
Abstract
Introduction
Chronic renal (kidney) failure (CKD) is an important chronic disease that physically, psychologically, mentally and socially affects the individual. Its prevalence worldwide is 13.4% (11.7–15.1%). Hemodialysis (HD), peritoneal dialysis (PD) and kidney transplantation are applied for the treatment of CKD. The rates of HD, PD and kidney transplantation treatments are 76.1%, 4.7%, and 19.2%, respectively (Seyhani et al., 2018). Whatever treatment is applied, patients experience anxiety, stress (Durmuş & Ekinci, 2021), spiritual problems (Angın, 2021), deterioration in quality of life (L.Kimmel et al., 2021) starting from the first stage of their disease. It is stated that the anxiety experienced is actually death anxiety (Ghiasi et al., 2021; Hashemi et al., 2021; Hosseini et al., 2022; Khodarahimi et al., 2021; L. Kimmel et al., 2021). Both HD and PD patients experience this anxiety, and the dose of anxiety increases as the disease progresses (Nia et al., 2017).
Death has been a part of humanity since ancient times. With the meaning of death, “death anxiety” has also begun to be interpreted. Death anxiety is a feeling of worry or fear that is typically triggered by the thought of death. Death anxiety is wide-ranging. It can include death and separation from loved ones, suffering, being alone, worrying about being buried, spiritual concerns, etc. (Pollak, 1980; Templer, 1970). It is seen that death anxiety is very common in individuals with chronic diseases and this has a psychological origin (Bibi & Khalid, 2020). Death anxiety is among the psychological problems experienced by individuals with CKD, and it is argued that this should be reduced. To ensure this; applications such as psychotherapies (Khodarahimi et al., 2021; Saki et al., 2021), directing the patient to perceive the disease more positively (Soleimani et al., 2018), providing social support (Bibi & Khalid, 2020), strengthening of spirituality (Asadzandi, 2020; Durmuş & Ekinci, 2021; Hosseini et al., 2022), increasing psychological resilience through religious coping (Angın, 2021), praying (Gholami et al., 2020) are recommended. It is stated that anxiety can be reduced with moral support (Chen et al., 2021).
Spirituality is defined as “one’s experience of connecting with the essence of life, seeking connection with oneself, others, nature and divinity” (Steinhauser et al., 2017). The spiritual background of the individual (Asadzandi, 2020; Durmuş & Ekinci, 2021; Gholami et al., 2020; Hosseini et al., 2022), or religious perspective (Angın, 2021; Sağlam Demirkan, 2020) are the features that affect death anxiety and increase coping power. For this reason, it is recommended to strengthen the spirituality of individuals who experience death anxiety (Angın, 2021; Asadzandi, 2020; Durmuş & Ekinci, 2021; Gholami et al., 2020; Hosseini et al., 2022; Sağlam Demirkan, 2020). It is known that spirituality affects death anxiety in Muslim societies (Saleem & Saleem, 2020).
It is seen in the literature that; religious perspective ((Angın, 2021; Sağlam Demirkan, 2020), spiritual well-being (Asadzandi, 2020; Durmuş & Ekinci, 2021; Gholami et al., 2020; Hosseini et al., 2022), death anxiety (Asadzandi, 2020; Ghiasi et al., 2021; Hosseini et al., 2022; Nia et al., 2017; Saki et al., 2021; Soleimani et al., 2018) are studied in different groups of patients with chronic renal failure. In the study of Sağlam Demirkan (2020), it is recommended to investigate death anxiety and religious attitudes in patients with chronic renal failure (Sağlam Demirkan, 2020). The aim of this study was to determine the correlation between death anxiety and religious attitudes of patients receiving hemodialysis and peritoneal dialysis, and the factors that affect the death anxiety.
Method
It is a descriptive and correlational research.
Research questions: In hemodialysis and peritoneal dialysis patients; (1) What is the religious attitude status/level? (2) What is the level of death anxiety? (3) What are the factors affecting death anxiety? (4) Is there a relationship between religious attitude and death anxiety?
Universe and Study sample
The universe of the study consisted of patients followed by the Nephrology Clinic of XXX University Medical Faculty Hospital and receiving hemodialysis and peritoneal dialysis treatment in the same hospital.
Study sample
The data of a similar study was used in the study. In the aforementioned study, the death anxiety score of the spiritual care group and non-spiritual care group was 18.53 ± 10.49 and 31.28 ± 12.56 (p < 0.001) (Hosseini et al., 2022). According to these results, the sample size was calculated according to the difference between the scores of the two independent groups in the G*Power 3.1.9.4 package program. Since p < 0.001 was reported in the source article, the margin of error was taken as 0.001 in the calculation. According to this calculation; it was determined that the sample size should be at least 84 people, with a margin of error of 0.001 and a power of 0.99. Sample size was increased according to literature (Yıldırım Kaptanoğlu, 2013) and the study was completed with 105 individuals. The study includes: patients who are >18 years old, who continue to receive HD or PD treatments, who belong to the religion of Islam, who do not have a communication barrier, who are not in the process of cancer treatment. Being in the terminal period and having cognitive problems are exclusion criteria.
Data Collection Forms and Data Collection
Descriptive Characteristics Form, Religious Attitude Scale and Death Anxiety Scale were used to collect data.
Descriptive Characteristics Form
The characteristics features form was created by the researchers based on the literature (Durmuş & Ekinci, 2021; Gholami et al., 2020; Hosseini et al., 2022; Khodarahimi et al., 2021; L. Kimmel et al., 2021), and it consisted of twelve questions in total. Headings that make up the questions can be added (sociodemographic and disease characteristics, etc.)
The Ok-Religious Attitude Scale
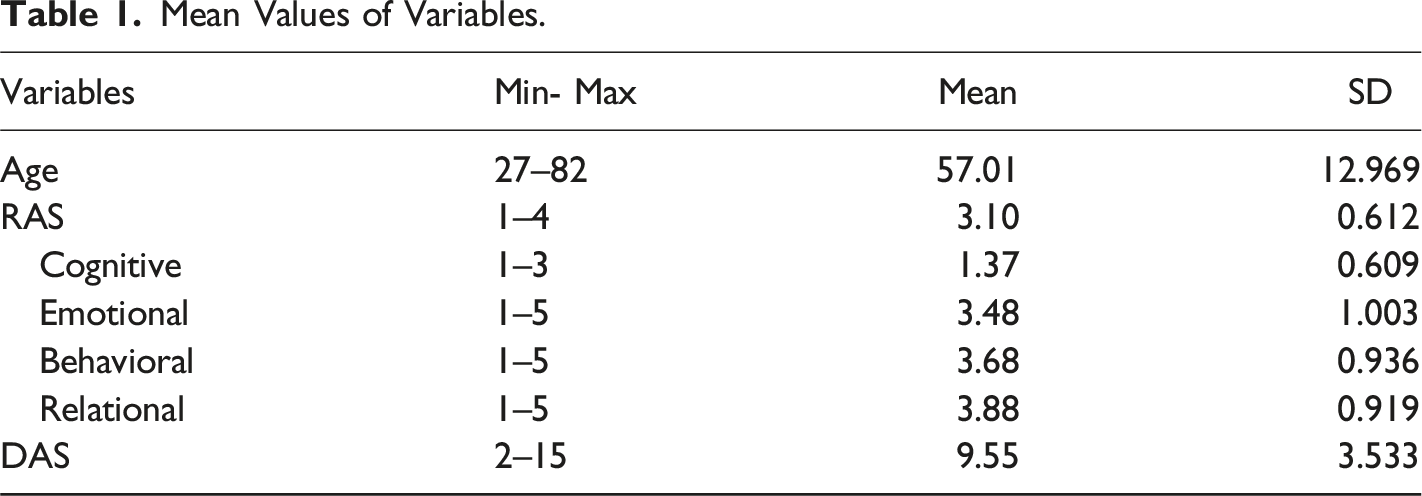
The scale was developed by Ok (2011) in order to assess religious attitudes for Muslim groups. There are four sub-dimensions (cognitive, emotional, behavioral, relational) in the eight-item scale. It is a five-point Likert scale. The items are coded as follows: strongly disagree (agree not at all) (1), slightly (a little) agree (2), fifty-fifty (half the time) agree (3), mostly (mainly) agree (4), completely agree (5). The first and second items are reverse scored. The scale is evaluated over the total score as follows; 1.00–1.49 = little or no religion at all, 1.50–2.49 = a little religious, 2.50–3.49 = moderately religious, 3.50–4.49 = highly religious, 4,50–5.00 = devoutly religious/strong believer. Although the Cronbach Alpha internal consistency reliability coefficient varies in the sub-dimensions (0.90–0.75), it is 0.90 for the whole scale (Ok, 2011; 2016). In this study, the Cronbach Alpha coefficient was 0.828.
Death Anxiety Scale
The scale was developed by Templer et al. (1970) to measure death anxiety (Templer, 1970). Re-examination of the scale, whose validity and reliability studies were carried out before, was performed by Akça and Köse (2008). The scale is a binary Likert type scale consisting of 15 items and answered as true or false. One point is given for the “correct” answers to 1, 4, 8, 9,10,11,12,13,14 questions and the “false” answer to the other questions. The highest score that can be obtained from the scale is 15. As the score obtained from the scale increases, the level of death anxiety increases. A total score of 8 and above indicates the presence of death anxiety in the individual. The Kuder Richardson-20 reliability coefficient of the Turkish scale is 0.75 (Akça & Köse, 2008). The Cronbach Alpha coefficient was 0.829 in this study.
Data collection
Data were collected face-to-face by the researchers during the periods when patients were in PD and HD units. During data collection, protective measures were taken for the risk of infection transmission. An explanation was given to the patients and their verbal/written consent was obtained.
Variables of the Study
Dependent variable
Death anxiety score
Independent variables
Religious attitude score, age, gender, type of dialysis treatment, duration of dialysis treatment, presence of other comorbidities, marital status, income level, education level, employment status.
Ethical Aspect of the Study
Research permission (2022/2195) was obtained from XXX University Health Sciences Scientific Research Ethics Committee, and application permission (E-14567952–900–190074) was obtained from XXX University Medical Faculty Hospital. In all stages of the study, the STROBE (Equador, 2019) checklist and the Declaration of Helsinki were followed.
Statistical Analysis
SPSS 25 (IBM) statistical program was used for statistics. The normality of the distributions was determined according to the Skewness-Kurtosis test result, the −1/+1 range was accepted (George, 2019).
It was shown that age, gender, presence of another disease, education level, duration of dialysis, employment status, income status RAS total, emotion, behavior, god sub-dimension scores, DAS total score is normally distributed, and other variables (type of dialysis, marital status, RAS cognition sub-dimension score) were not normally distributed. Sociodemographic data were analyzed by number, percentage, mean ± standard deviation. Independent Simple T test and One Way Anova were used in the analyzes for normally distributed variables, and Mann Whitney-U and Kruskal Wallis tests were used for non-normally distributed variables. Pearson and Spearman correlation analysis was used to compare the correlation. Correlations were evaluated as follows: r ≤ 0.25 very weak; 0.26 ≤ r ≤ 0.49 weak; 0.50 ≤ r ≤ 0.69 moderate; 0.70 ≤ r ≤ 0.89 strong; 0.90 ≤ r < 1 very strong. Linear Regression Analysis was performed for suitable variables.
Results
Mean Values of Variables.
Distribution of DAS Score According to Independent Variables (n: 105).
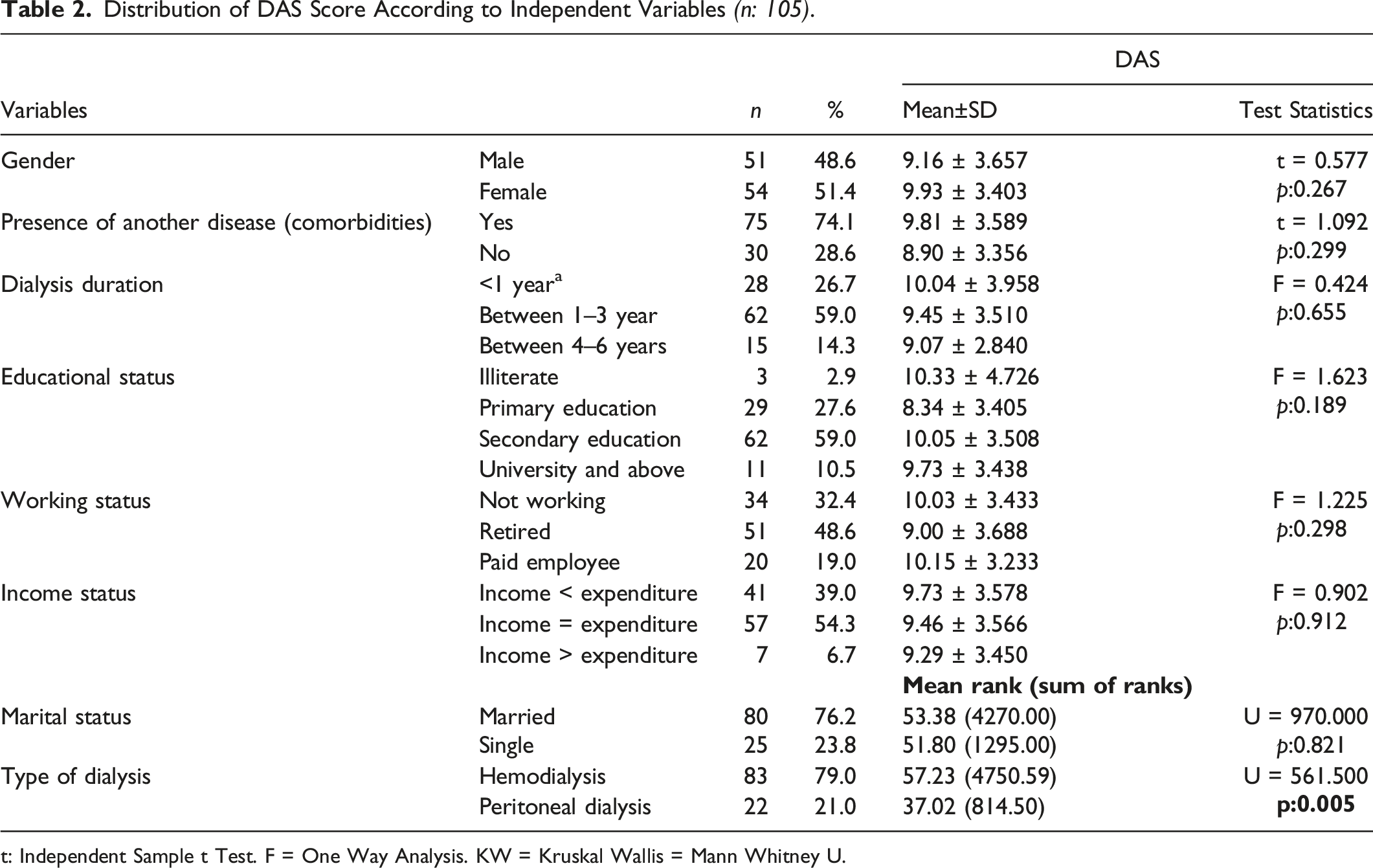
t: Independent Sample t Test. F = One Way Analysis. KW = Kruskal Wallis = Mann Whitney U.
Correlation between DAS and other Scale Scores and Age.
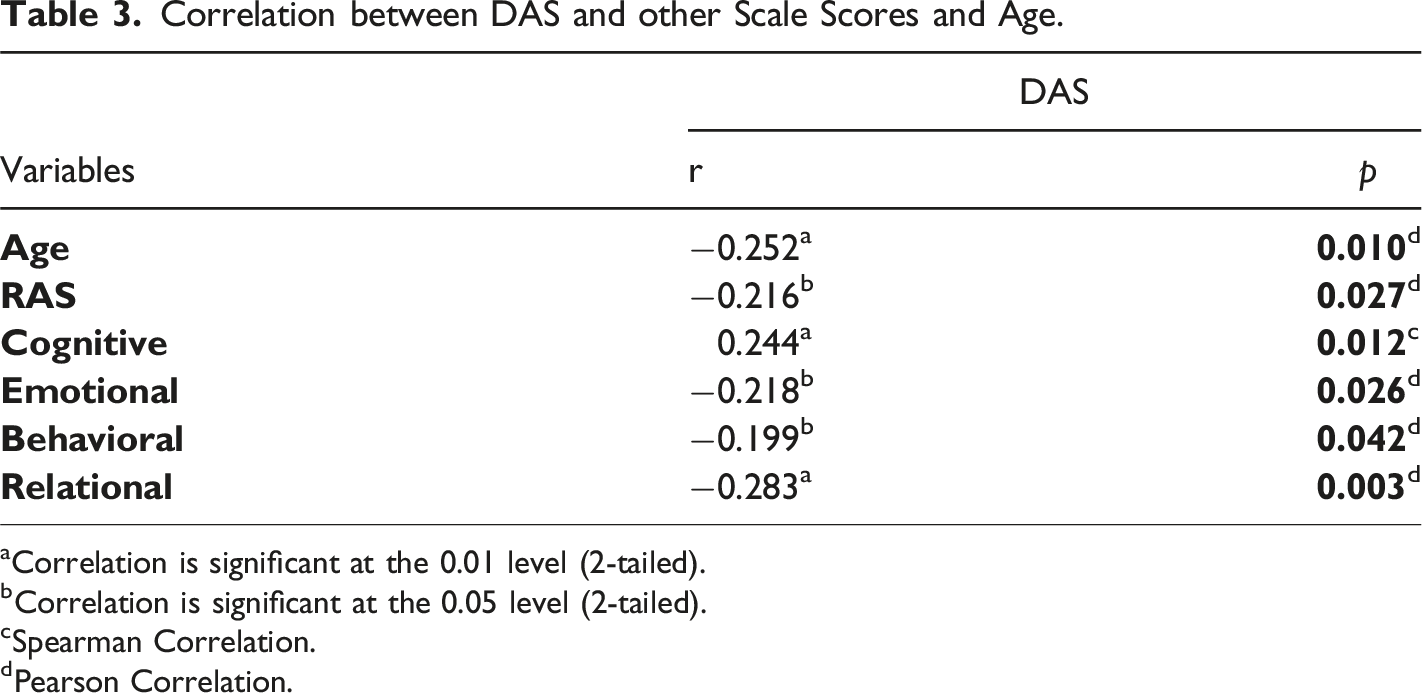
aCorrelation is significant at the 0.01 level (2-tailed).
bCorrelation is significant at the 0.05 level (2-tailed).
cSpearman Correlation.
dPearson Correlation.
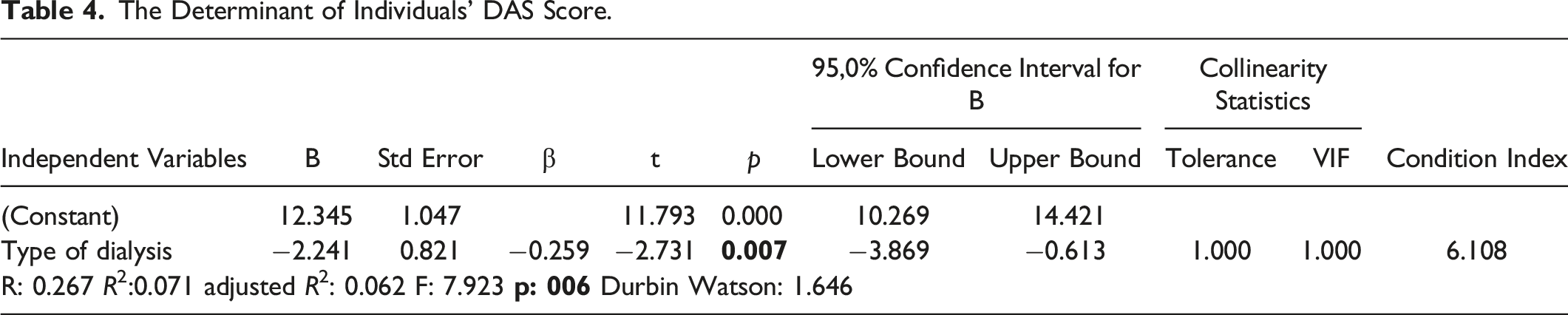
The Determinant of Individuals' DAS Score.
Discussion
In this study, it was aimed to determine the relationship between death anxiety and religious attitudes of patients receiving hemodialysis and peritoneal dialysis, and to determine the factors affecting this correlation, and to determine the differences between the two treatment groups. The results were discussed in the light of the literature.
In general, fear of death in patients with kidney failure is observed as “Fear of premature death”, “fear of sudden death” and “fear of dying”. Situations such as worsening of health conditions, having problems with vascular access, dietary restrictions, future anxiety, etc., increase the fear of these patients (Frontini et al., 2021). It has been stated that patients in the dialysis treatment process are emotional and depressed, which triggers their death anxiety (Dönmez et al., 2021). It has been reported that death anxiety is moderate in Muslim individuals (Gholami et al., 2020; Saleem & Saleem, 2020). One of the biggest problems causing death in PD patients is peritonitis. These patients are afraid of peritonitis and therefore dying (Tekkarışmaz & Torun, 2020). It was shown as a result of a study conducted in Jordan that having a deadly disease and the experiences during the disease process are accepted even if death anxiety increases (Othman et al., 2022). In this study, it was found that both HD and PD patients had death anxiety, but HD patients experienced more anxiety. It is possible for hemodialysis patients to continue dialysis 3 days a week, to stay away from their social environment in this process, to re-establish vascular access before each dialysis procedure, to experience pain, to have restrictions on nutrition and fluid intake, to be in the same environment with other patients, and to be adversely affected by poor patients. On the other hand, PD patients do not experience these negativities or experience them to a much lesser extent. This difference may affect death anxiety.
It is known that death anxiety is associated with age, and anxiety increases with age (Dadfar et al., 2018). It has been reported that age is the most important determinant of death anxiety in Iranian elderly adults with chronic diseases, and death anxiety decreases with age (Rezaei Aderyani et al., 2020). On the contrary; it has been reported that death anxiety increases with increasing age in patients who become ill during the COVID-19 process (Kandemir, 2020). Another study states that there is no correlation between age and death anxiety (Tepe, 2020). The fact that adults and individuals with chronic diseases use more drugs is a factor that increases the fear of death (Şanal Karahan & Hamarta, 2019). In this study, it was determined that the participants' fear of death increased with advancing age and increase in cognition. Individuals gain sufficient knowledge about their treatment over time. In this process, the age of individuals is advancing. It can be thought that this situation may support the reduction of death anxiety.
In Muslim societies, the presence of a chronic disease causes the individual to fear the experience of dying, while it is seen that individuals leave the situation to Allah’s discretion/surrender to Allah (Othman et al., 2022). An increase in surrender and spirituality can reduce dialysis patients' problems with psychological origins, such as pain (Nikmanesh & Azaraein, 2017). Emotion-focused coping methods are recommended for individuals to control stress (Kobra et al., 2015). One of the most common coping methods used by dialysis patients is religious coping (Mistik et al., 2016). Religion contributes to the patient’s ability to stay on dialysis longer and thus to the effectiveness of the treatment (Al Zaben et al., 2015). It has been stated that there is a negative correlation between religion and death anxiety (Saleem & Saleem, 2020). A study conducted in Tunisia showed that religious individuals have less death anxiety (Fekih-Romdhane et al., 2020). The outcome of a study of individuals with cancer in Pakistan was similar. Cancer patients who are religious experience less death anxiety (Abbas et al., 2022). Similar studies have shown that patients' religious practices (praying, etc.) increase their quality of life (Burlacu et al., 2019; Harbali & Koc, 2022). Studies carried out in countries with a large number of Muslims such as Philippines (Soriano & Calong, 2022) and Iran (Mina et al., 2018; Rezaei Aderyani et al., 2020), show that being religious affects death anxiety in a positive way. In general, it is explained that religion positively affects the anxiety caused by death, which is the basis of existence (Kandemir, 2020). Similar results were obtained in this study as well. Those who are religious have less death anxiety. Considering that the idea of surrendering to Allah is more intense in religious people among Muslim societies, and this supports the reduction of death anxiety, it can be said that the same condition is true for the Turkish population, which is mostly Muslim.
Conclusion
HD and PD patients have moderate religious attitudes and death anxiety. Death anxiety is higher in HD patients. There is a weak correlation between religious attitude and death anxiety. The most important result of this study is that with the increase in consciousness in dialysis patients, death anxiety decreases and HD treatment increases the fear of death.
Recommendations
It can be suggested that nurses who care for dialysis patients, should be aware of the role of religion in the lives of dialysis patients and its relationship with health outcomes, and it may be recommended to apply holistic care for these patients to express their feelings and their concerns about death. It should not be forgotten that anxiety is higher in HD patients, it may be appropriate to plan regular meetings with this patient group so that they can express their concerns and receive support from professionals who will provide moral support.
Limitations
The inclusion of patients treated in a single center in the sample and the collection of data during the Covid-19 process are the limitations of the research. Since the research was conducted with only one patient group in a hospital, it cannot represent the whole universe. It can only be generalized to the date and group of the study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.