
Abstract
The aim of this study is to determine the effect of the birth story of individuals on personality traits and death anxiety. This descriptive and analytical research was completed with 1,635 people who participated voluntarily. The study data were collected with the Personal Information Form, Cervantes Personality Scale (CPS), and Abdel-Khalek Death Anxiety Scale (ASDA). The research sample is average means 31.63 ± 11.04 years, most of the female (72.7%) and married (54.6%). In our study, it was observed that women’s death anxiety was higher than men’s. Our study found that individuals born by caesarean section had greater neurotic personality traits, emotional stability/neuroticism score averages, and death anxiety scores compared to individuals born vaginally. In the model made with multiple regression analysis, birth type did not significantly predict death anxiety, while sex and emotional stability/neuroticism personality trait significantly predicted death anxiety.
Introduction
The act of birth, which is a natural part of life, is a unique event and an important factor that leaves permanent traces in the memories of women and their children (Aktaş Reyhan & Dağlı, 2022) and affects many processes of life. The birth story is a subjective event affected by social, environmental, political, and structural factors intertwined with physical and psychological processes (Aslan, 2016). In the literature, negative birth stories such as preterm labour, difficult delivery, need for surgical intervention at birth, small foetus according to the gestational week, low birth weight, and newborn with low APGAR score (Çalık & Aktaş, 2011), as well as positive birth stories such as easy birth, normal birth, painless birth can be found.
While vaginal birth, which provides the opportunity to create positive birth stories, is a birth method that suits the physiological structure of the woman, caesarean birth is a birth method that involves surgical intervention. Caesarean birth can be perceived as traumatic because it involves negative risk factors for both the mother and the baby (Vasile et al., 2023). For many years, therapists have believed that the traumas experienced at birth will continue to haunt a person throughout their lives until these traumas are understood and resolved (Straussner & Calnan, 2014). Otto Rank, a colleague of Freud’s, proposed that the majority of psychological issues could be understood as responses to the traumas of birth (Pizarro Obaid, 2012). For instance, it was revealed during therapy that the patient who complained of chronic coldness was born in a particularly cold environment at the time of birth. The findings of the study conducted by therapist Chamberlain (1999) indicated that despite the prevailing belief that infants lack the capacity to recall the events surrounding their birth, hypnosis can facilitate the recollection of birth memories (Chamberlain, 1999).
The perception of the birth story as traumatic may cause negative effects on the child’s life in the long term (Yılmaz et al., 2021). In a study, it was found that children and adolescents born by caesarean section were more likely to experience anxiety disorders later in life, especially if the caesarean section was not planned (Ståhlberg et al., 2022). In another study, it is thought that perceived loss of control and emotional problems in mothers who had caesarean section may affect their attachment to their children and may be a factor in anxiety disorders (Lobel & DeLuca, 2007). It is reported in the literature that attachment styles have an important effect on personality development (Anlı, 2019). Since the type of birth, whether caesarean section or vaginal, affects the duration of contact between mother and baby; it is thought that it may delay the positive development of the relationship or attachment between mother and baby and negatively affect attachment because it causes separation.
Death, like birth, is an inevitable part of life. Although death is a natural process accepted by society, it is a difficult reality to accept compared to birth (Turhan, 2021). Individuals perceive death in different ways. According to Freud, the founder of psychoanalytic theory, the concept of death is associated with two drives, the death instinct and the life instinct. The representation of these two concepts is based on the archetypes in Greek mythology that first defined these two drives, Eros (the life instinct) and Thanatos (the death instinct). Eros, our life drive, is what keeps us alive. We continue our lives with an impulsive sexual drive to pass on our genes to the next generation. It can be said that the act of birth or childbirth is related to the basic impulses of human beings when viewed in the context of producing new lives and mediating the transfer of our genes to the next generations. Klein, on the other hand, argues that the representation of death is located in the unconscious. In the Kleinian perspective, destructiveness corresponds to the representations of evil and oppressive objects (Terbaş, 2021). All of our behaviors that we harm or may harm ourselves stem from the unconscious death drive. We can see destructiveness not only as harming others, but also within ourselves when we cannot reach satisfaction. Whether death is considered as a condition that has no representation in the unconscious from Freud’s point of view or as a condition that arises from our unconscious from the Kleinian point of view, every being who comes into the world brings the fear of death and a significant part of his/her personality traits from birth, even if he/she does not consciously recognize death and himself/herself. At the moment of birth, the baby is confronted with a multitude of stimuli without adequate defences, and the anxiety caused by this situation is the first example of anxiety in later life. The first reaction to the unexpected change after birth is in the form of symptoms such as breathing, crying, rapid heartbeat, etc., and the symptoms of anxiety in adult life are similar to these symptoms at the time of birth (Geçtan, 1998). Existential theorists have suggested that the main source of anxiety is death anxiety (Zorlu & Ünübol, 2018).
While death is a source of anxiety for some, it is a factor that reduces stress for others (Koç, 2002). Death anxiety, a condition that causes biological and psychological health problems in individuals, causes the person to experience uneasiness, fear, or anxiety related to death (Saleem & Saleem, 2020). Being aware of the path to acceptance of death and finitude can result in a depressed mood (Gedik & Bahadır, 2014). In some people, fear of death can limit life satisfaction and happiness (MacLeod et al., 2016). There are many factors affecting death anxiety. Although there is no direct study showing that birth history affects death anxiety, a study found that the risk of death due to chronic disease was higher in people born prematurely (Luu et al., 2016).
Each individual’s reaction to death anxiety and coping strategies are different. Therefore, it should always be taken into consideration that each individual is unique and unique. One of the features that make people unique and distinctive is their personality (Aytaç, 2004; Weinberg & Gould, 1999). Bandura (1986), in his Social Learning Theory, mentioned that a person’s character develops through both nature (genetic, innate) and nurture (environment). It has been reported that neuroticism and extraversion personality structure, which are personality traits that begin to be shaped by the birth process, especially affect the health status of the individual (Yılmaz et al., 2021). Neuroticism reflects the degree of negative emotions and pessimism experienced by the person in general and is generally associated with low self-esteem, depression, and anxiety, while extraversion is associated with positive emotional experiences and an optimistic outlook on life. The other end of the extraversion personality structure is known as introversion. Individuals with this trait are usually lonely and have longer periods of experiencing negative emotions (Blais et al., 2016). It is also known that personality can remain the same or change over time (Bandura, 1986). In this context, birth story may be one of the characteristics that affect personality. There are no studies on this subject in the literature. However, it is stated that the intestinal microbiota of the newborn differs negatively at birth and this negativity continues in the following life periods (Demir, 2023). A study also shows that there are different bacteria and metabolomes associated with each personality trait (Boolani et al., 2022). In the literature, it has been proven that there is a positive association between among personality traits neuroticism and death anxiety (Frazier & Foss-Goodman, 1989; Pradhan et al., 2022; Yıldız & Bulut, 2017; Özdemir et al., 2021).
In this context, this study is the first study planned to determine whether birth history and type of birth are effective on personality traits and death anxiety of individuals. Therefore, it is thought to contribute to the literature.
Research Questions
Several research questions have been formulated to investigate the effect of birth stories on personality traits and death anxiety. These research questions are designed to gain insight into how one’s birth story can impact their personality and level of death anxiety. 1. Does the birth story or type affect personality traits? 2. Does the birth story or type affect death anxiety? 3. Is there a relationship between the birth story and both personality traits and death anxiety? 4. Do socio-demographic characteristics (age, gender, marital status, employment status, etc.) affect death anxiety?
Methods
Participants
The population of the study consisted of male and female individuals over the age of 18 living in Türkiye. The survey link was shared via social media and WhatsApp through free cross-sharing and paid support campaigns. Participants who clicked on the link were then provided with detailed information about the study, namely a description of the objectives, inclusion criteria, and the ethical statement of the study. Participants were informed that their participation was voluntary and anonymous. The sample of the study consisted of men and women who met the sampling criteria and agreed to participate in the study. The t-test analysis in the G*power statistics program calculated the study sample number as 1,540, 414 males and 1126 females, based on a 0.01 error level, 99% power, and 0.28 effect (Aydin Ozkan & Kucukkelepce, 2019). The research data was completed with 1,635 people, 446 men and 1189 women. Post-hoc power analysis of the study was calculated with the G*Power 3.1.9.7 program (Faul et al., 2007). When the effect size was 0.68 and alpha 0.01, the power of the study was found to be 1.0 (%100). According to this power level, the sample size was found to be sufficient.
Data Collection Tools
The data of the study were collected with the Personal Information Form, Cervantes Personality Scale (CPS), and Abdel-Khalek Death Anxiety Scale (ASDA).
Personal Information Form
In this form prepared by the researchers, demographic characteristics of the participants such as age, sex, educational status, marital status, employment status, whether they have a chronic disease, whether they have any psychological disorders, their breastfeeding status, death of a family member, and their birth stories. The content of birth stories included a range of questions pertaining to various aspects of the birthing process. These included questions regarding potential complications, such as intervention during labour, the speed of labour, the possibility of miscarriage during pregnancy, the mode of birth (vaginal or caesarean section), and any issues with the mother or baby during the birthing process.
Cervantes Personality Scale
Developed by Castelo-Branco et al. (2008) and adapted into Turkish by Demirgöz and Hotun (2011), the scale is a six-point Likert-type scale comprising 20 questions. Extraversion/introversion (7 items: 1st, 4th, 7th, 10th, 12th, 15th, and 18th), stability/neuroticism (7 items: 2nd, 5th, 8th, 11th, 13th, 16th, and 19th), and consistent/inconsistent (6 items/control: 3rd, 6th, 9th, 14th, 17th, and 20th) subscales are used to determine personality traits. This scale includes extraversion/introversion and emotional stability/emotional instability (neuroticism), two basic personality traits, along with the sub-dimension of being consistent/inconsistent. The consistency/inconsistency sub-dimension was designed to evaluate the answers given to the other two dimensions and is not a personality factor. Each item on the scale is scored from zero to 5. As the score from each subscale decreases, extraversion, emotional stability, and consistency characteristics increase. Scores range from zero to 35 points in extraversion/introversion and emotional stability/emotional instability (neuroticism). In the study of Bal and Sahin (2011), Cronbach’s alpha values were 0.97 for the extraverted/introverted dimension; 0.81 for the emotional stability/neuroticism dimension; and 0.71 for the consistent/inconsistent dimension (Demirgöz & Hotun, 2011). For this study, Cronbach’s alpha values were 0.68 for the extraversion/introversion dimension, 0.85 for emotional stability/neuroticism, and 0.74 for consistent/inconsistent. In addition, the mean scores of participant CPS consistent/inconsistent sub-dimensions was 9.91 ± 5.34.
Abdel-Khalek Death Anxiety Scale
Developed in Arabic and English by Abdel-Khalek (2004) and validated in Turkish by Sarıçiçek Aydoğan et al. (2015), the five-point Likert-type scale (1 = none to 5 = very much) consists of 20 items (Abdel-Khalek, 2004; Saricicek Aydogan et al., 2015). Scores can vary between 20 and 100 points; a higher score indicates a higher level of death anxiety. In the study of Sarıçiçek Aydoğan et al. (2015), the scale Cronbach alpha value was 0.86. The Cronbach alpha value for this study was calculated as 0.94.
Ethical Procedure
Ethical approval to conduct the research was obtained from the Ethics Committee of Sakarya University (no: E-61923333-050.99-197543, date: 8 Dec. 2022). After the participants were informed about the purpose and method of the research, their consent was obtained, and they were asked to complete the form. The names of the participants were not requested for the confidentiality of the data.
Statistical Analyses
The SPSS 16 program was used in the analysis of the study data. Number, percentage, mean, standard deviation, independent t test, one-way analysis of variance (ANOVA), and Pearson correlation analysis were used in statistical analysis. To measure significant difference after ANOVA analysis between groups (due to equal variance homogeneity; p > .05), the post-hoc Gabriel test was used in groups with close n numbers, and Hochberg’s GT2 test in groups with different n numbers. Modelling was done with multiple regression analysis (Chatterjee, 2006). The results were evaluated at 95% confidence interval and p < .05 significance level.
Results
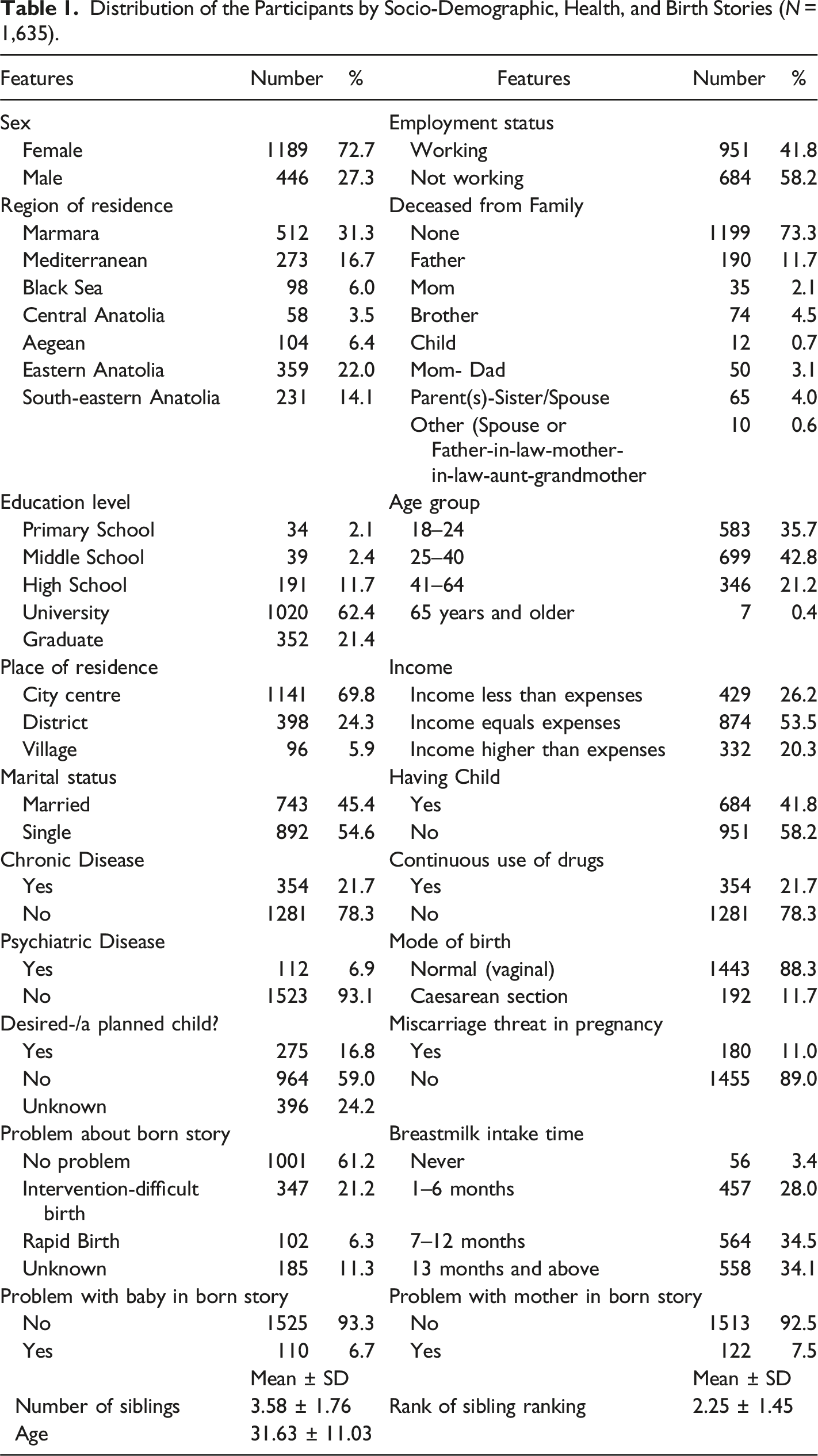
Distribution of the Participants by Socio-Demographic, Health, and Birth Stories (N = 1,635).
Distribution of CPS and ASDA Scores According to the Birth Stories and Socio-Demographic Characteristics of the Participants (N = 1,635).
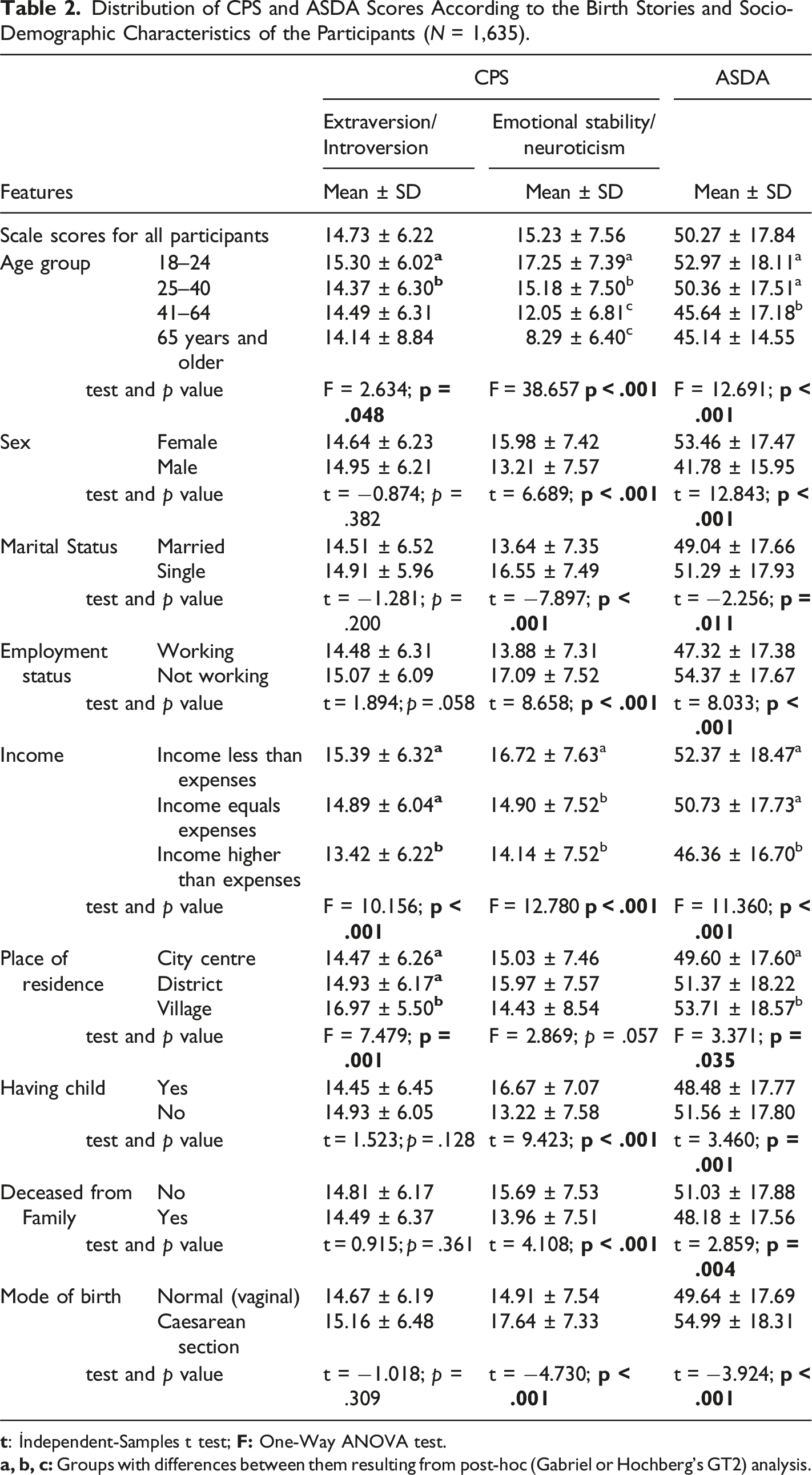
The distribution of CPS and ASDA scores, according to the birth stories and socio-demographic characteristics of the participants, is shown in Table 2. Accordingly, a statistically significant difference was found between the mean score of the CPS extraversion/introversion sub-dimension and level of income (p < .001) and place of residence (p = .001). There was a significant difference between marital status in terms of mean score of emotional stability/neuroticism (p < .001), and death anxiety (p = .011).
Additionally, a significant difference was found between emotional stability/neuroticism and sex, employment status, having children, death in the family, and income levels (p < .001). There was no statistically significant difference between the groups in terms of the mean score of the CPS extroversion/introversion sub-dimension and born type (p = .309). However, there were statistically significant differences between groups in terms of the mean score of emotional stability/neuroticism (t = −4.730; p < .001), and death anxiety in terms of mean score (p < .001) and born type.
Correlation Analysis Results According to Scales.
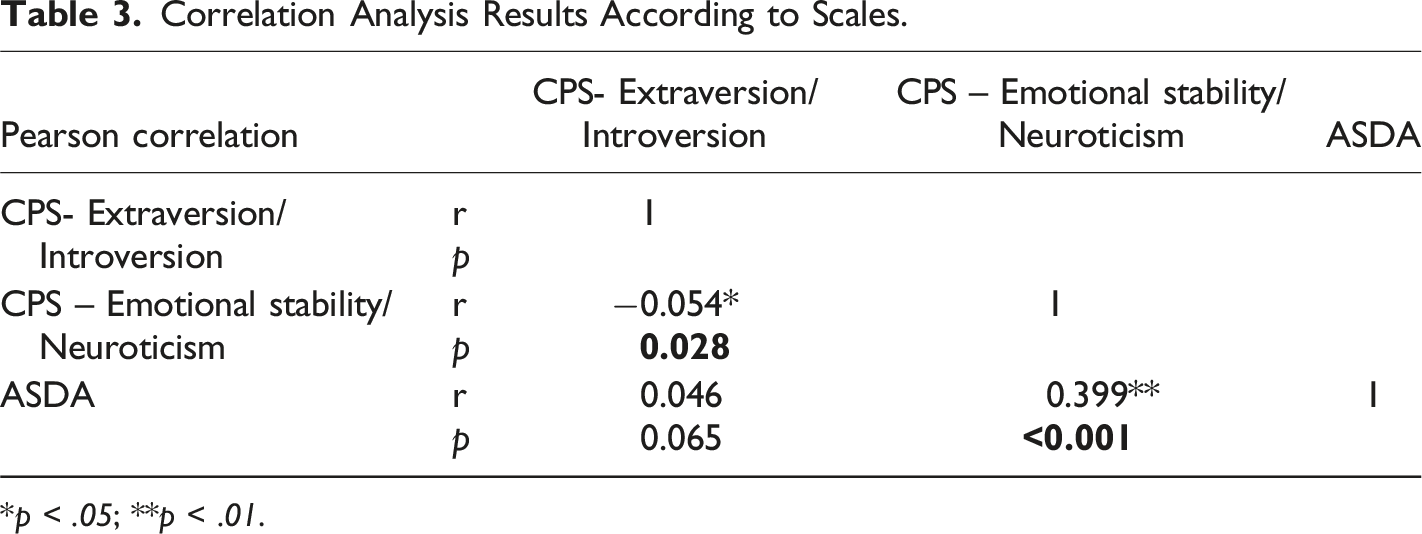
*p < .05; **p < .01.
Multivariate linear regression analysis was performed by establishing the following hypotheses to predict the Emotional stability/neuroticism variable using birth type, gender and death anxiety variables:
The independent variables of age group, marital status, type of birth, gender, employment status, income, having child, deceased from family and death anxiety do not significantly predict the dependent variable Emotional stability/neuroticism personality trait.
At least one independent variable of age group, marital status, type of birth, gender, employment status, income, having child, deceased from family and death anxiety significantly predicts the emotional stability/neuroticism personality trait.
Multiple Regression Analysis Results With Emotional Stability/Neuroticism as the Dependent Variable.
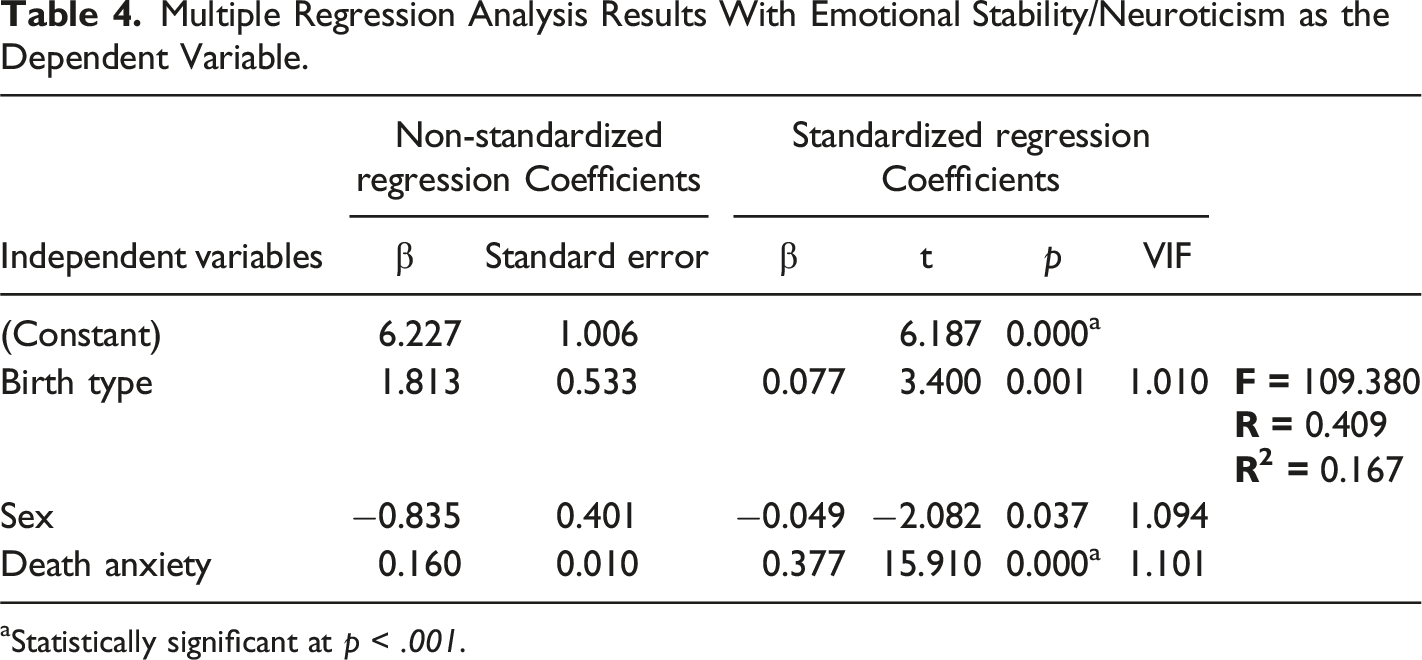
aStatistically significant at p < .001.
Multiple regression equation: Emotional stability/neuroticism = 6.227 + 1.813* birth type + −0.835* gender + 0.160*death anxiety (Table 4).
Multivariate linear regression analysis was performed by establishing the following hypotheses to predict the death anxiety variable by using the born type, sex, and emotional stability/neuroticism personality variables:
H0 = The independent variables of age group, gender, marital status, employment status, income, place of residence, having child, deceased from family and emotional stability/neurotic personality do not predict the dependent variable of death anxiety.
H1 = At least one of the independent variables of age group, gender, marital status, employment status, income, place of residence, having child, deceased from family and emotional stability/neurotic personality trait predicted the death anxiety dependent variable significantly.
Multiple Regression Analysis Results With Death Anxiety as the Dependent Variable.
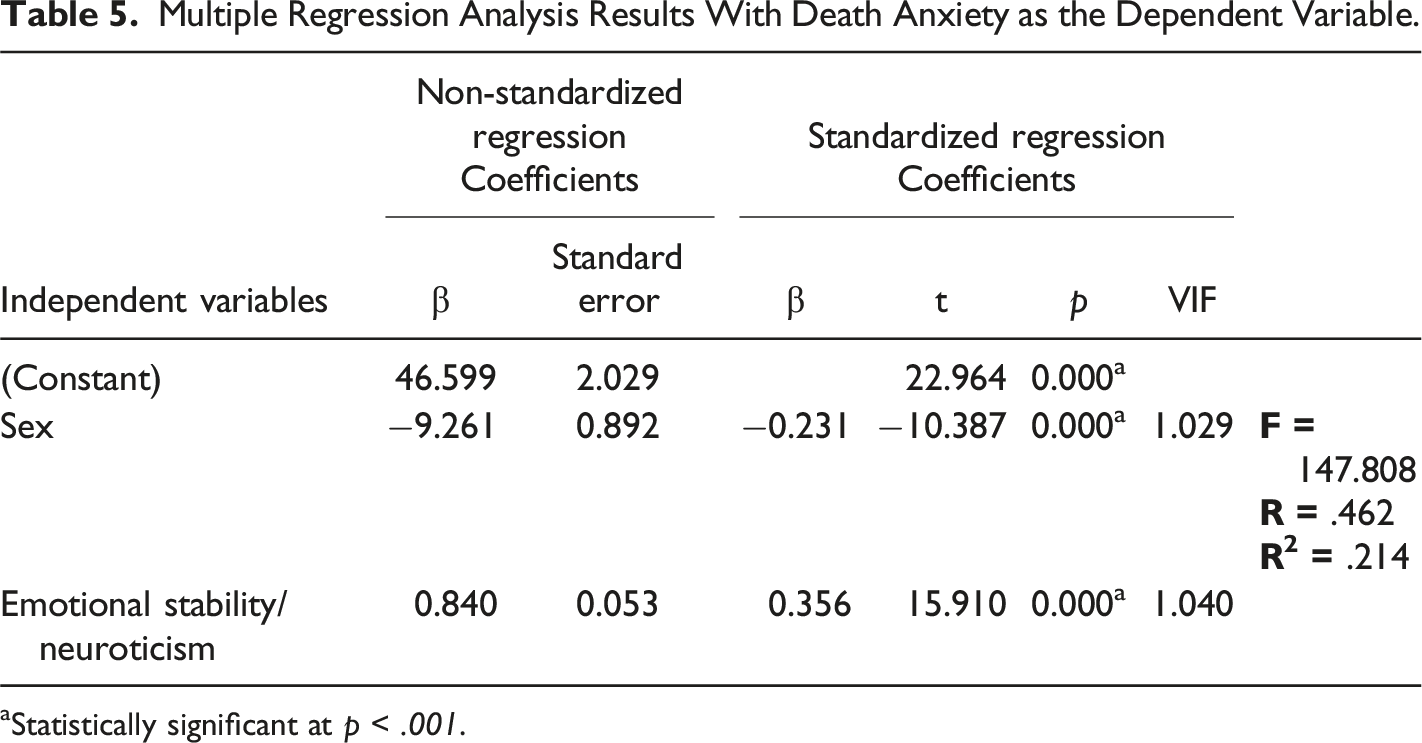
aStatistically significant at p < .001.
Multiple regression equation: death anxiety = 46,599 + −9,261 * sex + 0.840 * emotional stability/neuroticism personality trait (Table 5).
All of the hypothesized variables were added to the model, and variables that did not significantly predict emotional stability/neuroticism and death anxiety are not shown in the table. Only significant predictors are included in the table (Tables 4 and 5).
Discussion
Death is an undeniable reality of life. According to existential theories, death anxiety is a universal emotional experience that affects people from birth and represents the root of many fears. Research has shown that individuals’ death anxiety can be heightened by traumatic events that induce anxiety (Hamama-Raz et al., 2016; Karadağ et al., 2022). It was found that studies investigating the fear and anxiety of death experienced by women who have had or will have a caesarean delivery (Fentie et al., 2022; Şanal Karahan et al., 2020). Nevertheless, no research has been conducted into the impact of an individual’s birth story on their personality traits and death anxiety. This study aimed to investigate the impact of birth story on personality traits and death anxiety while also examining other potential variables that may affect these outcomes.
The study determined that the participants were closer to the extroverted and emotionally stable/neurotic traits, and their death anxiety was at a moderate level. Our results are consistent with previous literature (Aydin Ozkan & Kucukkelepce, 2019; Orhan Ergin & Yağmur, 2018; Yılmaz et al., 2021). It has been demonstrated that traumatic events that elevate anxiety also raise an individual’s death anxiety (Hamama-Raz et al., 2016; Karadağ et al., 2022). In a study conducted by Abdel-Khalek (2004) with Egyptians, the participants’ death anxiety was similar to our findings. Additionally, studies carried out during the pandemic have observed an increase in death anxiety due to pandemic-related factors (Cakir Kardes et al., 2022; Gundogan & Arpaci, 2024; Kandemir, 2020; Karadağ et al., 2022; Saleem & Saleem, 2020).
The study examined whether there was a difference between the groups in terms of death anxiety and personality traits according to various characteristics of the individuals and birth story information. Furthermore, it examined the correlation between personality traits and death anxiety. Regression analysis was performed on the basis of the significant results obtained. The multiple regression analysis showed that type of birth, gender and fear of death had an effect on the neurotic personality trait. Individuals born by caesarean section had higher mean scores for emotional stability/neuroticism than those born vaginally. There is no literature on the relationship between birth type story and personality traits. However, a caesarean birth is typically performed in the event of an unanticipated situation or emergency. In such instances, the mother’s stress level and emotional state may influence the infant’s emotional development following birth, and the oxytocin hormone may also be a contributing factor. Oxytocin has been demonstrated to reduce anxiety and foster a sense of trust by suppressing cortisol release, which is triggered by stress (Kirsch, 2015). While vaginal birth is initiated by an increase in oxytocin hormone, caesarean birth does not commence with oxytocin secretion (Kuğuoğlu et al., 2012). The reason why the emotional stability/neuroticism characteristics of individuals born by caesarean section are at the forefront may be the effect of oxytocin hormone. Furthermore, maternal attachment levels may also influence personality traits, such as emotional stability and neuroticism. The process of bonding and interaction between mothers and babies during vaginal birth has been found to be faster and more intense than during caesarean birth (Ebrahimi et al., 2021). In mother-infant relationships where maternal attachment is high, the baby’s emotional development and personality development are positively affected (Davies et al., 2021). This high level of attachment has a positive impact on the baby’s emotional development, and the type of birth can affect personality traits. Pradhan and colleagues (2022) reported that death anxiety was positively correlated with neuroticism (Pradhan et al., 2022). It can be said that individuals prone to neurotic personality traits are anxious, angry, emotionally unstable, prone to stress and depression, and that these factors make them more susceptible to death anxiety.
According to the multiple regression analysis, sex and emotional stability/neuroticism personality structure contribute significantly to the level of death anxiety. In our study, it was observed that women’s death anxiety was higher than men’s. Similar findings were obtained in the literature (Ayten, 2009; Kimter & Koftegul, 2017; Özdemir et al., 2021; Pérez-Mengual et al., 2021; Power & Smith, 2008; Saleem & Saleem, 2020; Yıldız & Bulut, 2017; Yüksel et al., 2017). According to Saleem and Saleem’s 2020 study, while women express their thoughts and feelings about death more openly, men tend to keep them to themselves. This can be explained by the fact that women’s expressions of emotion and anxiety are stronger (Bal et al., 2013; Yıldız & Bulut, 2017). In the study by Yıldız and Bulut (2017), it was found that sex made a greater contribution to death anxiety level than personality traits.
Strengths and Limitations of the Study
This research is one of the preliminary studies investigating birth story and death anxiety in the literature, and it is a strong study with a 100% reliable sample size. However, the sample represents only the Turkish population.
One limitation of the study is its 11.7% (197 individuals) caesarean section rate. The rate of caesarean section deliveries in Türkiye, which was nearly 0% in the 1990s, has now risen to about 50% in the past two decades (Demirbaş et al., 2018). Therefore, the 11.7% represents the number of individuals over 18 years old who were born by caesarean section in the country. The study’s high total number of samples is considered crucial, as it represents a good starting point for researching the correlation between birth type and death anxiety and personality traits.
Another limitation of this study is the scales used to measure death anxiety and personality traits. There are different tools that measure death anxiety and personality traits.
Conclusion
In this study, it was found that the type of birth had no significant effect on death anxiety, while gender and personality traits had a more significant effect on death anxiety. It was also found that mode of birth, gender and death anxiety influenced the personality trait neuroticism. It is crucial to recognise that a caesarean section may create a perception of traumatic birth in both the mother and the infant. Consequently, it is of paramount importance to support normal and natural birth with health policies. For infants born via caesarean section, early skin-to-skin contact can enhance the quality of the mother-infant bond. This can positively impact the infant’s emotional development. Postnatal support programmes can be developed for families of infants born via caesarean section. These programmes may include emotional and psychological support, as well as guidance on recognising and meeting the infant’s emotional needs. This study demonstrates the significance of implementing supportive practices to assist individuals with high death anxiety in developing positive personality traits that will facilitate their coping abilities.
The data used in this study are representative of the Turkish population. It is recommended that similar studies be conducted in different cultures/countries and populations with different socio-demographic characteristics. It is also recommended to investigate different factors that may influence personality traits and death anxiety. Furthermore, it is possible to conduct further research utilising alternative instruments to measure death anxiety and personality traits.
Footnotes
Acknowledgments
The authors would like to thank all participants for their time.
Author Contributions
ZT: Conceptualization; methodology; investigation; data curation; writing—review and editing; writing—original draft. SÜ: Conceptualization; methodology; data curation; writing—review and editing; ÇŞT: Investigation; methodology; data curation; writing—review and editing. GD: Supervision; writing—review and editing. All authors read and approved the current version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Submission Declaration
This manuscript is not under consideration for publication elsewhere, its publication is approved by all authors and tacitly or explicitly by the responsible authorities where the work was carried out, and if accepted for publication, it will not be published elsewhere in the same form, in English or in any other language, including electronically without the written consent of the copyright-holder.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.