
Abstract
End-of-life care is a critical aspect of long-term care, yet there is limited understanding of nursing home staff’s experiences and preparation in this area, particularly among facility administrators. To address this gap, two cohorts of Administrators-in-Training (2021 & 2022) were interviewed about their knowledge and practices regarding end-of-life care in skilled nursing facilities. Interviews focused on involvement in end-of-life discussions, coping strategies, grief support, and personal perspectives on death. The findings revealed a significant lack of training on death management and end-of-life care for Administrators-in-Training (AITs), with limited grief support mechanisms in place within skilled nursing facilities. Personal experiences with death influenced AITs' approach to end-of-life care, and various coping strategies were observed. The results highlight the need for comprehensive training programs and improved support for AITs to enhance end-of-life care delivery.
Keywords
Introduction
The provision of quality end-of-life care is of utmost importance in nursing homes, where a significant number of older adults receive such services. The COVID-19 pandemic has further highlighted the need for effective end-of-life care, as a growing number of older adults make end-of-life decisions and receive care in nursing homes (Chidambaram, 2022; Miller et al., 2010).
Quality care during the end of life is crucial for individuals and their families, as it enables them to approach death with dignity and maintain a sense of identity and control over their end-of-life decisions (Motamedi et al., 2021). This concept of dying with dignity aligns with the broader theoretical framework of person-centered care, which emphasizes tailoring care to meet the unique needs and preferences of each individual (Hadler et al., 2022). To understand the significance of this research within the broader framework of end-of-life care in nursing home settings, it is important to consider the historical developments and context of nursing home services. Traditionally, nursing homes primarily focused on custodial care, providing assistance with daily living activities and basic medical needs (Eaton, 2000). However, there has been a shift towards person-centered care, which recognizes the importance of holistic support, including end-of-life care, in meeting the complex needs of older adults (Feinberg, 2014; Oliver et al., 2005) This philosophy aligns with the cultural change movement in nursing homes, which began in the early 1980s as a response to concerns about substandard care (Jurkowski, 2013). The concepts of “quality of care” and “quality of life” emerged as inseparable and equally important, influencing subsequent legislation and regulations (Koren, 2010). The Institute of Medicine’s report in 1986, “Improving the Quality of Care in Nursing Homes,” recommended changes in policies and procedures to ensure satisfactory care for nursing home residents, emphasizing the need for person-centered care (Koren, 2010). The Nursing Home Reform Act of 1987 solidified the requirement for nursing homes to provide person-centered care, making it a unique statutory mandate in the healthcare industry (Koren, 2010). Through person-centered care, healthcare staff can create an environment that promotes the dignity, well-being, and comfort of individuals nearing the end of life, enhancing the overall quality of care provided (Cohen et al., 2022; Koren, 2010).
Yet, research has shown that the quality of end-of-life care throughout the healthcare system is in need of improvement (Oliver et al., 2005). There are several barriers to the administration of end-of-life care specific to skilled nursing homes: difficulty in discussing death with residents and their families (Sjöberg et al., 2021), insufficient communication among staff (Gjerberg, et al., 2015), and workforce shortages (Young et al., 2017). But the most important barrier appears to be the lack of education on caring for the dying (Aldridge et al., 2016).
Education related to death and dying has gained recognition within healthcare professions as an essential component of comprehensive care. Various disciplines, such as nursing, social work, and counseling, now acknowledge the importance of equipping professionals with the necessary knowledge and skills to address end-of-life needs effectively (Hughes et al., 2018). For example, nursing education programs have incorporated coursework and clinical experiences focused on death and dying, covering topics like pain management, ethical considerations, and communication skills (Taylor et al., 2018). By integrating comprehensive training on death and dying across long-term care professionals, we can align with the principles of person-centered care and further enhance the quality of end-of-life care in nursing homes.
While progress has been made in death training, there is still limited understanding of the perspectives and training of administrators in nursing homes. Developing a model of end-of-life care for people in nursing homes requires an understanding of the priorities and concerns of key stakeholders, including administrators. Administrators play a crucial role in the delivery of care and organizational policies within nursing homes, and their perspectives are essential to understanding the challenges and gaps in training and support. Organizational support theory provides a valuable framework for understanding the significance of comprehending nursing home Administrators-in-Training perspectives on end-of-life care, their training experiences, and coping mechanisms (Taylor & Alfred, 2010). According to this theory, employees' perceptions of the support they receive from their organization play a critical role in their well-being and job performance (Kurtessis et al., 2017). In the context of nursing home care, Administrators-in-Training are key individuals who contribute to shaping the overall care environment. Investigating the training programs and experiences of Administrators-in-Training is essential to identifying potential gaps and challenges in their preparation for dealing with end-of-life care. Therefore, this study aims to provide qualitative information from Administrators-in-Training (AITs) to gain detailed insight into the factors that affect end-of-life care in nursing facilities, and to inform leadership development and training in this area.
The COVID-19 pandemic serves as a catalyst for reflection and investigation, providing an opportunity to understand how the pandemic has influenced the provision of end-of-life care in nursing homes and the specific training needs of administrators during this challenging period. Nursing home staff have faced rapidly changing circumstances in caring for a vulnerable population of residents in the wake of the COVID-19 pandemic, and there has been a disproportionately large number of morbidity and death rates among long-term care residents (Chidambaram, 2022). COVID-19 deaths in long-term care facilities make up at least 23% of all COVID-19 deaths in the United States (Chidambaram, 2022). Throughout the past 3 years, information and research on the COVID-19 pandemic has evolved quickly. Yet, with the lack of current studies, the experiences of nursing home staff are limited to data focused on nurses and front-line staff (Beattie et al., 2023). However, managers in skilled nursing care are also an important influence in the delivery of end-of-life care (Griffiths et al., 2019).
Therefore the aims of this study are twofold: (1) To increase the understanding of nursing home administrators’ preparation for dealing with end-of-life care during career development (i.e., identify the system gaps in leadership development regarding end-of-life care support and training) and (2) to provide qualitative information from AIT’s to yield further detailed insight into factors that affect end-of-life care at nursing facilities during the COVID-19 pandemic.
Methods
Data Collection
Recruitment was conducted through a program for long-term care administration at a midwestern university [specific university name redacted], resulting in a convenience sample. Data collection took place between Spring 2021-Spring 2022. A total of 66 students from the 2021 and 2022 cohorts completed the interviews, resulting in a response rate of 92%. The AIT’s completed their residency in 46 different skilled nursing facilities in 6 states (Colorado, Wisconsin, Minnesota, Illinois, Iowa, and Oregon). Students had completed at least 4 months of their 12-month residency at a skilled nursing facility at the point of the interview. The lead researcher, as an instructor in this program, had knowledge and familiarity with the subject matter and the AIT curriculum. Participants were informed by the lead researcher about the study’s purpose and were informed about the voluntary nature of their participation in the study. AITs were assured that they had the right to withdraw at any point, ensuring their autonomy and comfort throughout the research process. Because anonymity was assured, interviews were administered by an objective third party (graduate student) who was trained in qualitative surveying techniques. The interview lasted between 20–45 minutes. All the participants’ names were replaced during the transcription of the interviews.
The Survey
Building off research by Metallinou et al., (2021) the questionnaire utilized for this research consisted of 6 open-ended questions that investigate experiences and training related to end-of-life care in skilled nursing facilities (SNFs). While the specific focus of Metallinou et al.'s study differs from our research in nursing homes, certain aspects of their findings, such as coping strategies, staff support, and discussions about end-of-life decisions, can be applied to the context of nursing homes. By incorporating questions related to these topics, this study aims to explore similar themes in the experiences of nursing home staff, including administrators, to gain insights into their perspectives on end-of-life care and identify areas where support and training can be improved within the nursing home setting. By drawing on the research by Metallinou et al. (2021), we can enhance our understanding of the challenges and needs of healthcare professionals involved in end-of-life care and apply those insights to the specific context of nursing homes. The purpose of these questions was to examine end of life care in SNFs, education and death management, discussions about end-of-life decisions, coping strategies after death, staff support, and death focusing on personal life. Interviews were formatted in a semi-structured layout as an interview guideline and included the following prompts: (1) Have you had any training in death management (i.e., any training on providing end-of life care services)? (2) Do you provide any training in your facility about death, dying, and grief? (3) Thinking about your facility’s experience during the COVID-19 pandemic, who made decisions and was involved in end-of-life care at your facility? (4) What coping strategies do you use when faced with death, dying and grief at work? (5) Is there grief support available to staff within your SNF? (6a) What are your previous experiences dealing with death? (6b) Do you think these experiences impact your experience with dealing with death at work?
Data Analysis
Researchers used a multi-step inductive approach to seek patterns of meaning within interview responses (a conventional content analysis method) (Allen et al., 1997). Reliability was assured by investigator triangulation, with data being collected by one investigator and coding being completed by three individuals separately. The research team (this included student researchers) completed an initial review of the data set seeking common responses, utilizing in-vivo coding (looking at direct quotes rather than summarizing interviews) and descriptive coding to identify themes that emerged. Researchers then joined together to discuss the observations and identify common themes. Once primary categories were identified, the student research assistants and the faculty member then coded responses and added subcategories. In addition to considering relative frequency of responses throughout thematic categories, the data was also reviewed and categorized into strata on the basis of similarities and differences, and finally, a set of examples was prepared for each of the themes of the data.
Results
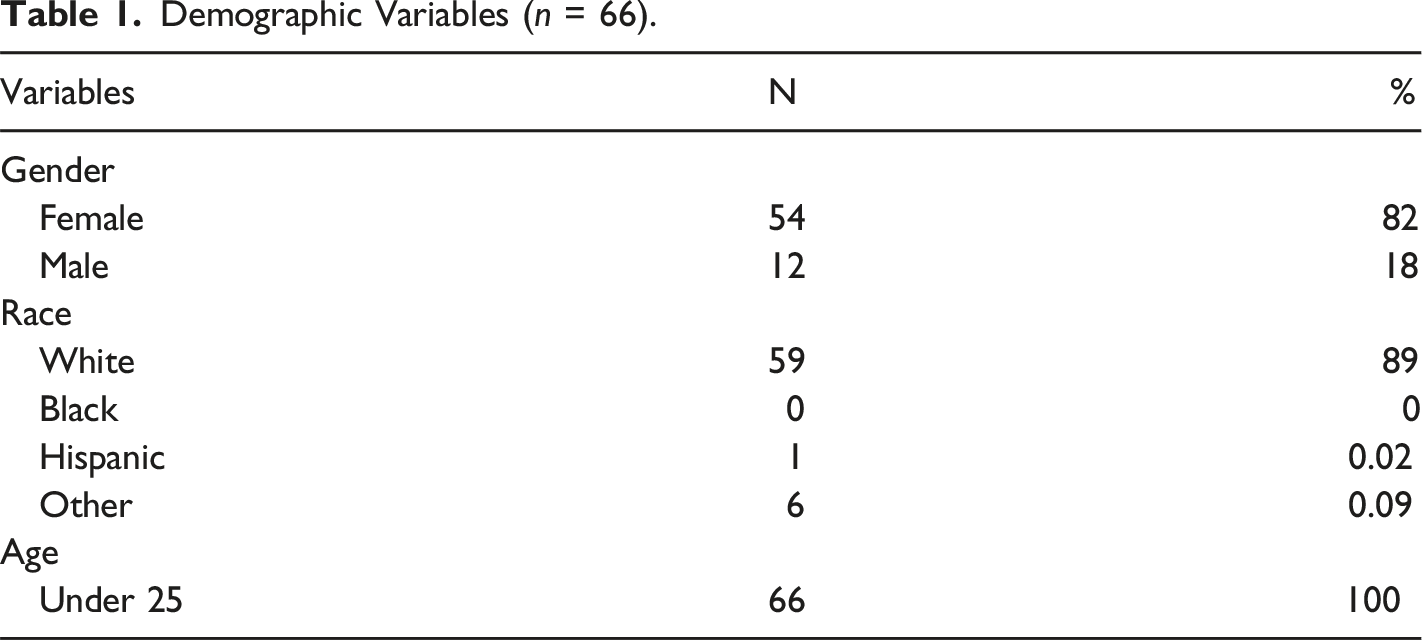
Sample
Demographic Variables (n = 66).
Who Deals With Death in Your Nursing Home?
Findings revealed that all staff members were involved to some extent in end-of-life care, and 92% of respondents highlighted this point. When expanding on who makes decisions surrounding end-of-life care, multiple respondents highlighted the role of the social worker, offering emotional and practical assistance to both residents and their families. In addition, religious services were mentioned as playing a role in supporting individuals' spiritual and emotional well-being during the end-of-life journey. Direct care staff, particularly those in the nursing department, and the Director of Nursing (DON), were highlighted by all respondents to play a crucial role in making decisions and delivering care to residents nearing the end of life, as evidenced by the following quote: “The primary people who made decisions regarding end-of-life care were the nurse managers, and the DON. They often made the decisions together about whether hospice was appropriate for the resident and discussed code status.” -Respondent 5.
As noted in the previous quote, hospice services were mentioned as a crucial service in end-of-life care, providing specialized care and expertise. Interestingly, several AITs stated that they had limited understanding of all the roles and tasks of the hospice agency with which the skilled nursing facility was contracted. This is important because the limited knowledge of Administrators-in-Training in nursing homes about the services provided by contracted hospice agencies could lead to inadequate patient care and communication challenges.
Additionally, the Infection Control Nurse Manager had a specific focus on addressing the unique challenges posed by COVID-19. Their expertise contributed to decision making related to end-of-life care, ensuring infection control protocols were followed to safeguard the well-being of residents, staff, and families. This is showcased in the following statement: “As for COVID-19 end-of-life care, our administrator and DON, in conjunction with our IDT [interdisciplinary team]worked to create a COVID-19 unit and ensure it was sufficiently staffed so our residents received the highest quality of care possible.” - Respondent 24.
What is Available at Your Facility for Training About Death, Dying, and Grief?
When analyzing the data from Administrators-in-Training, it was apparent that a significant number of students had not received training on death, dying, and grief within their facilities. Approximately 88% (58) of the AIT students answered “no” when asked about staff training in their facilities. One respondent (Respondent 4) shared, “I did not have any formal training in death management at my residency. I learned through the experiences of deaths in my family.”
Furthermore, the majority of respondents (87%) acknowledged their lack of personal training in death management and end-of-life care services. Respondent 18 expressed interest in seeking training, stating, “No, I have not. This would be a great thing to seek out and get training on though.”
A smaller group of respondents (8) mentioned having some form of training available at their facility, but they emphasized its minimal nature. Among these, specific types of limited training that were mentioned included online training courses (3 respondents), orientations (2 respondents), and a Chaplaincy rotation (1 respondent). Additionally, two respondents mentioned having access to cheat sheets or protocols related to death management.
These findings indicate that there is a significant gap in training for Administrators-in-Training regarding death, dying, and grief within their facilities. The expressed interest in seeking training highlights the recognition of the need for comprehensive and structured programs to equip administrators with the necessary knowledge and skills in this important area.
What Grief Support is Available to Staff at Your Facility?
Within skilled nursing facilities, it is concerning to note that a significant number of respondents (34 out of the total) reported the absence of formal grief support in their respective facilities. This indicates a lack of structured mechanisms to address the emotional needs of staff involved in end-of-life care. Furthermore, among those who reported some form of grief support, a striking 94% expressed the need for improvement in these support systems.
While chaplains and pastors were identified as individuals who provided support, it was noted that limitations existed in accessing their assistance. Respondent 10 emphasized that staff members were often hesitant to approach the pastors for grief support, suggesting a potential barrier to seeking help within this resource. On a positive note, some facilities did offer counseling services through employee assistance programs, behavioral consulting services, or support hotlines. Additionally, a few respondents mentioned social workers (4 respondents mentioned) and administrators (6 respondents mentioned) as available sources of support for staff and as individuals who assist families of residents after their passing.
What are Your Previous Personal Experiences With Dealing With Death?
When asked about their experiences with death, AIT’s shared various perspectives that showcase a range of experiences with death, from direct involvement in professional settings to personal experiences with friends or family members. Four respondents mentioned working as a caregiver (e.g., certified nursing assistant) in an assisted living or nursing facility previously and personally witnessing the passing of residents, thus providing them with firsthand experience of death in their professional life. A different respondent stated that they had only experienced the deaths of grandparents, which, although sad and expected, was supported by the presence of family. Two respondents acknowledged the significance of witnessing the grief and loss experienced by their friends or peers, highlighting the empathetic understanding they gained through these relationships. Such exposure to the experiences of others further contributed to their overall understanding and awareness of death and its effects.
What is the Impact of Your Previous Personal Experience on Dealing With Death at Work?
The experiences shared by Administrators-in-Training reflect the significant influence of their previous encounters with death on how they handle death in their work at nursing homes. Approximately 81% of the AITs acknowledged that their previous experiences with death shaped their approach to death in the workplace. One respondent (respondent 25) expressed a deep emotional connection, stating, “The connections you make with the members here are ones you will always remember. When they do end up passing, it makes me feel like I have just lost a grandparent of my own.” Some AITs mentioned feeling numb, yet unaffected in a negative way, indicating a coping mechanism: “Yes, but I feel like these experiences have made me numb. I don’t think that it really affects me in a negative way because I try to just continue on with the tasks that I need to get done.” – Respondent 48. Others noted heightened sensitivity and support for grieving staff due to these experiences: “I am more sensitive and supportive of staff who are grieving a loss as I have gone through similar experiences in my past.” – Respondent 2.
What Coping Strategies do you use When Faced with Death, Dying and Grief at Work?
AITs employed a range of coping strategies to navigate the experience of death, dying, and grief in their role as Administrators-in-Training. However, it is worth noting that some AITs acknowledged not having developed specific coping mechanisms for dealing with death, often due to their limited personal experience. Conversing with coworkers and providing mutual support emerged as a prevalent approach, as one respondent (respondent 10) expressed, “I mainly talk with my coworkers. I find it helpful to talk over these feelings with those that are going through the same thing. Also talking to other people in the industry who can relate.” Sharing positive memories and stories about the deceased residents was identified as another effective coping mechanism by several AITs, as respondent 51 stated, “When faced with death, dying, and grief at work, I like to reflect on all of the conversations and fun I had with that individual. It can break my heart to think about that, but it reminds me of how precious this life is.” These coping strategies highlight the importance of support from colleagues and the power of reflection and reminiscence in navigating the emotional impact of loss in their workplace setting.
Discussion
Our findings provide further support that patient deaths in a nursing home setting impact not only the residents' families but also the entire staff (White et al., 2021). It is crucial to recognize and support all members of the nursing home, from direct care staff to administrative personnel, as they navigate the emotional toll of patient loss and ensure their well-being.
Additionally, the involvement of different departments and professionals in decision-making was noted. Nurse managers, DONs, families, and residents were identified as primary decision-makers, discussing aspects such as the appropriateness of hospice care and code status. The interdisciplinary team, including nurse leadership, social services, therapy, and physicians, collectively addressed declining health situations and determined the inclusion of palliative or hospice services in the care plan. These findings highlight the significance of a team-based approach and the collaboration among various healthcare professionals to provide optimal end-of-life care (Fendler et al., 2015).
The results of our study reveal a clear disconnect between administrators and contracted hospice services, resulting in uncertainty regarding the actions and support provided by the hospice. Administrators often lack clarity regarding the specific responsibilities and protocols of the hospice, which can impede effective collaboration and comprehensive care provision. These findings align with the research conducted by Parker-Oliver and Bickel (2002), which also highlighted this issue in their examination of the nursing home experience with hospice services.
Furthermore, our results highlight a concerning lack of training in death, dying, and grief within the surveyed facilities, supporting previous research (Katz et al., 2001). The majority of AITs reported no training provided for staff or themselves, indicating a significant gap in knowledge and preparedness around the topic of end-of-life care. The absence of adequate training related to end-of-life care is a concern as it can have an impact on the quality of care provided to residents and the well-being of staff. The reliance on personal experiences or the limited resources mentioned in the quotes underscores the urgent need for comprehensive training programs. Facilities should consider implementing structured training initiatives that cover topics such as death management, end-of-life care, and grief support. By addressing this training gap, administrators and staff can gain the necessary knowledge and skills to provide compassionate and effective care to residents during the end-of-life journey, while also promoting their own emotional well-being.
The qualitative findings from this study also highlight a concerning limitation in the provision of formal support systems for staff dealing with grief (Whittaker et al., 2006), with the majority of respondents reporting the absence of such support. This suggests a critical gap in addressing the emotional needs of staff members during difficult times. However, amidst this lack of formal support, chaplains and pastors emerged as significant sources of support within the SNFs. These spiritual figures were identified as individuals who offer support to the staff, although it was acknowledged that some staff may not feel comfortable approaching them for grief support. This finding underscores the importance of recognizing and enhancing the existing informal support networks within SNFs to better address the emotional well-being of staff members during periods of grief. These resources provide avenues for staff members to seek support for their grief-related challenges.
The qualitative findings also provide insights into the impact of previous experiences with death on how Administrators-in-Training deal with death at work. The majority of students acknowledged that their prior experiences with death do influence their approach to dealing with death in their professional roles. These experiences were seen to enhance their empathy and awareness towards the grief experienced by family members and other staff. AITs also expressed that their personal experiences allowed them to better support staff members and families who are going through the process of loss. Some students noted that their prior encounters with death made them more comfortable with processing and grieving the death of a resident, while others felt that it helped them recognize death as a natural part of life. While most AITs believed that their previous experiences impacted their response to death and grief at work, a few students mentioned that these previous experiences brought about more negative responses. Depersonalization at work is a phenomenon that can occur in nursing home settings, where caregivers may detach emotionally from their work and the residents they care for (Abhicharttibutra & Tungpunkom, 2019). In this study, some Administrators-in-Training expressed experiences of depersonalization at work in nursing homes, particularly among students who had prior exposure to death in other work roles. They described feeling numb or emotionally detached, which can have detrimental effects on the well-being and care of the residents. Depersonalization may hinder the formation of meaningful relationships and empathetic connections with residents, potentially compromising the quality of care provided.
By drawing on their own coping mechanisms and empathetic understanding, AITs strived to provide compassionate care and support to both staff members and families during times of loss within the facility. The coping strategies mentioned by AITs highlight the importance of social support and reflection in dealing with death, dying, and grief at work. Informal support and engaging in conversations with coworkers was a common theme mentioned for dealing with death at work. This underscores the value of shared experiences and mutual support within the work environment. However, it is worth noting that some AITs acknowledged not having developed specific coping strategies or feeling unsure about their current approaches. This indicates the need for ongoing support and training to equip AITs with effective coping mechanisms.
Implications
The COVID-19 pandemic has had a significant impact on the findings of this study, as it served as the contextual backdrop for the data collection period. Throughout our analysis, the influence of the pandemic on end-of-life care and the well-being of staff was evident. The likelihood of experiencing patient deaths, the importance of interdisciplinary collaboration in decision-making, and the gaps in training and support systems were all amplified by the unique circumstances brought about by the pandemic. The findings highlight the urgent need for comprehensive and tailored training programs that address the complexities of providing end-of-life care during times of crisis. Furthermore, the pandemic underscored the importance of formal and informal support systems for staff members dealing with grief and emotional challenges. This gap in leadership development suggests a systemic deficiency in adequately equipping administrators with the necessary knowledge and skills to navigate the complexities of end-of-life care. Additionally, the absence of formal grief support programs within nursing homes further exacerbates the limitations faced by AITs. Only a small percentage of facilities reported offering any form of grief support, often relying on chaplains, pastors, or limited counseling options. This lack of formal support leaves AITs and staff members ill-prepared to address the emotional and psychological needs of residents and their families during the challenging end-of-life period. The gaps in leadership development regarding end-of-life care support and training underscore the urgent need for comprehensive and standardized programs that equip administrators with the necessary knowledge, skills, and support systems to effectively navigate the complexities of end-of-life care within nursing homes.
Limitations
The study sample consisted of AITs from two cohorts from a university with students in nursing home facilities in six states. The findings may not be representative of all nursing home administrators or facilities across the United States. The demographics of the participants, including age and racial composition, may also limit the generalizability of the findings. This underrepresentation could be attributed to various factors, including the demographics of the specific cohorts and the geographic regions from which the participants were recruited. Future research could benefit from exploring the perspectives and experiences of administrators in different locations to gain a more comprehensive understanding of the challenges and needs related to death, dying, and grief in nursing home settings across diverse contexts. Furthermore, this study includes a limited scope of training assessment; the study focused primarily on training related to death management and end-of-life care. Therefore, the assessment of training in the study may not capture the full range of knowledge and skills needed for effective end-of-life care. In future research, it would be valuable to include an exploration of participants' training preferences and needs, allowing for a comprehensive understanding of their experiences and the training they desire in light of those experiences. This additional insight could contribute to more tailored training interventions in the future.
Conclusion
This study sheds light on the limited understanding and preparation for dealing with end-of-life care among nursing home staff, particularly among facility management such as administrators. The experiences of Administrators-in-Training provide valuable insights into the challenges and gaps in their training and support related to end-of-life care in skilled nursing facilities. The findings highlight the need for enhanced education and training programs that specifically address the unique demands of providing quality end-of-life care in long-term care environments.
Footnotes
Author Contributions
The author would like to thank all the research participants for their valuable contribution.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Wisconsin- Eau Claire COB Summer Research Grant.
Ethical Approval
IRB Number: 202223791.