
Abstract
The aim of this study was to adapt the short form of Death Literacy Index (DLI-9) into Turkish and to examine its psychometric properties. This study has a methodological cross-sectional design. The study was conducted with a sample of 400 adults across Türkiye during October-November. Content Validity Index, Exploratory Factor Analysis (EFA), Confirmatory Factor Analysis (CFA), Convergent and Discriminant Validity Analyses, test-retest reliability, Cronbach’s α-coefficient, item-total-score correlation, 27% upper-lower-group item analysis and Hotelling-T2 test were used in data analysis. In the EFA analysis, the scale consisted of 2 factors. The original two-factor structure of the scale was confirmed by CFA. CFA model fit values were found as CMIN/DF = 2.078, RMSEA = 0.074, RMR = 0.077, SRMR = 0.0455, CFI = 0.960, NFI = 0.927, TLI = 0.945, GFI = 0.946, and AGFI = 0.906. The total Cronbach’s α reliability coefficient of the DLI-9 was found to be 0.84. This study indicates that scale is a reliable tool for evaluating death literacy in the Turkish population.
Introduction
Death is a universal and inevitable reality that people have to cope with in their lives (Çekiç et al., 2024). Death is not only an individual experience but also a social and cultural phenomenon. Death, encompassing various interpretations such as the unknown and annihilation, remains a taboo in numerous nations and cultures (Serra-Sutton et al., 2024). The removal of death from being a taboo, seeing it as a natural part of life, and being able to talk about death are related to the level of death literacy (DL) (Li et al., 2024).
The DL concept, developed as a result of years of research in Australia, encompasses all skills related to knowledge, experience, beliefs, and practices concerning death (Noonan et al., 2016). Understanding death, improving individuals’ quality of life, preparing for death, and determining the mourning processes, which constitute the content of palliative care, are included within the scope of death literacy (Leonard et al., 2022; Van Dinther et al., 2025). In this context, the Death Literacy Index (DLI) was developed by Leonard et al. (2022) to evaluate death and post-death processes, taking into account the comprehensive views and experiences of many experts and participants with experiences related to death.
The DLI consists of 29 statements in a 5-point Likert-scale, encompassing the sub-dimensions of “practical knowledge (talking support, hands-on care), experiential knowledge, factual knowledge, and community knowledge (others can help me provide end-of-life-care, support-groups in my community)” (Leonard et al., 2022). As DL, a new concept, has been understood, interest in scale has gradually increased, and social and cultural adaptations have begun to be made rapidly. It has been reported that the validity and reliability of the scale, which has been validated in the United Kingdom (2022), China (2023), Sweden (2023) and Türkiye (2024), is still being culturally adapted in many societies (Che et al., 2023; Graham-Wisener et al., 2022; Johansson et al., 2023; Semerci et al., 2024).
The authors developing the DLI found that, based on the feedback from researchers making cultural adaptations, there are generally very few cultural differences regarding DL. Based on the feedback and suggestions they received, the authors developed a shorter form of the DLI, without altering its original version, in order to improve the scale’s readability and applicability (Noonan et al., 2024). It is believed that researching individuals’ DL levels with this brief and practical tool will facilitate the work of all professionals in the fields of health and social sciences. This study was conducted with the aim of adapting the newly developed short form of the Death Literacy Index (DLI-9) into Turkish to evaluate DL in the Turkish population.
Methods
Study Design
The design of this study is cross-sectional and methodological.
Participants
The population of this study consisted of individuals aged 18 and over from across Türkiye. The criteria for inclusion in the study were being literate, consenting to participate in the study, and being 18 years old or older. According to DeVellis (2017), psychometric studies are reported to have a sample size of 200 for moderate, 300 for good, and 500 for excellent. The study was completed with 400 individuals who met the inclusion criteria, using the snowball sampling method.
As a result of analysis conducted to determine adequacy of sample size for validity and reliability analyses, Kaiser-Meyer-Olkin (KMO) coefficient was 0.819 and Bartletts test was χ2 = 623.397; p < .001. According to these results, it was concluded that sample size was sufficient for further analysis.
Data Collection Tools
The data were collected using the Personal Information Form and DLI-9.
Personal Information Form
In this form prepared by researchers, there are 8 questions including age, gender, educational, marital, employment status, income status, place of residence and death of a relative.
DLI-9
The scale was developed by Noonan et al. (2024). The scale consists-of 9-items.The five-point Likert type scale consists of 2 sub-factors. Factor 1 (4 items) addresses the private sphere and Factor 2 (5 items) addresses the public sphere. Although it has been shown that the DLI-9 has two factors, it is recommended to use it as a single scale with nine items. The Cronbach’s α-coefficient of the DLI-9 is 0.87, Cronbach’s α-coefficient for Factor 1 is 0.82, and Cronbach’s α-coefficient for Factor 2 is 0.87, indicating high internal reliability.
Procedure
There are many methods for adapting scales to different cultures. The translation and cultural adaptation process of the scale was carried-out in accordance with the guidelines published by Professional Society for Health Economics and Outcomes Research (ISPOR) (Wild et al., 2005). Firstly, permission for the use of the scale was obtained from the scale owner via e-mail. Then, to ensure the validity of the language, the scale was translated from English-to-Turkish by two independent translators who were fluent in-both languages. Translation was reviewed and evaluated by researchers. The scale was then evaluated by a Turkish language expert in terms of grammar and comprehensibility. Necessary corrections were made by researchers. The Turkish version of the scale was retranslated into English by two different independent translators. After back translation, it was confirmed that the Turkish version of the scale was very similar to the English version. Subsequently, to evaluate the content validity of the scale, the opinions of total of 4 experts from the fields of public health nursing, internal medicine nursing, psychiatric nursing and basic medical sciences were consulted. After expert opinion, the Content-Validity-Index (CVI) was calculated and minor corrections were made. Afterwards, a pilot study was conducted with 30 individuals with similar characteristics to the sample. In the pilot study conducted to evaluate the readability and comprehensibility of the scale, no negative feedback was received, and no corrections were made. The final version of the scale was created. Those who had participated in the pilot study weren’t included in the study-sample.
Data Collection
The data were collected online by the researchers between October 20 and November 20, 2024, using the Personal Information Form and the Turkish version of scale via Google Forms. Before starting the survey questions in the online form, a written explanation about the study was provided, and a question was asked to determine whether they were willing to participate in the research.
Ethics
Permission for the use of the scale was obtained from the owner of scale via e-mail. Ethics committee approval (17.10.2024/Decision-no:70–08) was obtained for the research. Before starting the survey questions in the online form, a written explanation about the study was provided. Consent was obtained by asking a question regarding their willingness to participate in the study. In this study, scientific and universal principles were followed. The study was conducted in accordance with the Declaration of Helsinki.
Analysis
IBM SPSS (v. 25) and AMOS (v. 21) software packages were used to analyse the data. Statistical significance level was accepted as p < .05. Descriptive statistics were provided for the participants’ demographic characteristics. The distribution of the data was analysed in terms of skewness and kurtosis and it was determined that the data showed a normal distribution between ±2. For validity, CVI, Exploratory Factor Analysis (EFA), and Confirmatory Factor Analysis (CFA) were conducted. Polit and Beck CVI method was used to determine the content validity of the scale-items. Four experts were consulted for the scale’s CVI. EFA was conducted with 200 data points to determine the construct validity of the scale. The original two factor structure of scale was confirmed by CFA with 200 different data. Before starting the CFA in AMOS, it was evaluated whether the data were normally distributed (multivariate), whether there was multicollinearity and whether the sample size was sufficient. All assumptions were met. Maximum Likelihood estimation method and covariance matrix were used for CFA. For reliability, test-retest reliability, Cronbach’s α-coefficient, item-analysis based on item-total-score correlation and item-analysis based on 27% upper-lower-groups were performed. Hotelling-T2 test was applied to determine response bias of the scale. Average-Variance-Extracted (AVE) and Composite-Reliability (CR) were calculated for the validity of convergence and divergence.
Results
The mean age of the participants was 35.31 ± 17.90 years (18–88 years). 53.3% of the participants were female, 57% were single, 72% were high school graduates, 70% were not employed, 60% had an income-equal to their expenses, 60.5% lived in urban areas, and 73.5% had experienced the death of a close relative.
Validity Analyses
Content Validity
The opinions of 4 experts were consulted for the content validity of scale. Item-Content Validity Index (I-CVI) and Scale-Content Validity Index (S-CVI) were calculated using the Polit and Beck CVI method. I-CVI and S-CVI/Ave were set as 1.00.
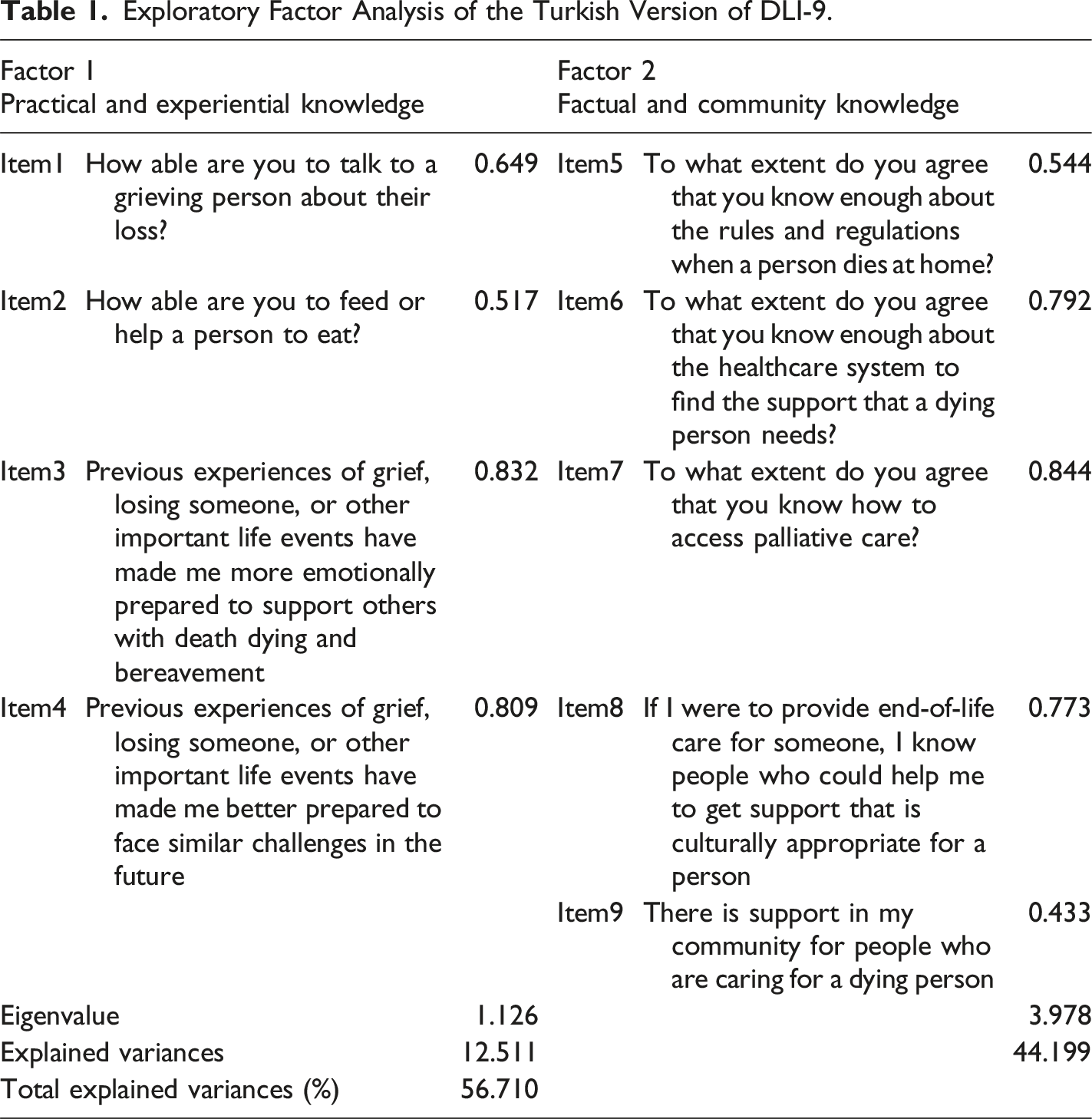
EFA
Exploratory Factor Analysis of the Turkish Version of DLI-9.
CFA
CFA was conducted on the data to confirm two-factor construct validity of the Turkish version of scale. As a result of the CFA, the factor loadings of 9 items were found to be between 0.55 and 0.83. CFA model fit values were found as CMIN = 54.032, DF = 26, CMIN/DF = 2.078, RMSEA = 0.074, RMR = 0.077, SRMR = 0.0455, CFI = 0.960, NFI = 0.927, TLI = 0.945, GFI = 0.946, and AGFI = 0.906.
Factor loadings of scale-items related to CFA are shown by the path diagram (Figure 1). Path diagram.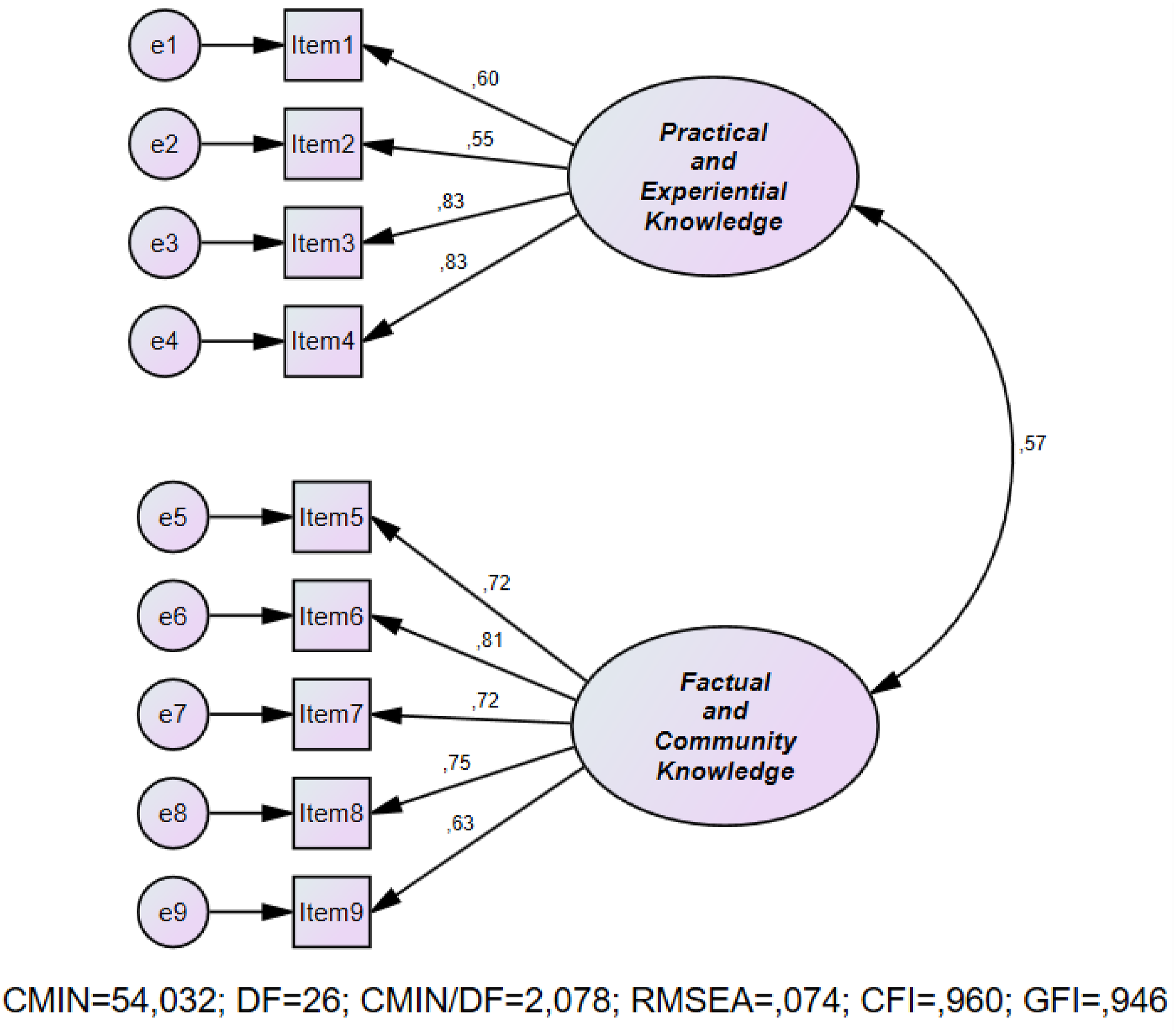
Convergent and Discriminant Validity Analyses
For the first sub-dimension (Practical and Experiential Knowledge), the CR value was found to be 0.801, and for the second sub-dimension (Factual and Community Knowledge), it was found to be 0.848. The AVE values for the sub-dimensions were determined to be 0.510 (1st sub-dimension) and 0.530 (2nd sub-dimension), respectively. The results of the analysis showed that the CR was higher than the AVE, confirming that the scale has both discriminant and convergent validity.
Reliability Analyses
Test-Retest Analysis
Test-Retest Results Based on Overall DLI-9 and Its Subscales.
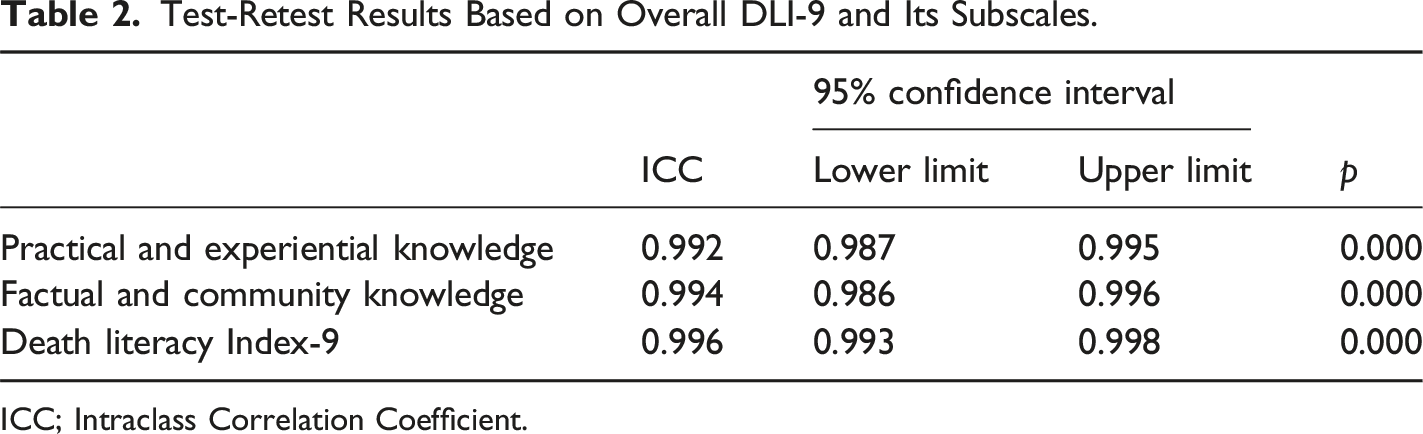
ICC; Intraclass Correlation Coefficient.
Cronbach’s α-Reliability Coefficient, Item Analysis
Cronbach α Reliability Coefficient and Item Analysis of DLI-9.
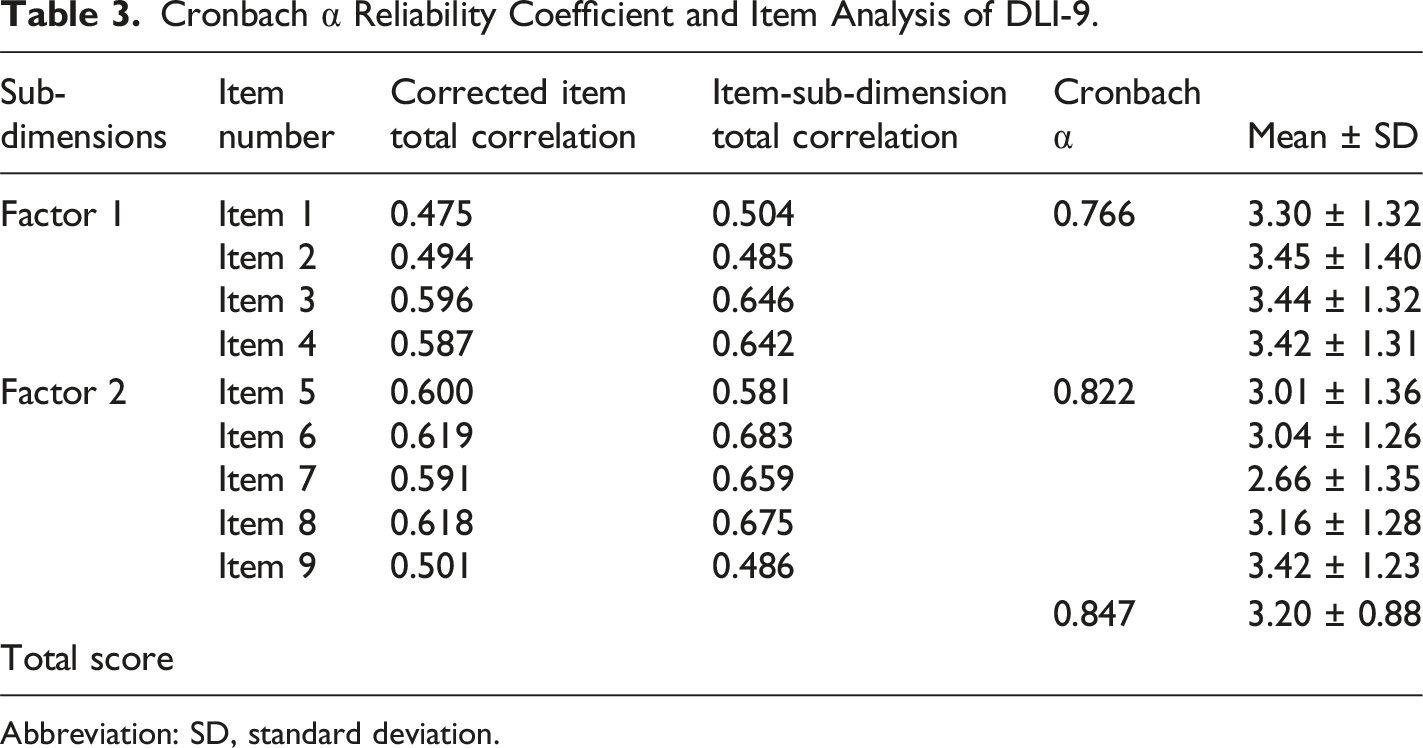
Abbreviation: SD, standard deviation.
In the item analysis based on the upper and lower 27% groups, the difference between the means of the upper and lower groups was determined using an independent-samples-t-test. It was found that the items of the scale had a discriminative feature in the researched subject (p < .001). As a result of the Hotelling-T2 test conducted to evaluate whether the individuals’ responses to the scale-items were equal, Hotelling-T2 = 175.891 p < .001 was found.
Discussion
DL is the knowledge and skills that enable understanding the care options during the final stages of life and the dying process, and making informed decisions based on these options (Noonan et al., 2016). The evaluation of DL is important in terms of developing care options during the end-of-life and death process. The DLI was developed by Leonard et al. (2022), and adapted into Turkish by Semerci et al. (2024). It would be useful to use a short survey to evaluate DL (Noonan et al., 2024). Accordingly, in this study, the DLI-9 developed by Noonan et al. was adapted to Turkish culture and its psychometric properties were examined. This study is the first study on the adaptation of the DLI-9 to different cultures.
Validity Analyses of the DLI-9
Content Validity
Translation and cultural adaptation process of the DLI-9 was carried out in accordance with the guidelines published by the ISPOR (Wild et al., 2005). Content-validity was used to determine the extent to which entire scale and each item in it represents the construct to be measured (Çam & Baysan-Arabaci, 2010). Polit and Beck’s (2006) CVI, one of the content validity methods, rates expert opinions as (1)'Not appropriate’, (2)'Somewhat appropriate’, (3)'Quite appropriate’, and (4)'Extremely appropriate’. In this method, the number of experts marking options (3) and (4)is divided by total number of experts to obtain I-CVI and S-CVI. If the number of experts is between 3 and 5, these values are expected to be 1.00 (Polit & Beck, 2006). The I-CVI and, S-CVI values of DLI-9 translated into Turkish, which were calculated using 4 expert evaluations, were found to be high. Additionally, no significant issues regarding the clarity of the scale items were reported by the participants in the pilot study. These results supported that the translation process was successful and the DLI-9 had sufficient content validity in the Turkish sample.
Construct Validity
Before examining factor structure of a scale, KMO-test is applied to evaluate the adequacy of the sample for factor-analysis, and Bartlett-test is applied to assess its suitability. To conduct factor-analysis, KMO-value is expected to be above 0.60, while a value above 0.80 indicates very-good-fit. Bartlett-test result of p < .05 indicates that correlation matrix is significant, the dataset is appropriate, and the sample size is adequate (Karagöz & Bardakçı, 2020; Kamiloglu & Vural, 2022). In this study, the KMO and Bartlett tests showed that, the sample size was sufficient and the dataset was suitable for factor analysis.
In this study, EFA and CFA were applied to evaluate construct-validity. In EFA, it is recommended that factor loadings be at least above 0.32. In determining the factors, those with an eigenvalue greater than 1.00 are considered significant, and the high variance ratios enhance the strength of the scale’s factor construct. In the literature, it is stated that a variance ratio between 40% and 60% is sufficient (Gürbüz & Sahin, 2017). In this context, it can be said that the results of current study are consistent with the literature, that there isn’t need-to remove any items according to the EFA results, and that the scale has a strong construct validity.
The two-factor structure present in the original form of the DLI-9 was also validated in the Turkish version. According to the results-of CFA analysis, the factor loadings of all-items were found to be above 0.30 (Karagöz & Bardakçı, 2020; Çapık et al., 2018). During CFA, various fit indices related to the scale are examined, and it is expected that these indices reach a certain level (Brown, 2015; Karagöz & Bardakçı, 2020). The SRMR, RMSEA, TLI, and CFI fit index values of the original form of the scale were found to be within acceptable limits (Noonan et al., 2024). In this study, it was determined that the CMIN/DF, RMSEA, RMR, SRMR, GFI, AGFI, NFI, TLI, and CFI values are within acceptable limits, consistent with the original scale (Brown, 2015; DeVellis, 2017). The CFA results obtained in this study have demonstrated the construct validity of the scale and confirmed that scale is a valid-measurement-tool.
It is recommended that convergent and discriminant validity analyses be conducted to ensure that the scale items, and sub-dimensions can measure targeted concept without interfering with other concepts (Coskun et al., 2024). In the literature, it is emphasized that CR values should be above 0.70, AVE values should be above 0.50, and CR-values should be greater than AVE-values (Tabachnick et al., 2013; Yaslioglu, 2017). The analysis results obtained in this study has revealed that the scale has both convergent and discriminant validity.
Reliability Analyses of the DLI-9
Test-Retest Reliability
It is recommended to evaluate the test-retest reliability and internal consistency for many multi-item scales such as self-report and observational scales (Polit & Beck, 2017). The test-retest coefficient should be high and the scores between the two measurements should not differ (Weir, 2005). In this study, two administrations were conducted with a three-week interval, and a high positive correlation was calculated between the first and second administrations. Additionally, a paired samples t-test was conducted, and the means of the first and second administrations were found to be very close and similar to each other (Karagöz & Bardakçı, 2020; Weir, 2005). In this context, it can be concluded that the measurements made at different times with the DLI-9 are similar and support reliability of scale.
Cronbach’s α-Reliability Coefficient, Item-Analysis
Whether the scale items are consistent with each other and whether they measure the same feature can be evaluated with Cronbach’s α-coefficient. Higher Cronbach’s α-coefficient, the more reliable scale is considered to be (Seçer, 2018; Tavsancil, 2006). In the present study, the Cronbach’s α-coefficient was calculated as 0.847 for the DLI-9, 0.766 for Factor 1, and 0.822 for Factor 2. In a similar manner to this study, the original scale’s Cronbach’s α value was reported as 0.879, with Factor 1 at 0.820 and Factor 2 at 0.872. In addition, the item-total-score, and item-sub-dimension total-score correlation values of all items in this study were above 0.40. A high item-total-score correlation indicates that relevant-item is appropriate for the theoretical construct being measured, and a correlation-coefficient of 0.20 and above is desirable (Karagöz & Bardakçı, 2020; Çokluk et al., 2018). These results supported the high internal consistency of the DLI-9. Accordingly, it can be stated that all the items in the DLI-9 have a homogeneous structure within themselves, similar to the original scale.
In the item discrimination analysis based on the bottom and top 27% groups, it is evaluated whether the scale can accurately distinguish between the situations related to the subject being investigated (Karagöz & Bardakçı, 2020). A significant difference is expected to be found between the bottom and top groups formed according to the total test scores (Büyüköztürk, 2008; Tavşancıl, 2006; Şencan, 2005). In this study, it can be concluded that the items of the DLI-9 have a distinctive feature regarding the subject being investigated.
The Hotelling-T2 test, conducted to determine the response bias of scale, examines whether the participants’ responses to the scale-items are equal to each other (Karagöz & Bardakçı, 2020; Özdamar, 2002). In this study, it was concluded that there is no response bias in the DLI-9. The reliability of the DLI-9 was supported by the results obtained from all reliability analyses.
Limitations
The participants were reached using the snowball sampling method. This situation may tend to result from the participation of individuals with higher DL, and data is based on self-reports from participants. The DLI-9 was developed in the Australian community and adapted to the Turkish community; it will need to be tested for use in other communities.
Conclusion
In conclusion, it has been observed that the DLI-9 is a valid, and reliable tool for assessing DL in Turkish society. This tool adapted to Turkish is short and practical for evaluating adults’ DL. The scale will facilitate the evaluation of DL for all professionals working in the fields of health and social sciences.
Footnotes
Ethical Approval
Before starting the study, approval was obtained from the Bayburt University Non-Interventional Clinical Research Ethics Committee (Decision No: 2024/70/8-Date:10/17/2024).
Informed Consent
Before starting the survey questions in the online form, a written explanation about the study was provided and a question was asked about whether they were willing to participate in the study. Those who agreed to participate in the study answered the survey questions.
Author Contributions: CRediT
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Upon reasonable request, data can be made available to researchers. Requests should be directed to the corresponding author.