
Abstract
Research has given limited attention to family and friends bereaved by a drug-overdose death. To examine the ways in which stigma may uniquely impact the grieving processes of the bereaved, a thematic analysis of 35 semistructured in-depth interviews with family members and adult peers who lost a loved one to an overdose was conducted. Our findings demonstrate that the bereaved experience stigmatization after their loss. Specifically, respondents emphasized stigmatizing interactions with law enforcement, alienation from friends and family, a lack of social support, exchanges that enforced feeling rules, and being confronted by narratives of blame and individual choice as contributing to the degrees of stigmatization they experienced. Our findings highlight how bereavement becomes stigmatized to varying degrees through multiple interactions that have a compounding effect on mourners. We refer to this process as stigmatized bereavement, whereby the frequency of such interactions informs the degree of stigmatization the bereaved faces.
The opioid epidemic continues to surge through the American landscape as overdose deaths rates climb annually. Since 1999, over 600,000 Americans have lost their lives to an opioid overdose, prompting an outpouring of research on the biopsychosocial determinants of opioid use disorder, treatment efficacy and availability, public responses, and the societal impacts of the opioid epidemic. Additionally, research has also focused on familial experiences when a loved one actively uses opioids (e.g., Lander et al., 2013; McCann & Lubman, 2018). However, one area of discussion that has received far less attention has been the experiences of friends and family who have lost a loved one to an overdose.
Drug-related deaths (DRDs) have been documented as a unique form of loss – a “special death” (Dyregrov et al., 2019; Guy & Holloway, 2007; Lambert et al., 2021; Titlestad, 2021; Titlestad et al., 2020a; Valentine et al., 2016) – that receives different public responses than other forms of loss, prompting a unique bereavement process for the bereaved. One factor that makes this form of bereavement different from other losses is the process of the “death spiral” that the bereaved are confronted with prior to the loss of their loved one. Feigelman et al. (2020) describes the death spiral as a process whereby family members of people who use drugs experience a cycle of anticipatory grief while their loved one is using, mixed with hope during periods of sobriety, preceding a DRD. Upon the loved one’s death, the bereaved may experience symbolic loss, 1 sudden loss, and emotions ranging from anger to relief.
Feigelman et al. (2012) document the impacts of stigma on family members bereaved by a drug-overdose death (DRD), highlighting that bereaved family members often experience a lack of social support from peers and other family members following their loved one’s death. In examining the common experiences of the bereaved through a systematic review of the literature, Titlestad et al. (2021) identify three themes. First, that the bereaved go through an “emotional roller-coaster” preceding and following a DRD. The emotional roller-coaster is defined as the process in which “The family member experiences years of uncertainty, despair, fear, hopelessness, and powerlessness and following this, the drug user often dies” (p. 8). Specifically, the bereaved experience “the consequences of drug involvement, the fear of death, the trauma of death, complex and chaotic emotions, and guilt reflections” surrounding their loved one’s substance use and death (p. 7). Second, that the bereaved experience a “lack of understanding by the social world” whereby the bereaved experience stigmatization surrounding their loved one’s substance use, serving as a barrier to support and help-seeking behaviors. Third, that the bereaved engage in a unique process of “meaning making,” which refers to a broad range of help-seeking and memorialization efforts that the bereaved partake in throughout their bereavement (see Stout & Fleury-Steiner, Forthcoming). Other scholars have further explored the ways in which those bereaved by a DRD grieve and mourn, highlighting that the stigma surrounding drug use impacts and informs their bereavement process (Feigelman et al., 2011; Guy & Holloway, 2007; Nowak, 2015; Stout, 2022; Templeton et al., 2017; Titlestad et al., 2021; Valentine et al., 2016). Furthermore, those bereaved by a DRD often encounter stigmatizing language following their loss, in which blame is ascribed to the lamented (Dyregrov & Selseng, 2022).
Largely missing from our understanding of this unique form of bereavement is precisely how this stigmatization is experienced by the bereaved, and what impacts this may have on their grief and mourning processes. Even though the United States has the highest overdose death rate (World Health Organization, 2021), scholarship surrounding this topic has been relatively limited. Notably, most of the research on those bereaved by an overdose death has emerged in the Netherlands and the United Kingdom. While this research has been informative to our understanding of this unique form of grief, this research seeks to provide an account of the stigmatization of substance use in the American context. We begin by highlighting the importance of Goffman’s classic account of stigma as a social process in the context of substance use and DRD. Next, we turn to the extant research on the stigma surrounding drug use and DRDs.
Following the seminal work of Lindesmith (1968) and Goffman (1963), an imposing body of research shows how stigmatization is experienced as a social process by people who use drugs (e.g., Courtwright, 2009; Lindesmith, 1968; Lloyd, 2013). By contrast studies of DRD bereavement, tend to focus mostly on individual-level stigmatization. Following Link and Phelan (2001), we agree that the sociocognitive approach to stigma provides a limited understanding of stigma in the context of a “power situation that allows these processes to unfold” (2001, p. 382). Building on Goffman’s original framework, Link and Phelan, moreover, call attention to how “human differences are socially selected for salience” in a process of labeling individuals as stigmatized and call attention to systems of power: “Stigma is entirely dependent on social, economic, and political power – it takes power to stigmatize” (p. 375). Stigmatization thus can be understood as a dynamic process that occurs across all levels of interaction, rooted in cultural beliefs such as the criminalization of people who use drugs.
Families of drug users also experience a “courtesy stigma” (Guy, 2004; McCann & Lubman, 2018; Valentine et al., 2016). Courtesy stigma “involves public disapproval that is a consequence of associating with stigmatized persons” (Phillips & Benoit, 2013, p. 139). In the case of family members, courtesy stigma may occur as the direct result of their relational proximity to someone who is actively using drugs. However, little is known about how this courtesy stigma impacts those closest to people who use drugs following an overdose death. Courtesy stigma evokes many of the same interactional experiences as direct stigma – individuals may face various forms of discrimination, stereotyping, and prejudices based upon their proximity to someone who has died from a DRD. Individuals stigmatized by their substance use are often placed in the position of concealing or revealing their stigmatized identity (Matthews, 2019). Similarly, the DRD bereaved may choose to conceal/reveal aspects of their loved one’s death due to stigma (Stout, 2022). Beyond how courtesy stigma is negotiated by the DRD bereaved, however, it is important to examine how stigma may impact bereavement processes. In order to do so, it is essential to provide some definitional distinctions between grief, bereavement, and mourning.
Grief, bereavement, and mourning have often been used interchangeably in research on DRDs. However, there are important distinctions that can be made. Buglass (2010) notes the importance of these distinguishing these terms. Grief describes the emotional experiences of an individual following a loss (Homans, 2000). Mourning is the outward expression of the internalized feelings of grief (Buglass, 2010). Bereavement, on the other hand, refers to state of being after a loss, during which time grief and mourning occur (Buglass, 2010). Thus, while grief refers to individual affect, bereavement is more interactional and involves experiences after loss. Beyond semantics, these distinctions become important for the discussion of stigma and DRDs. Specifically, to understand the effect of stigma through an interactionist perspective it is important to make explicit how the individual’s sense of self is informed by perceptions of others. Furthermore, stigma consists of societal pressures that may inform the bereavement processes and interactions, but does not describe a state of emotion, such as grief.
Scholars have highlighted that when an individual dies from an overdose, the bereaved often experience a continuation of stigmatization regarding their loved one’s substance use, which may disenfranchise their grief (Valentine et al., 2016):
Disenfranchised grief can be defined as the grief experienced by those who incur a loss that is not, or cannot be, openly acknowledged, politically mourned, or socially supported. Isolated in bereavement, it can be much more difficult to mourn, and reactions are often complicated. It is important to recognize and try to meet the needs of those whose grief is not acknowledged by society, whatever the emotional or financial costs (Doka, 1999, p. 37).
Individuals who have lost a loved one to a DRD—a long stigmatized death in the U.S.—are disenfranchised from their grief (Valentine, 2016). However, the processes and interactions in which the bereaved experience such stigmatization are less understood. In this way, our contribution is influenced by expectations from Cassidy’s (2021) important research on how perinatal grief is disenfranchised “within the broader cultural values of death and dying” (p. 2). Drug addiction and drug-related deaths has long been stigmatized in American culture as the “bad choices” of individuals (Hari, 2015). Doka’s theory of disenfranchised grief and studies of DRD provide an essential framework for further understanding the role that stigma has on the bereavement processes for those who have lost a loved one to a drug overdose. Interactionist theory posits that interactions shape social meaning (Garfinkel, 1967). The present analysis thus takes an interactionist approach to understanding how the stigmatization of substance use in the U.S. impacts the bereaved.
Method
To explore how the stigma surrounding substance use impacts the bereavement of those who have lost a loved one to an overdose, 35 in-depth interviews were conducted with adult peers and family members who had lost a loved one to DRD. Drawing from existing qualitative DRD research conducted by Titlestad et al. (2020b), a grounded theory approach (Strauss & Corbin, 1994), whereby the data was coded for emergent themes used to further structure our theoretical frameworks surrounding stigma and bereavement, was taken in a reflexive thematic analysis of the data as outlined by Braun and Clark (2021a). Data collected was stored and analyzed using the qualitative analysis program NVivo 12. NVivo 12 provided a platform for organization of transcripts, and was utilized to perform inductive coding, identify themes, and allow for collaborative review throughout the analysis process (Jackson & Bazeley, 2019). We followed the “Standards for Reporting Qualitative Research: A Synthesis of Recommendations” (O’Brien et al., 2014) in structuring this article.
Recruitment
Recruitment for the study began through a partnership with a Delaware-based advocacy organization founded by DRD bereaved parents called atTAcK addiction. The capitalized letters represent the initials of the cofounder’s son who died from an opioid overdose. The organization was founded as an advocacy group to combat the stigmatization surrounding substance use. Although atTAcK addiction does not provide formal grief support services, at monthly meetings the bereaved come together to share their experiences. Beginning June 2018, both authors attended these monthly meetings to discuss our study and recruit potential recruitment. Snowball recruitment became an important recruitment technique, whereby participants would recommend others to participate in our study. Additionally, the first author of this study was involved in the recovery community of the area through their work at a long-term sober living program, allowing for ancillary participants to be recruited by displaying the recruitment flier on social media (Facebook, Twitter, and Instagram). We focused not on the number of participants we could recruit, but on the “information power” provided by our sample. Information power is defined by Malterud et al. (2016) as the relevant information a sample holds which results in less of a need for a greater number of participants.
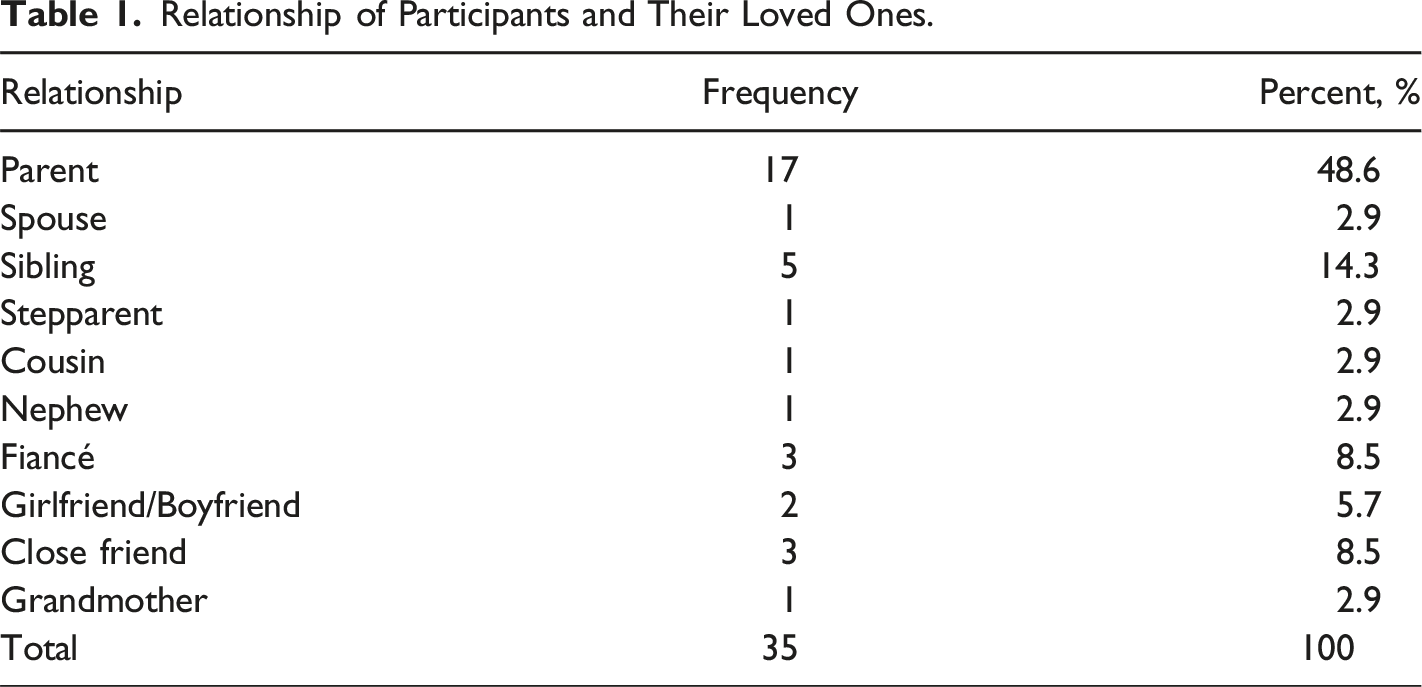
Relationship of Participants and Their Loved Ones.
Semistructured In-Depth Interviews
A semistructured interview guide was developed for the interviews. The guide consisted of six themes: (a) events leading up to the death; (b) interactions with others at the time of death; (c) reactions of others when learning of loss; (d) memorialization; (e) impacts of loss; (f) advise to others bereaved by DRD. These themes were created by the authors in collaboration with the Center for Drug and Health Studies at the University of Delaware, where the second author works as a faculty research associate. We began each interview with an open-ended question encouraging participants to tell us about their loved one’s history of substance use and the circumstances surrounding their death. To examine stigma, participants were asked to describe their interactions with others about their loss. Specifically, respondents were encouraged to discuss their interactions with emergency personnel, health care providers, family and friends immediately following their loss. The bereaved were then asked how others reacted to their loss, social support received from peers, support groups, and family members. We also asked interviewees to provide insight into what services they felt ought to be provided for DRD-bereaved individuals.
At the time of the study, the first author held a position at a long-term sober living program in Delaware, placing him in close proximity to the deceased. Accordingly, the second author conducted all interviews with any participants previously known by the first author. The second author interviewed 29 respondents, and the first author interviewed 6. Each interview was conducted in a private setting chosen by the participant (either at the participants home or at an office in the Center for Drug and Health Studies). 12 parents elected to be interviewed together, 1 interview was conducted with a mother and son, and 1 with a mother and fiancé, at the discretion of participants. Interviews were audio recorded and transcribed by a research assistant and the first author. These interviews consisted of 24 hours and 17 minutes’ worth of audio, and transcription of these interviews rendered 343 pages of single-spaced text.
Sample
Table 1 reflects the relationship of the bereaved to their loved ones. In total, 23 deceased persons were represented across the 35 interviews. All respondents indicated that their loved one died from an accidental overdose. The average age of the decedent is 32. 74.3% of decedents were male, and almost all were white. 14.5% of respondents in our sample witnessed the overdose of the deceased, and 17.1% were present when the body was discovered. 43.6% of participants knew of previous non-fatal overdoses of the deceased and 57.4% reported that the deceased had no prior history of non-fatal overdoses. Our sample consisted of included 23 females and 12 males. The average age of respondents was between 56-65 years old, with 17 of our participants being parents to the deceased. Our sample consisted primarily of white, upper-middle-class respondents. Time since loss ranged from 6 months to 7 years (M = 32 months).
Analysis
We analyzed the data using a reflective thematic analysis (Braun & Clark, 2021a; Titlestad et al., 2020b). Braun & Clark (2021a) outline six phases for reflective thematic analysis: (1) familiarization with data; (2) coding; (3) developing themes; (4) reviewing initial themes; (5) defining and naming themes; (6) producing the report. Multiple readings of transcripts were conducted by both authors. We noted emergent themes to create codes representative of these themes that were analyzed using NVivo 12. The analysis of identified themes was conducted by the first author through continual deliberation with the second author. Braun & Clark (2021b) note that “Coding quality in reflexive [thematic analysis] stems not from consensus between coders, but from depth of engagement with the data, and situated, reflexive interpretation” (p. 209). Thus, the discussions between both authors bolstered trustworthiness. The final themes for analysis were determined by both authors collaboratively (Braun & Clark, 2021a; Titlestad et al., 2020b).
Statement of Reflexivity
The first author worked at a sober living program during this study, which placed him in close relational proximity to the deceased. While the first author knew many of these individuals, the focus of this study was on the experiences of family members and friends. To maintain objectivity, author one frequently discussed preconceptions and findings with author two. There has been significant debate on the role of insider/outsider status regarding reflexivity in qualitative research. Ultimately, insider/outside status can be fluid given the various interactions and contexts and may acts as a “double-edged sword” (Mercer, 2007). While this status allowed for fruitful recruitment, to avoid potential biases, findings and interpretations were compared to prior research and well-established theoretical frameworks.
Ethical Considerations
Oversite for this project was conducted by the University of Delaware institutional review board. All participants signed a written informed consent outlining potential risks, the purpose and methods of the study, and confidentiality. Pseudonyms were created for each participant and their loved ones, and all revealing information was redacted. All data was deidentified and stored in a secure research cloud server at the university. Participants received a $25 gift card for participating in the study.
Findings
After losing a loved one to a DRD, respondents reported multiple interactions in which they experienced stigmatization. Our findings indicated five primary themes: Interactions with police; experiencing alienation; facing a lack of social support; enforcement of feeling rules; and being confronted by narratives of substance use and/or death being a choice that was made by the lamented.
Interactions with Police
For many participants, the first interaction following their loved one’s death was with law enforcement, either through police informing the bereaved or by the bereaved contacting emergency services upon discovering their loved one. While not all interactions with law enforcement were negative, for some, this was a stigmatizing experience. The “war on drugs” has frequently utilized stigmatizing imagery and labels towards individuals with substance use (Hari, 2015; Kruis et al., 2020). Police have been shown to make moralizing judgments that demoralize and otherize people who use drugs (Murphy & Russell, 2020).
Two parents described the stigmatizing interaction with police following their son Nolan’s death. Nolan was in recovery from alcoholism and sober for multiple years with no history of opioid use. However, one month after being prescribed opiates for a medical procedure, he was found dead. Below is an account of Patrick and Penelope’s interaction with police officers at the time of Nolan’s death: Patrick: …I stayed until they [paramedics] took him out in a body bag. Penelope: His girlfriend, Lily, felt like the police wanted her to come inside [Nolan’s apartment]. She was really upset. She said they treated her like a heroin couple. She didn’t even do drugs. Patrick: She hardly drank. She would have a glass of wine with dinner when they went out, but that was about all. Penelope: She said they treated her terribly. Patrick: She was totally shocked that Nolan had done this. . . The police questioned me. The officer was like, “So, he’s a long-time user?” And I said no, as far as we know, this is the first time he used it. And he goes, “That’s impossible. He’s probably been using it a long time.”
This interaction is telling in a few ways. First, Nolan’s girlfriend experienced courtesy stigma by being labelled as a user, receiving interrogation rather than support. Second, the officer expressed a stereotyping view that only long-term user’s overdose. Lastly, the father further describes law enforcement as unsympathetic.
Jeremy, and his girlfriend, Hailey, had both been sober for two years. One night after she had not arrived home for dinner, Jeremy went searching for her, eventually finding her overdosed in her car in a shopping center parking lot. Jeremy describes how his past interactions with police as a drug user, and the courtesy stigma of being in relational and physical proximity to an overdose, shaped his interactions with law enforcement: [The] county police department showed up first…They looked at us like scumbags…It’s like one of those things like you [the police] haven’t seen me in two years, yet you’ve seen the hundred-pound crackhead I was. You see me in my own car sober as fucking dirt trying to take care of my girlfriend, and you’re sitting here still calling me a junkie.
Jeremy’s account highlights multiple ways in which he experienced stigma. First, he reflects on a calloused indifference by officers towards the departed and the bereaved upon their arrival to the scene. Second, he highlights that the stigmatizing label of “junkie” was still readily ascribed by officers even though he was sober and seeking life-saving care for Hailey.
Sarah pointedly stated that the cops were unfriendly towards her when it came to her son, Marshall, proceeding his death. These prior interactions, whereby her son was labeled as a criminal, informed her experience with law enforcement when they arrived at her house to conduct the death investigation. She recalls the following: I said to them, “Could you please be nice to me? My son’s dead.” Because they were never nice…I believe they were out to get him over stupid stuff. Just because they knew he was an addict. My son didn’t rob stores or hurt people, but [the police] would follow him and arrest him for crossing the railroad tracks because that’s against the law…They would throw him in jail for a couple of hours just to break him. And when he broke probation, they came to my house looking for him. They were so disrespectful coming to my house, acting like he was a criminal. He wasn’t a criminal...And I’ll never forget that...
Sarah was worried that the police would treat her with animosity rather than sympathy. The stigmatization and criminalization experienced prior to her son’s death fostered negative expectations at the time of Marshall’s death.
Alienation
Stigma itself creates separating categorizations of “us” versus “them” (Link & Phelan, 2001). There is a long history of alienation and exclusion of people who use drugs in society (Courtwright, 2009; Hari, 2015). Participants described how stigma surrounding substance use is often a profoundly alienating experience. Specifically, family and friends actively alienated the bereaved as stigmatized outsiders versus “everyone else.” In discussing the loss of her fiancé with someone, Rose recalls an exchange that left her feeling misunderstood and alienated: Someone asked me, “How could you love an addict?” I wanted to [put] my hands around their throat… “Are you kidding me? Do you know anything about this population? They’re incredibly traumatized and incredibly hurting. They need people like me to love them.” I didn’t love an addict. I loved a man who struggled with some demons.
The otherizing label of “addict” in this exchange not only angered Rose but dehumanized her loved one and her love towards him.
Participants recounted alienating experiences by friends and family that were more overt. Jennifer recalled how her family abandoned her after her sons passing. Jennifer describes, through tears, how her family did not provide any support after she lost her son: I don’t think I’ll ever forget that. If my sister’s [children] died, my mother would have gotten a ride and been over there for her. But nothing for me. Why? Because Eugene was an addict? Because I had an argument with my family members? They need to let that go…I couldn’t believe it [crying]
Jennifer further noted that her other living son no longer speaks to her following the death of his brother, and that at the funeral, “He was outside the funeral home [telling] people that I was a bad mother and [that I] don’t pay attention to my grandkids.” Jennifer’s experience is emblematic of the alienating stigmatization experienced by the bereaved. Specifically, stigmatization leaves the bereaved with feelings of isolation from family members. The grief of losing a loved one to an overdose death is compounded by the grief experienced by the loss of living family members who may blame the bereaved.
Another mother, Kathleen, who lost her son, Tanner, describes how the lack of support by her mother had a negative impact on their relationship: My mother didn’t even come to my house for fifteen days after he died. She finally called me, and asked, “What are you doing?” I said, “Well, I’m writing Tanner’s obituary.” I was crying and the only thing she said to me was, “Well, don’t include me or dad in the obituary.” And I said, “Oh really?” And she said, “Yeah, no, don’t, please don’t include us.” And I said [in a stern voice], “Okay, mom, you don’t want to be included in my son’s obituary? You won’t be included in mine either.”
Kathleen’s mother sought to distance herself from the stigma of Tanner’s substance use. Interactions such as this highlight the unique way stigma surrounding substance use creates alienating experiences for the bereaved.
Other participants recounted how they were, at times, blamed for their loved one’s death. Such experiences further alienated the bereaved from prosocial support. Our participants experienced alienation in three primary ways. First, the bereaved experienced exclusion from social networks; Second, individuals were isolated from their family; Third, blame was placed on the bereaved. Narratives such as these are rooted in the longstanding cultural stigma of substance use as a personal or moral failing (Courtwright, 2009; Dyregrov and Selseng 2022). This ideology of individual responsibility undermines the bereaved’s need for social support (Doka, 1989, 1999; Feigelman et al., 2011, 2012).
Lack of Social Support
In addition to experiencing alienation from friends and family, the bereaved often felt that they could not turn to various services (such as support groups) either. Alienation described above reflects stigma experienced through interactions. However, stigma was also internalized by the bereaved, serving as a barrier for their seeking of support. As Tan et al. (2020) observe: “Stigma affects an individual’s help-seeking intentions and behaviors, insomuch that a person considering treatment may be discouraged from doing so due to the anticipation of potential discrimination” (p. 2).
Some respondents chose to reveal the manner in which their loved one died, while others engaged in label avoidance by concealing the nature of the death. Corrigan and Wassel (Corrigan & Wassel, 2008) define label avoidance as “dodging a group altogether to escape the negative effects of public stigma and self-stigma” (p. 44). One mother stated, “I wanted to hide the fact that he had died of an overdose, because then they’d know he had a drug problem. And not everybody knew that we battled with the drug problem. I felt very vulnerable. It was very hard.” Concealing the nature of the death in this way further highlights the impact of stigma on the bereavement process. In an attempt to avoid stigmatization, some participants felt the need to hide how their loved one died rather than potentially receiving communal support.
Fear of stigmatization served as a barrier for some respondents seeking support from support groups: Penelope: Somebody told us about [a grief group] for people who have lost a child. But we were afraid. I remember talking to our counselor [who] said, “you could go to a meeting and be the only [parent] that lost somebody to drug addiction.” I don’t know that I ever would say that people look down on you… Patrick: [They may believe that those who died from an overdose] did it to [themselves]. Penelope: They did it to themselves. It’s not like we lost our child to cancer or an accident…I think that’s what kept me from going through.
Penelope and Patrick believed that the stigmatizing narrative of choice surrounding substance use would prevent them from receiving support. Notably, in this exchange, they both disenfranchise their own grief as well by comparing the nature by which their son died to other “more acceptable” forms of loss. As Titlestad et al. (2021) observe “Along with stigma comes social isolation, which is internalized as an intense feeling of shame” (p. 9).
Feeling Rules
Prior research on drug overdose deaths highlights that this type of loss does not align with the cultural narrative of “time healing all wounds” (Titlestad & Dyregrov, 2022). Kathleen, who experienced alienation from her mother following Tanner’s passing discussed above, reflected on how people told her the grief would subside after the first year: [W]e’re not supposed to mourn. You’re supposed to get that first year. And everybody tells you, “get through all those firsts.” [I]t’s like, “oh, okay, so if I get through it, I [will] feel like the weight of the world has been lifted off my shoulders?” Well, I can tell you, that second year was horrible.
The bereaved may experience otherization through message such as this, which signify that they are not grieving appropriately or “moving on” fast enough, causing the bereaved to feel unsupported in their process.
Feeling rules (Hochschild, [1983] 2012) and grief rules (Doka, 1989) have been observed as a way in which individuals are disenfranchised in their grief. In some instances, these feeling rules of what the bereaved ought to feel, and when, acted as a barrier to support. One mother who lost her son described how her husband – the stepfather of the deceased – left her feeling unsupported in her grief due to his enforcement of feeling rules: [B]ecause he lost both of his parents, he doesn’t understand. . . [H]e feels as though I should be better by now . . . I should be okay but, [losing a child is] not the same [as losing your parents], and it will never be the same . . . If I lost my parents, I would get past that because they are in their late sixties and early seventies - you expect it. You don’t expect to lose your child, especially at the age of thirty.
Feeling rules and expressive norms convey the stigmatizing message to the bereaved that they are grieving inappropriately and that the nature of their loss does not align with normative scripts. Otherization is created by the normative feeling rules creating categories of “us” versus “them”. Specifically, those who grieve in the ways constructed as normative are accepted as insiders into the sentimental normativity. Adversely, those who receive messages that their grief is expressed inappropriately or has not been overcome in an acceptable manner or timeframe, may have an outsider experience in this grief. Such enforcement of feeling rules and expressive norms is something widely expressed in society and is not limited to DRD-bereaved. However, when placed in the context of DRD, such interactions proved to be stigmatizing when they occurred in connection with the other forms of stigmatization discussed above.
Choice Narratives
Blame is often placed on people who use drugs as responsible for their substance use, and in turn, deserving of social ostracization (Lloyd, 2013). Valentine et al. (2016) highlight how this may impact those bereaved by DRD: The experiences of those who are grieving so-called self-inflicted deaths can be obscured by commonly held assumptions and stereotypes… along with the life of the deceased, the grief of those left behind was also devalued due to their being considered in some way complicit in the death. (p. 286)
In reflecting on her friend and coworker Erica’s death, Maggie’s account evokes the cultural narrative of addiction as a sign of personal weakness: [W]hen people talk about heroin addicts in a derogatory fashion I wanna say, “Do you have any idea what you’re talking about?” It bothers me that people think it’s a weakness.
This statement highlights both the “derogatory” ways that those with substance use are commonly discussed and how such statements focus on the ideas of individual choice. Some respondents recalled that they experienced interactions that moved beyond just narratives of choice, to hearing accounts that people who use drugs deserve to die. As Fran recalls: My anger flares when people feel like addicts deserve death, that’s what gets me. It’s okay if they don’t understand [addiction], but when they flat out say they deserve to die or something like that, I can’t take it. I get angry.
Messages such as this are another arena in which bereavement becomes stigmatized, for rather than receiving compassion or support, the bereaved are told that their loved one deserved to die, and in turn, that they deserve to be bereaved.
Discussion
Participants in our study were asked to describe positive and negative interactions with others following the loss of their loved one. These qualitative accounts illuminate how stigma is experienced by the bereaved across multiple interactions and settings. Bottomley et al. (2023) find that factors preceding the loss of a loved one to a DRD “predict levels of stigmatization, guilt, and shame in the aftermath of an overdose death” (p. 17). Our findings provide some qualitative support to this important empirical research. Specifically, this research shows how frequent and reoccurring stigmatizing interactions experienced by the bereaved had a compounding effect. Meaning, that as the bereaved experienced more stigmatizing interactions, there were greater negative effects of stigma observed. Various signals that their loved one was marginalized because of their substance use were often conveyed to the bereaved through these interactions, indicating that the loss experienced by the bereaved is less legitimate compared to other forms of loss. Research on stigma typically has focused on one stigmatized characteristic or examined stigma in a particular setting. The findings here highlight how the DRD-bereaved experience a stigmatizing process involving a multiplicity of experiences.
Prosocial support and interactions have been shown to aid individuals in their grieving process (Cacciatore et al., 2021). In the case of the DRD-bereaved we interviewed; however, healthy grieving may be more challenging. Specifically, our findings indicate that individuals feel—often on multiple occasions—alienated in their grief and judged by others. We refer to this process as the stigmatized bereavement; a series of interconnected interactions that increase the degree of stigmatization experienced by the bereaved, which impacts their bereavement and mourning processes. Respondents described experiencing stigma through their interactions with law enforcement, by being alienated by friends and family, in feeling ostracized from support services, by feeling rules, and through choice-based narratives. As the DRD-bereaved experienced more of these interactions across various settings, they describe stigma as not a static event, but a multiple events and interactions that may have a compounding effect.
These findings support an interactional approach to the study of stigma in which the “elements of labeling, stereotyping, separation, status loss, and discrimination occur together in a power situation” (Link & Phelan, 2001, p. 377). Our qualitative analysis highlights how stigmatized bereavement might extend the theory of disenfranchised grief (Doka, 2002) by demonstrating the ways in which stigma further alienates the bereaved. Goffman (1963) describes the way in which stigma creates a “spoiled identity” for individuals that is shaped by, and subsequently informs, interactions. Our findings indicate that being bereaved by a DRD serves as a stigmatizing “mark” on individuals, which shapes subsequent interactions. Beyond courtesy stigma, the identity of the bereaved as a person worthy of healthy grieving is attacked. Figure 1 below highlights this process. Stigmatized bereavement process.
Limitations
Future research may also be guided by exploring the limitations of this study. First, our sampling was limited to the Mid-Atlantic region. Respondents were predominately white and upper-middle class. Future studies should explore the experienced of the bereaved in other locations and across more representative groups. Second, the findings presented above provide a rich qualitative analysis. However, exploring stigmatized bereavement through more robust quantitative methods is needed as well. Lastly, gendered interactions were not explored in this analysis, but were present across interactions. We encourage future studies to explore the ways in which stigmatized bereavement may be gendered.
Conclusion
Our findings demonstrate that stigma uniquely impacts individuals bereaved by a DRD. Specifically, stigma surrounding substance use informs the interactions the bereaved experience following the loss of a loved one to an overdose. Participants in our study experienced stigma through their interactions with law enforcement, friends and family, and broader cultural expectations on how they are supposed to feel about their loss. Stigmatized bereavement can provide a deeper understanding of the self-concept of the bereaved. Future research may utilize the stigmatized bereavement process to further explore how interactions may influence the grief and mourning practices of DRD-bereaved. Furthermore, this model may be assessed in the context of other deaths that may also be stigmatized. Indeed, recent research by Bottomley et al. (2023) finds no significant differences in the levels of stigmatization experienced by individuals bereaved by an overdose death as compared to those bereaved by a suicide.
Further attention needs to be given to support for the DRD bereaved. Our findings highlight that stigmatization can, and does, occur in grief support groups. We suggest that counselors and group facilitators ought to be more aware of the unique experiences of DRD bereaved. Notably, these individuals need a multitude of individualized support services (Stout & Fleury-Steiner, Forthcoming). In demonstrating the stigmatization experienced by the bereaved by law enforcement, awareness and sensitivity training could help officers respond to such deaths in ways that are more supportive of the needs of the DRD-bereaved.
Footnotes
Acknowledgements
We would like to thank the reviewers for their insightful suggestions and comments. We are grateful to atTAcK addiction for their unyielding support of the Overdose Bereavement Project. We also thank Dr. Tammy Anderson, Dr. Jennifer Carrano, Dr. Valerie Earnshaw and Center for Drug and Health Studies director, Dr. Christy Visher, at the University of Delaware for their feedback in the early development of this research. Additionally, thank you to Dr. Feigelman (Nassau Community College), Dr. Titlestad (Western Norway University of Applied Sciences), Dr. Stroebe (Utrecht University), and Dr. Dyregrov (Western Norway University of Applied Sciences) for their invaluable guidance and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.