
Abstract
The purpose of this study was to determine racial/ethnic differences in provider-engaged religious belief discussion with older adults in the final month of life. Data were derived from the combined 2012 to 2020 National Health and Aging Trends Study. Chi-square tests were used for bivariate analysis, and a binary logistic regression model was used to test the association between race/ethnicity and provider-engaged religious belief discussions at the end of life. After controlling for other explanatory factors during the analysis, results showed that providers were less likely to have religious belief discussions with Black and Hispanic older adults compared to Whites. The results of this study point to a significant gap in knowledge among healthcare providers whose diversity training may not be inclusive of religious/spiritual cultural humility. Implications for research, policy, and practice are provided.
Introduction
According to the Centers for Disease Control and Prevention (CDC), chronic illnesses such as heart disease and cancer are the leading causes of the death in the United States (Xu et al., 2020). Most recently, the National Council on Aging (2021) estimated that about 80% of older adults (65+) have at least one chronic illness, and 70% of Medicare beneficiaries have two or more. While there are increasing advances in medical care, the impact of chronic illness on quality of life remains a dire area of focus in the field of palliative and end-of-life care (Rome et al., 2011). Research shows that physical comfort, psychological well-being, and spiritual health can all moderate the quality of a person’s life along the chronic illness trajectory (Neimeyer et al., 2011; Vazquez & Satone, 2011). While physical and psychological factors have been recognized as important factors for older adults with chronic illness, religious/spiritual health has only begun to emerge as a priority area of focus for end-of-life researchers.
Religion at the End of Life
Research on the role of religion at the end of life has specifically burgeoned over the past few decades, as researchers continually recognize how faith can be a source of support for older adults with chronic illnesses. For example, some researchers have discovered that individuals with religious beliefs are more likely to have greater self-rated health, more social participation, and fewer depressive symptoms at the end of life compared to those without religious beliefs (Idler et al., 2009). Across the lifespan, research shows that religion is positively associated with greater quality of life (Counted et al., 2018). Religious beliefs can also impact the choices made at the end of life, including preferences for medical treatment, advance care planning, and needs for spiritual support (Gijsberts et al., 2019; Sharp et al., 2012; Zhang et al., 2012). Overall, there is consensus that religious/spiritual support is important to those with religious beliefs.
Religion Among Black and Hispanic Older Adults
Christianity is the most common religion practiced in the United States, and data from the Pew Research Center (2022) shows that Blacks and Hispanics are more likely to identify as Christian, and more likely to state that they have an absolute belief in God. Research in the end-of-life field also suggests that Black and Hispanic older adults may consider religious/spiritual beliefs as more important at the end of life compared to Whites (Scherer et al., 2021). Additionally, studies show that religious beliefs tend to dictate the choices made by Black and Hispanic older adults, leading to a preference for aggressive/life-saving treatment and an aversion to alternative options such as palliative and hospice care (Johnson, 2013). Religion also affects beliefs about end-of-life outcomes among Black and Hispanic older adults, including views of pain as a test of their religious faith, and the hope for a miracle cure (Koffman et al., 2008; Sanders et al., 2016; Witcher & Meeker, 2012).
The Current Study
While some studies have begun to examine the role of religion at the end of life, few studies have explicitly aimed to determine whether health professionals discuss religious beliefs with patients at the end of life. Asking patients about their religious beliefs has been identified as a critical aspect of cultural competence in health professionals (Fang et al., 2016; Givler et al., 2020; Pentaris & Thomsen, 2020), yet emerging data suggests that Black and Hispanic individuals are less likely to have religious support from providers (Kutney-Lee et al., 2017). Discussing religious beliefs and patient preferences is a critical first step to ensuring that patients receive religious/spiritual support at the end of life. As such, this study aimed to examine racial/ethnic differences in provider-engaged religious belief discussion with older adults at the end of life. Specifically, the study sought to determine if White, Black, and Hispanic older adults were equally likely to have a health professional engage them in discussions about their religious beliefs. Considering preliminary data from previous studies, the study hypothesis is that Black and Hispanic older adults will be less likely to have provider-engaged religious discussions.
Research Design and Methods
Data Source
Data were derived from the combined 2012 to 2020 last-month-of-life interviews from the National Health and Aging Trends Study (NHATS). The NHATS is an annual longitudinal panel survey of Medicare beneficiaries (aged 65 and older) living in the United States (Kasper et al., 2021). The NHATS is funded by the National Institute on Aging and conducted by researchers from the University of Michigan (Kasper et al., 2021). The last-month-of-life interviews are conducted with a proxy such as a family member in the year after a NHATS participant dies (Kasper et al., 2021). The interviews take place during the specific survey period of the NHATS, so it is important to note that the time since death may vary across different responses. To account for underrepresentation in research studies, the NHATS oversamples individuals who identify as Black/African American and those aged 85 and older. NHATS data are available at: https://www.nhats.org/researcher/data-access/public-use-files. Since this study used publicly available secondary data, it was exempt from Institutional Review Board review per the guidelines of the authors’ institutions.
Dependent Variable
The main dependent variable for the study was “religious belief discussion.” Proxies were asked, “During the last month of life, did any doctors, nurses, or other health professionals talk with SP [sample person] about his/her religious beliefs?” All the responses were coded as either “Yes = 1” or “No = 0” in the sample. The religious belief discussion question is a routine question for the last-month-of-life interviews and has been asked since the first round of interviews in 2012.
Independent Variables
The main independent variable for this study was race/ethnicity. The race/ethnicity variable was coded as White = 0, Black = 1, and Hispanic = 2. Only Whites, Blacks, and Hispanics were included in the sample because they represented 60%, 12%, and 18% of the U.S population, respectively (Kaiser Family Foundation, 2020). The sample sizes from other racial/ethnic groups were excluded because they were too small to make meaningful analyses.
Covariates
In order to account for other factors that could influence provider-engaged religious belief discussion, the following covariates were included: age, sex, income, education, living arrangement, geographic residence, overall health rating (the SP’s self-rated health in the year before they died), and year of interview, which were all measured as categorical variables during the analysis. Year of interview was included to ensure that historical events such as a policy change did not increase or decrease the number of religious belief discussions had in a given year (i.e., internal validity).
Statistical Analyses
At the univariate level, descriptive statistics that included frequencies and percentages were obtained for all variables included in the study. At the bivariate level, Chi-square tests were used to test the association between all independent/control variables and provider-engaged religious belief discussion. At the multivariate level, a binary logistic regression model was used to determine the significant association between race/ethnicity and provider-engaged religious belief discussion at the end of life. To account for the complex sampling design of the NHATS, final analytic weights were used at all levels of analyses (DeMatteis et al., 2021). All statistical tests were performed using SPSS, version 27.
Results
Univariate Results
Univariate and Bivariate Results (N = 2573).
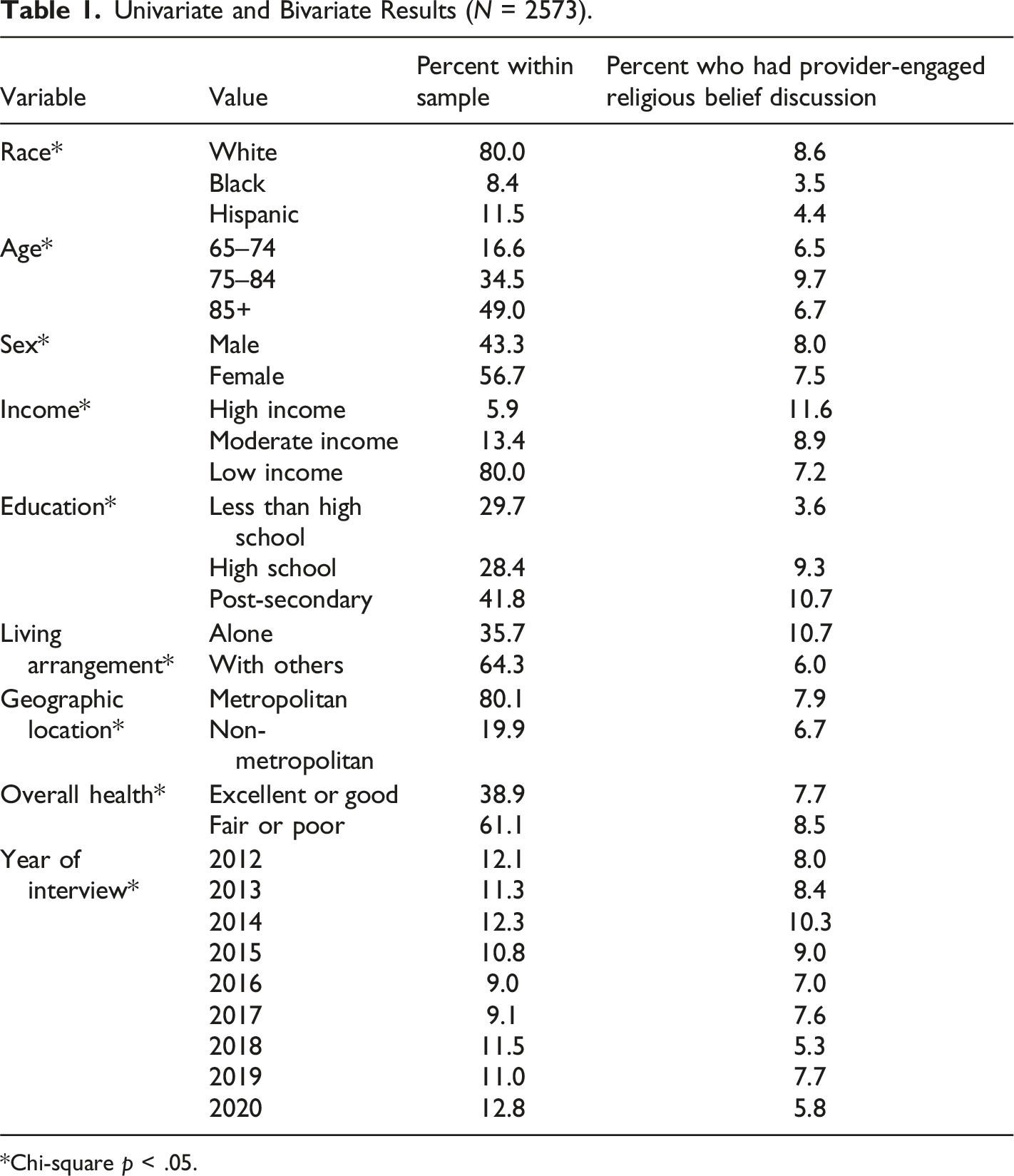
Chi-square p < .05.
Bivariate Results
Without controlling for other factors, the Chi-square test for the association between all independent variables and all dependent variables was statistically significant (p < .05). For the race/ethnicity measure, 8.6% of Whites had religious belief discussions, 3.5% of Blacks had religious belief discussions, and 4.4% of Hispanics had religious belief discussions.
Multivariate Results
Multivariate Results (N = 2573).
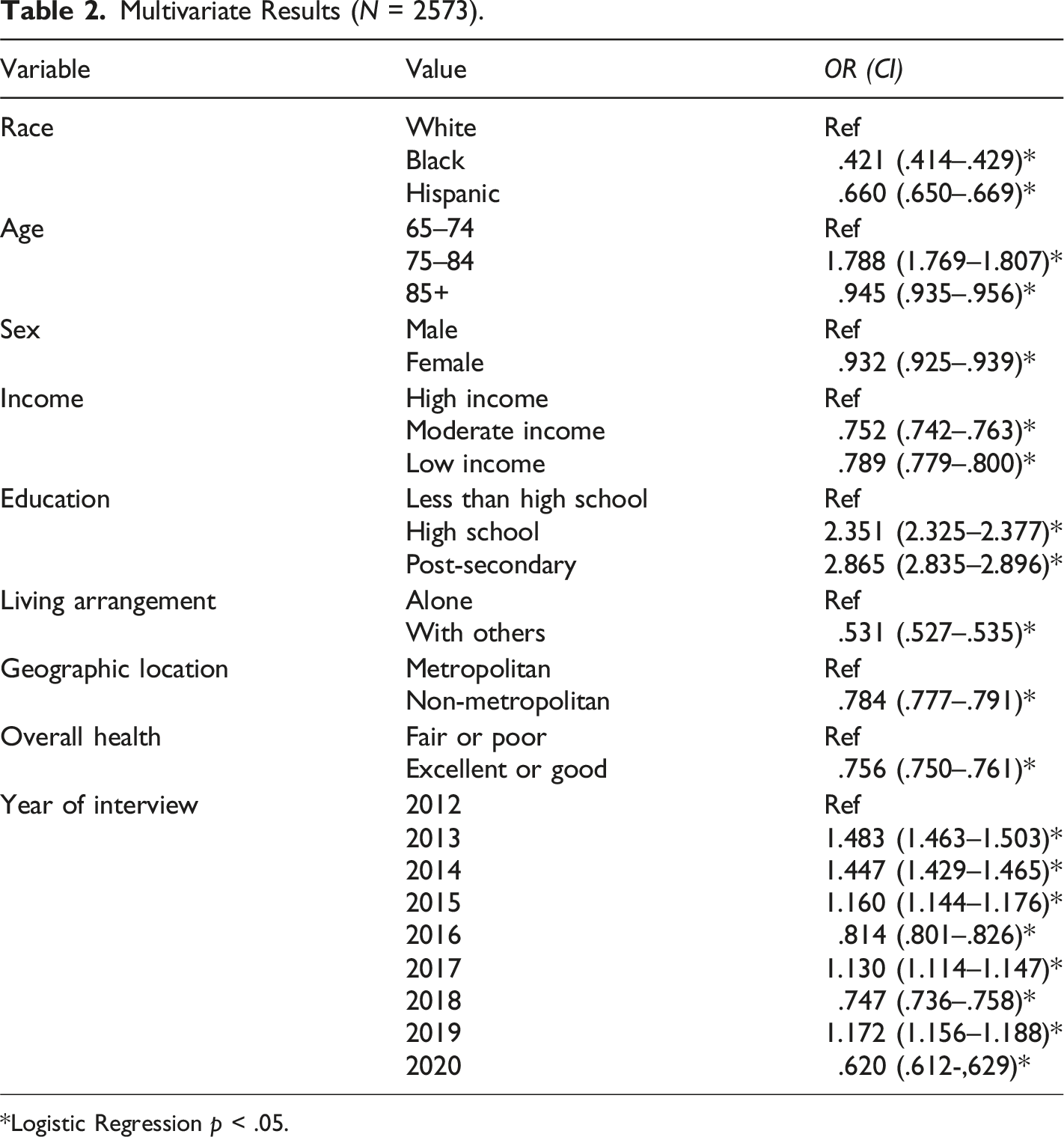
*Logistic Regression p < .05.
Discussion and Implications
The aim of this study was to determine racial/ethnic differences in provider-engaged religious belief discussions with older adults at the end of life. Results showed that health care providers were less likely to discuss religious beliefs with Black and Hispanic older adults compared to Whites. Although there aren’t many other studies with similar analyses, studies that have assessed the importance of religion at the end of life suggest that Black and Hispanic older adults do value religious beliefs in making end-of-life decisions (Gijsberts et al., 2019; Sharp et al., 2012; Zhang et al., 2012). For example, research shows that Black older adults are less likely to have hospice care at the end of life, less likely to have palliative care services, more likely to use aggressive/intensive care, more likely to have emergency room visits at the end of life, and more likely to die in a hospital (Karanth et al., 2018; Orlovic et al., 2018). While factors such as provider discrimination and structural barriers contributed to these noted differences, research also shows that personal preferences may be at play (Johnson, 2013). Black and Hispanic older adults often cite religious beliefs as the reasons why they pursue all treatment possible at the end of life, even though research shows that intensive/aggressive care is associated with lower quality of life at the end of life (Johnson, 2013). There is an emphasis on preserving life at all costs within several religious doctrines, and cultural values in both Hispanic and Black communities also view life preservation as the key priority (Choudry et al., 2018; Johnson, 2013).
Furthermore, prior research often presents lack of engagement in end-of-life services such as hospice care as a matter of ignorance among Black and Hispanic older adults, but research focused on cultural influences points to the importance of considering religious and cultural beliefs as key influencing factors in end-of-life decision-making (Johnson, 2013). To better understand the needs and preferences of Black and Hispanic older adults, providers must first understand how their cultural and religious backgrounds may influence their end-of-life choices (Givler et al., 2020). This is why several studies recommend that providers conduct psychosocial assessments with patients at first contact, asking questions about their religious and cultural background, including denomination, specific rituals/traditions, and needs for religious/spiritual support (Fang et al., 2016; Givler et al., 2020; Pentaris & Thomsen, 2020). Understanding religious beliefs allows providers to incorporate a patient’s needs and preferences into the care provided, which may improve overall treatment outcomes for the patient and increase satisfaction with care (Givler et al., 2020; Swihart et al., 2021). The topic of religion at the end of life is especially important in light of the COVID-19 pandemic, which restricted patients’ access to their religious communities and their overall support systems (Ting et al., 2021). As healthcare facilities continue to consider a patient’s needs at the end of life, the provision of religious/spiritual services is increasingly important, as the number of spiritual and/or religious persons continues to rise in the United States (Lipka & Gecewicz, 2021).
Although there is increasing acknowledgement of religion as an important factor at the end of life, research shows that most providers do not engage in such discussions with their patients (Givler et al., 2020). This study further shows that providers who do engage in religious belief discussions are more likely to have discussions with White older adults than Black and Hispanic older adults (Scherer et al., 2021). Research also shows that Black and Hispanic older adults often feel that they cannot communicate with their health providers due to cultural misunderstanding and a general mistrust in the healthcare system from years of racial/ethnic injustice in the United States (Johnson, 2013; Johnson et al., 2016). As such, providers are essential in starting/engaging such conversations with patients, so that they can better understand their end-of-life needs (Givler et al., 2020). The results of this study indicate that there may be a bias in how providers choose to communicate with patients, prioritizing engagement with White older adults over Blacks and Hispanics. This, in turn, affects quality of life at the end of life for Black and Hispanic older adults, who may be denied the opportunity to the receive religious/spiritual support that is of great importance to them.
Implications
In considering the implications of this study, it is crucial to recognize that several factors influence the lack of communication between patients and providers. First, Black and Hispanic older adults themselves are often not comfortable enough to bring up their religious/spiritual needs to providers, so providers must be intentional in engaging in those conversations (Givler et al., 2020; Johnson et al., 2016). Second, providers may be unaware of the importance of religion at the end of life for Black and Hispanic older adults because cultural humility training often neglects to include religion as a critical part of both Hispanic and Black culture (Givler et al., 2020). In the antebellum era, for example, religion was often a safe haven for enslaved Blacks, who relied on religious communities for support and comfort in difficult times. Since then, churches have remained a key source of support for Blacks (Scheirer et al., 2017). For Hispanics, religion may also be a safe haven in the United States due to the difficulties associated with immigration and assimilation. Research shows that two-thirds of Hispanic worshippers attend churches with Hispanic clergies, where services are conducted in Spanish, and most congregation members are also Hispanic (Pew Research Center, 2007). In a country where English is dominant, religious services may be a place of comfort and community for Hispanics. Cultural humility training in all medical settings should include an in-depth history of religion for Blacks and Hispanics, and how religion influences cultural traditions in both communities. Having the historical context would aid providers in supporting and adhering to the needs of Black and Hispanic older adults at the end of life. One critical study found that faith-based interventions successfully increased the use of hospice services and engagement in advance care planning among Black and Hispanic older adults (Catlett & Campbell, 2021). With a greater understanding of the role of faith in Black and Hispanic communities, providers may be better positioned to ensure that Black and Hispanic older adults have a greater quality of life in their final months of life.
Limitations
This study has limitations that should be taken into account when interpreting the results. First, the study was cross-sectional in nature, limiting the ability to establish cause and effect. Second, the respondents for the study were proxies and not the decedents themselves, which may result in inaccurate answers. The use of proxies also led to several cases of missing data, as respondents had the option to answer, “don’t know” or “refused.” Furthermore, the last-month-of-life interviews are conducted during the survey period of the NHATS, which creates variation in time since death among proxies, and may affect their ability to recall events at the end of life. Third, there were no data available on the profile of the providers, which may have provided further insight into the reasons for engaging or not engaging patients in religious belief discussions. Fourth, the religious belief discussion variable only asked if such a discussion occurred, without additional context as to why providers chose to initiate those conversations. Without such context, it is unclear whether providers deliberately avoided those conversations, or if they were unable to have those conversations (e.g., due to an unconscious patient). Finally, the results of the study were purely quantitative, and qualitative interviews may have provided greater insight into the nature of conversations about religious beliefs between providers and patients at the end of life. While this study does provide the initial foundation for the consideration of racial differences in religious belief discussions at the end of life, the sample was restricted to the United States, and is therefore limited in its generalizability to other countries and contexts.
Conclusion
This study aimed to determine racial/ethnic differences in provider-engaged religious belief discussion. Results showed that providers were less likely to have religious belief discussions with Black and Hispanic older adults compared to Whites. While research evidence shows that religion is more important to Blacks and Hispanics at the end of life, providers may be unaware of the relationship between religion, culture, and end-of-life decisions. As such, cultural humility trainings in medical settings should include an account of the historical value of religion in Black and Hispanic communities, and how religious/spiritual beliefs affect end-of-life decision making. Providers should also be encouraged to assess religious preferences with patients and should make active effort to provide religious/spiritual support to all patients regardless of race/ethnicity. Future studies should include profile information about providers and test the impact of religious cultural humility training on provider engagement with patients at the end of life.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.