for a long time defined as long COVID-19 (Shinde et al., 2022). The acute physical condition of the patient for a long time (such as severe fatigue, breathlessness, the possibility of sudden death, and chronic and severe neurological problems) and the deteriorated psychological condition (such as post-traumatic stress symptoms and low levels of quality of life) create difficulties for their caregivers (Razai et al., 2021; Russell et al., 2022), which can be considered as a major stressor. These factors can cause psychological distress during patient care.
Although several supportive studies have been conducted during the COVID-19 pandemic, there are still limited cross-sectional studies focusing on caregivers and their mental health after more than 2 years since the outbreak. Consistent with our findings, the findings of the study by Nia et al. (2022) showed that the implementation of an online support group based on FCEM could reduce psychological distress such as depression, anxiety and stress in family caregivers of COVID-19 patients after patient’s discharge (Nia et al., 2022). Also, the results of Shariati et al. (2020) showed that using online communication between the nurse and the patient’s family members had a significant effect on reducing perceived stress in the family members. In the mentioned study, the relationship between the nurse and the patient’s family members was performed during the hospitalization of the patient, but in present study the relationship was performed after the discharge of COVID-19 patients. However, the results were aligned, which indicates the importance of web-based and online interventions. Nowadays, web-based communication is one of the best ways of communication between staff, patients, and their family members (Suen et al., 2020). Rather than caregivers, the supportive interventions have been focused on COVID-19 patients. In this regard, the results of Shaygan et al. (2021) showed that the implementation of online multimedia educational psychological interventions had a significant effect on promoting resilience and reducing perceived stress in COVID-19 patients (Shaygan et al., 2021). According to the study conducted by Wei et al. (2020), using internet-based psychological interventions was effective in relieving the depressive symptoms and anxiety of COVID-19 patients (Wei et al., 2020).
Since individuals, especially caregivers of COVID-19 patients, are dealing with an emerging disease with conflicting information, they must receive up-to-date education. Furthermore, due to the increased psychological burden such as depression and stress, they should be under psychological support. Thus, the importance of online interventions is doubled (Gallagher & Wetherell, 2020; Moazzami et al., 2020). Furthermore, due to the contagious nature of the disease and risk of infection, all the support sessions were held online.
The results of a study conducted on caregivers of COVID-19 patients showed that these individuals are in dire need of online support (Rahimi et al., 2021). Other studies also indicated the positive effect of online supportive interventions on reducing psychological distress in caregivers. Although these studies were not concerned with COVID-19, the results were in line with the present study. For example, the results of a systematic review and meta-analysis study showed that the use of electronic health interventions such as online interventions had a significant effect on reducing depression and improving the life quality of caregivers of family patients with cancer (Li et al., 2022). According to Karagiozi et al. (2021), using online psychoeducation interventions for health caregivers significantly helped physicians and nurses working with family caregivers. Particularly, the implementation of this type of online intervention reduced the level of anxiety, depression, and care burden in caregivers of patients with dementia during the quarantine period due to the COVID-19 pandemic (Karagiozi et al., 2021).
In providing psychoeducation, in addition to reducing psychological distress, online communication was used to educate the patient and family, which showed positive results (Cox et al., 2018). The implementation of online support groups for caregivers is affordable and does not require advanced clinical facilities. Also, caregivers in these groups might share their caregiving experiences, which is a contributing factor to patient care. As shown by previous studies, another advantage of participating in these groups includes the opportunity to share and obtain information and receive support from others (Akbari Shaker et al., 2020; Haik et al., 2019).
Considering that COVID-19 is an acute respiratory disease with high contagious nature and the home care period for affected survivors is usually 3 weeks, the generalizability of the results of the present study to other situations may be limited. As a limitation, although we did not consider caregivers' COVID-19 infection during care from the beginning of the study, no individuals were infected based on our daily evaluation until the end of the study.
Conclusion
Family caregivers of COVID-19 survivors experience psychological distress such as perceived stress during the care period after the discharge of their patients. Using an online psychoeducational support group is suggested as a useful and low-cost solution to relieving the psychological stress of caregivers of COVID-19 survivors.
ORCID iD
Seyedmohammad Mirhosseini https://orcid.org/0000-0002-2087-0164
Footnotes
Acknowledgments
The study was a result of a nursing thesis approved by the research council of Mashhad University of Medical Sciences under referral code of 990450. We would like to express our thankfulness and gratitude to this university and study participants for their contributions to this research and we thank Mr Samuel Grimwood who provided text editing that greatly assisted the research.