
Abstract
Keywords
Background
Death and Death Anxiety
Death is an unavoidable fact that directly affects humanity. It is a terrifying and inescapable life situation that is often acknowledged as one of the most agonizing personal experiences that humans undergo. Usually, the death time is accompanied by high levels of physical and psychological distress. Death is defined as the depletion of respiratory and circulatory functioning, as well as the irreversible cessation of all brain operations or damage to brain stem functions (Sarbey, 2016). Individuals have two different kinds of death sentimental responses: they either refuse to accept death and are extremely stressed and worried regarding it, or they accept death passively (Langner, 2006). Death is perceived differently by different people depending on a variety of factors such as cultural background, self-awareness, and developmental stage (Abdel-Khalek, 2005).
Nurses and other health care providers habitually witness death as part of their professions, which could significantly raise their death anxiety as well as increase their awareness regarding their own mortality (Peters et al., 2013; Ek et al., 2014 & Nia et al., 2016). To illustrate, a previous research study showed that 68% of health care providers reported a high level of death anxiety (Moudi et al., 2017).
Death anxiety is commonly conceptualized as a feeling of insecurity, anxiety, and fear of death or nearly dying; it is correspondingly induced by death awareness and understanding and is frequently noticed among individuals who have been subjected to disease, trauma, aggression, or even death (Nia et al., 2016; Vance. 2014 and Lehto & Stein, 2009).
Death anxiety has been recognized as an obstacle while caring for end-of-life patients (Brown et al., 2014; Peters et al., 2013). As a result, death anxiety has a negative impact on health care providers' attitudes toward dying patients and death, as well as their emotional well-being, life satisfaction, and might indeed lead to suicidal thoughts (Gurdogan et al., 2019). Furthermore, death anxiety was substantially associated with a significant loss of self-confidence and recurrent avoidance behaviors during end-of-life care planning conferences with dying patients' close relatives; thereby, all of these negative consequences have a negative impact on attitudes toward caring for terminally ill patients, as well as causing a delay in end-of-life care planning (Clare et al., 2020).
High level of death anxiety has detrimental consequences. For instance, a previous cross-sectional research study was conducted to measure the level of death anxiety among nurses from different work environments using the Death Anxiety Scale and including 184 nurses. The results revealed a significant association between the level of death anxiety and the involvement in social interaction; the participants with a high level of death anxiety reported poor social interaction (Moudi et al., 2017). Also, a high positive association between fear of death level, and death avoidance was reported by a previous descriptive correlational cross-sectional study that collected data from Israelis 147 nurses (Braun et al., 2009).
Associated Factors Influence the Death Anxiety Level
Gender, age, length of experience, religious beliefs, personal experience with loss, and several other variables have a significant impact on the level of death anxiety, and the fear of death level. As a result, several research studies have been conducted in an attempt to anticipate these contributing factors. Multiple research studies have revealed that gender is highly associated with the level of death anxiety; for instance, a cross-sectional research study conducted by Abu Hasheesh et al. (2013) recruited 155 nurses from general hospitals in Jordan revealed that the female nurses had higher death anxiety levels than male participants. Correspondingly, a similar result was reported by a previous Turkish study conducted by Gurdogan et al. (2019) that collected data from 376 nursing students, the results indicated that the level of death anxiety varies between genders as female participants reported a higher level of death anxiety. However; In contrast, a study was conducted among medical students at the University of Cambridge demonstrated that there are no statistically significant variations in the level of death anxiety between males and females (Thiemann et al., 2015).
The length of experience with terminally ill patients, as well as frequent exposure to mortality significantly influence the death anxiety level. Numerous studies have been indeed indicated that the level of death anxiety significantly decreased among nurses and physicians with clinical experience, specifically at the palliative and hospice units (Xu et al., 2019; Halliday & Boughton, 2008; Mondragón-Sánchez et al., 2015 and Peters et al., 2013).
Religious beliefs have a significant effect on death anxiety and fear of death. A literature review was done previously by (Ellis et al.,2013) conclude that there is a significant negative association between religious beliefs and fear of death among people who asserted being at least modestly religious. Inconsistently, a similar conclusion was reported by (Xu et al., 2019), as nursing students who did not have religious beliefs scored a higher fear of death levels than participants who claimed that they have strong religious beliefs. Correspondingly, many other studies revealed that religion significantly influence the death anxiety level (Iranmanesh et al., 2008; Peters et al., 2013; Asadpour et al., 2016; Peterson et al., 2010; Arslan et al., 2014; Saleem and Saleem. 2020)
Terror Management Theory
Terror management theory is an interesting and one of the modern theories driven by Becker’s (1973) existential view of death. This theory has been offered out to explain the origin of ageism (TMT). TMT contends that culture and religion are human creations that give the world a meaning and structure. Furthermore, TMT’s underlying principle is that all people have an innate desire to survive and continue existing while also being aware of their impending mortality (Greenberg et al., 1995; Solomon et al., 1991). The hypothesis suggests that they will consciously feel a fear of dying as a result. The fear of annihilation, or ultimate nonexistence, lies at the heart of death fear. It includes the fear of having one’s body destroyed as well as having one’s mind, spirit, and soul destroyed. Without a way to keep such death fear from entering one’s awareness, these theories contend, the experience would be debilitating. Finding the elements contributing to this suppression’s maintenance is the theory’s key aim (Cicirelli, 2002).
Furthermore, according to the TMT researchers' “dual process hypothesis,” both conscious and unconscious fears of dying triggering a different defense mechanisms; “Proximal defenses” suppress thoughts of dying by rejecting one’s vulnerability. These defenses are triggered by a process known as Mortality Salience, which occurs when evidence of impending death is brought to the current attention (MT). When death-related knowledge is revealed, “distal defenses,” such as self-esteem and cultural worldviews, intervene to reduce fear of death. Self-esteem and belief in one’s cultural worldview are linked to symbolic systems that convey meaning, values, and the belief that one’s existence is portion of a greater enduring than oneself (Greenberg et al., 1995; Vess et al., 2009 & Cash, 2012).
In contexts of religiosity, according to TMT’s worldview defense hypothesis, there is a relation between religiosity and death anxiety. That is, death anxiety is considered to be significantly low among the religious individuals, while it is highest among the uncertain, leading to the assumption that the level of death anxiety decreases as religiosity increases, or vice versa (Greenberg et al., 1990 & Atmaca, 2021).
Study Aim
Up to the researcher’s search and knowledge, still there is a lack of literature regarding the death anxiety level among oncology nurses and physicians worldwide in general and in Jordan specifically, thus,
Methods
Design
A descriptive cross-sectional design was used to collect data and to assess the level of death anxiety among oncology nurses and physicians, and to determine the associated factors that influence their level of death anxiety.
Sample
A convenience sample of 200 oncology nurses and physicians working at one specialized cancer hospital in Jordan were recruited in this study. The participants invited via email to complete the online questionnaire designed by using Google Forms. The appropriate sample size was estimated using the G*power software version at small effect size, power of 0.80, alpha at 0.05 level of significance and two-tailed test; the minimum required sample size is around 200 participants.
Eligible nurses and physicians were recruited according to the following criteria: (1) Registered nurses or physical who completed a Bachelor’s degree program, (2) A full-time nurse or physicians working in the selected cancer hospital, (3) have a minimum of 1 year of experience as a direct care nurse, (4) Willing to participate in the study. The exclusion criteria for were (1) nurses or physicians who are working on paediatric oncology departments, and (2) Nurses and physicians in administrative positions since their position may result in less exposure for patients.
Data collection procedure
Before data collection, the researcher obtained ethical approval from the research and ethics committee/Institutional Review Board at the selected hospital
Instruments
The package of online data collection questionnaire includes demographic sheet data and Collett-Lester fear of death scale
Demographic Data sheet
Demographic variables were Age, gender, educational level, job profession (nurse or physician), length of experience, experienced death with close relative previously (Yes or No), exposure to death at the workplace (Yes or No), and if the participant attended educational courses regarding death and dying previously or not.
Collett-Lester Fear of Death Scale
It is a multidimensional instrument structured to measure four different dimensions. Thereby, this instrument aimed to measure the death anxiety level among oncology nurses and physicians. Collett-Lester fear of death scale consists of four subscales comprises 28 items (seven items for fear of death of others, seven items for fear of death of self, seven items fear of dying of others and seven items fear of dying of self), each statement rated from 1 to 5. The highest total score is 140. Furthermore, the cut-off point that indicates a low death anxiety level for each statement is less than two. In the current study, the researcher utilized the third version of this scale that had been published in the English language in 2003, which consists of 28 items distributed over four subscales
Ethical Considerations
Approval for this study was sought and obtained from the IRB committee at the included hospital. Also, Permission to use the instrument was obtained prior to data collection. The purpose of the study and the voluntary participation were mentioned clearly in online information sheet. No identifying information was collected to promote the participants' confidentiality. All data was saved on the principal investigator personal computer and the file kept locked with password and the principal investigator having sole access.
Data Analysis
Data were entered and analyzed using SPSS 26.0. Collett-Lester fear of death scale followed normal distribution and met the assumption of homoscedasticity parametric tests were used to analyze. Descriptive statistics (frequency, means, and standard deviations) were calculated for sample characteristics and the mean scores of Collett-Lester fear of death scale. The differences in nurses’ and physicians' based on their demographic variables were examined using the Independent samples t-test and the One-way ANOVA test; post hoc analysis was conducted by Tukey HSD test.
Result
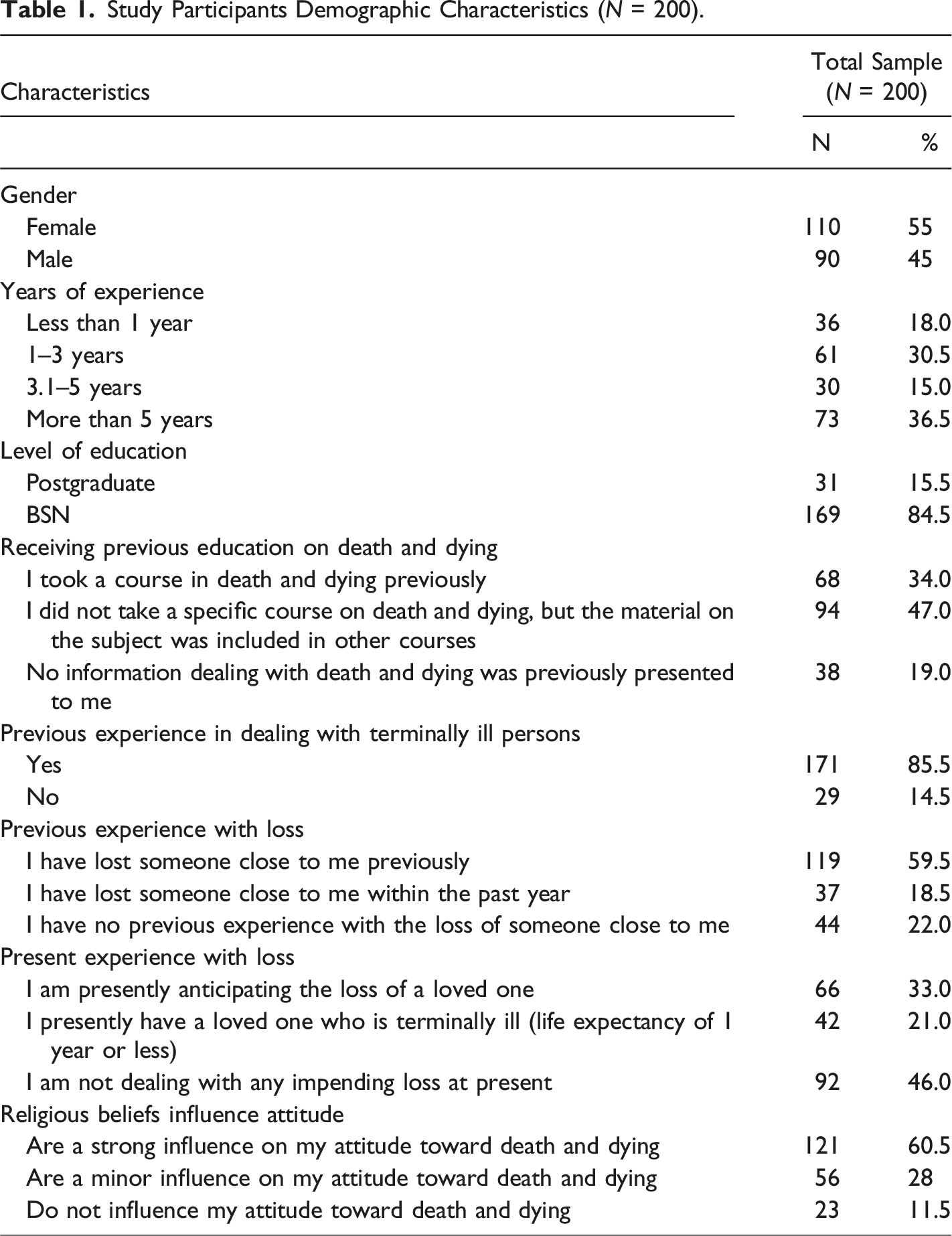
Participants’ Demographic Characteristics
Study Participants Demographic Characteristics (N = 200).
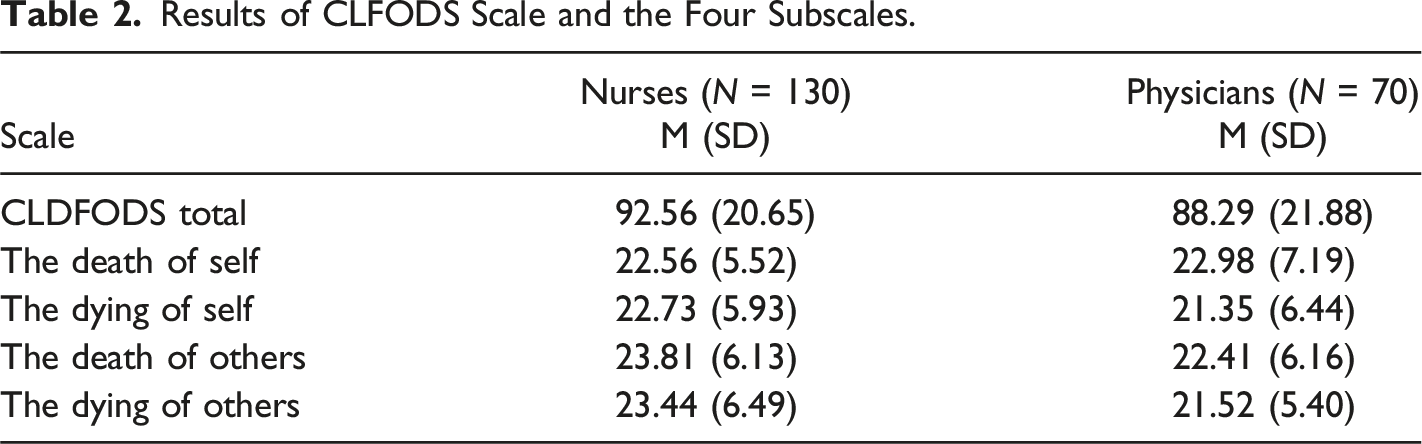
Death Anxiety Levels
Results of CLFODS Scale and the Four Subscales.
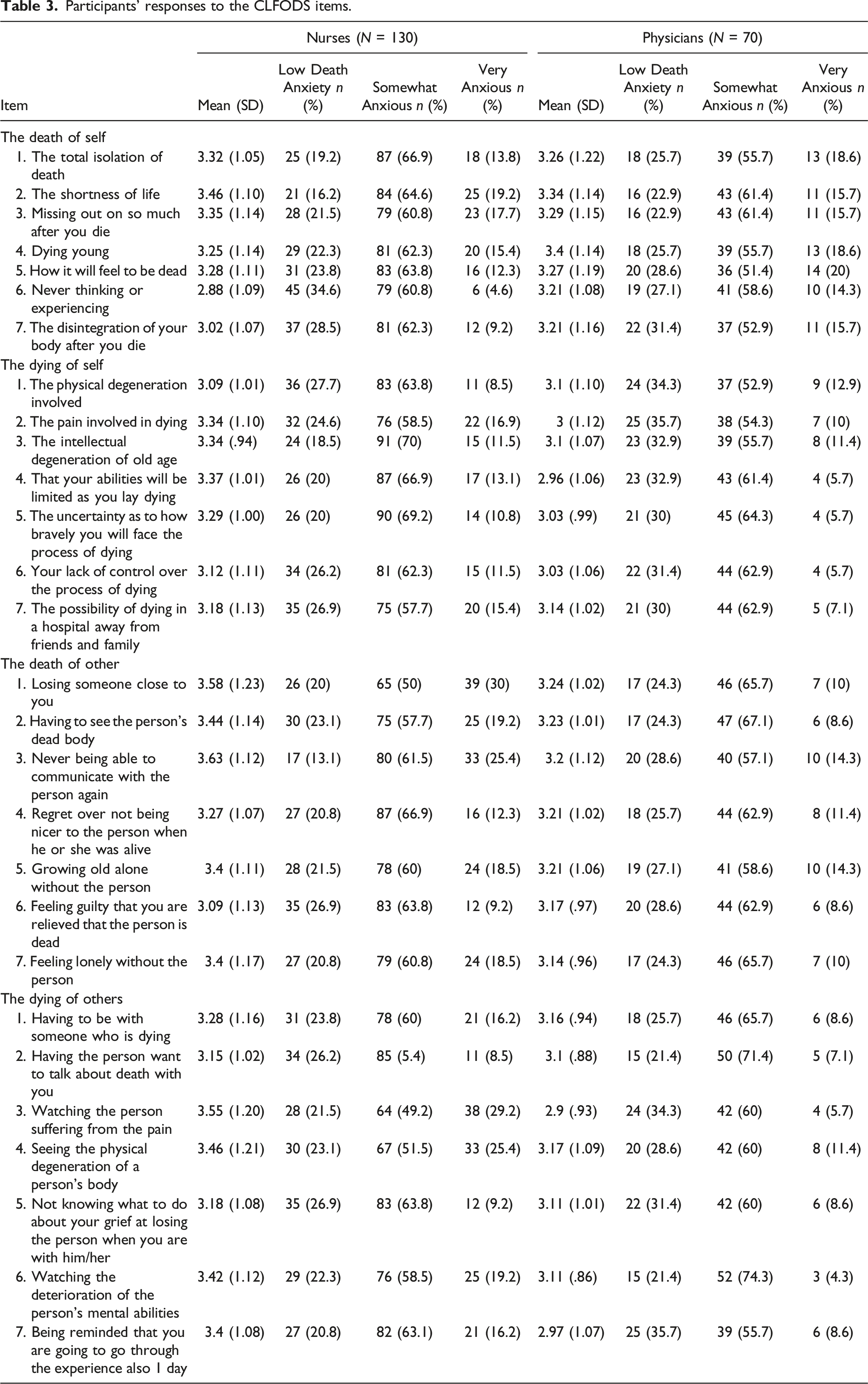
Participants’ responses to the CLFODS items.
Differences in Participants’ Level of Death Anxiety Based on Their Demographic Characteristics
Differences in Nurses’ and Physicians’ Death Anxiety Level Based on their Demographic Characteristics.
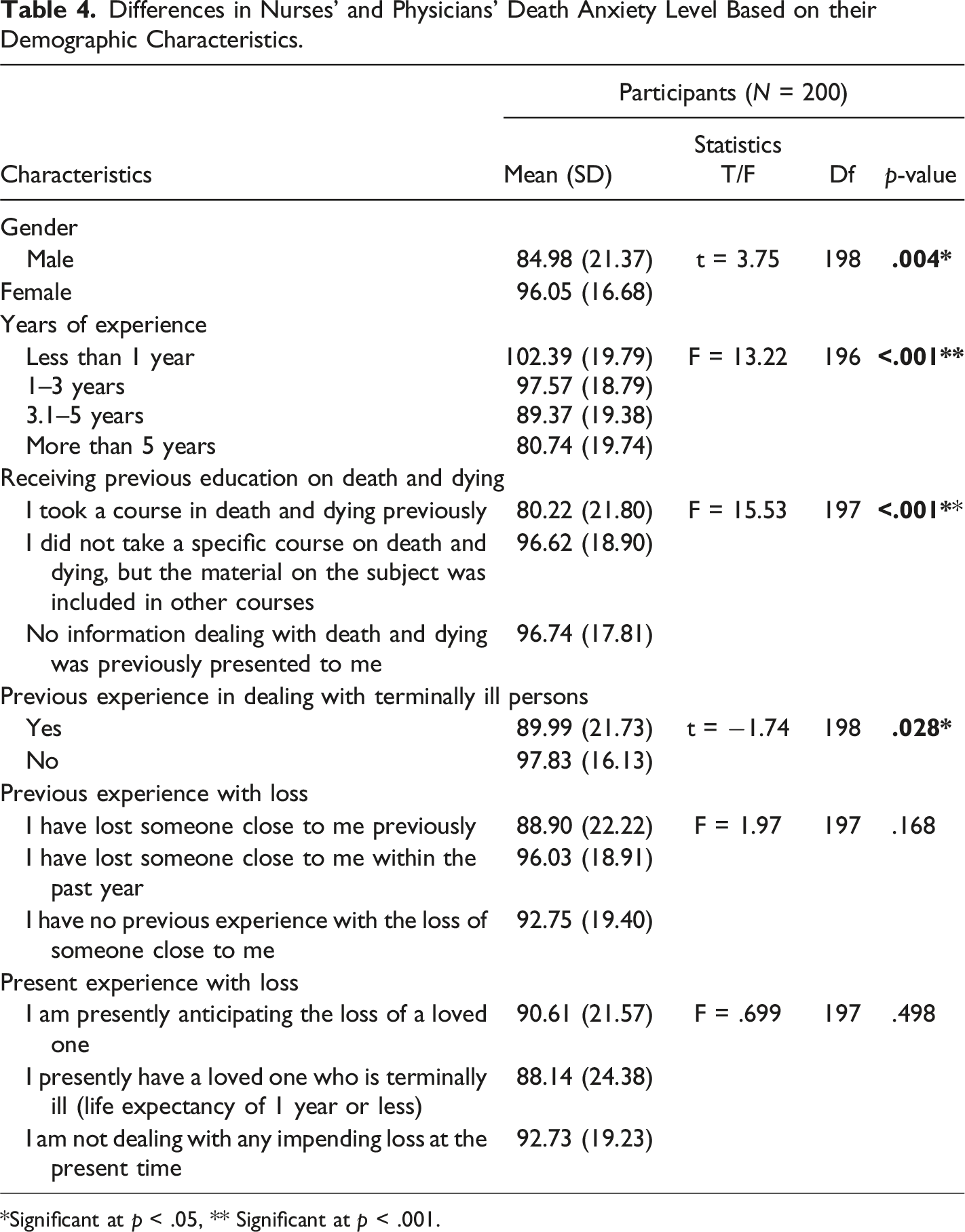
*Significant at p < .05, ** Significant at p < .001.
Post hoc analysis (Tukey HSD test) revealed that the mean score for nurses and physicians with more than 5 years’ experience (M = 80.74, SD = 19.74) was significantly lower than nurses whose years of experience were less than 1 year (M = 102.39, SD = 19.79) or ranged between one to 3 years (M = 89.37, SD = 18.79). Similarly, nurses and physicians who attended an entire education course on death and dying had significantly lower anxiety levels (M = 80.22, SD = 21.80) than those who only received educational material (M = 96.62, SD = 18.90), and those who did not receive any education at all (M = 96.74, SD = 17.81). Lastly, nurses’ and physicians’ who stated that their religious beliefs have a strong influence on their attitude had statistically significant lower anxiety scores (M = 83.30, SD = 17.36) than nurses whose religious beliefs have a minor influence on their attitude (M = 102.29, SD = 17.67) and those whose religious beliefs do not influence their attitude (M = 104.61, SD = 27.80).
Discussion
The current study was assessed the level of death anxiety among oncology nurses and physicians in Jordan, furthermore the differences in death anxiety level between participants were determined based on several factors.
Death Anxiety Level
Based on the finding of this study, oncology nurses and physicians in Jordan have a moderate level of death anxiety, Furthermore, the findings of this research exhibited that nurses experience a higher level of death anxiety than physicians, which supports implies that the nursing profession is a challenging and stressful occupation that exposes nurses to stressful situations more frequently than other health care professionals. The current result is consistent with the findings of a previous study of oncology nurses, which found that oncology nurses had a moderate fear of death level (Braun et al., 2009). This finding might be explained by the fact that nurses build close relationships with patients and their families, interact more directly with death, and encounter the feelings and emotions that arise when they witness a patient die suddenly (Mondragon-Sanchez et al., 2015 and Wazqar, 2019).
Demographic Variables and Death Anxiety Level
The present study revealed that there are a statistically significant differences in nurses’ and physicians’ death anxiety level between mean groups based on their demographic variables:
Gender
The current finding revealed a variation in death anxiety according to gender; female participants reported a higher level of death anxiety than males. That could be explained considering societal norms as males do not find it desirable to communicate their emotions. In the contrast, females learned that sharing their own feelings and emotions is allowable (Abdel-Khalek, 2005). Moreover, females are more compassionate and attentive to the needs of individuals facing terminal disease or death, which justifies their higher level of death anxiety and apprehension. Further, females are expected to share their emotions more than males at a younger age (Scalpello Hammett, 2012; Abdel-Khalek & Al-Kandari, 2007; Chan & Yap, 2009).
Correspondingly, this finding is consistent with a previous research study conducted among Jordanian nurses which found that female nurses had higher death anxiety levels than male nurses (Abu Hasheesh et al., 2013). In concord, the same result was found in multiple research studies conducted among nursing students. Also, Gurdogan et al. (2019) conducted a recent study among nursing students in Turkey, which supports our findings that gender influences the level of death anxiety and fear of death. Also, the current finding is in line with the result of previous research studies (Acehan & Eker, 2013 and Pehlivan et al., 2020), which revealed a statistically significant correlation between gender and death anxiety since the females reported a higher level of anxiety compared to males.
Previous Education
Previous education about death has a statistically significant impact on the level of death anxiety, as well as fear of death. As a result, participants who claimed that they attended a death course previously reported a lower level of death anxiety, since the attendance of educational courses regarding death and dying assists individuals in acquiring a tremendous sense of control, particularly control over their death perception, as well as over their death-anxiety emotions (Testoni et al., 2019). Moreover, death education assists in utilizing effective adaptation methods for dealing with death anxiety to combat negative consequences such as poor communication, and improve quality of life (Nia et al., 2015).
Correspondingly, our study findings are consistent with numerous research studies. For instance, a study conducted among medical students at the University of Cambridge, which revealed that the fear of death level decreased after palliative care education (Thiemann et al., 2015). Correspondingly, another study published in Greek among nurses supports the current observation, indicating that nurses who had completed specific palliative care training had no fear of death and had less trouble communicating about death and dying (Zyga et al., 2015).
Death Anxiety and Religious Beliefs
Religion assists individuals in coping with life and death concerns through offering a context for the expected life and what happens to them after dying (Chan and Yap. 2009). According to the findings of this study, religious beliefs have a significant effect on the level of death anxiety and fear of death. As a result, the participants who stated that religious beliefs significantly affect their attitudes toward death and dying reported less death anxiety level than those who stated that religious beliefs had no influence on their attitudes toward death and dying care.
Several studies were conducted among different groups (nursing students, medical students, registered nurses, and physicians) who identified religious beliefs as a significant contributor to death anxiety and fear of death, which supports the results of the current study. For instance, a review of a literature study was done by (Ellis &Wahab. 2013) conclude that there is a significant negative association between religious beliefs and fear of death among people who are asserted that they are at least modestly religious. In agreement with the current conclusion, a prior study (Xu et al., 2019) indicated that undergraduate nursing students who did not have a religious belief scored higher in the subcategory of fear of death. Also, several studies found that religious beliefs influence death anxiety and fear of death (Iranmanesh et al., 2008; Peters et al., 2013; Asadpour et al., 2016; Peterson et al., 2010; Arslan et al., 2014; Saleem & Saleem, 2020)
Experience With Dying Patients
Another interesting finding in the current study was that the experience of caring for dying patients reduces death anxiety and fear of death levels significantly. The current observation is consistent with (Xu et al., 2019), who found that previous experience has a substantial effect on nursing students' fear of death level. Since the experience of mortality enhances the comprehension of terminally ill patients' concerns, reduces the level of anxiety among health care professionals, and makes them comfortable while dealing with terminally ill patients.
Correspondingly, a previous study conducted by (Halliday & Boughton, 2008) revealed that nurses with previous experience with dying patients showed lower death anxiety levels than participants who had no prior experience with dying patients. Furthermore, the results of this study substantially corroborate the findings of a previous study conducted in Mexico to compare the level of death anxiety and fear of death among registered nurses and nursing students using the Collett-Lester fear of death scale (Mondragón-Sánchez et al., 2015). Lastly, the present finding is in line with the result of a previous study conducted by (Mallory, 2003) in Appalachian Mountains, which claimed that the experience of caring for a patient with cancer has a positive influence on death anxiety since it enhances their end-of-life coping skills.
Study Limitations, Implications and Recommendations
The current study provides a deeper understanding of the death anxiety level and the fear of death among oncology nurses and physicians. Furthermore, the current study highlighted the main factors that affect the death anxiety level. Additionally, the study findings increased oncology nurses' and physicians' awareness about their level of death anxiety. Importantly, the current study findings could be implied in both nursing and medicine fields to establish practice guidelines that improve the quality of care. However, there is a gap in literature regarding how to decrease the level of death anxiety and fear of death among nurses and physicians. Therefore, the result of this study could be utilized as a reference point for future research studies and considered as a baseline for future studies investigating death anxiety levels among nurses and physicians, as well as the demographic characteristics that is influence the level of death anxiety among oncology nurses and physicians and impacts the caring for dying patients.
However, this study has a few limitations; first, the participants were recruited from only one specialized cancer hospital in Jordan. Second, the findings may be limited by the convenience sample of nurses and physicians, which is not representative of all Jordanian nurses and physicians and included only oncology nurses and physicians, which could potentially limit the generalization of the findings
Oncology nurses and physicians are highly vulnerable to mortality and frequently caring for dying patients. Consequently, they should have the knowledge and skills required for optimum care, as well as have efficient interaction and communication with patients and their families. Furthermore, younger and inexperienced employees should be given special attention and extensive training. Since the findings of this study offered baseline data that could be implied as evidence that the inexperienced employees who did not attend previous courses have a negative attitude toward death and a high level of death anxiety.
Conclusion
On a routine basis, medical professionals are in close contact to terminally ill and dying individuals. The manner in which they will react to death and end-of-life care will also vary depending on their prior experiences, which makes their reaction to mortality unpredictable. Furthermore, exposure to death occurrences is typically linked to a high level of death anxiety among physicians and nurses, which severely impacts the quality of care. However, caring for dying patients is an extremely challenging task that requires both skill as well as an understanding of the nurses' and physicians' own personal thoughts regarding death and dying. Moreover, they have to address the inevitability of mortality since they are caring for dying patients frequently. They have to understand and acknowledge death anxiety level before interacting with dying patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Dr.