
Abstract
Bereavement professionals who keep up with current research have wisely discarded the “five stages of grief” theory in favor of more contemporary, more functional models, including continuing bonds, tasks of grieving, meaning-reconstruction, the six Rs of mourning, and the dual-process model. But the stage theory has stubbornly persisted, despite a steady stream of criticism in academia and countless commentaries on the dangers of using it in bereavement counseling. Public support and pockets of professional endorsement for the stages continues to exist, undeterred by the knowledge that there is very little, if any, evidence to support its usefulness. Because there is a tendency for the general public to embrace ideas popularized in mainstream media, the stage theory clings tenaciously to public acceptance.
By now, most bereavement professionals know that the five stages of grief theory originated by Elizabeth Kubler-Ross (EKR) in her 1969 book, On Death and Dying is not a viable model for assessing or treating bereaved individuals. Stroebe, Schut and Boerner boldly declared that the theory “should be discarded by all concerned (including bereaved persons themselves); at best, it should be relegated to the realms of history” (2017, p. 456). A quintessential summary of the stage theory’s flaws can be seen in Kastenbaum’s astute analysis (Kastenbaum, 2012, p. 131): (a) The existence of these stages as such has not been demonstrated. (b) No evidence has been presented that people actually do move from Stage 1 through Stage 5. (c) The limitations of the method have not been acknowledged. (d) The line is blurred between description and prescription. (e) The totality of the person’s life is neglected in favor of the supposed stages of dying. (f) The resources, pressures, and characteristics of the immediate environment, which can make a tremendous difference, are not taken into account.
Those of us who keep up with current research have indeed discarded the stages, working instead with more contemporary, more functional models, including continuing bonds (Klass & Steffen, 2018), tasks of grieving (Worden, 2018), meaning-reconstruction (Neimeyer & Sands, 2011), the six Rs of mourning (Rando, 1993), and Stroebe and Schut’s dual-process model (1999).
But the stage theory has stubbornly persisted, despite a steady stream of criticism in academia and countless commentaries on the dangers of using it in bereavement counseling (Stroebe et al., 2017, p. 458–459). Public support and pockets of professional endorsement for the stages continues to exist, undeterred by the knowledge that there is very little, if any, evidence to support its usefulness. Because there is a tendency for the general public to embrace ideas popularized in mainstream media, the stage theory clings tenaciously to public acceptance (McLean et al., 2022, p. 1415).
After the first round of success for On Death and Dying, the stage approach received an extra promotional boost in 1995 when EKR collaborated with David Kessler (who is not an academic or a mental health professional) to produce a spin-off book called On Grief and Grieving (Kubler-Ross & Kessler, 2005). While the stages were originally intended to represent the responses of terminally ill people facing their own deaths, the EKR/Kessler alliance launched the idea that the stages should also be applied to the process of grieving.
Despite widespread criticism, Kessler stands firmly behind this theory, and reaffirms it frequently. In a 2017 Huffpost article he stated, “We taught that these same stages were shown to be present in all loss—whether it is death, divorce, moving or changing jobs. I apply those stages to my work in all of these areas today” (Kessler, 2017). In Konigsberg’s 2007 interview with Kessler, he claims that he’d once suggested to EKR that the term “response” might be more accurate than “stage,” but at that point, said Kessler, “the stages were so ingrained in the culture, so prevalent in our society, that there was no pulling them back” (2011, p. 69).
It’s not difficult to understand his reasoning. The EKR/Kessler brand was not only firmly established, it was also extremely lucrative. So much so, that despite decades of skepticism about the stages, Kessler further solidified his position in 2020 by publishing a new book subtitled “The Sixth Stage of Grief.”
An Example From Hospice Care
As an example of how insidious and persistent the grief stage theory can be, as a hospice chaplain who regularly evaluates the bereavement needs of individuals and families, I am confronted daily with documentation software that requires me to discuss the stages of grief with our clients (Figure 1). Problem statements—interventions and Goals Report (2020).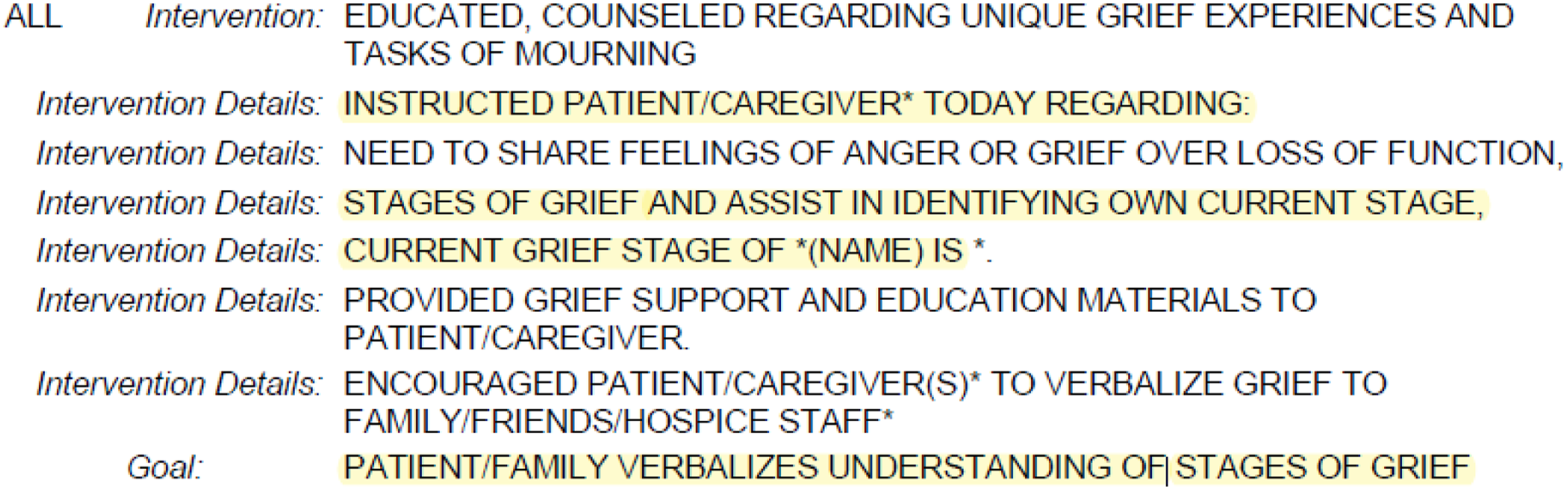
The software interface consists primarily of pull-down lists and checkboxes with a selection of auto-populated replies, all of which require answers before moving to the next screen. When all the boxes are checked, the answers form the foundation of the client’s specific care plan. Most of the questions are reasonably relevant, and in some places, we can enter a narrative note in our own words (though these notes are not part of the care plan calculation). It’s an unwieldy format, and it’s frustrating for clinicians, but for the most part, it’s tolerable.
With one glaring exception.
In the bereavement assessment section, it asks us to verify that we’ve completed the following interventions:
“Instructed patient/caregiver regarding stages of grief, and assist in identifying their own current stage.”
“Current grief stage of (name) is __________________.”
The final checkbox in that list confirms that this goal has been met:
“Patient/family verbalizes understanding of stages of grief.”
In an email conversation I had about this with one of our hospice executives, she indicated that she was well aware of the problem, and that she shares the frustrations of the clinical staff: HCHB [the software] has not changed the stages of grief language in those sections in many years. Here’s the rub, most social workers, chaplains, etc. are not grief experts, so they still default to Kubler-Ross instead of the prevailing theory for bereavement plans of care. We have made multiple pitches to change the software, and since we could not, we changed it within other sections where we had some control. HCHB has been promising a change, and next year we are hoping to finally get it (Zatulovsky, personal communication, Oct. 31, 2022).
Examples From Other Industries and Disciplines
In addition to encountering grief stage theory in clinical settings like the one illustrated above, we find it utilized in almost every corner of our culture, from art to technology. A few examples: A 2017 study on how employees adapt to changes in the workplace tracks their responses “along the stages of grief from initial denial to final acceptance” (Friedrich & Wüstenhagen, 2017, para. 5). In the practice of law, a study explored how 3-D printing might pose a threat to patent-holders, and uses the stages to show how those individuals adjust to the threat. The authors refer to this as “the five stages of patent grief” (Syzdek, 2015). In addiction recovery, the stages of grief have been used to explore the process of attachment adaptation (Chambers & Wallingford, 2017, p. 454). In medical school, the five stages have been applied to the way medical residents respond to working extremely long hours (Barone & Ivy, 2004, para. 1). The stages have been used to track how health care workers come to accept the introduction of new electronic technology for documenting medical records (McAlearney et al., 2015, para 1). In art and design, one researcher laments that the stages have not been depicted adequately in visual form, and proposes that we need more visual art “that outlines all stages of the grieving process” (Rygh, 2018, p. 9). In feminist studies, the stages are proposed as a process experienced by women who are “coming to terms with living in bodies that do not comply with societal standards” (Courtney, 2008, p. 362).
Konigsberg gives numerous examples of how the five stages of grief have permeated society, from their appearance on popular television shows like The Simpsons and Grey’s Anatomy to news commentaries, corporate policies and literature (2011, p. 2). Konigsberg says, “The stages are so pervasive they that they have become axiomatic, divorced from the specific time and place of their origin” (2011, p. 3). In reference the stage theory, the first chapter of Konigsberg’s (2011) book, The Truth About Grief, is called “The Idea That Won’t Die.”
Alternatives and Solutions
In addition to my work as a hospice chaplain, I am also an instructor in thanatology programs at two universities, and teaching my students about the non-viability of grief stages is an important part of the curriculum. I start with a general history of what is now popularly known as “grief work,” beginning with Freud’s idea of hyper-remembering the lost person with the ultimate goal of cutting emotional ties to them (Clewell, 2004, p. 44). I then lead students up to current theories such as continuing bonds, in which we maintain those ties rather than severing them (Klass & Steffen, 2018, p. 4). Along the way, I insert my own theory about how that change came about… after China’s invasion of Tibet in 1950, Buddhist monks and their teachings migrated into the west, and Buddhist concepts of the afterlife began to seep into western thinking, which paved the way for the idea of continuing bonds (but that’s a subject for another paper).
My students are all-too familiar with the stage theory, and are fascinated when they begin exploring its critiques. Interestingly, EKR herself admitted that they are not necessarily stages, but can be seen as “defense mechanisms in psychiatric terms, coping mechanisms to deal with extremely difficult situations” (Kubler-Ross, 1969, p. 122).
Clearly, she knew the difference between a stage and a response. In the anecdotal research she conducted for her book, she simply isolated the five most common responses that she encountered in her interviews with dying patients, and called them “stages.” Those five responses—denial, anger, bargaining, depression, and acceptance – are certainly common, and a griever could potentially experience all, some, or none of them. But what stage theory fails to recognize is the vast constellation of additional – and equally common – responses, which may (or may not) include any of EKR’s top five, and may actually be more affirming than distressing.
Is Intense Distress Necessary?
EKR’s five stages tip the scales in favor of distress, and don’t leave much room for positive emotions (other than perhaps “acceptance,” which could be interpreted as merely a form of passive resignation). Language that suggests healing, hope, restoration and reconstruction is glaringly absent. Also missing from the stage formula is any acknowledgement of resilience.
According to the American Psychological Association (2011), there are specific characteristics and intrapsychic resources that can contribute to one’s capacity for resilience. These include the ability to make decisions and take action, skill in communication, and an understanding that change is a natural part of human life. Additionally, cultural influences and religious beliefs have a powerful impact on how we respond to loss. A belief in divine punishment for example, can exacerbate guilt as a grief response (Bonanno, 2008, p. 98, Pattison, 2000, p. 190), while at the same time, some forms of spiritual coping can be helpful in the meaning-making process (Lichtenthal et al., 2011. p. 116).
Wortman and Boerner talk about how the expectation of intense distress has been a hallmark of classic bereavement theories for decades, with the assumption that a griever who does not express deep sorrow or become depressed may be having a maladaptive response (2011, p. 290). In their paper on “The Myths of Coping with Loss,” Wortman and Silver observed that “a complex mixture of biased input and interpretation of data by outsiders… as well as limited opportunity for open communication between parties, has led to a perpetuation of unrealistic assumptions about the normal process of coping with loss.” (1989, p. 355). These assumptions include the belief that intense distress is inevitable, and that a lack of distress is problematic (p. 354). They pointed out that the belief in required distress is so pervasive that when it’s absent in a griever, it is assumed that the person is in denial or incapable of forming healthy attachments (p. 350).
Bonanno cautions us to bear in mind that many people who experience loss and trauma can still have positive emotions without extreme distress or major disruptions in normal functioning. He reminds us that most of the information we have about how adults cope with loss comes from people who have sought treatment due to high levels of distress, and because resilient responses are not recorded as frequently, they are often viewed as outside the norm (2008, p. 101). Similarly, Janoff- Bulman observed that because the majority of information we have about trauma and loss responses comes from people who have sought professional help, it could follow that those who have fewer problems are under-represented (1992, p. 170).
A 2022 study by McLean, et all examined the lay public’s perception of grief responses, and found that symptoms of prolonged grief disorder (intense, enduring sorrow, loss of sense of self), and responses that match the five stages of grief were perceived as “most normal,” while adaptive responses (continuing bonds, meaning-making, post-traumatic growth) were perceived as the “least normal.” These findings suggest the possibility that individuals may strive to match cultural expectations of mourning behavior (2022, p. 1419). The authors conclude that there is a gap between the way people actually adjust to loss and societal expectations for how they are expected to behave. This could potentially result in a resilient griever experiencing disapproval and receiving less social support (p. 1414). Conversely, even though there is a prevailing expectation that intense grief reactions are socially acceptable, McLean et al. (2022) also found that individuals with intense grief reactions may also be stigmatized (p. 1416).
Anybody who has worked with grieving individuals has observed a far-reaching range of responses that exist on a spectrum from extreme distress and dysfunction on one end, to relief and serenity on the other. Here are just a few selected examples of responses that go beyond the five stages, and can be applied to someone facing their own death as well as someone grieving a loss of any kind: Shock, numbness, disbelief Avoidance Isolation Regression Stoicism Distancing Guilt/regret/shame Blame Resentment Obsession/perseveration Fear/anxiety/dread Equanimity Relief Anticipation/exhilaration Curiosity Gratitude Optimism Increase in social engagement Finding new strengths Freedom from an oppressive relationship Accepting impermanence Spiritual expansion (or rejection of toxic religious beliefs)
Four Case Examples
So how do we break the stage habit? How can we best support grievers who are restrained by the belief that their grief should align with only five possible responses, or that grief should be characterized by intense distress and prolonged suffering?
Following are four anecdotal examples from my chaplaincy and counseling experience demonstrating different ways of identifying loss responses that don’t fit neatly into the stage theory box.
Example 1 – Non-Death Loss
Tammy is a 42 year-old advertising executive who has experienced numerous wins and losses throughout her adult life. She’s divorced, financially independent, and has an 11 year-old son. She describes herself as a “workaholic” and also a “serial monogamist,” so she reflects on her past losses primarily in terms of her career (loss of jobs or projects/financial setbacks), and her personal relationships (friendships or romances that have ended). In counseling, Tammy discovered that she habitually reacts to losses according to this pattern: Shock – How could this happen? It doesn’t make sense. Blame – It’s someone’s fault. Righteous indignation – I have been wronged. Anger – Directed at the blamed party Woundedness – Feeling injured, attacked, victimized, disrespected Shame/Self-Loathing - I’m a failure Everybody hates me Obsession/perseveration – Constant thinking/talking about it Intellectualization – Searching for logic and rational conclusions Taking action – Seeking resources, reconstructing, rebuilding
Tammy noticed that she tends to move sequentially from one of these responses to the next in the course of coping with a loss. With the exception of anger, none of EKR’s stages are present, but there are plenty of other responses and emotions. For Tammy, going through each of these responses in order has proven to be a predictable pattern, so she refers to this as her own “personal grief stages.”
Example 2 – Expected Death
Brianna was the primary caregiver for her mother Anna, who struggled with dementia and various medical conditions for years before her death. While Brianna experienced anticipatory grief as she slowly lost the mother she knew, her response to the dementia diagnosis was not a surprise, because she’d been painfully aware of the symptoms for quite a while. When asked if she experienced any of EKR’s stages of grief, she replied: I went straight to acceptance. It was a relief to finally understand what was happening, and the diagnosis helped me figure out what to do. There was nothing to bargain about, and because I’m a very action-oriented person, I didn’t have the luxury of sinking into depression. I just jumped in and did what had to be done.”
1
Eventually Anna needed more care than Brianna could provide, and she was moved to a memory care facility, where Brianna visited almost every day. After Anna’s death, Brianna again went straight to acceptance, and also experienced relief and a sense of peace because her mother’s suffering had ended, and so had the tasks of caregiving. Brianna inherited money and property from her mother’s estate, and she was excited about having financial stability, while also experiencing guilt for feeling relieved and hopeful.
Example 3 – Traumatic Death
Randall and his wife Sarah lost their 9 year-old son via drowning in their backyard pool. Overwhelmed with guilt and self-blame, the couple scoffs at the idea that they could possibly have passed through stages such as denial or bargaining. “I saw my child’s dead body,” said Sarah. “How do you deny that? I buried him in a grave. Who do you bargain with for that?”
Randall adds: Was I angry? Absolutely. But at whom, or what? And what was there to bargain for? My son died; there’s no negotiating or coming back from that. Was I depressed? Of course, but what does depression look like exactly? Sure, I cried for months. I still do. I always will. I wanted to hide from the world because I couldn’t bear to see people living normal lives. I couldn’t stand to go to the grocery store, or drive through our neighborhood and see my son’s school on the corner. And yes, I felt that I should have died instead of him, and I wished that I could be dead rather than feel this pain. Could a therapist have diagnosed with clinical depression? I don’t know. Probably. I just know that the term ‘depression’ doesn’t come close describing what this feels like. That term is a joke.”
Example 4: Relinquishment Loss
Rudy is a 63 year-old man who loves to cook, and had a 25-year habit of daily wine drinking connected to the preparation and enjoyment of meals and hosting lavish dinner parties for his friends. He’d have his first one or two glasses while cooking dinner, and then another two or three with his meal, which amounted to essentially a full bottle of wine every evening. Although this habit had never presented a problem in terms of behavior or dangerous activities (such as driving), when he developed gout and high blood sugar, he knew it was time to quit. Rudy sees his journey as perfect fit with the five stages: There was a lot of denial. I knew drinking a whole bottle of wine every day for 20+ years was too much, but it wasn’t causing any harm, and it didn’t even make me drunk, so it was fine. When I got the lab results, I got angry at the doctor and at the unfairness of it all. And I definitely did the bargaining thing. I thought I could cut down my consumption and drink more water, but that didn’t work; it had to be all or nothing. So then, because I was giving up one of my greatest pleasures in life, I got depressed, missing this beloved thing that I was losing. I couldn’t picture my life without it, like there was no joy left. Eventually, over time, I surrendered to it, so now I guess I’m in acceptance.”
Although Rudy sees his experience in terms of the five stages, there were many other responses that occurred between the lines. He felt guilt for the harm he’d done to his body, shame for not having the strength to quit, anxiety and dread as he faced the daunting task of quitting, and a loss of interest in social engagement as parties and dinners with friends lost their appeal. At the same time, he also experienced excitement/anticipation about what the future might look like as he lost weight and gained energy.
A Dual Process Exercise
Strobe and Schut’s “dual process model” (DPM) recognizes how bereaved individuals engage in coping with a loss while also making adjustments in their lives to adapt to that loss. In this dual process model, the griever’s energy is constantly oscillating back and forth between “loss orientation” (LO) and “restoration orientation” (RO) (2010, p. 57).
When I teach my thanatology and chaplaincy students about the DPM, and when I talk about it with bereavement clients, I offer them a simple little exercise to help track their own oscillation movements between LO and RO. I present this as a tool that helps to keep energy from stagnating and becoming calcified in too much loss or too much restoration. The goal is for the griever to tend both gardens while becoming aware of the constant energetic shifting between the two.
To do this, I ask them to create a “Loss and Restoration Tracking Sheet” (Figure 2), in which they track their movements throughout any given day, week, month or year. It’s a simple journaling-style process in which a sheet of paper is divided into two vertical columns, one for loss and one for restoration. Through the day or week (or month or year), the griever enters notes about what they are experiencing, in either the loss or restoration column. This gives them a visual snapshot of where their energy is going at any given time. Loss and restoration tracking sheet sample.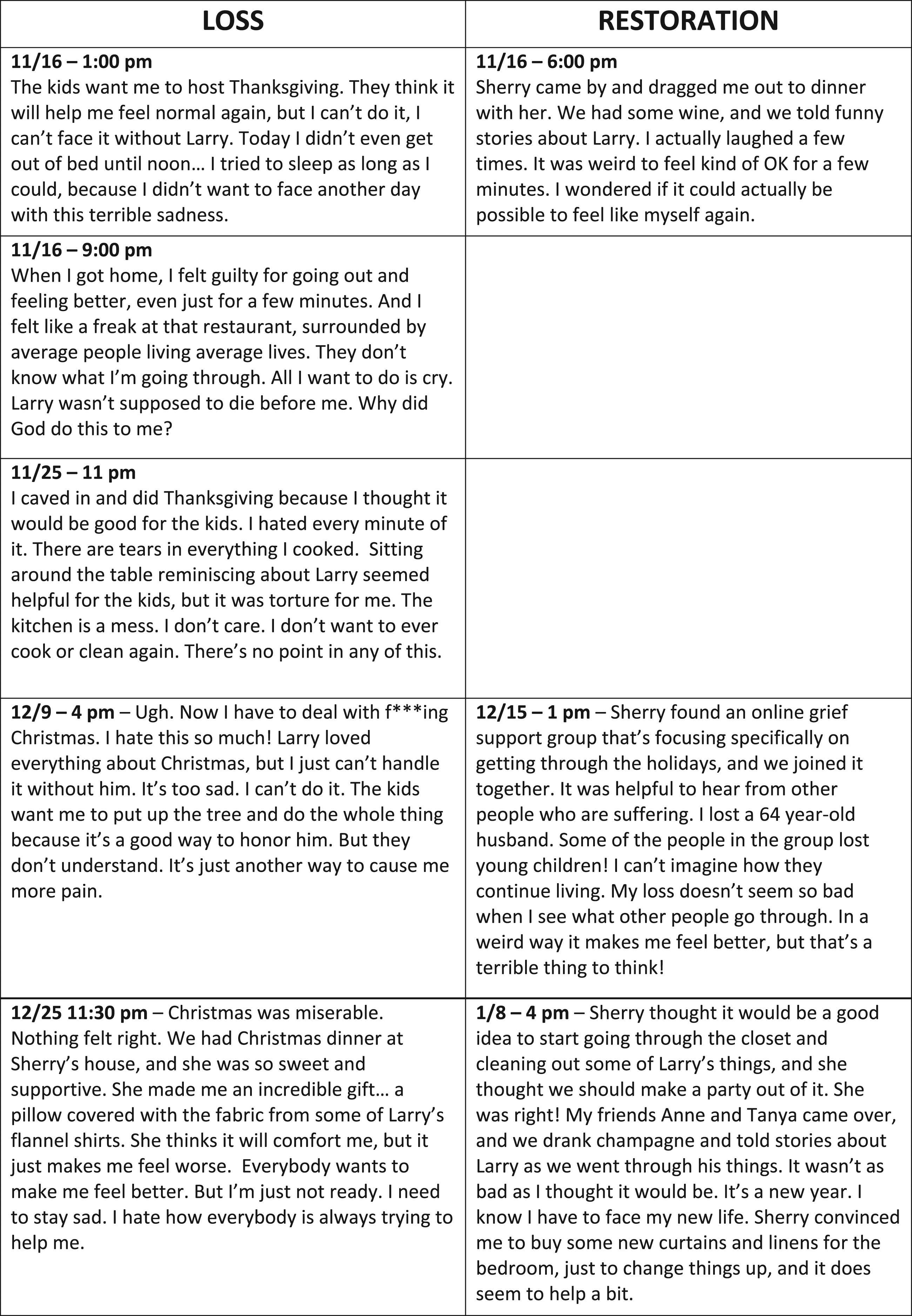
In this sample, 58 year-old Laura is grieving the death of her husband Larry, who died unexpectedly 3 months ago from a traumatic brain injury after falling down a flight of stairs. Laura has two adult children, and is particularly close to her 31 year-old daughter Sherry, who lives nearby.
These entries were made during the holiday season, which can be especially difficult for bereaved individuals (Daniel, 2017):
When Strobe and Schut first published their DPM theory in 1999, they said, “Confrontation with the reality of loss is the essence of adaptive grieving. It needs to be done, the cognitive business needs to be undertaken, but not relentlessly, and not at the expense of attending to other tasks that are concomitant with loss” (Stroebe & Schut, 1999).
This tracking sheet shows Laura’s movements between LO and RO, and how those movements have an ever-changing, organically shifting life of their own. They allow for the addressing of multiple tasks of grieving (Worden, 2018, p. 42–53), and give Laura a chance to become intimately familiar with her own unique grief fingerprint. As Carr explains: One of the greatest strengths of the DPM model is that it allows for individual-level agency and innovation. Unlike classic “stage theories” of grief, which assume that bereaved persons proceed through a series of stages in lock-step fashion… the DPM model allows that there are multiple paths to adjustment, and that individuals will oscillate between LO and RO coping based on one’s own needs and demands (2010, p. 376).
Conclusion
The five stages of grief are not likely to go away any time soon. And now, with the popularity of Kessler’s sixth stage, along with the online workshops he’s offering to “certify” people as “grief educators” (Grief Educator Certification with, 2022), the theory is becoming even more embedded in pop culture.
Thankfully, academic research is doing an admirable job of countering that trend, making it easier to recognize a myriad of responses to loss. But it will be an uphill battle as long as the stage theory continues to receive publicity. Corr has this to say about how the marketing machine contributes to the problem: One way to help move people beyond the five stages, misunderstood or not, would be to stop writing about them and to avoid giving them what appears to be great prominence in a book published 45 years after they were first presented (2015, p. 228)
Corr made that comment in 2015, and it is now 2022. The 45 years he refers to is now 53 years… and counting.
The stage theory is so ingrained in the public mind that it has generated a sort of complacency, in which one believes something to be true just because it has been promulgated so heavily for so long. This interpretation came to my attention via a comment from an attendee at one of my workshops, who felt that since so many people are familiar with stage theory, it should be accepted, regardless of what the research suggests.
Choosing pop psychology over evidence-based research is not an advisable position to take when trying to help an extremely vulnerable population, and this person’s comment begs the question… is the next generation of grief counselors going to have the same attitude, simply because the theory is popular? The individual who made this comment was a professional who has the benefit of solid academic resources readily available. But countless others are marketing themselves as “certified grief educators,” based solely on David Kessler’s online workshops. And they will likely continue to perpetrate the stage myth.
The importance of familiarity with a wider range of responses to loss cannot be overstated. In simple terms, the benefit of moving beyond the stages is clear… our interactions with the bereaved would be “less judgmental and more facilitative of their healing and growth” (Wortman & Boerner, 2011, p. 317).
Our task now, as counselors, teachers and researchers, is to work toward unifying traditional bereavement research that focuses on the painful aspects of grieving with strategies of “resilience psychology” (Hone & Reivich, 2017, p. 33–34). and the affirming experiences that promote healing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.