
Abstract
Hope is a critically important concept in palliative care that enables coping and increases quality of life. This qualitative study was conducted to determine how palliative care patients describe hope and the factors that increase or decrease hope after a hope intervention. Data were collected through semi-structural interviews with 10 palliative care patients. The analysis followed a thematic analysis approach. The participants defined hope as the joy of living in general, and the strength to cope with difficulties and stated that spending time with loved ones increased their hopes, the worsening of their diseases reduced their hopes, hope made them feel good psychologically, and health workers had an important role in increasing hope. It is recommended that hope interventions be person-centric in palliative care settings and that care should be structured by considering the factors that maintain and prevent hope.
Introduction
Hope is a positive coping mechanism that contributes to psychological well-being at all stages of illness, especially important for palliative care patients (Beng et al., 2022; Olsman et al., 2015). Farran et al. (1995) stated that hope is to find a balance between different dimensions, such as experiencing painful experiences, being in a relationship with other people, being intertwined with spirituality, as well as being in a situation that arises in difficult times (Farran et al., 1995). According to Snyder (2000, 2002), hope consists of three cognitive dimensions: thinking about the action to achieve a goal, thinking about ways to achieve the goal, and planning (Snyder, 2000, 2002). Hope at the end of life is a complex and dynamic emotion (Guedes et al., 2021). Each discipline approaches hope from its perspective, which complicates attempts to integrate all views into their entirety.
Receiving the news of a serious illness is a very difficult experience for a person. At this point, it's important to understand why some people give up, why others fight, and why some accept (McKay, 2004). Kubler-Ross states that when patients learn that their illness is incurable, they experience five stages: denial, anger, bargaining, depression, and acceptance. These stages are non-linear; people can experience these stages at different times, and they do not necessarily occur in one particular order. Additionally, Kubler-Ross asserts that along with acceptance, hope is what actually makes the pain bearable for days or months (Kübler Ross, 1973).
According to the World Health Organization (WHO), each year, an estimated 56.8 million people, including 25.7 million in the last year of life, need palliative care. The global need for palliative care will continue to grow as a result of the aging of populations and the rising burden of non-communicable diseases and some communicable diseases (World Health Organization, 2020).
In the literature, it is reported that structured hope intervention programs in end-of-life care and diagnosis of serious illness increase hope and quality of life and reduce mental distress (Duggleby et al., 2007; Herth, 2001; Rustøen et al., 2011). In addition, qualitative studies underline that hope always exists in palliative care, gives the patient the strength to continue even in the most adverse situations, and has an important role in maintaining the comfort of the patient (Beng et al., 2022; Laranjeira et al., 2022). Although there are studies evaluating the meaning of hope in palliative care, studies on how hope is shaped after a hope intervention and what can be done in addition are limited. Turkey is a country where palliative care is in the structuring stage and there has not been any study on this subject in our country.
This qualitative study was conducted to determine how palliative care patients describe hope and the factors that increase or decrease hope after a hope intervention. This empirical information is critical for recommendations on how to develop hope-based interventions for palliative care patients.
Methods
Study Design
As part of a randomized controlled hope intervention study, we conducted a qualitative study to gain a deeper understanding of the hopes of patients in the intervention group. The intervention was performed in three sessions for three consecutive days and each lasted approximately 20–30 minutes. In the first session, a brief training was carried out on hope. In the second session, strategies for maintaining hope were discussed (Connecting with others, personal strategies, cognitive methods, activating moments and setting goals). After the training, goal exercise, which is one of the strategies that improve hope, was done. The third session included hope-oriented activities. The implementer of the study holds a master’s degree in psychiatric nursing.
This study used a qualitative descriptive design to provide insight into the phenomenon of hope through subjective experiences (Creswell & Poth., 2016). The data were gathered and reported according to the checklist created by the Consolidated Criteria for Qualitative Studies (COREQ) (Tong et al., 2007).
Participants and Setting
The study was conducted with patients who were treated as inpatients in a palliative care center in Turkey between October 2020 and January 2022 and who met the research criteria.
Inclusion criteria were: aged 40 years or more, agrees to participate in the study, can speak Turkish, there is no deterioration in cognitive functions (assessed by means of brief version of Mini Mental State Exam), does not have have any disability to communicate. Exclusion criteria were: developing obstacles in communicating for any reason, deteriorating general health status (e.g. delirium, cognitive impairment), and not agreeing to participate in the study.
The study was conducted at a university hospital’s palliative care center in Sivas, Turkey, which provides comprehensive interdisciplinary care to 11 patients.
Sample Selection
The sample of the study consisted of 10 patients in the intervention group and these patients were determined by the analogous sampling method, which is one of the homogeneous sampling methods. Homogeneous sampling is used (Neuman & Robson, 2014) when studying key issues that affect individuals who have had similar experiences, where differences between participants are small. In our study, participants whose Herth Hope index score level was above the middle level were included in the qualitative study. The number of participants was determined (Polit & Tatano-Beck, 2010) according to the principle of data saturation applicable in qualitative research.
Data Collection, Analyses, and Synthesis
Interview Questions.
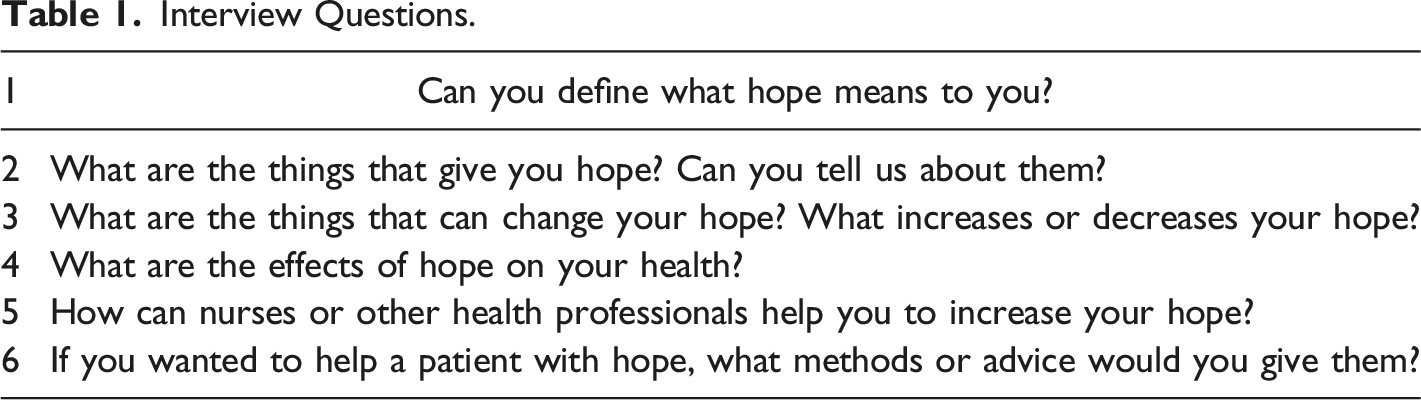
In our study, data were analyzed using the processes of thematic analysis outlined by Braun and Clarke (2006), which involves familiarization with data, generating initial codes, constructing themes, reviewing potential themes, defining and labeling themes, and writing up analysis. The study was explained to the participants in detail and written consent was obtained for the audio recording of the interviews. The researcher then listened to the recordings carefully and repetitively and turned the data into written text. The written text was read repeatedly by the researchers. The document created for each patient was examined and coded independently by the researcher and a qualitative research specialist. The documents coded by the two people were compared when completed and the themes were finalized. MAXQDA Analytics Pro 2020 was used for coding and data management.
Ethical Approval
Before the start of the research, written permission was obtained from the Research Ethics Committee (2019-11/07) and the center where it will be applied (93596471-774.99-E.465839). The protocol conforms to the provisions of the Declaration of Helsinki. In addition, all participants gave their informed consent to participate, and the researchers ensured that patient anonymity was preserved. Voice recordings were encrypted and stored on a personal computer. Access was available only to authors.
Results
Descriptive Characteristics of the Participants (n = 10).
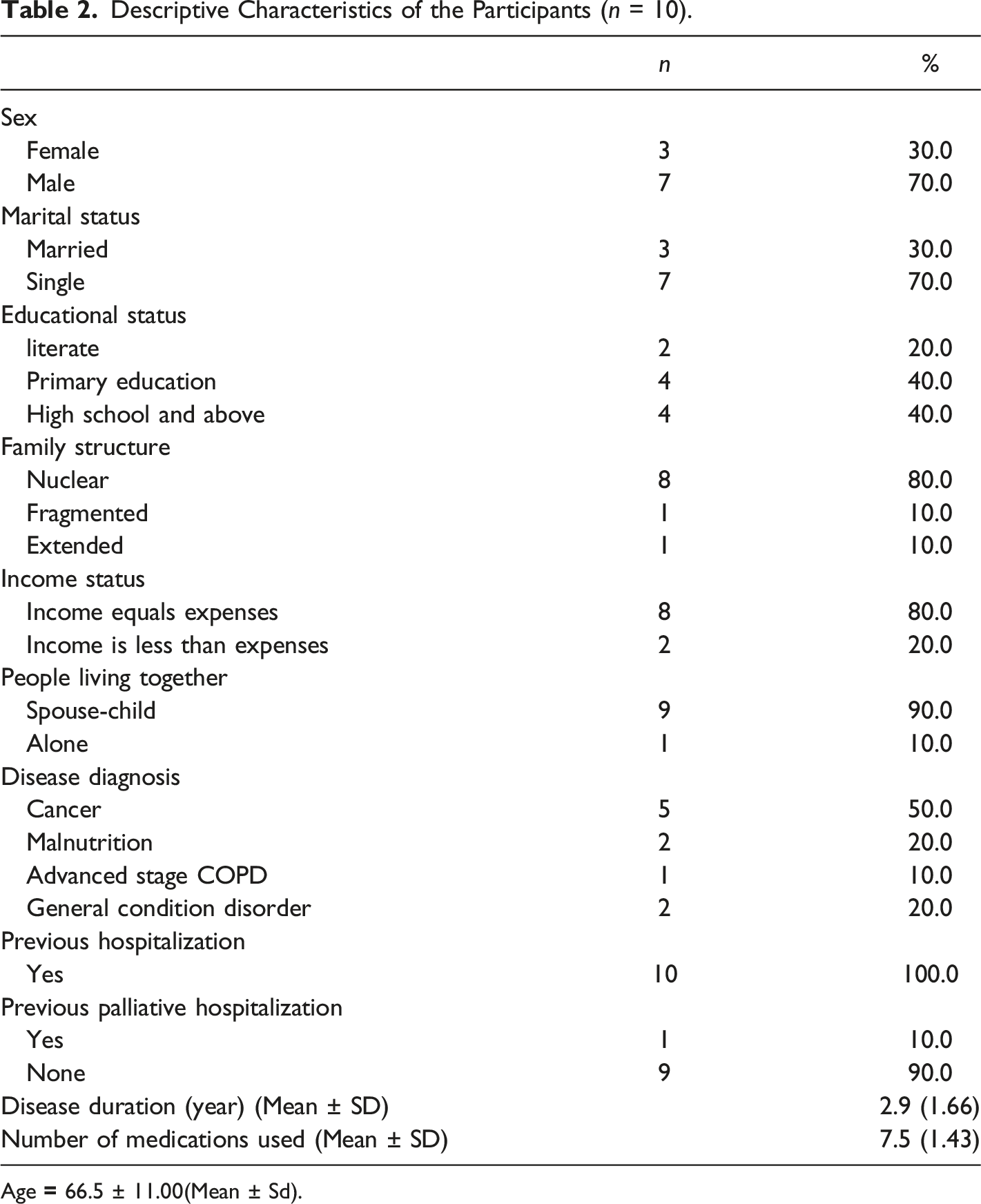
Age
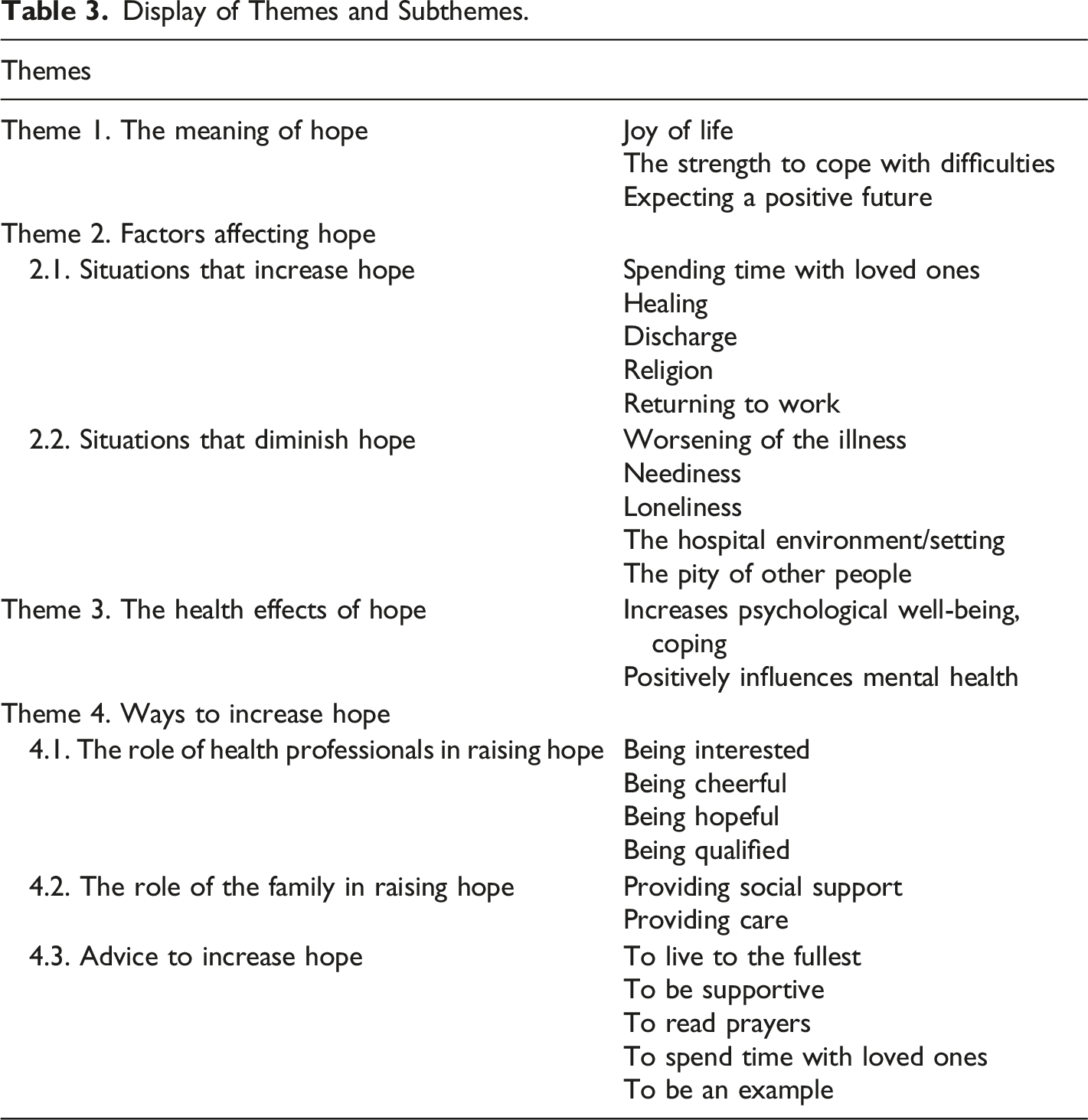
Display of Themes and Subthemes.
The Meaning of Hope
On the theme of the meaning of hope, participants expressed intense opinions about the joy of living “For me, it means the joy of living” (P1) and participants mentioned that hope was their reason to continue living “Hope is what keeps you going to live even though you know you’re going to die” (P10), “Hope is what sustains us, the reason we live…” (P6).
Hope meant the strength to overcome difficulties. The statements of the participants P7 and P9 on the subject are as follows: “Hope is the force to overcome every challenge” (P7), “Hope is the emotion that keeps us alive, that makes us think about everything getting better, that keeps us alive, that makes us cope with challenges” (P9).
It was determined that hope is not always about treatment. For many patients, hope means living a little longer, healing, enjoying the remaining life, seeing tomorrow, or expecting a positive future, knowing that the prognosis will not be able to improve. Participants mentioned that: “For me, it means healing. Yes, I know it is difficult, but even if people come to the last point, they always wait for a miracle to be found or a cure... I think that's hope” (P3). “It is hope for me to go out tomorrow. Always waiting, hoping...” (P2), “Hope for me means continuing to live even in this state... I'm always waiting for a new day” (P4).
Factors Affecting Hope
Two sub-dimensions have been created belonging to the second theme of the research, factors affecting hope. These are situations that diminish hope are situations that increase hope.
Situations that Diminish Hope
The factors that diminished hope were mostly related to the disease. The worsening of the illness and the consequent increase in unpleasant symptoms such as pain and the need to be cared for by someone else were factors that decreased hope: “The progression of the disease, the increase in my pain.” (P3), “A bad situation reduces my hope.” (P7), “The deterioration of my condition, not being able to get out of the hospital…” (P3). Participants indicated that being bed-bound and needy of others would diminish their hopes: “If I’m thoroughly bedridden, if I never get up, my hope diminishes” (P1), “To languish completely, to be a burden to my loved ones” (P6).
Loneliness was also a factor that diminished hope. “Being alone diminishes. Thank God my children are coming to visit me here. Without them, my hope would have faded if I had been abandoned” (P1), “Desolation. Here, one needs even a glass of water. What if I didn't have a daughter? Or as I said, seeing funerals diminishes. I think one day they will take me away” (P5).
In the clinic where this study was conducted, it is seen that factors such as the fact that the patient rooms mostly serve two or more patients, device sounds, crowded environment, hospital routines, patients in different diagnoses and stages, and witnessing death adversely affect the hope of the participants. Participants stated that seeing continuous funerals in the hospital caused a decrease in hope: “For example, there is a funeral here every day. Just the other day someone from this room was gone. At night screams and cries. I have no hope left. Negative things affect people” (P5) and: The hospital diminishes hope. It's very hard to be here. Yes, I wouldn't be able to live with these pains if it wasn't for this place, but if people are going to die, they have to die at home... Someone dies every day. I don't want to see that (P7).
Participants mentioned that they found it hope-diminishing for their relatives to feel sorry for them: “...I do not want them to look at me with pity thinking: what happened to him/her at a young age, how did it happen. I need morale, not pitying looks” “When other people talk about my illness, ask questions, say what a pity” (P4) and: They come to my room, they leave immediately saying you are sick and I need rest. But I need people. I need conversation, I need breathing. I'm not going to lie down all the time waiting in the room because I'm sick... They talk in a whisper, they look at me with pathetic eyes... I don't have any hope left, I guess my situation is very bad (P6).
And I'll never forget that when I first got sick, a doctor took the paper with my daughter and said you have cancer. My daughter cried there, she was sad, I was helpless… I felt sorry for her, not for myself. This is not the proper way to inform, they need to be understanding towards patients. These diminish hope. We need morale… (P2)
Situations that Increase Hope
In the sub-dimension of hope-increasing situations, five different subthemes have been created. These are; spending time with loved ones, healing, discharge, religion, and returning to work/home.
Participants mentioned that being with their family and loved ones raised their hopes: “My family gives hope, my grandchildren, my children” (P1), “Being with my loved ones increases” (P8) and that health professionals bringing patients together with family increased hope: “We have Corona here right now. Visitors are forbidden… I missed my grandchildren. Let me spend time with them… They give me hope…” (P2).
It was determined that the slightest positive development in diseases increased their hopes. Particularly the positive effects of disruption such as pain. Participants stated that recovery and reduction of their pain relief them hope: “Improvement in my health. Maybe it's weird to you here… But no matter how sick you are, you always carry in your heart the hope that you will be healed” (P6), “If my pain improves, my hope increases” (P7). Participants stated that health professionals gave good news and instilled hope in patients: “By saying if there is even the slightest positive thing... Giving good news...” (P8).
Participants stated that being discharged and returning home was a hope-increaser: “If I go home, for example, my hope increases. I don't want to stay here. Whatever will happen, let it be there” (P1) and: It's very hard to find hope here. Everyone is sick and some are worse off than me. But I still say thank you to this day and pray to Allah. It gives me hope to think I'm going home” (P7).
It was determined that the hope of positive future expectations such as returning to the past life and returning to work, as well as returning home, increased. “Going back to my work. To be the same as before...” (P10). Another sub-theme that participants expressed an opinion on in hope-increasing situations was religion/spiritual being/god: “Praying. I take refuge in Allah. Of course, I say this too shall pass. May Allah grant us His blessings...” (P7), “It gives me hope to think that I can be with my loved ones in heaven in the other world” (P10).
The Health Effects of Hope
Hope’s impact on subjective feelings of health has often been about psychological health. It was determined that hope increases psychological well-being and coping and positively affects mental health: “It gives us psychological strength. It wouldn’t have happened without him” (P1) and “If I recover my morale, my illness will also be cured. Hope is the necessary nourishment for these” (P3). Participants stated that hope gives them the strength to endure and cope with adversity: “Without hope, I would be like a living plant by now. It gave me stamina. And I say thank goodness for that” (P7) and: I became like this after a car accident, for example. I was unemployed, my family was devastated. My wife has to look at me all the time. But I said if there is breath, there is hope. I clung to life. This was thanks to hope. It's the reason for me to continue to live with my pain (P4).
Participants noted that hope had a positive effect on health: “When I have high hopes, my health is positively affected” (P2).
Ways to Increase Hope
Three sub-dimensions have been created belonging to the last theme of the research, ways to increase hope. These are; the role of medical staff in raising hope, the role of family in raising hope, and recommendations for increasing hope.
The Role of Health Professionals in Raising Hope
Concerning the role of health professionals in raising hope, participants expressed an intense opinion about being attentive. Participants mentioned that the attentiveness of health workers raised their hopes of providing the necessary care: “They’re doing what they can, they’re helpful by showing interest” (P1), “I would like them to take care of me and my illness. When my pain comes, they should give me medicine in time. They should treat me well” (P7).
Participants stated that the caring and friendly nature of health professionals increased their hopes: “Their friendly, loving, positive approach increases hope” (P3), “One is looking for a smiling face. Even hearing a good morning gives one hope. You feel valued, and that they strive for you” (P4).
The hope of health professionals also had a positive impact on patients. You said that if you don't have hope, borrow it from someone hopeful until you have hope. Spend time with hopeful people. Just like that, nurses and doctors should not look at us thinking they are going to die and there is nothing to do anyway. Let them be hopeful and we will be full of hope when we see them (P5).
Participants stated that the fact that health professionals are experienced and know their job gives hope to patients: “People want to know that they are in good hands here. I'm here, but these people have worked for me, they mean knowledgeable. It gives confidence that they are competent in their jobs…And of course the smiling face” (P6).
The Role of the Family in Raising Hope
In the sub-dimension of the role of the family in raising hope, 2 different subthemes have been created. These are; providing social support, and providing care.
In the role of the family in promoting hope, participants expressed an intense view of providing social support. Participants mentioned that it was hopeful to have family members come to visit: “Let them talk with me, come to visit me” (P2) and “Let them come to visit me. Let them talk, let them chat” (P9). Participants noted that family assistance in providing care to patients played a role in increasing hope: “It's very important that I feel their support and help with my care. Their presence is my greatest support.” (P3)
Advice to Increase Hope
To increase hope, six different subthemes have been created in the advice category, which are: to live to the fullest, to be supportive, to read prayers, to spend time with loved ones, and to be an example. Participants mentioned that patients should enjoy life. First of all, I would take him to a green place. People used to fresh air require refreshment in the hospital. Then spend it nice even if you have a day left. I used to say every cloud has a silver lining (P7) and Let him start every day by saying I'm going to do this today. Do not constantly occupy your head with illness. Everything comes to pass. The important thing is whether one is breathing now. Well, okay then. Let him do whatever he wants. (P10)
Participants stated that providing support by being with patients would increase hope: “I’d tell him everything would be fine. I would be supportive. Man’s breath is enough. I would be a comrade” (P1) and: I used to talk to him a lot. I would pull on a folk song. For example, you said: “Tell your life story.”, I liked it very much. I went back to those old days. I'd ask him to talk to me and I'd have a cup of tea and listen… (P6), I'd take him out into the open air. We would look at the sky, the sun, the green and spend time in the fresh air. I would ask him about the music and books he liked. I used to visit regularly and try to boost morale…” (P3).
Another statement that respondents gave their opinion on in the category of advice to increase hope was spending time with loved ones. Participants indicated that spending time with loved ones and family would increase the hope of other patients: “I would recommend him to have a good time with his family” (P8) and “I say that the disease should not prevent them from living. Even if the remaining day is 1 day, let them spend it with their loved ones” (P2).
Religious rituals such as praying were among the participants’ hope-increase advice. Participants indicated that they advised patients to pray: “I used to tell him to take refuge in Allah. This trouble came to us from him. That’s what I do. I pray. I used to say to him, read beautiful suras and pray” (P5).
In the recommendations to increase hope, participants also expressed an opinion about leading by example. Participants indicated that they could open up and set an example to increase the hope of other patients: “… I’d say look at me… Seeing someone go through the same paths gives one hope that I will be healed” (P4) and: I would show myself to him. Yes, hard things happen, but life goes on. I would say if we have a day left, let's live with our loved ones. I'd call his family and tell them to come near him (P3).
Discussion
In the study, 4 themes were identified as a result of qualitative interviews we conducted to understand hope in more depth in patients receiving palliative care. These are; the meaning of hope, the factors that affect hope, the effects of hope on health, and ways to increase hope.
In this study, the expressions in the theme of the meaning of hope are defined as “waiting, the source that enables continuation, the power to struggle” similar to the work of Beng et al. (2022), and in this study, it is stated that hope continues to exist as long as there is life. In a study with patients receiving end-of-life care; hope has been (Laranjeira et al., 2022) defined as not being able to help thinking that there is no chance of a cure but it may still be possible. In this context, it can be said that hope has a different focus for patients in the terminal period. The majority of cancer patients describe (Duggleby et al., 2007) their hope as “relieving the pain” and “no longer suffering.” In a qualitative study on hope with advanced-stage cancer patients in China, they explicitly expressed (Chen et al., 2015) hopes for recovery or remission as the “best thing.” In this study, it was determined that hope is not always about treatment. It can also be said that hope continues to exist no matter what happens and is a psychological resource for the patient. Each individual had their perception of hope, and hope was a subjective concept.
Participants’ statements on factors affecting hope were divided into sub-dimension as factors that increase and decrease hope. They expressed especially intensely that the worsening of their illness and the worsening of their pain reduced their hopes. In parallel with the study findings, the biggest obstacle to hope in palliative care was the disease and disturbing symptoms, dependence on family members, financial problems, negative thinking and unpredictability of the future were among the other obstacles to hope for patients (Beng et al., 2022). The end of the patient’s life in the place of choice is an important indicator of the quality of palliative care (De Roo et al., 2014). Studies have shown (Coupland et al., 2011; Lee & Jang, 2018) that the preferred place of death can vary depending on the person’s cultural background In some cultures, it is preferred to die at home, and this is mostly because it is a familiar area where they can die when family members are around; on the contrary, in some cultures, terminally ill patients prefer to die in the hospital in the hope of receiving treatment to the end or reducing the burden of care for their families. Considering that in the culture where this study was conducted, the caregivers of the patient were mostly family members, and the participants may have expressed such a desire for reasons such as the perception of caring for sick parents as an important duty by society and the more respect and attention given to the patients in general. It seems that continuing their care at home will also increase their hopes, as patients accept the course of the disease, hope for themselves often turns into hope for others. A good future for those who remain has generally been a hopeful concept. In addition, similar to this study that the negative attitude of health professionals reduces hope, Laranjeira et al. (2022)'s study mentioned that poor communication with clinicians reduces hope.
Situations that increase hope include spending time with loved ones, hearing positive news about recovery or illness, being discharged, and returning to religion and work life. Participants especially mentioned that being with their family and loved ones increased their hopes. The support of family, friends, health care providers, and even pets is supportive in the emergence and enhancement of hope; it is especially mentioned that hope is increased by children and grandchildren (Beng et al., 2022; Sachs et al., 2013; Buckley & Herth, 2004; Hammer et al., 2009). The fact that the family helped the patient in many ways, visited, helped them meet their basic needs, and gave them advice, encouragement, support, and motivation to fight the disease or symptoms may have caused them to be seen as an important factor in increasing hope. Looking at the relationship between healthcare providers and hope, it has been shown that the dedication of the caregiver gives peace of mind to the patient (Harrington, 2004) friendly care increases hope, (Beng et al., 2022) it increases hope by giving the person a sense of security, support, and control through the provision of information (Hammer et al., 2009; Olsson et al., 2010) Cutcliffe and Zinck’s (2011) study with patients with AIDS shows that the despair of patients turns hopefulness into hope with compassion and non-judgmental care. In addition, as part of the implementation of this study coincided with the intense period of the COVID-19 pandemic and the strict application of visitor restrictions in hospital settings, patients complained of not being able to see their loved ones. (Cutcliffe & Zinck, 2011). It can be said that facilitating the connection of healthcare personnel with the patient’s family or loved ones can help increase hope. Again, in this study, faith-spirituality is expressed as another source of hope. Faith-spirituality gave the sick the strength to continue treatment, the calmness to endure pain and suffering, and the serenity to accept their illness and impending death. In the study, the hope of returning to work life was an expression of hope desired by the patients. Hope has been associated with better coping skills, increased endurance, decreased passivity, better quality of life, and less pain and anxiety in patients with advanced-stage cancer (McClement & Chochinov, 2008; Nierop-van Baalen et al., 2020; Penz, 2008). Studies show that hope is an important factor in the quality of life (Herth & Cutcliffe, 2002; Nierop-van Baalen et al., 2020; Penz, 2008) and coping with difficult situations (Balen & Merluzzi, 2021; Best et al., 2015;Laranjeira et al., 2022). In this study, too, participants mentioned that hope made them feel spiritually well, that it coped better with their symptoms, that it helped them feel better and fitter, and that it had an overall positive effect on their health.
In the theme of advice of patients to people with the same conditions to increase hope were listed as; living to the fullest, that is, enjoying the remaining life, religion and prayer, living day by day, establishing interpersonal relationships, symptom control, positive thinking and remembering positive memories. Regardless of the prognosis, it has been mentioned in many studies that thinking that tomorrow will be better, belief in gods, prayer, life after death, and thinking that you will be there again with your loved ones will increase hope (Buonaccorso et al., 2022; Olsson et al., 2010; Sachs et al., 2013; Hammer et al., 2009). Health professionals also have a role to play here, as they can contribute to the increase of hope by adding hope-supporting interventions to care.
Strengths and Limitations
In the study, the transcription of the data was carried out meticulously and support was obtained from a qualitative research expert independent of the study in the formation of the subthemes. Assessing hope after an intervention helped participants better define their hope. Because at the beginning of the study, hope in palliative care was an unknown or controversial topic among the participants. Instead of directly asking each participant about the effectiveness of the intervention, we tested the intervention with questions about hope. In addition, we have determined the aspects that need to be added through these questions. These factors can be listed as the strengths of the study. This study was conducted in a single center and with a limited sample. In addition, the fact that all participants were Muslims and that the sample included people with a certain level of hope are also among the limitations. Therefore, more studies are needed to generalize the results.
Conclusion and Recommendations
It was determined that the participants defined hope as the joy of living in general, the strength to cope with difficulties, that spending time with loved ones increased their hope, that the worsening of their illnesses reduced their hope, that hope made them feel good psychologically, and that health workers were important in increasing and maintaining hope.
It has been observed that hope in palliative care is independent of diagnosis and prognosis and continues to exist. While the family was a key factor in increasing the hope of some patients, it was determined that religious belief-spirituality was a more dominant factor in others. Here it is emphasized that hope interventions should be structured person-centered and the factors that increase and decrease hope should be taken into consideration. Management of bothersome symptoms is one of the important factors in hope. It has been determined that the other palliative care team, especially the nurses who form the basis of care, is an important factor in increasing and maintaining hope. It is recommended that health team members working in palliative care settings be informed about supporting hope and other psychosocial interventions.
Footnotes
Authors’ Note
The quantitative part of this study was prepared as a separate study, and “The effect of hope intervention on anxiety, hope and symptom levels of patients in palliative care: A pilot randomized controlled trial” was published in the journal Médecine Palliative.
Author Contribution
All authors have agreed on the final version and meet at least one of the following criteria [recommended by the ICMJE (![]() )]: substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content.
)]: substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Data Availability Statement
The data that support the findings of this study are available from the corresponding author.