
Abstract
Prolonged Grief Disorder (PGD) is characterized by extensive yearning, which includes a strong desire, for the deceased that occurs for at least 12 months. The aim of this study was to identify risk factors that contribute to PGD including the type of loss, relationship to the deceased, and coping. The sample included 190 bereaved adults (71 unexpected or violent loss and 119 natural loss) that experienced the loss of a loved one at least 12 months prior to completing the survey used in this study. There were non-significant results for type of loss, the presence of PGD, and coping. Findings showed that dysfunctional coping including self-blame explained the presence of PGD. Closeness to the deceased prior to the loss contributed to the presence of PGD. The findings highlight the risk factors for adults that experience a presence of PGD.
Keywords
Introduction
The psychological response to the loss of a loved one can develop into an extended grieving process that includes complex symptoms of grief, which are distinguished from pathological grief due to the mourning process. After years of contention regarding a formal diagnosis related to grief, Prolonged Grief Disorder (PGD) was formally introduced in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, text revision (DSM-5-TR) (American Psychiatric Association [APA], 2022) to provide clinicians with a framework for understanding extensive and complicated grief. Risk factors can influence one’s experience of PGD including the nature of the death, how one copes with symptoms, and the qualities of the relationship to the deceased prior to the death.
Criterion A and B of PGD in the DSM-5-TR indicates that the death loss must have happened at least 12 months prior and separation distress that occurs nearly each day or more often than not for at least a month (APA, 2022). Separation distress refers to excessive yearning or longing for the deceased or fixations on thoughts or memories of the deceased (APA, 2022). Criterion C dictates that 3 of 8 of the following symptoms including struggles with identity, disbelief of death loss, avoidance, challenges with reintegrating into life, feeling emotional numb, and believing that life is meaninglessness, and intense loneliness occur almost each day or more often for at least a month (Prigerson et al., 2021). Boelen and Lenferink (2022) compared bereaved individuals at one- and two-years post-loss, suggested that 71% of bereaved individuals that met criteria for PGD at one year were likely to have PGD in the second year, which demonstrates the pervasiveness of the disorder.
Studies have suggested that unexpected or violent loss contributes to increased rates of PGD (Djelantik et al., 2020; Eisma & Tamminga, 2022), yet neither of these studies utilized assessment instruments that are psychometrically validated in accordance with the DSM-5-TR diagnostic criteria of PGD. A more recent study reported that there were not significant differences in acute PGD severity between those bereaved by natural, unnatural, and COVID-19 related loss (Lenferink & Boelen, 2023). Although Treml et al. (2022) reported non-significance between PGD severity and cause of death, it is noted that the perception of violence in death can influence PGD. The inconclusive findings in the literature regarding type of loss and PGD severity is worth further exploration.
Perceived closeness to or conflict with the deceased prior to death has influenced the severity and extensivity of PGD symptoms (Sekowski & Prigerson, 2021). Closeness to the deceased prior to the death is significantly associated with PGD (Harrison et al., 2021; Heeke et al., 2017; Sekowski & Prigerson, 2022). On the contrary, there is evidence that closeness and conflict are predictors of grief reactions (Bottomley et al., 2019). This may be explained in that closeness prior to death loss has also demonstrated an increased likelihood of contributing to challenging grieving processes whereas conflict prior to the death may lead to a lack of resolve and adverse grief reactions (Smigelsky et al., 2020). Thus, clarifying how the relationship to the deceased prior to death relates to the presence of PGD is necessary.
Unhelpful coping strategies such as avoidance and loss rumination contribute to PGD (Smith & Ehlers, 2021). Repetitive negative thought processes assist in avoiding the reality of loss and have contributed to the intensity of PGD symptoms (Wenn et al., 2019). One study suggested that caregivers diagnosed with PGD utilized problem-focused coping strategies such as active coping, instrumental support, planning, and the emotion-focused coping strategy of acceptance (de la Morena & Cruzado, 2013). However, dysfunctional coping strategies like denial (p = .003; η2 = .98) and self-blame (p = .004, η2 = .91) increased the severity of PGD in caregivers (de la Morena & Cruzado, 2013). Furthermore, Fisher et al. (2020) found that individuals bereaved by an unexpected or violent death used dysfunctional coping such as denial, behavioral disengagement, and self-blame, which resulted in negative bereavement outcomes and higher grief severity. Adaptive coping strategies including active coping can serve as protective risk factors in the development of PGD (Miller et al., 2020). Adaption to loss through acceptance could alleviate PGD (Prigerson et al., 2022). The type of death and the relationship to the deceased affect the coping strategies implemented post-loss (Buckley et al., 2015; Kokou-Kpolou et al., 2020); thus, further analysis of the interaction between these variables as they relate to PGD can assist clinicians in understanding the new diagnostic criteria and appropriate interventions.
To our knowledge, there is limited research that addresses the DSM-5-TR diagnostic criteria of PGD and risk factors such as coping, as defined by Carver’s (1997) model, and the relationship to the deceased prior to death. Furthermore, it is clear that there is a gap in the literature regarding the presence of PGD for those bereaved by unexpected or violent loss and natural loss. The purpose of this study was to examine how type of loss (i.e., unexpected or violent vs. natural) influenced the presence of PGD and coping. Secondly, this study sought to assess associations between the presence of PGD and the relationship with the deceased prior to the death loss. The following research questions were assessed for the present study: (1) Is there a difference between type of loss and the presence of PGD? (2) What differences exist between type of loss and coping strategies? (3) Do dysfunctional coping strategies influence the presence of PGD? (4) Does the relationship to the deceased prior to the loss impact the presence of PGD?
Method
Participants
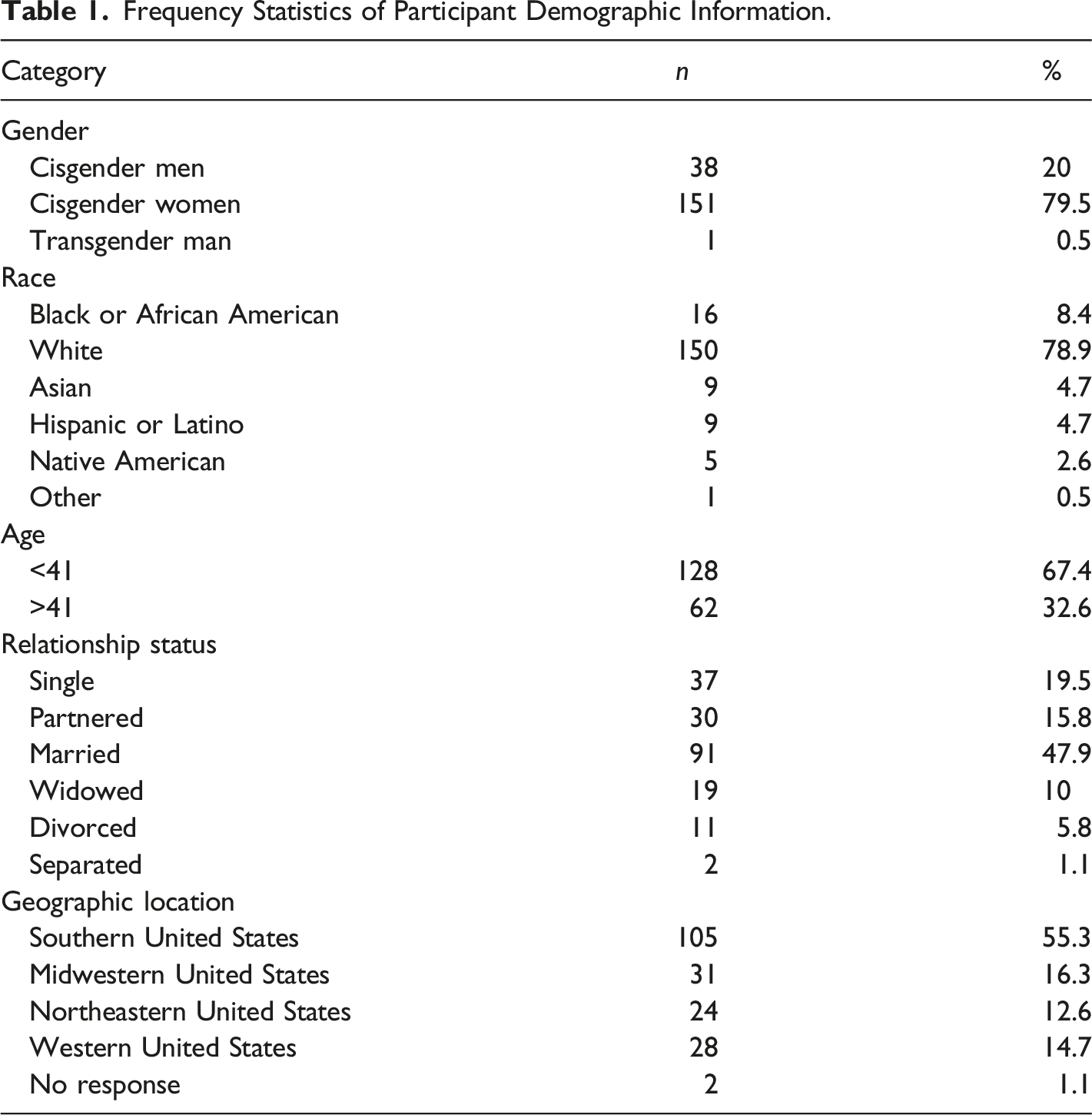
Frequency Statistics of Participant Demographic Information.
Loss Characteristics Based on the Presence of PGD.
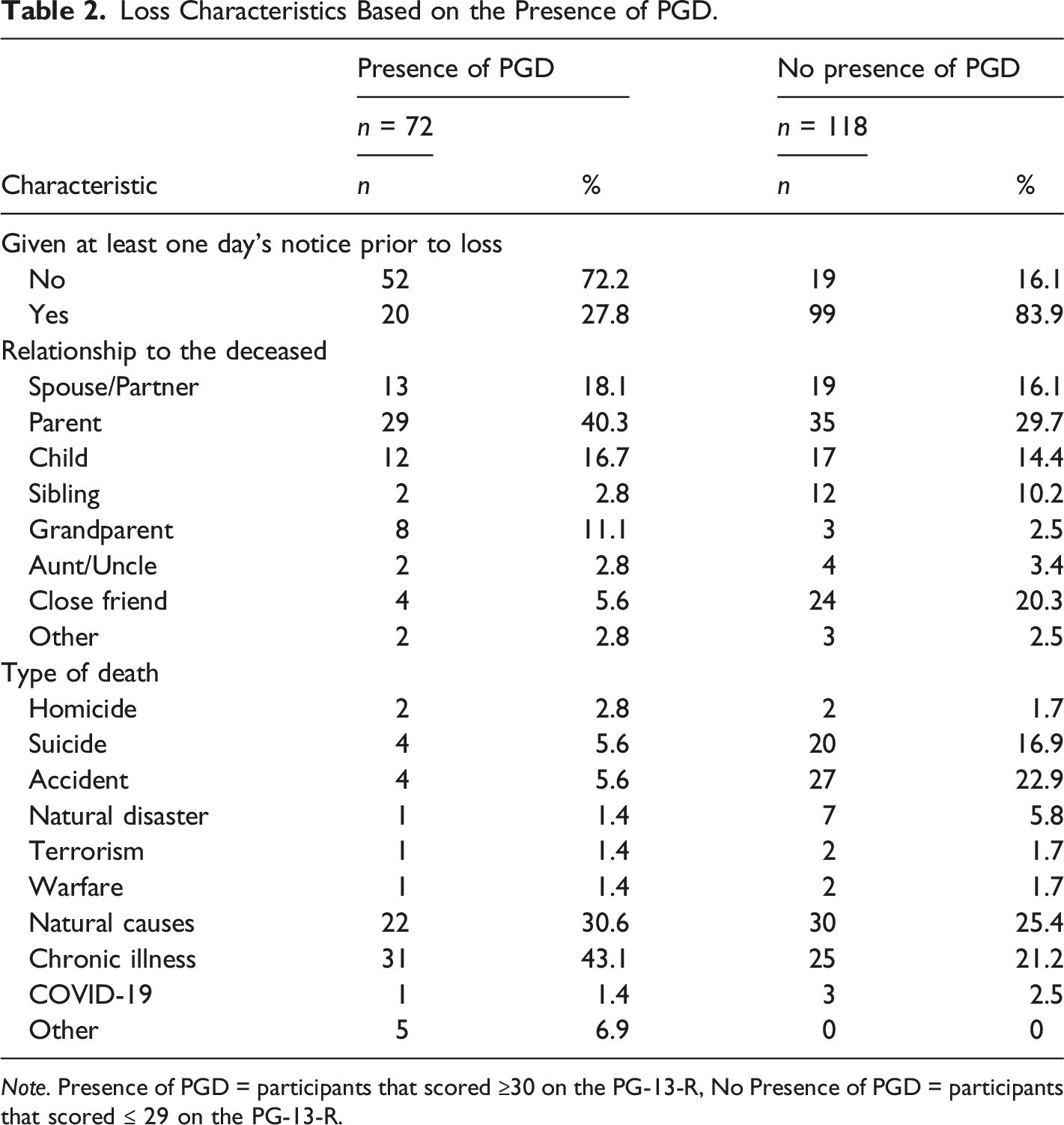
Note. Presence of PGD = participants that scored ≥30 on the PG-13-R, No Presence of PGD = participants that scored ≤ 29 on the PG-13-R.
The sample included two loss groups: 1. Participants bereaved by natural loss, comprising of 71 participants (51 females, 19 males, and 1 transgender male). Mean age was 37.41 (SD = 13.25). 2. Participants bereaved by unexpected or violent loss, comprising of 119 participants (100 females and 19 males). Mean age was 37.39 (SD = 12.75).
Procedure
Following IRB approval, participants were recruited through various clinical practices, grief-related groups, mental health listservs, and social media channels. All participants agreed to an informed consent prior to starting the survey. For the purpose of this study, participants were prompted to respond if they were given at least one day’s notice that the loss was going to occur. This study excluded individuals that were currently receiving inpatient services or residential treatment since these individuals are engaged in ongoing therapeutic processes that could influence results. Individuals that indicated having a diagnosis of a substance use disorder were excluded from the study since this would implicate findings on dysfunctional coping. Single episodes of loss were considered for this study to depict transparency of PGD severity. Participants that directly witnessed a violent death were excluded due to symptoms of PTSD influencing coping strategies. No identifying information of participants was collected.
The survey was administered using Qualtrics software. The survey consisted of five parts, which included a demographics survey, and three inventories; the Prolonged Grief Disorder-13-Revised (PG-13-R) (Prigerson et al., 2021), the Brief COPE inventory (Carver, 1997), and the Quality of Relationships Inventory-Bereavement Version (QRI-B) (Bottomley & Neimeyer, 2018), with a total of 70 items that included multiple choice and slider questions.
Instruments
Participant Demographic Survey
Participants were prompted to report demographic characteristics including age, gender, race, relationship status, and geographic location.
The PG-13-R evaluates the presence of prolonged grief based on the diagnostic criteria from the DSM-5-TR. The inventory contains two gatekeeper items that prompt responders to report if they have experienced a death loss and the number of months since the death loss. Responses for 10 symptom items are recorded on a 5-point Likert scale that ranges from “not at all” to “several times a day”, yielding a total score ranging from 10 to 50 (Prigerson et al., 2021). The responses of the 10 symptom items are summed to indicate a total score. A total score of 30 or greater suggests that the responder meets the criteria of PGD based on the DSM-5-TR. indicates the level of severity. The reliability of the scale in this study was α = .89.
The Brief COPE Inventory assesses for problem-focused, emotion-focused, and dysfunctional coping strategies by having participants rate their coping experiences on a 28-item instrument with 14 subscales that indicate scores for the three coping strategies with responses ranging from “I haven’t been doing this at all” to “I’ve been doing this a lot” on a 4-point Likert scale, resulting in a range from 2 to 8 (Carver, 1997). To determine the composite subscale scores of the coping strategies, the participant scores for problem-focused items (i.e., active coping, planning, and instrumental support), emotion-focused items (i.e., acceptance, emotional support, humor, positive re-framing, and religion), and dysfunctional items (i.e., denial, self-distraction, substance abuse, behavioral disengagement, self-blame, and venting) of the Brief COPE Inventory were categorized and summed. Subscales were created by summing the two items per coping strategy. In this study, the Cronbach’s alphas for the subscales ranged from .55 to .77.
The QRI-B instrument contains 13 items that measure two subscales (i.e., closeness or conflict) to assess the pre-death mourner-decedent relationship through a 4-point Likert scale wherein responses range from “not at all” to “very much” and scores are organized and summed for a total score to represent each subscale (Bottomley & Neimeyer, 2018). The QRI-B closeness scale assesses the support and intimacy of the relationship prior to death. The conflict scale recognizes the frequency and degree of interpersonal friction in the relationship prior to death. In this study, the closeness subscale α = .92 and the conflict subscale α = .83.
Data Analytic Strategy
Preliminary analyses of the data included an examination of assumptions. Specifically, assumptions of regression including the dependent variable (i.e., presence of PGD) is binary and ordinal, observations are independent of one another, and there was little to no multicollinearity between independent variables (i.e., coping, relationship to the deceased). Frequency statistics were performed on demographic information and loss characteristics. Descriptive statistics were conducted to calculate the means, standard deviations, and Cronbach’s alphas of the study variables. Pearson correlations were performed to explore the associations between the study variables. Independent samples t test and logistic regression were performed for this study. A p-value of .01 was used for significance in order to reduce the threat of Type I error. Analyses were conducted in SPSS version 29.
Results
Pearson’s r Correlation Matrix of PGD Scores.
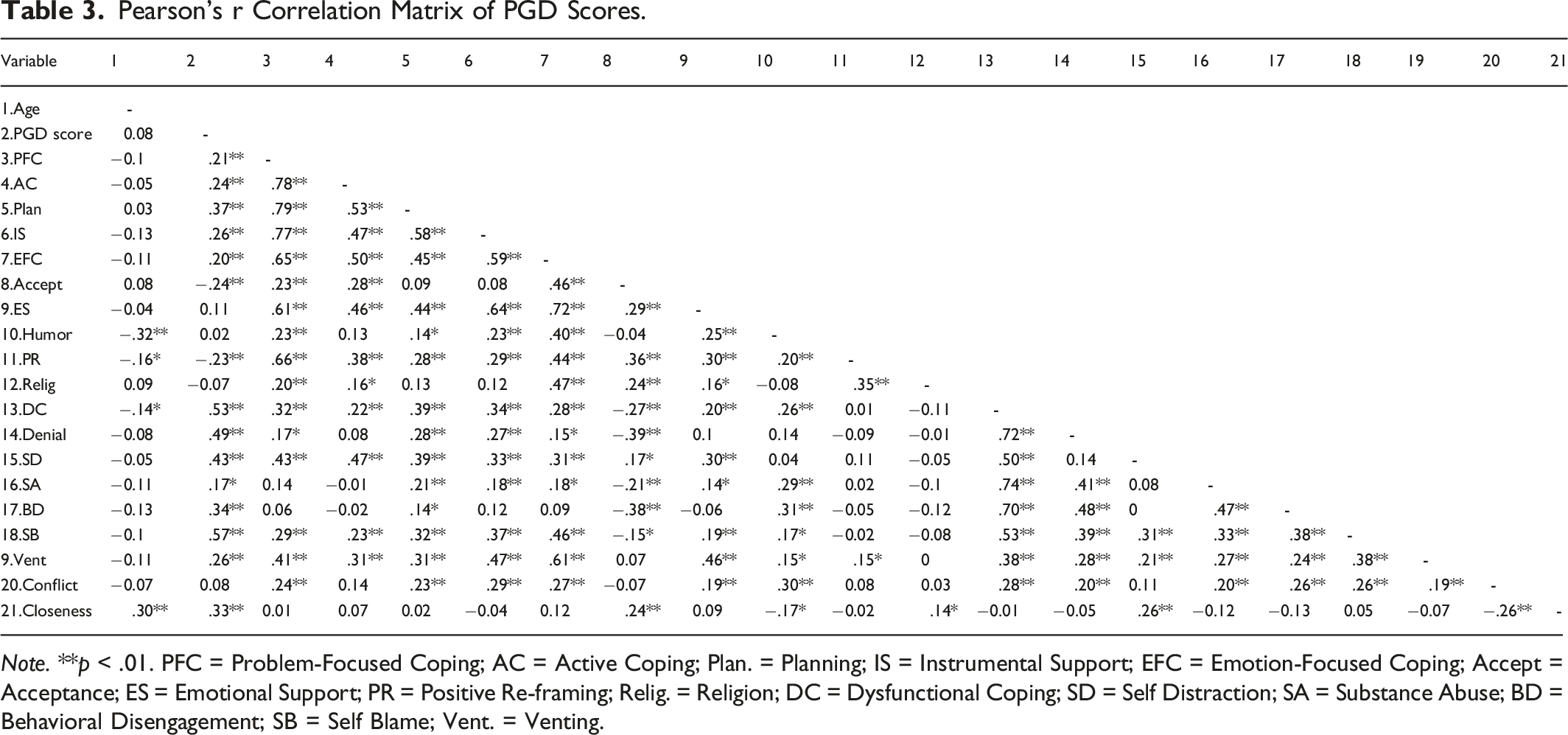
Note. **p < .01. PFC = Problem-Focused Coping; AC = Active Coping; Plan. = Planning; IS = Instrumental Support; EFC = Emotion-Focused Coping; Accept = Acceptance; ES = Emotional Support; PR = Positive Re-framing; Relig. = Religion; DC = Dysfunctional Coping; SD = Self Distraction; SA = Substance Abuse; BD = Behavioral Disengagement; SB = Self Blame; Vent. = Venting.
Means, Standard Deviations, and Cronbach’s Alphas of Scales.
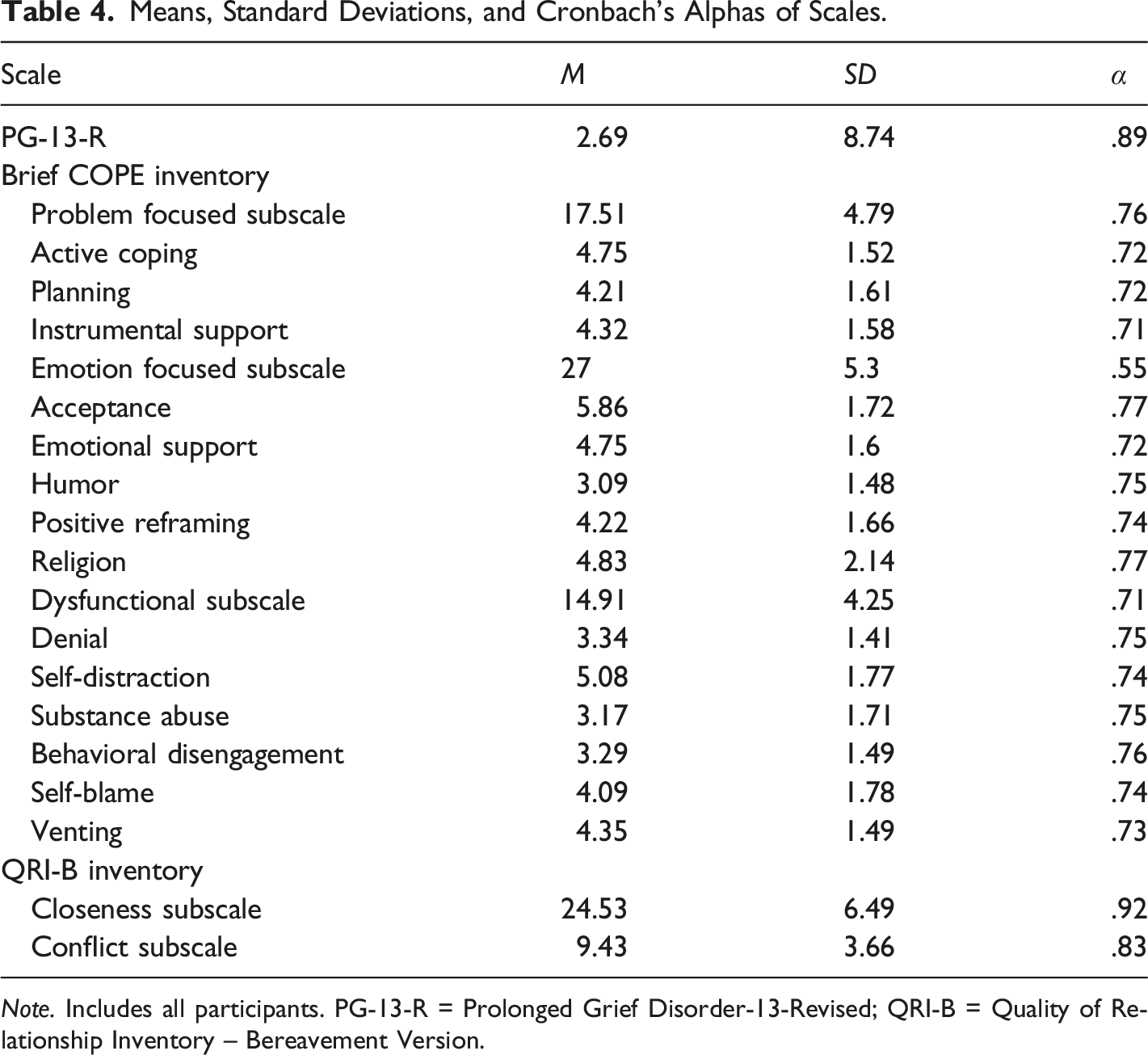
Note. Includes all participants. PG-13-R = Prolonged Grief Disorder-13-Revised; QRI-B = Quality of Relationship Inventory – Bereavement Version.
The independent samples t test did not indicate a statistically significant difference between the unexpected or violent loss group (M = 27.29, SD = 9.00) and natural loss group (M = 26.22, SD = 8.15) for the presence of PGD; t (188) = .820, p = .413. There was not a difference in the presence of PGD between those bereaved by unexpected or violent loss and natural loss.
A second independent samples t test did not indicate a statistically significant difference between the unexpected or violent loss group (M = 17.30, SD = 5.04) and the natural loss group (M = 17.85, SD = 4.35) with problem-focused coping; t (188) = −.773, p = .440. The independent samples t test did not indicate a statistically significant difference between the unexpected or violent loss group (M = 26.58, SD = 5.67) and the natural loss group (M = 27.69, SD = 4.57) for the emotion-focused coping composite subscale; t (188) = −1.388, p = .167. The independent samples t test for the dysfunctional coping subscale did not indicate a statistically significant difference between the unexpected or violent loss group (M = 14.78, SD = 4.32) and the natural loss group (M = 15.14, SD = 4.14); t (188) = −.563, p = .574. However, there was a statistically significant difference between the unexpected or violent loss group (M = 4.16, SD = 1.44) and the natural loss group (M = 4.67, SD = 1.50) with regard to venting; t (188) = −2.26, p = .025 with a small effect size (eta squared = .026). This suggested that the natural loss group endorsed venting more frequently than the unexpected or violent loss group.
Summary of Logistic Regression for Coping Strategies and Presence of PGD.
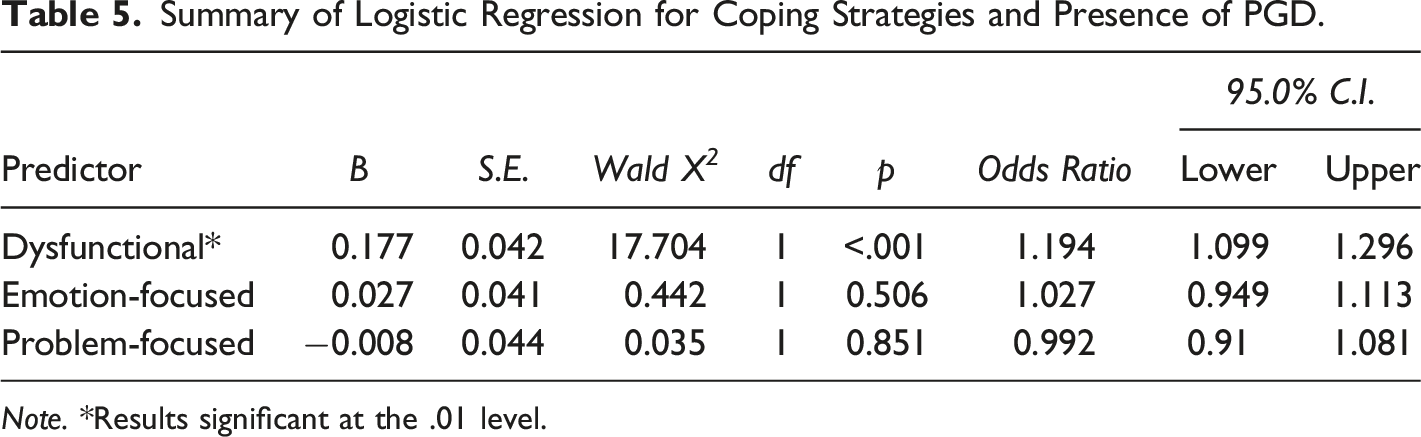
Note. *Results significant at the .01 level.
Summary of Logistic Regression for Dysfunctional Coping Strategies and Presence of PGD.
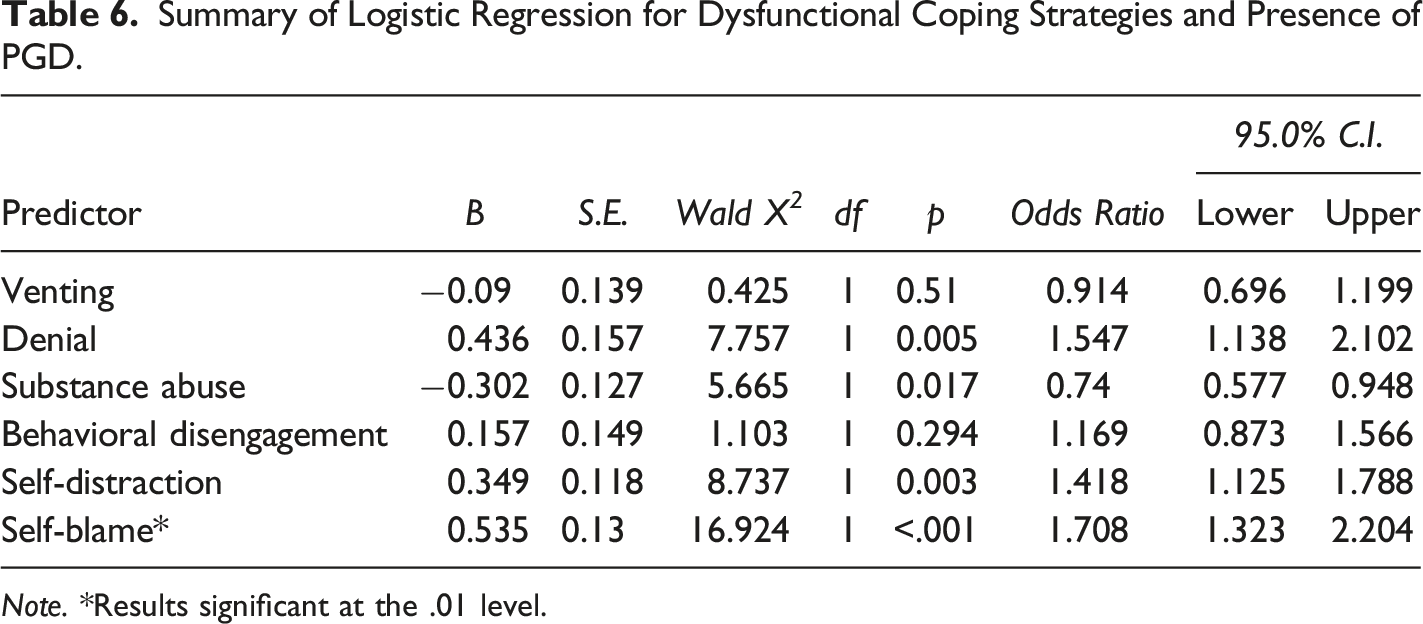
Note. *Results significant at the .01 level.
Summary of Logistic Regression for Relationship to the Deceased and Presence of PGD.
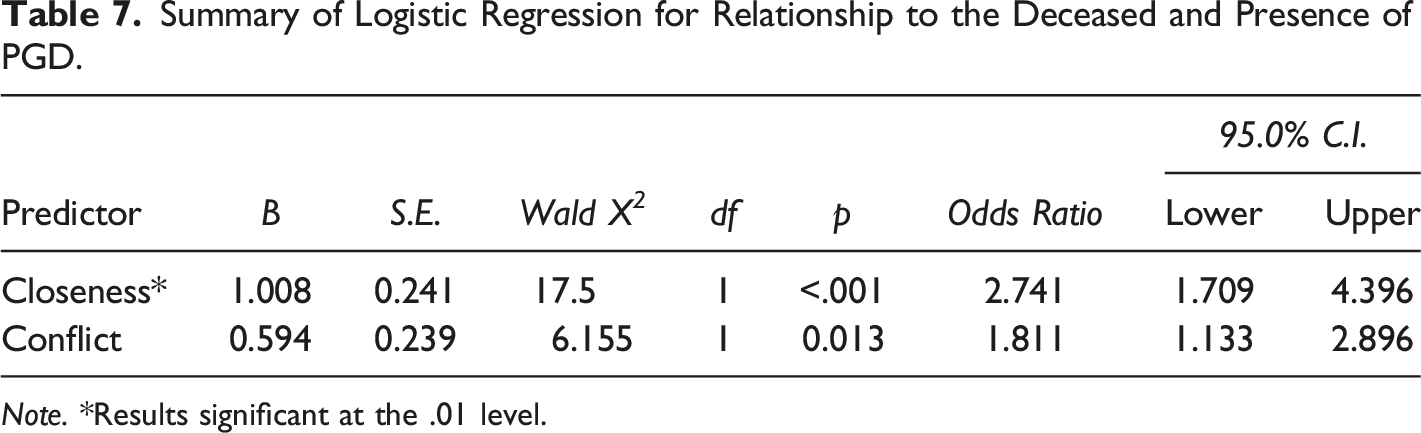
Note. *Results significant at the .01 level.
Discussion
The aim of this study was to examine how type of loss (i.e., unexpected or violent vs. natural) influenced the presence of PGD and coping. Secondly, this study sought to determine associations between the presence of PGD and the relationship with the deceased prior to the death loss. A goal of the study was to identify how risk factors contribute to the presence of PGD. Contradicting previously literature findings that unexpected or violent loss increases PGD severity (Buckley et al., 2015; Doering et al., 2022), there were not any differences in the presence of PGD between those bereaved by natural loss versus unexpected or violent loss. Yet, Sekowski and Prigerson (2022) noted that there was a weak association between unexpected loss and PGD severity. The lack of difference between these groups should be considered by clinicians when assessing for PGD.
Results of this study suggested that participants who had a presence of PGD endorsed higher scores of dysfunctional coping strategies including self-blame, which aligns with previous literature (Fisher et al., 2020; Wenn et al., 2019). Self-blame as described in loss rumination has demonstrated to be a contributor of PGD (Smith & Ehlers, 2021). These findings may be further explained by the perception of dysfunctional coping strategies require less effort as compared to emotion-focused or problem-focused coping. For example, Wenn et al. (2019) noted that the use of dysfunctional coping strategies may be related to the mental load of using coping strategies related to emotional processing, wherein bereaved individuals report exhaustion. Perpetuating symptoms of PGD via thought processes can develop into a feedback loop or cycle, which influences the coping strategies utilized by bereaved individuals (Smith & Ehlers, 2021). Furthermore, Prigerson et al. (2022) suggested that self-blame impedes the early grieving process, which may contribute to the development of PGD. It is recommended that clinicians assist clients with replacing dysfunctional coping with problem-focused coping strategies, which is perceived as the most beneficial coping strategy for those with PGD (de la Morena & Cruzado, 2013). Bereaved individuals can use the information in this study by re-evaluating the effectiveness of their coping skills, which may encourage them to pursue clinical treatment. Future studies should consider the influence of COVID-19 on coping strategies since individuals have been limited in coping due to previous quarantine guidelines (Fisher et al., 2022) and the lack of closure.
In this study, closeness to the deceased prior to the loss explained the presence of PGD, which has also been demonstrated in the work by Harrison et al. (2021) and Heeke et al. (2017). Stronger attachments to the deceased have added to the complexity of prolonged grieving processes (Djelantik et al., 2017; Sekowski & Prigerson, 2022). On the contrary, both closeness and conflict have contributed to grief severity (Bottomley et al., 2019; Smigelsky et al., 2020). These results offer further evidence to prior literature that closeness prior to the death loss has a strong relationship with PGD; however, conflicting findings across studies highlights the need for further research.
With regard to this study, generalizability is of concern. Although participants indicated varying locations around the United States, the majority of participants were located in the southern United States. Moreover, the majority of the participants of the sample identified as white and or cisgender women, demonstrating a lack of racial and gender diversity within the study. Due to the non-probability sampling method, there may be an overrepresentation of individuals that have sought support, which excludes those that have coped on their own; however, specific groups such as those bereaved by multiple losses or directly witnessed the death were excluded to limit bias. Future studies to incorporate samples with greater diversity, substance abuse disorder, and multiple losses or directly witnessing the death. This study relied on self-report measures, which can pose a concern with regard to construct validity. The utilization of survey as the method of data collection can also threaten internal validity as participants are responsible for their own interpretation of items. Nevertheless, the instrumentation selected for the study demonstrated adequate reliability and validity, resulting in the reduction of variable error. Thirdly, a limitation of this study was the lack of differentiation between unexpected and violent loss. Some of the participants in this study who reported a natural loss selected that the death was unexpected. It is specifically recommended that prospective studies focus on either unexpected or violent losses rather than including these terms together as this would provide further clarification with regard to the extensivity of grief experienced by bereaved individuals.
The findings of this study emphasize the importance of understanding the level of closeness or conflict to the deceased prior to the death loss and encourage the need for continued research on prolonged grief can provide normalization and validation for bereaved individuals. Closeness and dysfunctional coping offered explanation for the presence of PGD experienced by bereaved adults. Overall, the findings of this study demonstrate the importance of understanding PGD as a diagnosis in the DSM-5-TR along with the multiple factors that limit an individual’s ability to process grief.
Footnotes
Acknowledgements
We are grateful for each of the participants that contributed to this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial funding was provided by the Department of Special Education, Rehabilitation, and Counseling in the College of Education at Auburn University. Financial funding supported the raffle offered to participants as incentive for completing the survey in the study.
Ethical Statement
Data Availability Statement
Participants in this study did not consent to have their data shared publicly. Due to the sensitive nature of the topic of the study, supporting data is not available.