
Abstract
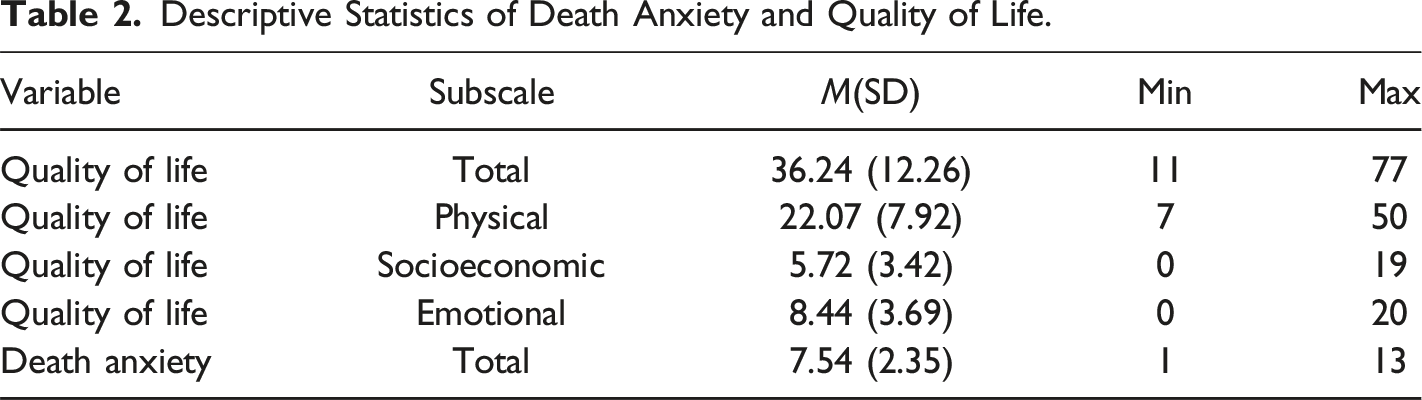
This study aimed to investigate the relationship between death anxiety and QoL in a sample of Iranian heart failure (HF) patients. A cross-sectional correlational design was employed to examine this relationship in a sample of 296 HF patients. Participants were recruited using convenience sampling from teaching hospitals in Kermanshah City, western Iran, between October and December 2023. Data were collected using a demographic questionnaire, the Templer Death Anxiety Scale (TDAS), and the Minnesota Living with Heart Failure Questionnaire (MLHFQ). Participants reported moderate to high levels of death anxiety (Mean [SD] = 7.54 [2.35]) on the TDAS and moderate to poor QoL (Mean [SD] = 36.24 [12.26]) on the MLHFQ. The statistical methods used in this study included descriptive statistics, independent t-tests, one-way analysis of variance (ANOVA), Pearson correlation coefficient, multiple linear regression analysis, and the Kolmogorov-Smirnov test. All statistical analyses were performed using SPSS version 26, with a significance level set at 0.05. A significant positive correlation was found between death anxiety and QoL (r = 0.329, p < .001), indicating that higher levels of death anxiety were associated with lower QoL. These results underscore the importance of addressing death anxiety in HF patients to improve their QoL. Interventions targeting the reduction of death anxiety and the enhancement of QoL are essential for optimizing care for this vulnerable population. The study recommends the implementation of psychological interventions, support groups, comprehensive counseling, education, and regular assessments for this purpose.
Introduction
Heart failure (HF) has emerged as one of the most prevalent cardiovascular diseases globally, imposing a substantial burden on healthcare systems worldwide. Approximately 64 million individuals are currently living with HF (Shahim et al., 2023), and this figure is projected to surge by 50% by 2030 in low- and middle-income countries (Lippi and Sanchis-Gomar, 2020). The American Heart Association (AHA) defines HF as a clinical syndrome resulting from structural and functional impairment of the ventricles, characterized by the heart’s inability to pump blood to the body effectively (Heidenreich et al., 2022).
A significant challenge faced by HF patients is the prevalence of psychiatric comorbidities, with anxiety being one of the most common (Costa et al., 2022). Anxiety, in general, is an emotional response to perceived threats or danger (Yıldırım and Kocatepe, 2023). One particularly anxiety-provoking concept is death. The contemplation of death can induce anxiety in anyone, although individual reactions vary based on personal experiences and attitudes toward life (Jaberi et al., 2022). Excessive preoccupation with death can have detrimental psychological consequences, leading to heightened anxiety when these thoughts become uncontrollable (Yıldırım and Kocatepe, 2023). For individuals with chronic conditions like HF, anxiety can be exacerbated. Anxiety in HF patients is associated with adverse clinical outcomes (Aggelopoulou et al., 2017; Easton et al., 2016), potentially impairing cardiac function and increasing mortality rates (Hiriscau and Bodolea, 2019). HF patients may experience elevated levels of anxiety due to factors such as progressive physical symptoms, complex treatment regimens, ineffective coping mechanisms, social isolation, fear of death, hopelessness, and financial concerns (De Jong et al., 2011).
Death anxiety, a transdiagnostic construct, is a prevalent anxiety type among these patients. It encompasses diverse facets of death, including self-death apprehension, fear of others’ demise, the dying process, and the unknown (Zuccala et al., 2022). Generally, death anxiety intensifies when individuals confront chronic or life-threatening illnesses (Sharif Nia et al., 2020). Research consistently indicates elevated death anxiety levels in HF patients (Asgari et al., 2018; Çamcı et al., 2024), which can adversely impact prognosis (Asgari et al., 2018). Furthermore, death anxiety underpins various psychological disorders (Iverach et al., 2014; Menzies et al., 2019). Thus, the significance of addressing death anxiety in these patients has become increasingly apparent. Soleimani et al. found that improved economic status, increased age, heightened hope, and stronger religious beliefs correlate with reduced death anxiety in patients with HF (Soleimani et al., 2020).
Quality of life (QoL) has emerged as a critical concern among patients with HF. The World Health Organization (WHO) defines QoL as an individual’s perception of life within the context of their culture and value systems concerning their goals, expectations, standards, and concerns (Organization., W. H, 1996). HF can detrimentally affect patients’ QoL by curtailing independence, hindering daily activities, and disrupting mental and psychosocial well-being (Fry et al., 2016, Comín-Colet et al., 2016). QoL is a paramount indicator of disease burden in HF patients, serving as a critical metric for assessing disease progression and clinical outcomes (Lawson et al., 2023). Enhancing QoL is now recognized as the primary objective of disease management (Ferreira et al., 2019). Factors such as disease severity, recurrent hospitalizations, unfavorable prognosis, suboptimal self-care, socioeconomic disparities, inadequate disease management knowledge, and limited familial or social support can adversely impact QoL in this patient population (Audi et al., 2017; Polikandrioti et al., 2015). Furthermore, a lower QoL is associated with increased mortality and hospitalization rates among HF patients (Johansson et al., 2021). Consequently, addressing QoL concerns is imperative for improving patient outcomes.
As previously mentioned, HF is a chronic cardiovascular condition that significantly compromises both the physical and psychological well-being of affected individuals. One prominent psychological consequence of HF is death anxiety, which can negatively impact patients’ QoL. Given the pivotal role of QoL in overall health and recovery, understanding the relationship between death anxiety and QoL in HF patients is crucial. Such knowledge not only illuminates the impact of death anxiety on QoL but also identifies potential intervention points for improving patient outcomes. Additionally, cultural and social factors can significantly influence both death anxiety and QoL perceptions. Therefore, it is essential to conduct country-specific studies to tailor interventions effectively (Hadian et al., 2021; Sarani et al., 2020; Sheikhbardsiri et al., 2022). While the importance of this topic is evident, research in this area, particularly in Iran, remains limited. Previous studies have primarily focused on the physical aspects of HF, neglecting the psychological dimensions. By investigating the relationship between QoL and death anxiety in Iranian HF patients, this study aims to contribute to the development of more effective interventions and strategies to enhance QoL. Also, this research can empower healthcare providers to recognize the significance of addressing psychological factors in HF management. By adopting a more comprehensive and patient-centered approach, healthcare professionals can ultimately improve patient outcomes. Therefore, this study aims to investigate the relationship between death anxiety and QoL in a sample of Iranian HF patients.
Method
Study Design and Participants
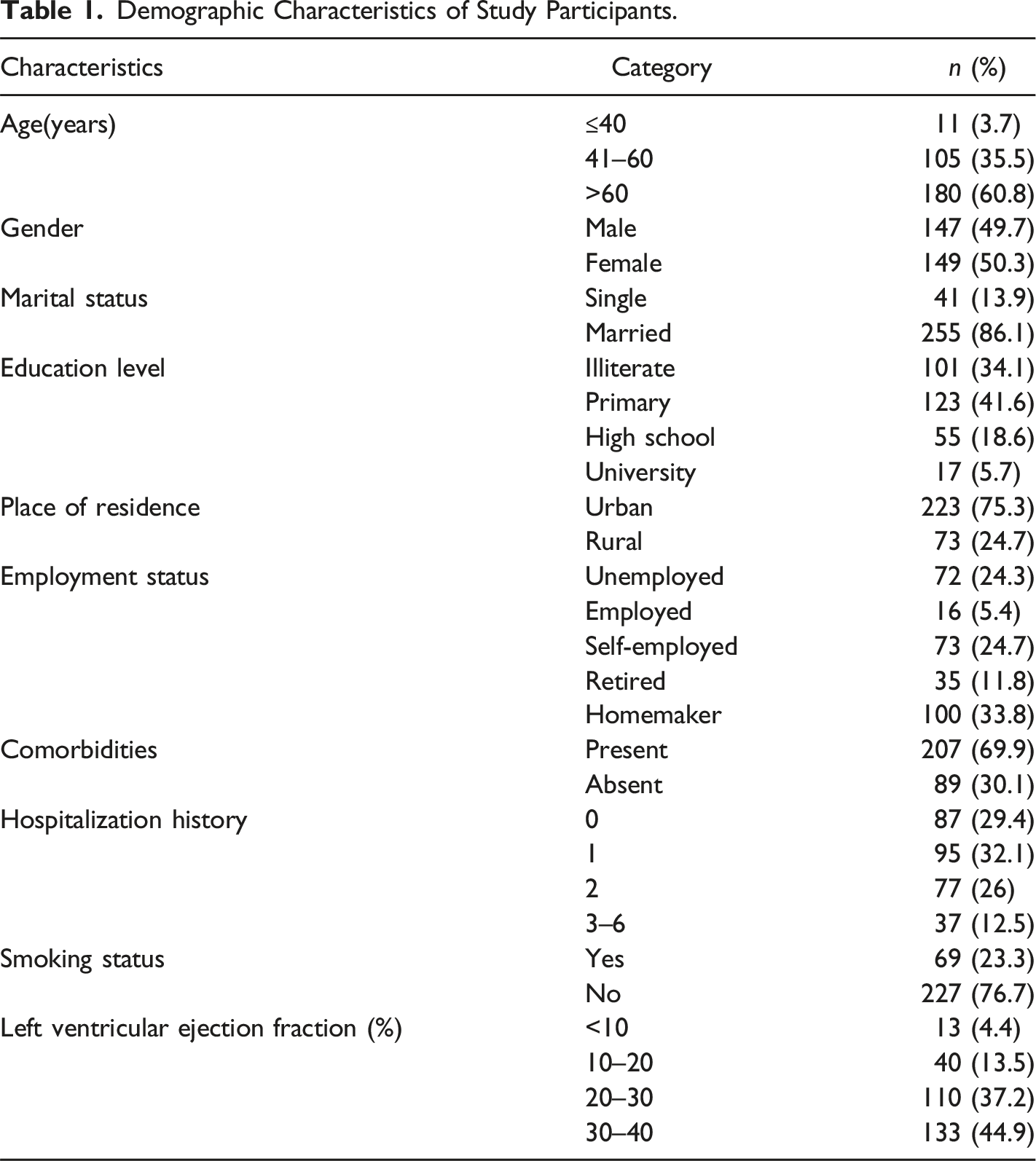
A cross-sectional correlational design was employed in this study. Participants were recruited using a convenience sampling method from a population of patients with HF seeking treatment at teaching hospitals in Kermanshah City, western Iran, between October and December 2023. Inclusion criteria for participants were as follows: age 19 years or older, a confirmed medical diagnosis of heart failure by a cardiologist, orientation to time, place, and person, stable vital signs, absence of severe mental disorders (as documented in medical records), and voluntary provision of informed consent. Of the initial 338 participants, 42 were excluded due to incomplete questionnaire responses (missing data >10%). The final sample consisted of 296 patients, yielding a response rate of 92.15%.
Sample Size and Power
To determine the necessary sample size for detecting a statistically significant relationship between death anxiety and QoL in Patients with HF, a power analysis was conducted. Assuming a minimum correlation coefficient of −0.2 between the two variables (as suggested by previous research (Jaberi et al., 2022)), a sample size of 265 was calculated to achieve a power of 90% at a 95% confidence level using the following formula:





A power analysis determined a minimum sample size of 265 participants to detect a significant relationship between the variables. To enhance the study’s power and precision, the sample size was increased to 296 participants.
Data Collection
Following coordination with Imam Ali and Imam Reza teaching hospitals, data were collected from patients in the CCU and post-CCU wards. To maximize participant recruitment, data collection occurred across various shifts (morning, afternoon, and night) throughout the week. Eligible patients were identified based on the inclusion criteria. After providing detailed information about the study and assuring participants of data confidentiality, written informed consent was obtained. Data were collected through self-administered questionnaires. For participants with illiteracy, questionnaires were completed through face-to-face interviews conducted by the researcher.
Instruments
Demographic Information Questionnaire
A researcher-developed questionnaire was employed to collect demographic data, including age, gender, education level, hospitalization history, marital status, place of residence, employment status, comorbidities, smoking status, and cardiac output.
Templer Death Anxiety Scale (TDAS)
Participants’ death anxiety levels were assessed using the 15-item Templer Death Anxiety Scale (TDAS) (Templer, 1970). The TDAS is a well-established measure with demonstrated reliability and validity in the Iranian population (Soleimani et al., 2016). Items are rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree), with six items reverse-scored. Total scores range from 15 to 75, with higher scores indicating greater death anxiety. Cut-off scores for mild, moderate, and severe death anxiety are 15–35, 36–55, and 56–75, respectively (Soleimani et al., 2016). In the current study, the TDAS demonstrated excellent internal consistency (Cronbach’s alpha = 0.84) and content validity (Content Validity Index = 0.87, Content Validity Ratio = 0.81).
Minnesota Living with Heart Failure Questionnaire (MLHFQ)
The Minnesota Living with Heart Failure Questionnaire (MLHFQ) was employed to assess participants’ QoL. This 21-item self-report measure evaluates the physical, emotional, and socioeconomic impacts of HF (Rector and Cohn, 1992). Items are rated on a 6-point Likert scale (0 = none to 5 = very much), with higher scores indicating poorer QoL. The MLHFQ has demonstrated robust psychometric properties in previous research, including a Cronbach’s alpha of 0.95 in the Iranian context (Eskandari et al., 2015).
Ethical Considerations
Ethical approval was obtained from the university’s research department prior to study commencement (IR.KUMS.REC.1402.247). After clarifying the study objectives and assuring participants of the confidentiality of their information, written informed consent was obtained from the participants, and the questionnaires were distributed among them. In addition, the principles of the Helsinki Declaration were observed. All methods were performed per the relevant guidelines and regulations.
Data Analysis
Descriptive statistics were used to summarize data, with means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Independent t-tests and one-way analysis of variance (ANOVA) were employed to examine the relationship between death anxiety scores, QoL, and demographic characteristics. To examine the relationship between death anxiety and QoL, a Pearson correlation coefficient was calculated. To identify factors associated with death anxiety and QoL while controlling for other variables, multiple linear regression analysis was conducted using the enter method. Prior to analysis, the normality of the data distribution was evaluated and confirmed using the Kolmogorov-Smirnov test. All statistical analyses were performed using SPSS version 26, with a significance level of 0.05.
Results
Demographic Characteristics of Study Participants.
Descriptive Statistics of Death Anxiety and Quality of Life.
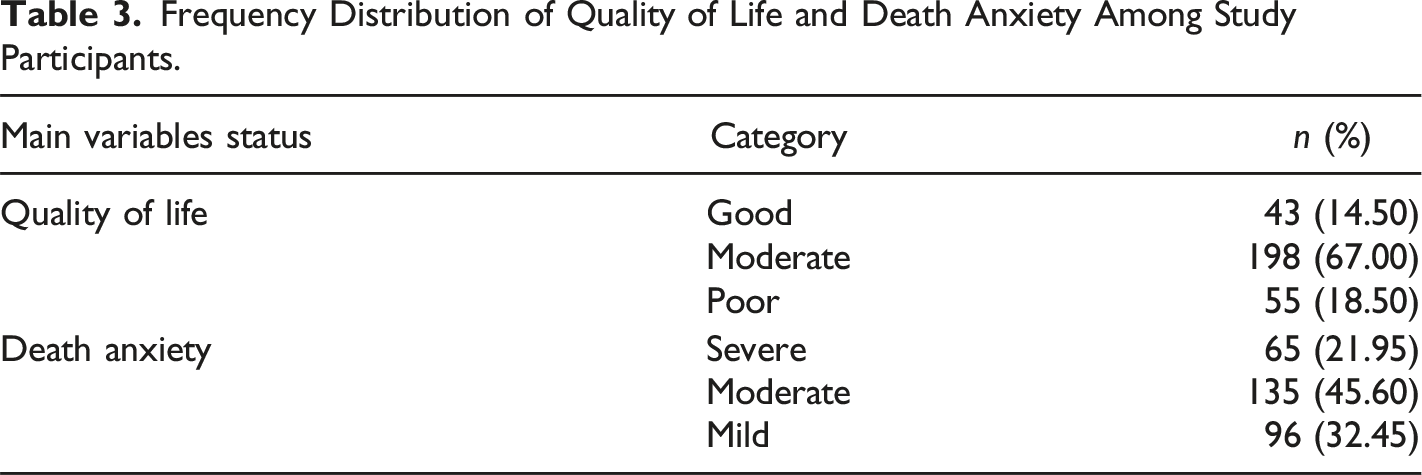
Frequency Distribution of Quality of Life and Death Anxiety Among Study Participants.
Correlations Between Death Anxiety and Quality of Life Dimensions.
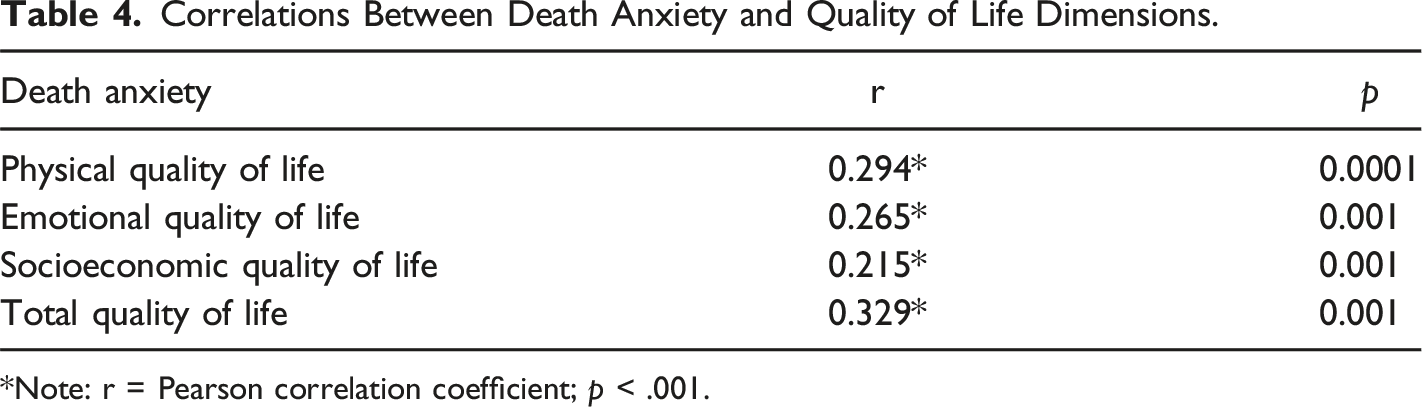
*Note: r = Pearson correlation coefficient; p < .001.
Discussion
The present study aimed to investigate the relationship between death anxiety and QoL among HF patients attending teaching hospitals in Kermanshah, western Iran. Death anxiety is a concept encompasses diverse facets of death, including self-death apprehension, fear of others’ demise, the dying process, and the unknown (Zuccala et al., 2022). This disorder can potentially worsen the prognosis of HF (Asgari et al., 2018) and lead to various psychological disorders in affected patients (Iverach et al., 2014; Menzies et al., 2019), significantly impacting their lives.
Results of the present study revealed that 67.55% of HF patients suffered from moderate to severe levels of death anxiety. Asgari et al. found that over 90% of HF patients experienced moderate to severe levels of death anxiety (Asgari et al., 2018). Similarly, Çamcı et al. (2024) reported that 62% of HF patients exhibited significant death anxiety (Çamcı et al., 2024). In a study by Yıldırım and Kocatepe (2023) on 300 patients with acute myocardial infarction in Turkey, most participants experienced severe or panic levels of death anxiety (Yıldırım and Kocatepe, 2023). These findings align with the results of the present study. Heart patients and those with other chronic diseases (such as cancer and hemodialysis patients) face similarly challenging circumstances in their struggle with illness and frequently grapple with the issue of death; thus, contemplating and fearing death is common among them. However, the results of a study by Seyedoshohadaee et al. (Seyedoshohadaee et al., 2019) on caregivers of multiple sclerosis patients showed that they often experienced low levels of death anxiety. The discrepancy between the results of this study and the present research may be attributed to the study population, as Seyedoshohadaee et al. (Seyedoshohadaee et al., 2019) measured death anxiety in caregivers rather than patients.
Results indicated that 67% of patients reported a moderate QoL. Overall, the majority (85.5%) experienced moderate to low QoL. The physical dimension yielded the highest mean QoL score, while the socioeconomic dimension demonstrated the lowest. This suggests that study participants with HF exhibited the greatest challenges in the physical domain, followed by emotional and socioeconomic domains. In alignment with the World Health Organization (WHO), QoL is an individual’s perception of life within the context of their culture and value systems concerning their goals, expectations, standards, and concerns (Organization.). HF negatively impacts patients’ QoL by diminishing independence, impairing daily activities, and compromising psychological and psychosocial well-being (Fry et al., 2016, Comín-Colet et al., 2016). Consistent with these findings, the study conducted by Aggelopoulou et al. on 231 patients with HF in Greece showed that, on average, these patients suffer from a low QoL (Aggelopoulou et al., 2017). Also, Adeeb et al. reported a low overall QoL among 132 cardiovascular patients using the World Health Organization Quality of Life (WHOQOL) scale (Adeeb et al., 2017). Furthermore, a systematic review and meta-analysis by Moradi et al. (Moradi et al., 2020) revealed that general QoL measures indicated a moderate QoL, while specific instruments identified a poorer QoL in chronic heart failure (CHF) patients. These findings align with the present study. While methodological variations existed across studies, the consensus is that cardiovascular patients experience diminished QoL.
The present study revealed a significant positive correlation between death anxiety and physical QoL among patients with HF. These findings suggest that as death anxiety increases in this patient population, their physical QoL diminishes. Consistent with these results, previous research by Adeeb et al. (Adeeb et al., 2017) on cardiovascular patients and Seyedoshohadaee et al. (Seyedoshohadaee et al., 2019) on caregivers of multiple sclerosis patients demonstrated that increased death anxiety was associated with decreased physical QoL. Additionally, Rechenberg et al. (Rechenberg et al., 2020) reported an inverse correlation between anxiety and physical QoL among 70 HF patients. Furthermore, the study by Ruku et al. on 180 patients with HF showed that physical performance is positively associated with health-related QoL (Ruku et al., 2024). Overall, a bidirectional relationship exists between physical QoL and death anxiety. Interventions aimed at addressing death anxiety may help alleviate physical symptoms and enhance the overall QoL for HF patients.
A significant positive correlation was observed between death anxiety and the emotional dimension of QoL among study participants. These findings suggest that elevated levels of death anxiety are associated with decreased emotional QoL in individuals with HF. Previous studies have consistently demonstrated that anxiety is associated with both the emotional dimension of QoL and the mental status of this patient population (Polikandrioti et al., 2019; Rechenberg et al., 2020). Additionally, Adeeb et al. (Adeeb et al., 2017) found a negative correlation between death anxiety and the psychological dimension of QoL in cardiovascular patients, suggesting that as death anxiety increases, the psychological aspect of QoL deteriorates. Furthermore, The results of the study by Fidelis and colleagues on 89 patients with HF showed that higher levels of anxiety in these patients are associated with lower emotional stability (Fidelis et al., 2021). The psychological impact of HF, characterized by uncertainty about the future and the potential for significant life disruptions, can precipitate heightened levels of death anxiety. Consequently, patients may experience exacerbated emotional distress and a decline in overall QoL.
A significant positive association was observed between death anxiety and the socioeconomic dimension of QoL in HF patients. These findings suggest that elevated death anxiety is associated with diminished socioeconomic QoL in this population. Generally, low socioeconomic status is associated with poor outcomes in patients with HF (Aguilera et al., 2023). Consistent with these results, Adeeb et al. (Adeeb et al., 2017) reported a link between death anxiety and social and environmental dimensions of QoL in cardiovascular patients. Moreover, Mushtaque et al. (Mushtaque et al., 2024) found that socioeconomic status is connected with poor QoL among elderly individuals with ESRD. The importance of social support in improving QoL was underscored by Bahrami et al. (Bahrami et al., 2013) in their study of Iranian women with cancer. Also, the results of the study by Yan and colleagues on 1552 patients with a confirmed diagnosis of CHF showed that anxiety, especially in older women and those with inadequate social support, significantly mediates the relationship between social support and mortality in this group of patients (Yan et al., 2022). Socioeconomic factors, including financial constraints and limited social resources, can significantly impact the QoL of HF patients by exacerbating disease symptoms, increasing anxiety, and hindering social participation. Conversely, adequate financial resources and strong social support networks may serve as protective factors against the development of elevated death anxiety and its associated adverse outcomes.
The present study revealed a significant positive correlation between death anxiety and overall QoL among HF patients. Previous research has consistently demonstrated a negative correlation between anxiety and QoL in HF patients (Mohannad, 2022; Vatutin et al., 2013). Similarly, Adeeb et al. found that QoL is negatively correlated with death anxiety in their study on a sample of 132 cardiovascular patients (Adeeb et al., 2017). Furthermore, Fidelis et al. reported that higher anxiety is associated with lower QoL in patients with HF (Fidelis et al., 2021). Consistent with these findings, previous research involving individuals with chronic renal failure (Jaberi et al., 2022) and women with cancer (Bahrami et al., 2013) reported a significant association between these variables. Also, Ji et al. (Ji et al., 2024) observed a negative correlation between death anxiety and QoL in a sample of Chinese patients with chronic diseases. In contrast, a study by Shafaii et al. (Shafaii et al., 2017) failed to identify a significant association between these variables in a cohort of hemodialysis patients. This discrepancy may be attributed to differences in patient populations. While hemodialysis patients often benefit from established treatment regimens and coping mechanisms, HF patients frequently experience symptom fluctuations and an uncertain prognosis. The perception of a declining cardiac function, coupled with the progressive nature of the disease, can evoke heightened levels of death anxiety, which may be exacerbated by physical symptoms such as dyspnea and fatigue.
Limitations
The generalizability of the study findings is constrained by its geographic scope, being limited to teaching hospitals in Kermanshah, Iran. Demographic, cultural, economic, and social factors inherent to the region may influence the observed associations and limit the extrapolation of results to other populations. The self-reported nature of the data is subject to potential biases. Given the sensitive nature of the questionnaire items and the psychological and physical burdens experienced by HF patients, social desirability bias and recall bias may have impacted the accuracy of responses. Furthermore, the relatively low educational attainment of a significant proportion of participants (75.7% illiterate or with primary education) could have compromised the reliability of self-reported data.
Future research should be conducted in diverse geographic locations with larger sample sizes to enhance the generalizability of these findings. Longitudinal studies can provide valuable insights into changes in death anxiety over time, allowing for the identification of causal relationships and the long-term impact of interventions. Incorporating objective measures, such as clinical assessments and physiological indicators, alongside self-reported data can offer a more comprehensive understanding of patients’ conditions.
Conclusion
The present study demonstrated a significant positive correlation between death anxiety and QoL among HF patients. These findings underscore the substantial burden of death anxiety on the overall QoL of this patient population. Given the observed association, interventions targeting the reduction of death anxiety through comprehensive QoL enhancement strategies are warranted. Such initiatives should prioritize identifying the modifiable factors influencing QoL and their integration into routine clinical care.
Future research should employ qualitative methods to delve deeper into the personal experiences and perspectives of HF patients regarding death anxiety and QoL. Additionally, investigating the impact of educational programs on reducing death anxiety and improving QoL, as well as the role of family, caregivers, and technology-based interventions (e.g., mobile applications) in managing death anxiety and enhancing QoL, is recommended. Cross-cultural comparisons can further illuminate how cultural differences influence the relationship between death anxiety and QoL in this patient population.
Footnotes
Acknowledgements
The authors gratefully acknowledge the Research Council of Kermanshah University of Medical Sciences. (Grant Number: 4020470) for the financial support. This Work was performed in partial fulfillment of the requirements for (insert degree for master thesis) of (Mahla Merati) in Faculty of Nursing, Kermanshah University of Medical Sciences, Kermanshah, Iran.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by the Deputy of Research and Technology at Kermanshah University of Medical Sciences. The authors gratefully acknowledge the Research Council of Kermanshah University of Medical Sciences. (Grant Number: 4020470) for the financial support. This Work was performed in partial fulfillment of the requirements for (insert degree for master thesis) of (Mahla Merati) in Faculty of Nursing, Kermanshah University of Medical Sciences, Kermanshah, Iran.
Author Biographies