
Abstract
Many people lost a relative during the COVID-19 pandemic. Such a loss may have deleterious implications due to the circumstances of bereavement during lockdowns and social distancing. This study aimed to explore depressive symptoms, complicated grief, and suicidal ideation in the grieving process among 104 bereaved jewish adults who had lost relatives during the COVID-19 pandemic by completing self-reported questionnaires. The results indicate high suicidal ideation, complicated grief, and depression among them. Bereaved with suicidal ideation have an avoidant attachment and a close relationship with the deceased. These results highlight the adverse implication of COVID-19 on the grief process.
Introduction
In 2020, the COVID-19 pandemic erupted around the world. The pandemic was the cause of an extended and long-lasting period of stress during which there was a sense that death was all around: Death was constantly reported on the news on television and social media; the ever-present sense of death was also enhanced by the policy of social distancing imposed by governments health authorities, which automatically affected the usual rituals following death and of the whole process of grieving. Many people lost a relative or a friend because of the pandemic. However, all those who lost someone during that time were affected regardless of the specific cause of death.
In response to the unpredictable nature of the virus, people are constantly worried about contracting the disease and whether they might have infected anyone else (Diolaiuti et al., 2021). In addition, there was a constant concern regarding the possibility of losing a loved one, which contributed to the development of a traumatic experience. Moreover, a shared sense of purposelessness in life was exacerbated by hopelessness and uncertain feelings about the pandemic progress and lack of preparation for death that applied to some cases. Another major stressor was the inability to receive warmth and affection from others while grieving and mourning. A reasonable expectation would be that going through grief processes under these circumstances caused by the COVID-19 pandemic would make it hard to adaptively overcome these traumatic experiences and increase the likelihood of complicated grief (CG).
Losing a loved one to death is one of the most painful situations in life and has various physical, psychological, and social implications. Grief and loss cannot be avoided in life and are usually accompanied by significant changes in our lives (Pease, 2020). Grief includes various symptoms; some pass with time, while others may not (Prigerson et al., 2021). Although the way one copes with grief is unique to each loss, some commonalities have been identified, such as accepting the reality of the person’s death, guilt, preoccupation with thoughts about the deceased, and trying to work through the pain (Prigerson et al., 2021; van Eersel et al., 2020). Although most bereaved people experience grief to only a mild or moderate degree and return to normal functioning relatively soon after the loss, a minority, about 9%–15%, suffer more complicated grief reactions (Aoyama et al., 2018; Tang & Xiang, 2021).
Complicated Grief (CG) is a condition of intense grief that lasts longer than expected based on social norms and causes significant difficulties in daily functioning (Aoyama et al., 2018; Gesi et al., 2020). It is also associated with sleep disturbances, suicidal ideation and behavior, substance abuse, and abnormalities in the immune system. Symptoms of CG can be divided into two categories: First, separation distress which includes longing, searching for the deceased, loneliness, sadness, and preoccupation with thoughts or images of the dead (Eisma et al., 2020; Prigerson et al., 2021). Second, traumatic stress, such as disbelief and an inability to accept the reality of death, mistrust, anger, shock, and somatic symptoms.
Complicated Grief (CG) seems to be a distinct traumatic response that follows the loss of a loved one (Eisma et al., 2020). Existential encounters with death are characterized by trauma and loss. They can expose people’s vulnerabilities so that the more one thinks about and fears death; the more likely one is to suffer from CG. According to some studies, going through grief in traumatic times, such as during the COVID-19 pandemic, is fundamentally different from non-traumatic times (Goveas & Shear, 2020; Worden, 2018). Experiencing grief during traumatic times is considered a significant factor in CG (Eisma et al., 2020; Worden, 2018). Whether or not a period is traumatic is determined by the circumstances of the period or specific events, not by the individual’s reaction, and the greater the intensity of exposure to stressors, the greater the impact on the individual.
The definition of suicidal ideation is often an elusive and fluid construct and usually refers to thoughts about engaging in suicidal behavior (Jobes & Joiner, 2019). As noted above, prior studies found high rates of suicidal ideation among patients with CG (Levi-Belz & Aisenberg, 2021). People who suffer from CG have a 9.7 more significant risk of suicidal ideation and behavior (Levi-Belz & Lev-Ari, 2022).
Depression during grief is a predictor of CG (Mason et al., 2020). Depression can be experienced regardless of death but could also be a symptom of grief. There are many similarities between grief and depression, such as impaired functioning, thoughts about worthlessness, psychomotor changes, and suicidality (Lenferink et al., 2020). Studies have found that 10% of grieving individuals experience the onset of the depressive syndrome within 1 year of the death of a loved one and that recent experience of grief is the most potent risk factor for a major depressive episode. Although depression stemming from bereavement may remit spontaneously, this is not always the case.
When discussing the reaction to grief, it is necessary to consider two other aspects that may play a significant role: the grieving individual’s attachment style and the social support provided through the grief process. Because bereavement often involves reorganizing attachment systems, attachment theory provides a valuable framework for understanding grief reactions (Smigelsky et al., 2020). Different reactions to losing a loved partner in adulthood are related to attachment representations in secure or insecure attachment patterns (Tidwell et al., 2021). Each style handles emotions differently, which is crucial to adjust to the loss. Insecure attachment has been suggested to play a vital role as a risk factor for CG (Smigelsky et al., 2020). Based on Bowlby’s theory, secure individuals experience an intense period of grief that eventually fades as they adapt to the reality of the loss (Tidwell et al., 2021). Many anxious-ambivalent individuals do not adapt over time and are likely to display more chronic grief with sustained levels of distress. Avoidant attachment is associated with abnormal grief characterized by delayed or absent types. People with this attachment style are more likely to adopt distancing strategies. Accordingly, those who reported closer attachment to the deceased reported greater levels of grief (Smigelsky et al., 2020).
Regarding social support, when a death occurs, the physical, mental, and social consequences of social distancing, such as those that many people experienced during the COVID-19 pandemic, may increase the risk of CG (Wallace et al., 2020). Grief can vary in intensity, duration, and frequency, depending on the manner of death, the individual family’s tradition, and the cultural beliefs surrounding death (Stelzer et al., 2020). Rituals, prayers, beliefs about death and the process of dying, including what is expected of those left behind after the passing of someone who matters, are part of every religion and culture (Roberson et al., 2018). Some basic social rituals are practiced during significant changes, especially related to death (McCoyd et al., 2021). Many studies have shown that these rituals (e.g., the funeral and sitting shiva among Jews) help the grieving person in two ways: firstly, they provide some sense of control of the situation, and secondly, these rituals decrease the intensity of mourning and grief.
In Jewish culture, funerals are usually held as soon as possible after the individual’s death (Roberson et al., 2018). The shiva, a traditional seven-day mourning period, begins immediately after the funeral. During the shiva, the deceased’s family is cared for by friends and the community while they grieve their loss. The grief process is impaired when these social rituals are damaged (e.g., by the government distancing policy during the COVID-19 pandemic, which prevented people from visiting grieving persons; (McCoyd et al., 2021)). Such a situation is termed disenfranchised grief, which means that the grieving persons do not get the support and sympathy they need from others to allow them to adapt to the loss in healthy ways. Recent studies have found that lower levels of social support, a lack of preparation for death, and guilt are risk factors for CG and depression (Eisma et al., 2021; Wallace et al., 2020). All these were relevant factors in dealing with death during the COVID-19 pandemic.
The Current Study
The COVID-19 pandemic has disrupted the normal grief process and approaches to providing support during grief (Wallace et al., 2020). Thus, the pandemic’s effects may have significantly impacted the physical and mental health and the general well-being of those who have experienced loss (Hanna et al., 2021). This led us to expect that experiencing loss during the COVID-19 pandemic would increase the probability of experiencing CG, depression, and suicidal ideation. This risk increases significantly if their rituals are not practiced as usual. In addition, we assume that there would be differences in the probability of experiencing CG, depression, and suicidal ideation between those who have suffered a loss due to COVID-19 or other causes. Furthermore, individuals with insecure attachments would suffer more from CG, depression, and suicidal ideation.
Methods
Participants and Procedures
The sample included 104 bereaved adult participants who had lost relatives, friends, or acquaintances during the COVID-19 pandemic; 82 females (78.8%), and 22 males (21.2%), with a mean age of 31. They were recruited through social media and snowball sampling. Participants gave their written consent. All respondents who participated in the study voluntarily and anonymously filled out an internet questionnaire and were provided a referral sheet with information about mental health services if such services were needed.
Measures
Inventory of Complicated Grief-Revised
This self-report measure consists of 15 items on separation distress and traumatic distress rated on a 5-point Likert scale. The final score is the sum of the scores for all items and ranges from 15 to 75. A cutoff of 36 or more is considered complicated grief (O’Connor et al., 2010). In this study, the internal consistency was high (alpha = .93).
Patient Health Questionnaire (PHQ-9)
The severity of depressive symptoms was assessed using the nine-item Patient health questionnaire, a module from the full PHQ (Kroenke et al., 2010). The PHQ-9 score ranges from 0 (not at all) to 3 (nearly every day) and is summed to obtain a total score from 0 to 27. A cutoff of 10 or higher is considered depression. In this study, the internal consistency was high (alpha = .88).
Suicide Behavior Questionnaire-Revised
The questionnaire included four items, each referring to another dimension of suicidality: item 1 relates to lifetime suicide ideation and behavior (score ranges from 1 to 6); item 2 assesses suicide ideation in the past year (score ranges from 1 to 5); item 3 is about whether the respondent shared their suicide thoughts with others (score ranges from 1 to 5); item 4 refers to the likelihood of suicide attempts in the future (score ranges from 1 to 7). The SBQ-R score is summed to obtain a total score from 4 to 23. A cutoff of 7 or higher is considered a high suicidal risk (Osman et al., 2001). In addition, every participant who marked anything else other than never in item 2 was considered to have had suicidal ideation in the last 12 months. In this study, the internal consistency was high (alpha = .84).
Experience in Close Relationship Scale-Short Version
The Experience in Close Relationship Scale-Short Version (ECR-S) includes 12 items developed from the original 36-item ECR (Wei et al., 2007). Six items assess anxious attachment, and the other six items assess avoidant attachment. Respondents rated each item on a 7-point Likert scale ranging from 1 (disagree strongly) to 7 (agree strongly) and is summed to obtain a total score from 12 to 84. Items 1,5,8,9 are reversed scored. This study’s coefficient alpha was .70 for anxiety and .73 for avoidance.
Demographic and Death-Related Characteristics
The questions included gender, age, marital status, and religiosity. Information about the deceased was also obtained, and had the following: relationship to the deceased, time of death, cause of death, and details about the funeral and shiva (whether it was conducted as normal, reduced amount of people, on zoom, and regarding shiva, if there wasn’t any at all).
Data Analysis
The surveys resulted in 10 participants with missing data, mainly for a single item. The relevant mean of this measure was calculated without this item. All analyses were conducted using IBM SPSS Statistics, version 27.0. The comparison between participants with suicidal ideation and non-suicidal thoughts utilized chi-square tests for dichotomous data (e.g., gender and other cutoff point measures) and t-tests or ANOVA for continuous data (the severity of depression, complicated grief, and social support). Variables that differed significantly between those with suicidal thoughts were included in multivariable logistic regression. Goodness-of-fit statistics were used to compare and select the most parsimonious models. The alpha value was set to .05.
Results
Demographic and Clinical Characteristics of the Sample
Demographic and Clinical Characteristics of the Sample.
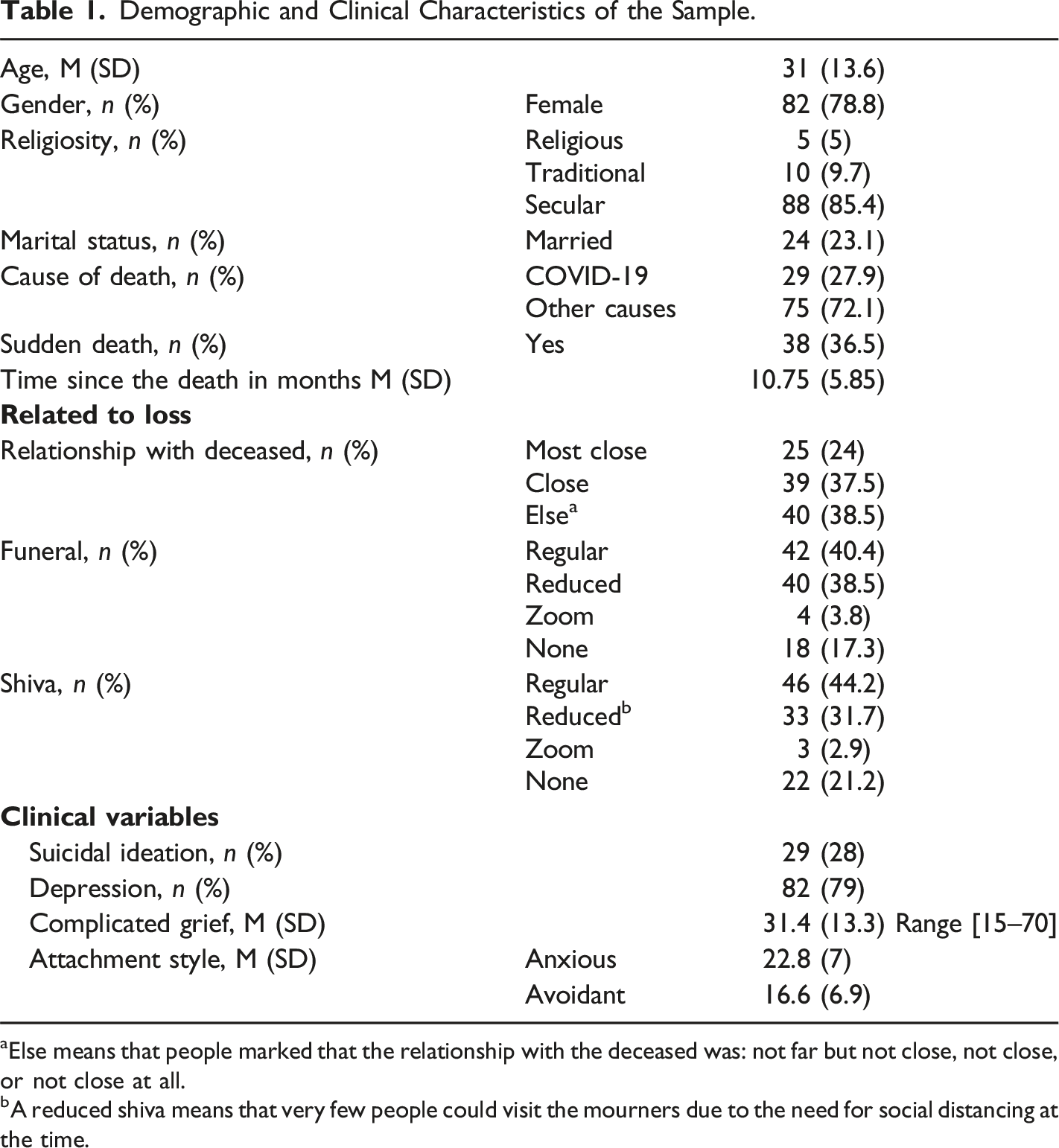
aElse means that people marked that the relationship with the deceased was: not far but not close, not close, or not close at all.
bA reduced shiva means that very few people could visit the mourners due to the need for social distancing at the time.
Clinically, a third of the sample reported CG (36%), more than 75% of the sample reported moderate to severe symptoms of depression (79%), and almost a third of the sample reported suicidal ideation (28%).
Pearson Correlation Matrix of Clinical and Related to Loss Variables.
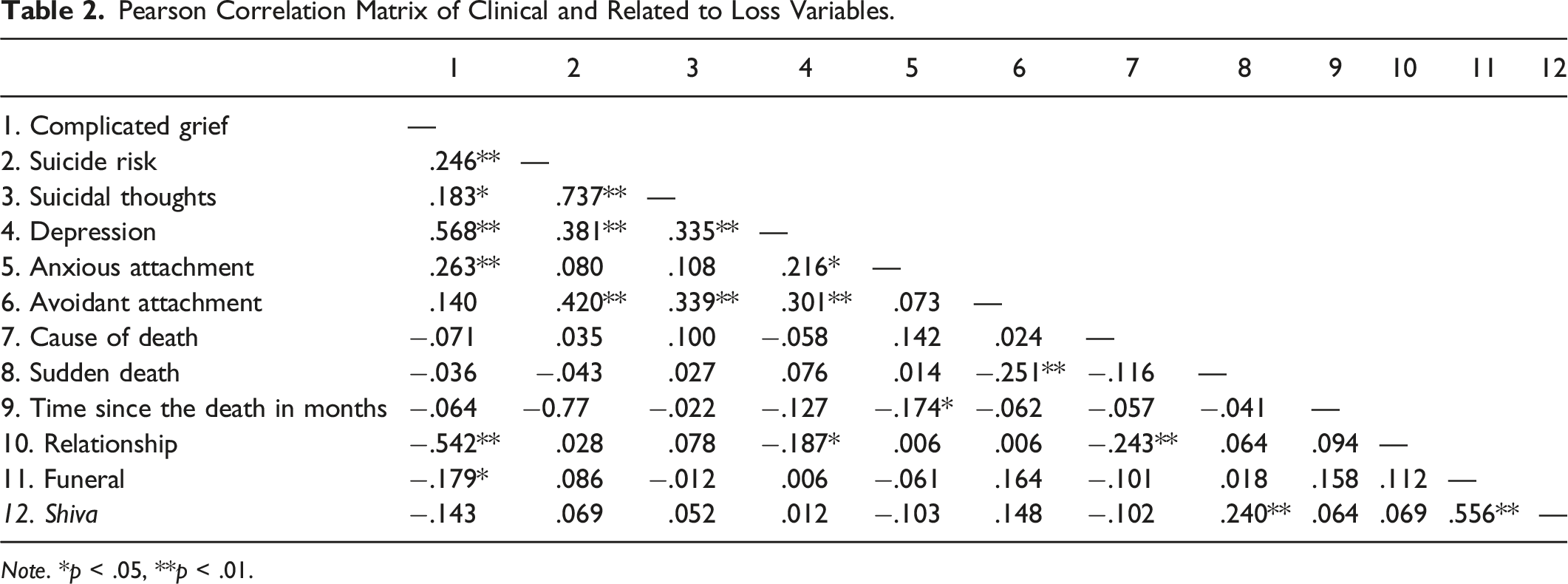
Note. *p < .05, **p < .01.
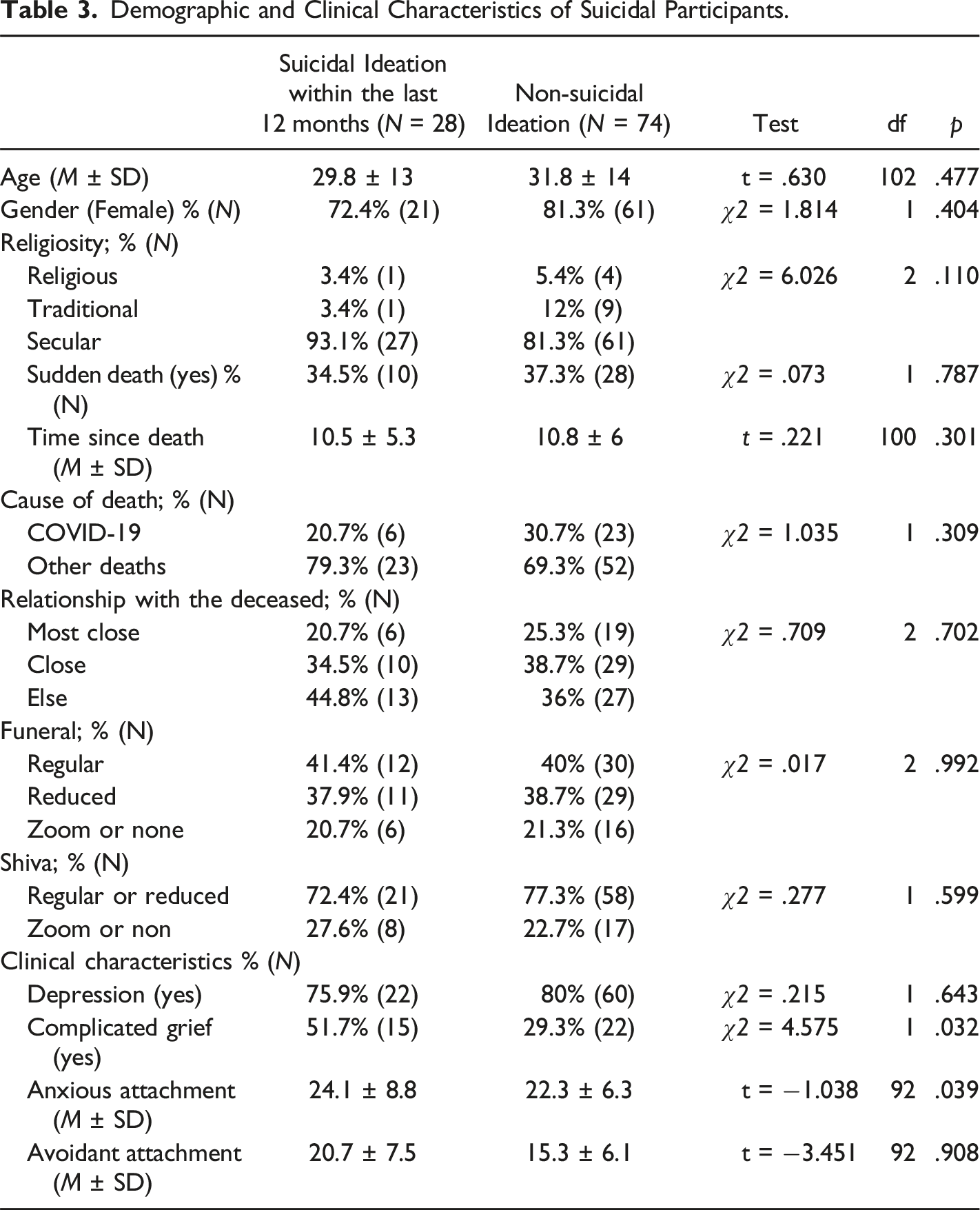
Comparison of Bereaved Participants with Suicidal Ideation in the Last 12 Months Versus Bereaved Participants Without Suicidal Ideation
Demographic and Clinical Characteristics of Suicidal Participants.
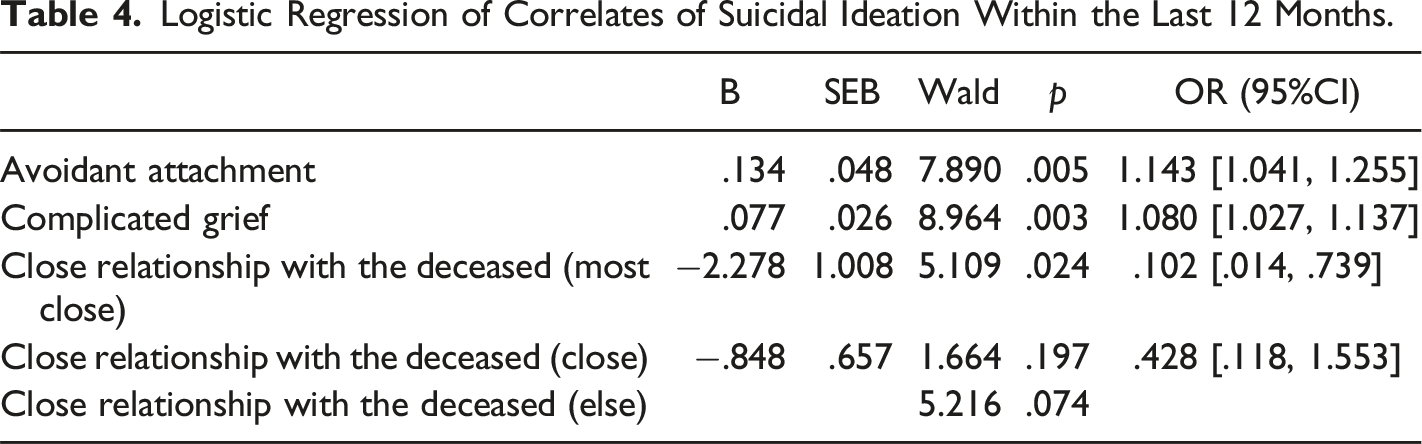
Logistic Regression of Correlates of Suicidal Ideation Within the Last 12 Months.
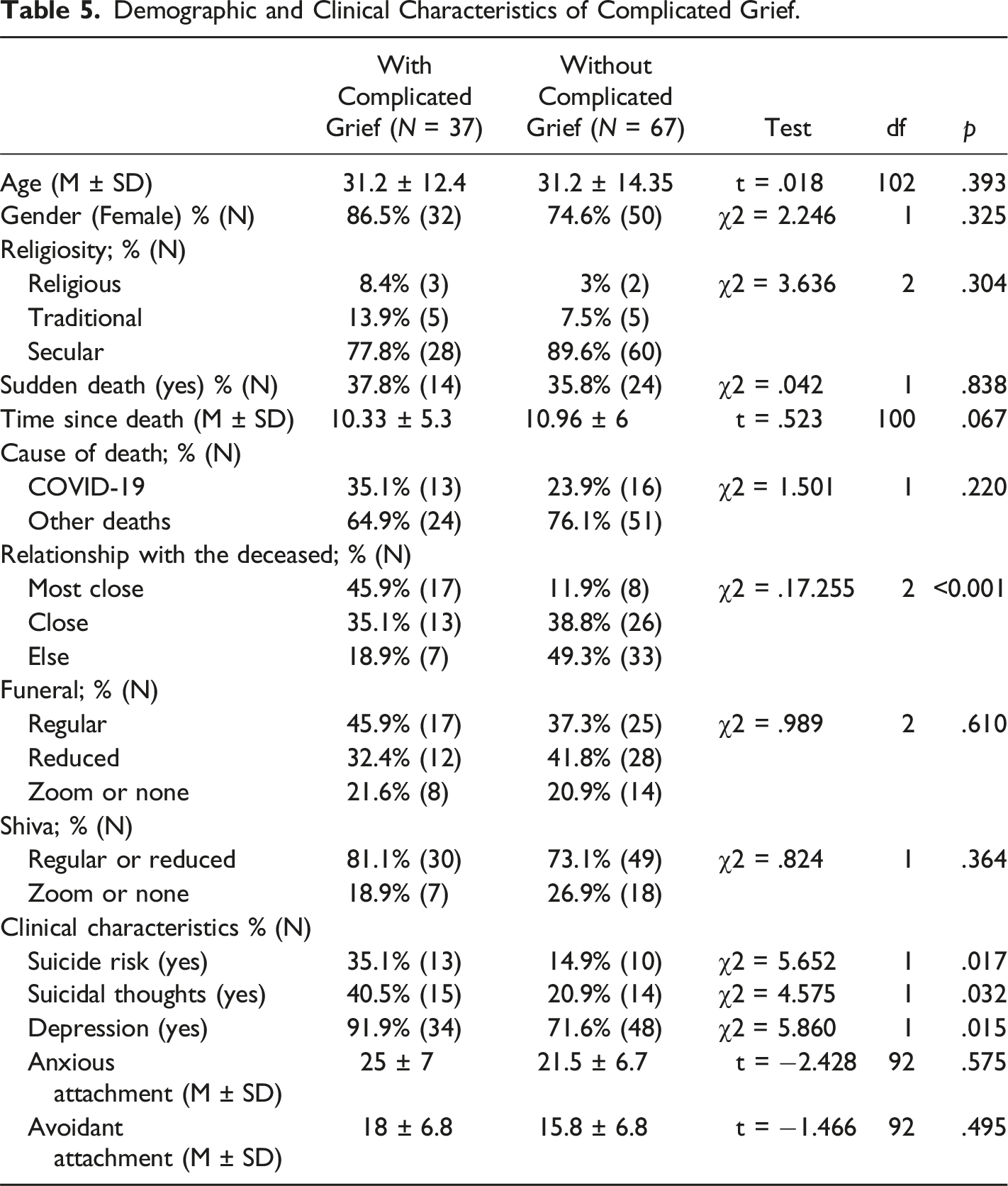
Comparison of Demographic and Clinical Aspects of Participants with High levels of Complicated Grief Compared to Those with Low Levels of Complicated Grief
Demographic and Clinical Characteristics of Complicated Grief.
Discussion
The aim of this study was to explore the possible effects of the COVID-19 pandemic on the grief process, assuming that it may have been compromised due to particular circumstances. The findings show a relatively high percentage of people who suffer from CG, depression, and suicidal ideation. We found that the closer the relationship to the deceased, the more likely the mental distress presents as CG, depression, and suicidal ideation. The highest risk for suicidal ideation was among people who suffered from CG, had an avoidant attachment, and for whom the relationship with the deceased was the closest.
These results highlight the role of stressful events, such as the COVID-19 pandemic, as a risk factor for developing CG, suicidal ideation, and depression while coping with grief, as discussed in other studies (Bertuccio & Runion, 2020; Eisma & Tamminga, 2020; Feder et al., 2021; Hanna et al., 2021; Maddrell, 2020).
A close relationship with the deceased found to be correlated to a high risk for suicide and to an increased presence of suicidal ideation. This is consistent with other results (Jobes & Joiner, 2019; Smigelsky et al., 2020). In addition, suicidal ideation is strongly associated with experiencing CG and having an avoidant attachment, consistent with other results (Levi-Belz & Aisenberg, 2021; Levi-Belz & Lev-Ari, 2022; Maccallum & Bryant, 2018).
An avoidant attachment was found to be correlated with suicidal ideation and CG. These associations may result from the fact that when a bereaved person with avoidant attachment loses a loved one, it is difficult for them to express their pain externally and rely on others. Therefore, this pain is directed inward and presents as suicidal ideation. This explanation, consistent with the findings of other studies, highlights the strong relationship between insecure attachment and suicidal ideation and the difficulty of coping with grief (Oon-arom et al., 2019; Smigelsky et al., 2020; Tidwell et al., 2021).
Previous studies have found a significant association between suicidal ideation and CG and suggest different factors that mediate this association, including social support, self-disclosure, and attachment style (Levi-Belz & Aisenberg, 2021; Levi-Belz & Lev-Ari, 2022). The interaction between CG and suicidal ideation in the manner that leads the grieving person to experience CG and the difficulty of accepting the loss of a loved one would sometimes increase suicidal ideation as a way of escaping reality.
Interestingly, we did not find a significant association between social rituals, such as funerals and shiva, and CG, although other studies have highlighted the importance of social support (McCoyd et al., 2021; Roberson et al., 2018; Wallace et al., 2020). Perhaps the effect of social distancing could be considered a part of the whole complexity of the period of the COVID-19 pandemic, which indirectly increased the chances of suffering from CG, depression, and suicidal ideation. For example, even if a shiva did take place, because of the fear of spreading COVID-19, people may have been more distant from each other than usual and spent less or little time in groups. Therefore, an indirect correlation might be hypothesized between social rituals and CG, depression, and suicidal ideation, suggesting further research is needed regarding the specific variables of funeral and shiva experience that could influence this correlation.
High rates of depression may be explained by the thought that dealing with COVID-19 generally increased depression among the population (Hawes et al., 2021; Ustun, 2021). It could also be explained by the similarity between CG symptoms and symptoms of depression, especially during the first year of grieving (Aoyama et al., 2018; Mason et al., 2020).
Limitations and Future Studies
While the current study provides more information about the implications of the COVID-19 pandemic on the grief process, the small sample size makes it difficult to generalize the results to other samples and groups. Much work remains to be done before a complete understanding of the extent of COVID-19 implications on grief is achieved. Replication of this research in other populations is needed to expand the knowledge about this issue worldwide. Additionally, this study was executed during the COVID-19 pandemic and not long after the participants had experienced the death of a loved one (a maximum of 2 years). Replicating this research for an extended period after COVID-19 would indicate the difficulties we currently witness over time and if more complications are revealed. Another limitation was recruiting through social media, which addresses the younger subject mostly. Continuation of examination of more adult subjects could provide more information on the application through different ages.
Conclusions and Implications
The present research contributes to a growing body of evidence suggesting that difficulties connected to the COVID-19 pandemic complicated grief for those who had lost someone during that time. Moreover, understanding the implications of COVID-19 on the grief process might contribute to a further understanding of the basic grief process.
These results have potential intervention implications, such as focusing more on depression and suicidal ideation among grieving persons and clinically differentiating between depressive and complicated grief symptoms. Furthermore, given the understanding that people are more likely to develop such symptoms (e.g., depression and suicidal ideation) and complicated grief during times of crisis, interventions are needed. Both for people who have experienced death and among the general public to alleviate symptoms of depression and suicidal ideation, and complicated grief.
Footnotes
IRB Statement
The study was approved by the Institutional Review Board (IRB) of the Academic College of Tel-Aviv Yaffo.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.