
Abstract
This study aimed to establish the frequency and congruence between preferred and actual locations of expected pediatric deaths and to identify associated factors. A retrospective review of death review forms and medical records was conducted in two pediatric palliative care services in Sydney, Australia, involving 486 patients who died between January 2017 and May 2024). Hospital was the most common LOD (49.8%), then home (28.4%) and hospice (21.0%). At the last documented LOD conversation, 36.2% of families preferred home, 28.6% hospice and 26.4% hospital. Preferred LOD outcomes were achieved for 87.7% of families, although 21% who preferred a home death did not achieve this. Preferred and actual LODs of home were significantly associated with having a community palliative care referral and palliative care home visit. The findings highlight the importance of enabling families to plan for their child’s LOD, and ensuring preferences are documented and communicated across health services.
Pediatric palliative care (PPC) teams provide medical, emotional, and spiritual care to children with life-limiting conditions (LLCs) and their family (Australian Institute of Health and Welfare, 2024; Fields et al., 2023). PPC teams may provide this support from diagnosis of a LLC, through to the end of life and into the bereavement period. Given the nature and length of their involvement, PPC teams are uniquely positioned to guide families in meaningful discussions about their preferred location of death (LOD) and to implement the necessary supports to facilitate their preference.
The available options for the LOD may vary based on where families live and the services accessible to them. For a home death, the home environment is reviewed, specialized equipment may be installed, community healthcare services involved, and parents supported to manage the child’s medical needs (Hansson et al., 2023; Winger et al., 2020). A hospital death can occur at a local or tertiary pediatric hospital, and may occur in a hospital ward, intensive care unit, or sometimes the emergency department (Trowbridge et al., 2018). Pediatric hospices are purpose built to support the needs of children with LLCs including those at the end of life, providing a home-like environment, but with the medical equipment and appropriate multidisciplinary support (Bear Cottage, n.d.; Paediatric Palliative Care Australia & New Zealand, 2023). However, pediatric hospices are limited in number in developed countries and often non-existent in less developed countries (Arias-Casais et al., 2020).
In one of the largest population-based reviews and retrospective analyses of pediatric deaths conducted in 2008, hospital emerged as the most common LOD in all countries (Håkanson et al., 2017). More recent studies have also mostly found hospital to be the most common location of expected pediatric deaths in well-developed countries (Australian Institute of Health and Welfare, 2024; Gibson-Smith et al., 2021; Peláez-Cantero et al., 2023), although some studies have found very similar proportions across locations (Siden et al., 2008; Sneha et al., 2023; Wiener et al., 2020). Notably, parents have reported a better PPC experience when they were able to plan the LOD, regardless of the location chosen (Bluebond-Langner et al., 2013; Rainsford et al., 2018). Therefore, empowering families to plan for the LOD and providing them the flexibility to change their choice is considered an important aspect of high-quality PPC (Dussel et al., 2009; Paediatric Palliative Care Australia & New Zealand, 2023).
Families will differ in their preferences of LOD, depending on the accessibility of services and the needs and priorities of the family (Papadatou et al., 2021). Families may also change their preferences as new factors emerge, or as they prioritize different considerations at different stages of the child’s disease progression (Bluebond-Langner et al., 2013; Vickers et al., 2007). To our knowledge, only one study (Vickers et al., 2007) has recorded LOD family preferences at multiple time points. In that study, 68% of families initially preferred a home death, but by the last month of their child’s life, this preference increased to 80% (Vickers et al., 2007). There is a need for a better understanding of how parental preferences for LOD change over time.
Although healthcare professionals endeavor to support the family’s goals of care for LOD, there are various reasons why achieving these goals is not always attainable. It may be difficult to instate certain supports if there is a lack of timely planning, thus limiting the options for LOD (Montel et al., 2009). Across varied international contexts - including Australia (n = 301) (Australian Institute of Health and Welfare, 2024), Spain (n = 164) (Peláez-Cantero et al., 2023), and the US (two studies, n = 140 (Dussel et al., 2009) and n = 150 (Lee et al., 2023))- between 87% and 99% of children receiving palliative care have been found to die at their, or their family’s, preferred LOD (Australian Institute of Health and Welfare, 2024; Dussel et al., 2009; Lee et al., 2023; Peláez-Cantero et al., 2023). While achieving a family’s preferred LOD is not always realistic or achievable due to a variety of factors related to service availability (Dussel et al., 2009), a better understanding of the circumstances in which a family may not be able to achieve their desired LOD may help inform parental decisions and enable clinicians to set more realistic expectations for families and address the barriers to achieving their preferred location.
The first aim of this study was to establish the proportion of expected pediatric deaths that occurred at home, hospital or pediatric hospice facility, in a sample of patients/families known to two Sydney-based pediatric palliative care services. These palliative care services, servicing families across New South Wales (Australia), routinely facilitated end-of-life care arrangements at all three location types. During the full period of data collection, one pediatric hospice facility was available to families. The second aim was to identify LOD preferences expressed by families and the reasons for these preferences, giving consideration to the frequency with which documented preferences changed over the last two weeks of the patient’s life. The third aim was to assess the level of congruence between the preferred and actual LOD, and determine what factors were associated with achieving a preferred LOD. Given the potential challenges documented in the literature in achieving home deaths (Montel et al., 2009; Sagha Zadeh et al., 2018; Zelcer et al., 2010), a secondary aim of the study was to analyze factors associated with actual and preferred home deaths relative to deaths in other locations.
Methods
Study Design
This multi-centred, retrospective study utilized information from death review (Clinical Excellence Commission, n.d.) forms and electronic medical records, including both quantitative and qualitative data.
Ethics approval was granted by the Sydney Children’s Hospital Network (SCHN) Human Research Ethics Committee (2023/ETH02510).
Cohort
The cohort was drawn from pediatric patients cared for by one of the two pediatric palliative care services in the SCHN (Sydney Children’s Hospital Randwick or The Children’s Hospital at Westmead). Within the catchment areas, families had access to two tertiary pediatric hospitals, a specialized pediatric hospice facility and community teams to support home care. The inclusion criteria were: (i) patients died between January 2017 and May 2024, and (ii) died before 19 years of age. There were no exclusion criteria.
Data Extraction and Coding
Data was extracted from death review forms and electronic medical records. Death review forms are completed by a member of the palliative care team based on feedback received during a death review meeting, typically held within one month of the patient’s death, with HCPs present from the various teams involved in the care of the patient. Data from death reviews was extracted for: demographic information (e.g., primary language spoken at home, cultural background, religion/spirituality), referral information (e.g., reasons for palliative care referral, if referral was timely, diagnosis) and LOD information (all documentation regarding conversations between HCPs and family members regarding possible locations of an impending death, as well as the location of the actual death). Although all LOD conversations were coded, these are most commonly documented by palliative care teams, as part of their routine discussions and planning for end-of-life.
Once death review forms were accessed, data for each patient was also extracted from electronic medical records. Key aspects of data retrieved from the electronic medical records included demographical information, whether a community palliative care team referral was carried out, whether a PPC home visit was made, and the Index of Relative Socio-economic Disadvantage (IRSD) percentile (Australian Bureau of Statistics, 2023). The IRSD is an Australian index used to provide information about socioeconomic disadvantage relative to other residential areas based on postal code, with a lower quintile denoting greater disadvantage (Australian Bureau of Statistics, 2023). Other key information collected from the medical records included the timing and preferences for each documented LOD conversations (namely any conversation with the family about considerations or decisions regarding the location at which death may occur), as well as the congruence between preferred and actual LOD. All medical records within three months of the patient’s death were reviewed and coded by one investigator (VS).
Figure 1 shows the information retrieved from the cohort that satisfied the inclusion criteria. Information retrieved from cohort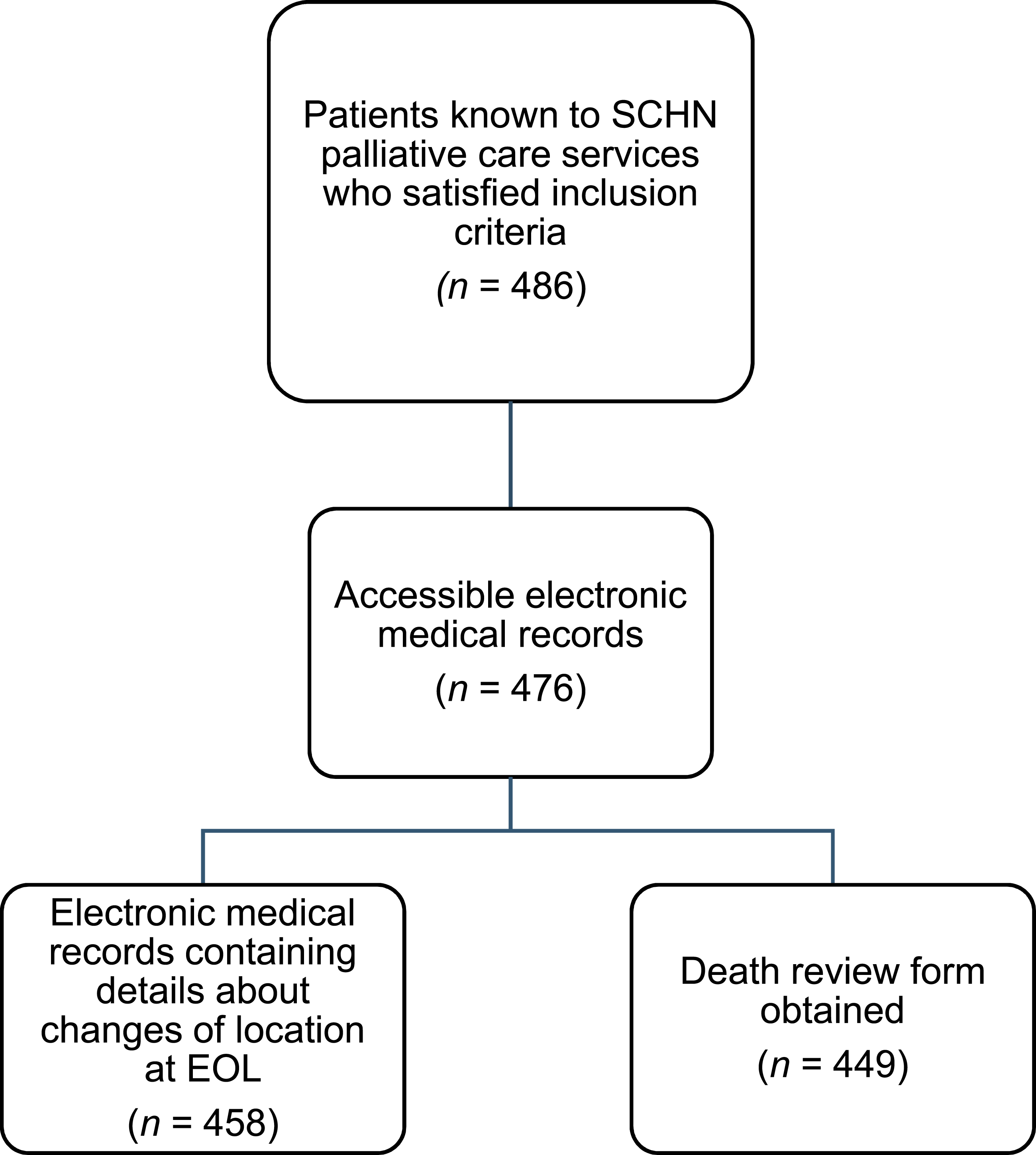
Statistical Analyses
Data elicited were primarily used to carry out descriptive analyses such as reporting the frequency of PPC patient deaths at different locations, the frequencies of different LODs preferred at different points in time, the timing of LOD discussions, and the frequency that congruence is achieved between preferred and actual LODs.
Chi-square tests were used to determine whether the actual LOD (home vs hospital or hospice) was associated with a range of categorical variables; whether the preferred LOD (home vs hospital or hospice) was associated with a range of categorical variables; and whether patients who had congruence between their preferred and actual LOD differed from those who did not, in terms of patient, family, or health service categorical factors extracted.
Continuous variables were screened for normality (skewness <1 and kurtosis <3) and if non-parametric, Mann-Whitney U tests were used to test for any significant differences between home and non-home deaths and preferences.
The total sample size (n = 486) afforded sufficient statistical power (at p < .05) to detect medium effect sizes, where they existed, when comparing home vs non-home LOD and preferences (Cohen, 1992) for patient, family and health service factors. Bonferroni corrections were applied due to the multiple tests conducted (Armstrong, 2014).
Thematic analysis was carried out for the documented reasons for a LOD preference. One researcher (VS) coded all data using codebook thematic analysis (Braun & Clarke, 2023; Roberts et al., 2019). This involved the development of initial codes based on a review of the literature and data familiarization, and editing and movement of themes/subthemes upon further reads and trial coding until agreement was reached with a second researcher (TJ) that the codebook could be assumed to represent the data.
Results
Patient and Family Demographics
Demographic Characteristics of PPC Patients Who Died Between 2017 and 2024 (n = 486) a
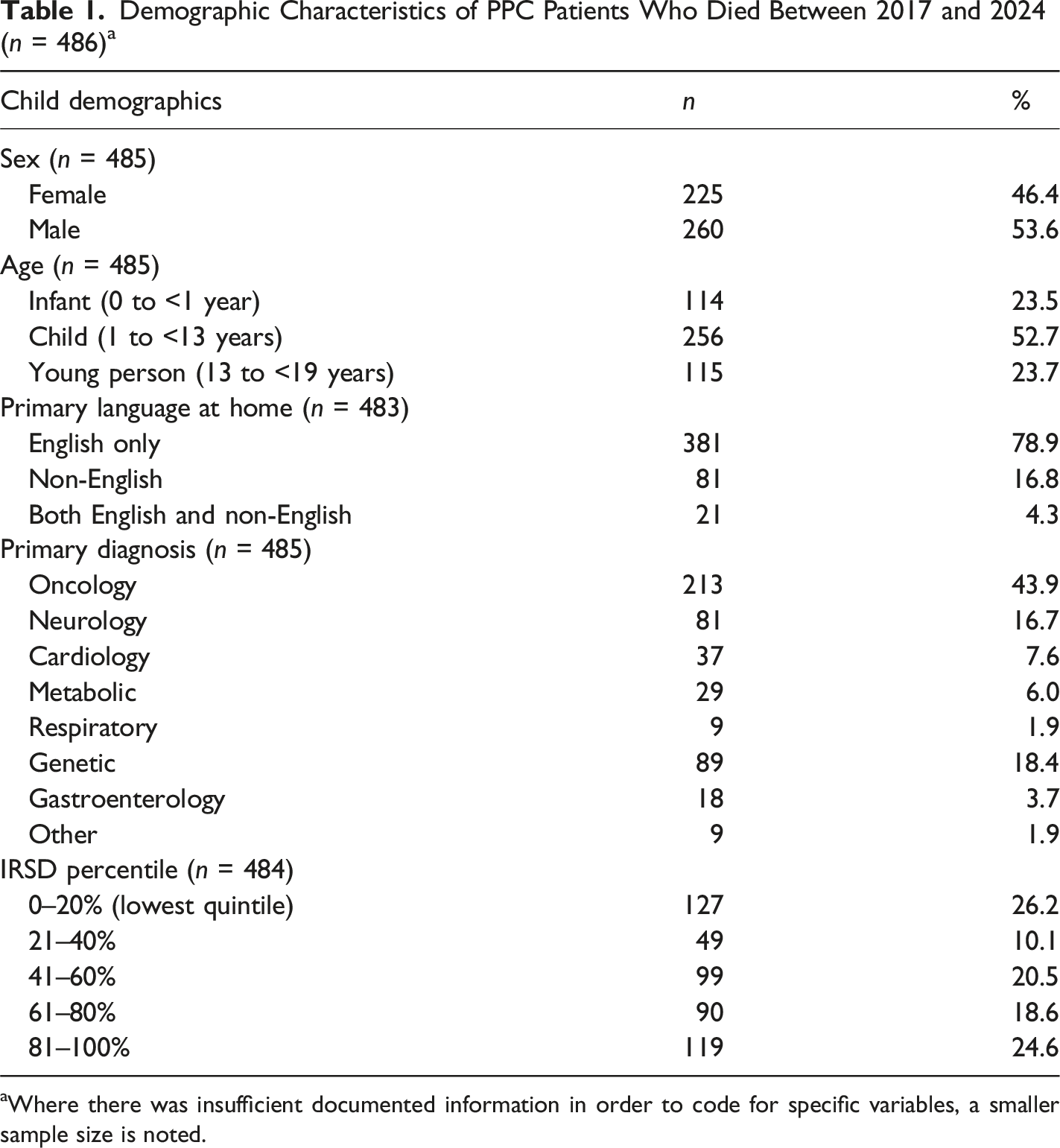
aWhere there was insufficient documented information in order to code for specific variables, a smaller sample size is noted.
Actual LOD
Frequency of Deaths at Different Locations
During the study period, 49.8% of pediatric palliative care patients (n = 242) died at hospital, 28.4% (n = 138) died at home, 21.0% at a hospice (n = 102) and 0.8% of patients (n = 4) died at another location. See Supplemental materials for information regarding temporal trends in deaths occurring at different locations between 2017 and 2024, revealing a relative spike in home deaths in 2021 and a spike in hospice deaths in 2022 (these being years in which COVID-19 had the greatest impact in New South Wales, Australia).
Factors Associated With Actual LOD
Associations (Chi-Square Tests) Between Actual LOD (Home Versus Non-Home) and Patient, Family, and Health Service Factors
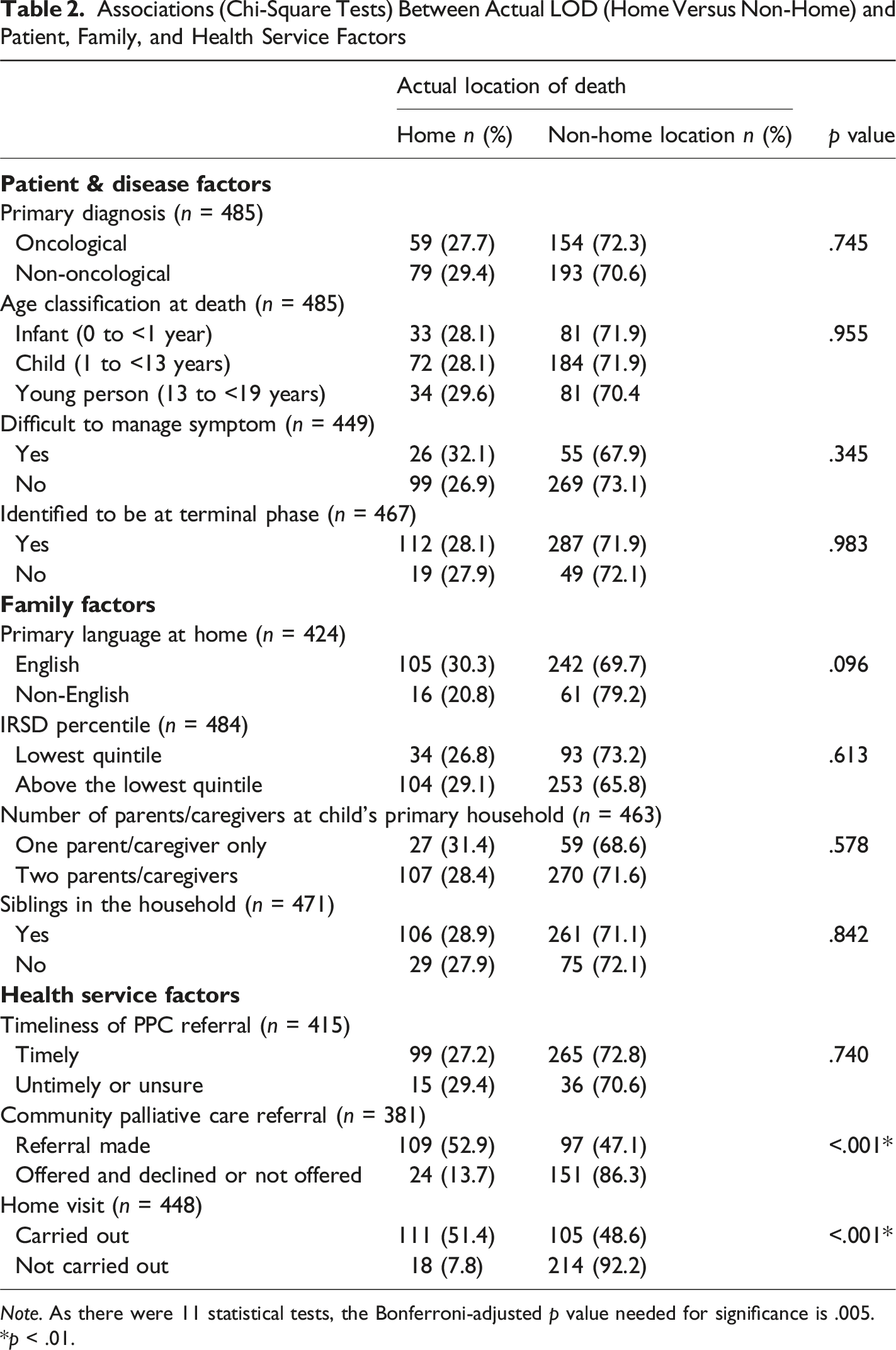
Note. As there were 11 statistical tests, the Bonferroni-adjusted p value needed for significance is .005.
*p < .01.
Post hoc analyses revealed that patients who had previously stayed at, or visited, a pediatric hospice were more likely to die at a hospice relative to at home or hospital (χ2 (3, n = 467) = 13.55, p < .001). Patients who died at a hospice did not differ from those who died at other locations in terms of existence of siblings versus no siblings (χ2 (3, n = 471) = .020, p = .888) or whether caregivers were single/separated versus a couple (χ2 (3, n = 463) = .005, p = .945).
Preferred LOD
Frequencies of Preferences and Timing of Discussions
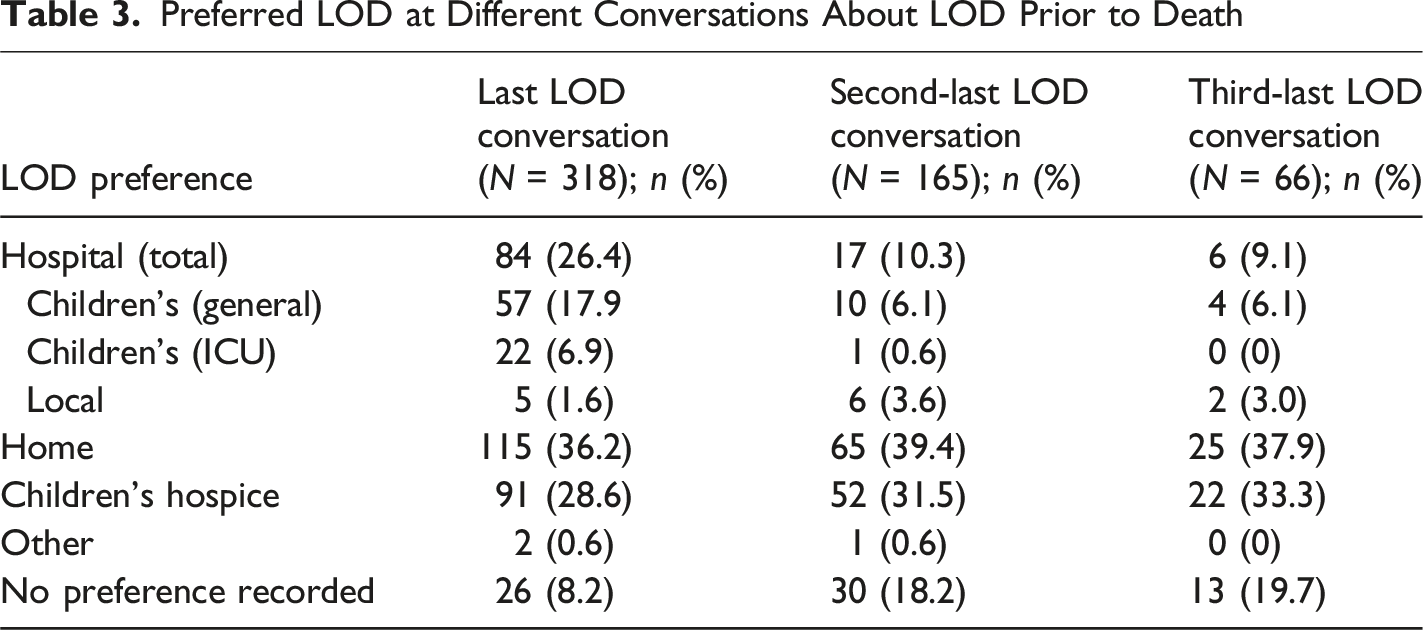
Preferred LOD at Different Conversations About LOD Prior to Death
Reasons for LOD Preferences
Primary Reasons for LOD Preferences as Documented in Medical Records
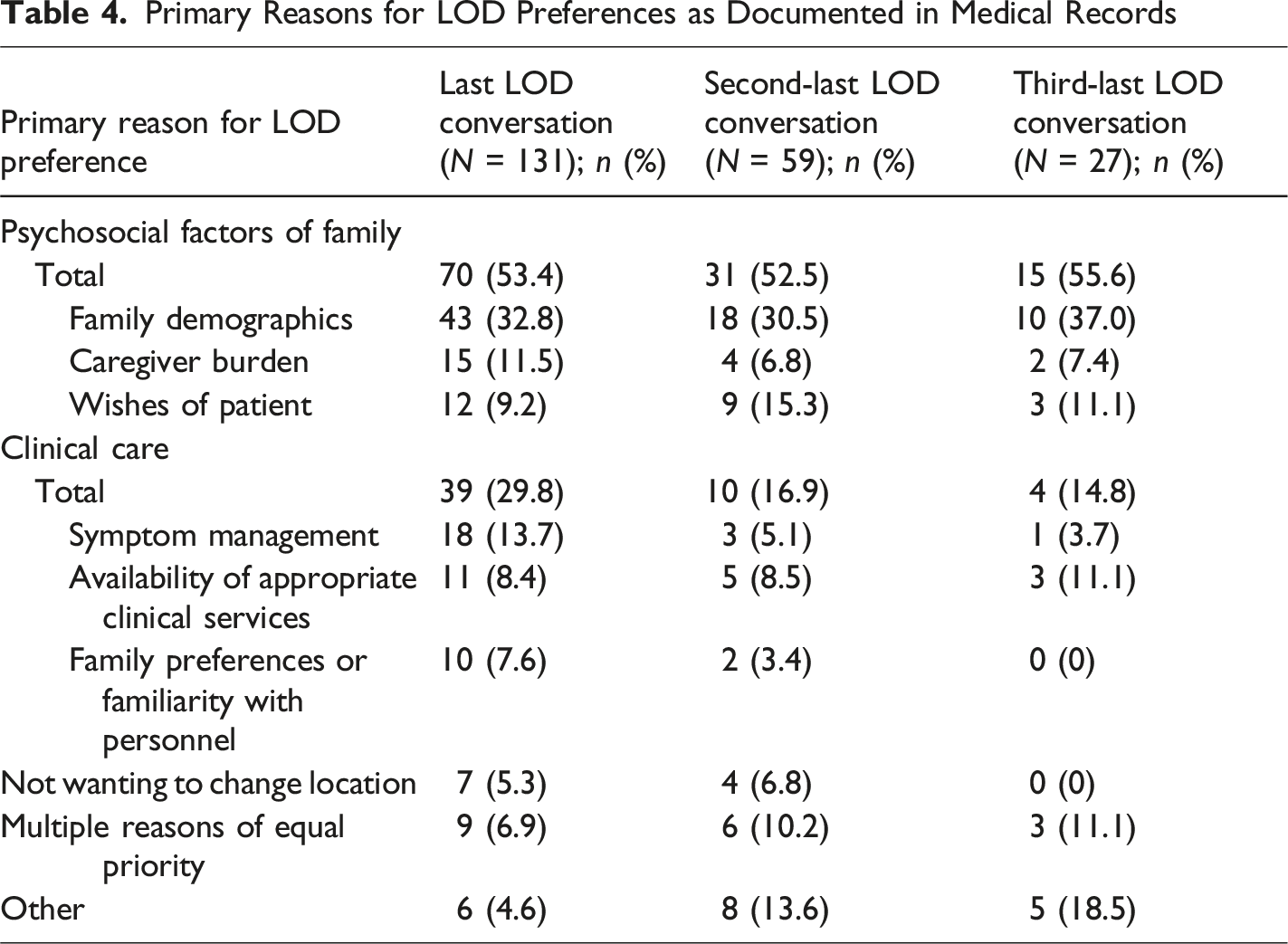
Over the last two weeks of life, 32.1% (n = 153) of families had at least one change of LOD preference (as documented in their medical records), and 3.8% had more than one change documented.
Factors Associated With Preferred LOD
Associations (Chi Square Tests) Between Last Recorded LOD Preference (Home Versus Non-Home) and Child, Family, and Health Service Factors
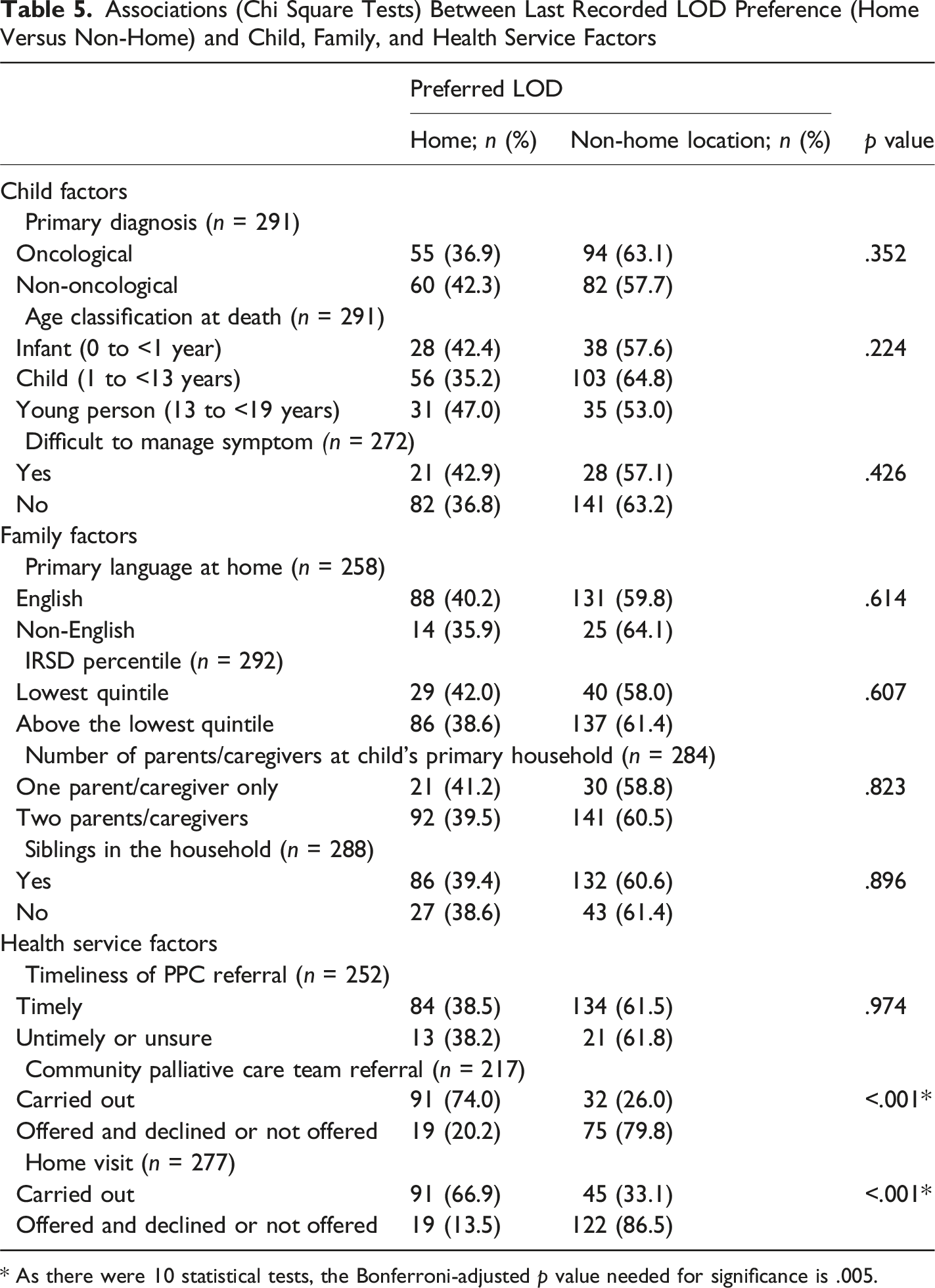
* As there were 10 statistical tests, the Bonferroni-adjusted p value needed for significance is .005.
Congruence Between Preferred and Actual LOD
Frequency of Congruence
Of the 292 cases with a documented preference regarding LOD at the last recorded discussion about LOD prior to death, 87.7% had congruence between the preferred and actual LOD. In response to the question on the death review form “was the end-of-life location goal met”, 83.5% (n = 345) of responses indicated that the location goal was met, 4.8% that the goal was not met, and 11.6% that it was unknown.
Factors Associated With Preferred and Actual LOD Congruence
Congruence Between Last Preferred LOD and Actual LOD
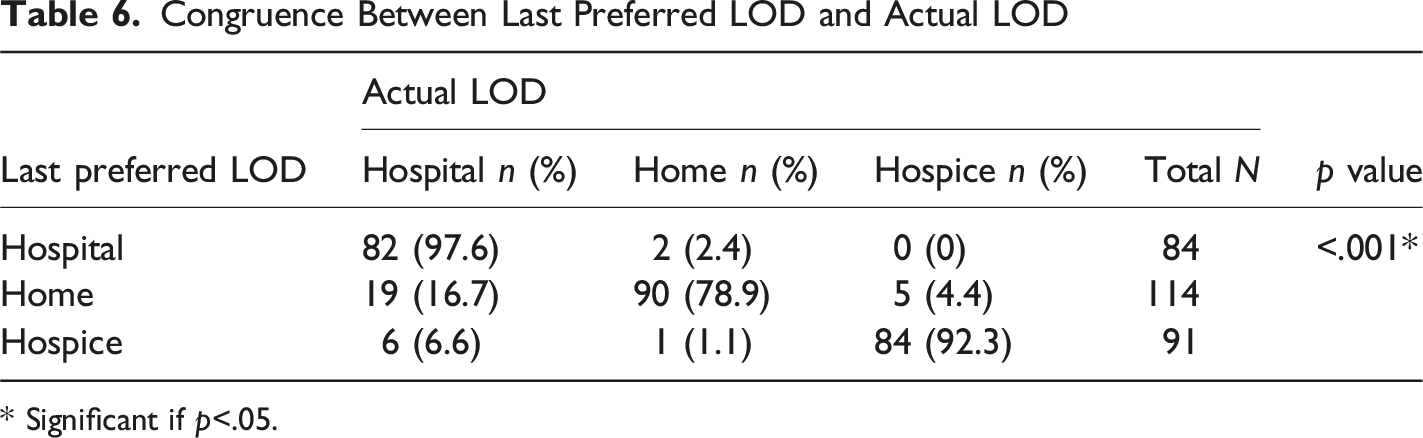
* Significant if p<.05.
Congruence Between Last Preferred LOD and Actual LOD by Patient, Family, and Health Service Factors
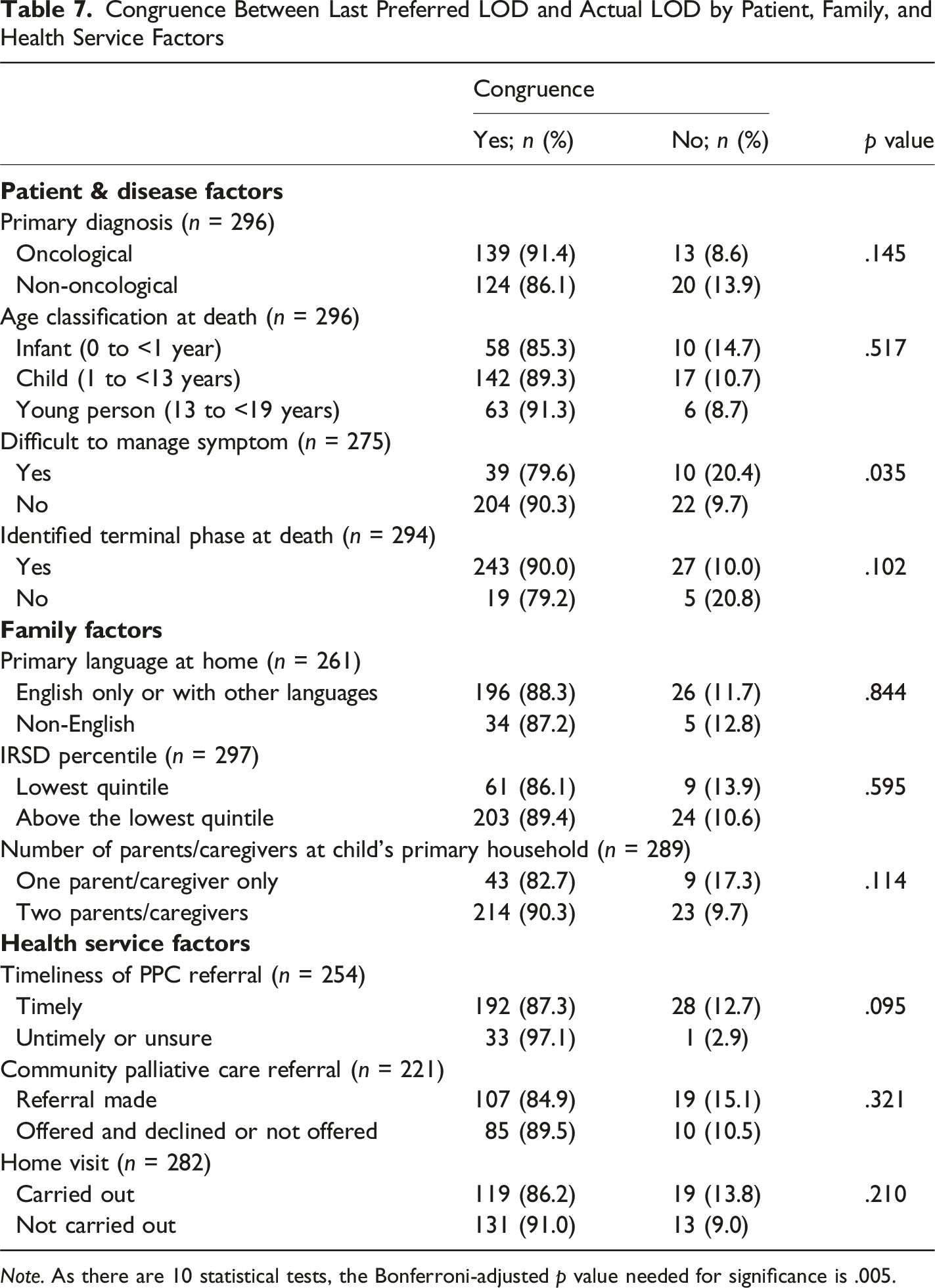
Note. As there are 10 statistical tests, the Bonferroni-adjusted p value needed for significance is .005.
Discussion
This study provided data regarding the actual and preferred LOD of children known to two tertiary pediatric palliative care services in Sydney, Australia. In line with the first aim of the study, 50% of the pediatric palliative care patients were found to die at hospital, 28% at home, and 21% at a pediatric hospice facility. The proportion of patients who died at home was lower than most figures reported across other pediatric studies and geographic contexts: England: 16% (Gibson-Smith et al., 2021), Canada/Australia/New Zealand: 35% (Siden et al., 2008), Australia: 38% (Australian Institute of Health and Welfare, 2024), Spain: 41% (Peláez-Cantero et al., 2023), India: 48% (Sneha et al., 2023), various countries: 43% (Wiener et al., 2020) to 58% (Noyes et al., 2022), Brazil 59% (Kurashima et al., 2005). The relatively low proportion of home deaths in the current study may in part be due to the relative ease of availability of a pediatric hospice facility to the current cohort.
For patients in the current dataset who died at home, referral to PPC generally occurred earlier than for those who died in non-home locations. Earlier PPC referrals likely allow for more opportunity for the necessary preparations for a home death to occur: a referral to the community-based palliative care team (Malcolm et al., 2020), the set-up of specialized equipment in a suitable home space (Sagha Zadeh et al., 2018), and parental education (Winger et al., 2020). Not surprisingly patients who received a referral to a community palliative care team or had any PPC home visit, were more likely to die at home as opposed to hospital or hospice, as community teams can provide the symptom-management and support that families need in order to feel comfortable at home (Hannan & Gibson, 2005; Noyes et al., 2022; Papadatou et al., 2021). Patients who died at home versus out-of-home were not found to differ on a range of patient, family or sociodemographic variables tested. This finding may suggest that equitable access of end-of-life options were available to families. For example, families who were non-English speaking or with greatest socioeconomic disadvantage did not differ in terms of their child’s actual LOD (home versus non-home location). However, caution should be exercised in drawing conclusions from null results (Harms & Lakens, 2018).
Patients who had previously visited or stayed at the hospice were significantly more likely to die at that facility, perhaps due to familiarity and previous positive experiences of receiving respite care at the facility (Dunbar et al., 2020). Encouraging families to visit a pediatric hospice before the end-of-life may help them realize the unique benefits (Gola et al., 2016; Hain, 2019) of the location, and to consider hospice as a potential LOD.
When addressing the second aim of the study, data was collected regarding family preferences for the location of an expected child death, and how these preferences changed over time. The percentage of families who preferred a hospital LOD more than doubled from the second-last (10.3%) to last (26.4%) documented LOD conversation. In contrast, the percentage of families that preferred a home LOD decreased across the second last (39.4%) to last (36.2%) documented conversation. These results highlight how LOD preferences may change over the illness trajectory, as families prioritize differently a range of psychosocial factors and clinical care. As the patient is nearing death, concerns about managing clinical symptoms, family psychosocial dynamics, or perceived limitations in support for a home death can lead families to feel less confident in their ability to successfully manage a home death (Hannan & Gibson, 2005; Noyes et al., 2022; Papadatou et al., 2021; Sneha et al., 2023).
It should be noted that less than two-thirds of pediatric palliative care patients had any medical record documentation regarding the family’s preferences regarding LOD. This implies that for one-third of pediatric palliative care patients, conversations regarding LOD preferences either did not occur with the family prior to the patient’s death, or that these conversations were not appropriately documented. There are several reasons why LOD conversations do not occur in a timely way. Some families are reluctant to engage in difficult discussions about their child’s impending death (Ulrich et al., 2018). Healthcare professionals may hold off on engaging in such discussions until they feel there is a more appropriate time to have this discussion, or until they have developed more rapport with the patient (Cox et al., 2011). Families and healthcare professionals may not recognize that death is imminent (Chu et al., 2019), with prognostication often difficult in the context of early phase clinical trials and medical interventions (Kennedy et al., 2021). Consequently, conversations about end-of-life planning and death may be postponed too long.
Regarding the third aim of the study, it was found that about 89% of patients died at the preferred LOD. This figure is consistent with findings from other studies, across a range of locations, with congruence figures ranging between 70% and 99% (Dussel et al., 2009; Kassam et al., 2014; Lee et al., 2023; Peláez-Cantero et al., 2023; Stilwell et al., 2022). While nearly all families in the current study preferring a hospital or hospice death achieved their desired outcome (98% and 92% respectively), only about 79% of families who preferred a home death achieved this location, with 17% of these patients dying at hospital. Other research has similarly reported that a significant proportion of families desiring a home death for their child, may not achieve their goals (Kassam et al., 2014; Stilwell et al., 2022). Families who prefer a home death may have their child die at hospital if the child rapidly deteriorates at hospital and is not stable enough to be transported (Stilwell et al., 2022) or if their medical needs cannot be adequately managed at home (Zelcer et al., 2010). Congruence between preferred and actual LOD was more likely for patients whose medical records documented that they were at the terminal stage, as this recognition may have provided time for transport to their preferred LOD.
Limitations
It is likely that not all conversations regarding LOD were documented in the patient’s medical records. Staff may have been more likely to record a preference for dying at home or in a hospice, as these require more preparation and coordination than a hospital death. This is consistent with the finding in the current study that patients without a recorded preference for LOD were most likely to die in hospital.
Although the current study assessed congruence between preferred and actual LOD, it was not possible to determine from the available documentation whether families were satisfied with the actual LOD. Moreover, some documented LOD preferences may have been a compromise, given the lack of feasibility of other options. Consequently, the level of congruence between preferred and actual LODs may be somewhat inflated.
When examining the frequencies of actual and preferred LOD death in the period 2017 to 2024, the impact of COVID-19 on this data is uncertain. During the period when the NSW health sector was most impacted by COVID-19 (2020 to 2022) (Australian Bureau of Health Information, 2023), strict restrictions were placed on the number of visitors allowed in hospitals, and to a lesser extent in hospices. There were also restrictions on the access of community palliative care teams as well as informal supports for patients and families in the home environment (Rattner, 2021), with greater reliance on telehealth (Weaver et al., 2021).
A strength of this study was its inclusion of children with a wide range of diagnoses requiring palliative care, given that previous studies examining LOD have drawn more extensively on pediatric oncological cohorts (Dussel et al., 2009; Kassam et al., 2014; Stilwell et al., 2022; Vickers et al., 2007).
Clinical and Research Directions
Given that only 62% of families known to pediatric palliative care teams had a documented LOD preference (at the time of the last LOD recorded discussion prior to death), there is a need to ensure that all families discuss and plan for the LOD, and that preferences are appropriately documented. Previous studies have shown that healthcare workers may experience difficulties discussing, recording and tracking goals of care (Cox et al., 2011); therefore more work is required to establish how this information may be more routinely recorded and communicated between health services. As LOD preferences are influenced by changing clinical, psychosocial and logistical factors, there is value in having LOD conversations with the family at multiple time points. Earlier PPC referral may provide more opportunities for these discussions, and if the preference is for a home death, more time for home supports to be instated and for adequate parental education (Malcolm et al., 2020; Sagha Zadeh et al., 2018).
As 21% of families were unable to achieve their preference for a home death, clinicians should consider if those preferring a home death have adequate supports in place. If such supports cannot be instated, it may be necessary to support families in identifying and achieving a more realistic LOD goal. Parents and caregivers who aim for a home death, benefit from clear guidance in how they can respond to clinical situations which may arise. Community palliative care team involvement is key in managing challenges to a home death, such as difficult to manage symptoms and rapid deterioration (Montel et al., 2009; Odejide et al., 2022; Stilwell et al., 2022). As these teams often primarily service adult palliative care patients (Contro et al., 2002), they may benefit from specialist pediatric outreach services (Mherekumombe, 2018; Mherekumombe et al., 2016).
Prospective, longitudinal studies are needed to more accurately identify changes in the LOD preferences of families. Furthermore, it would be valuable to assess familial satisfaction with actual LOD, irrespective of whether it was their preferred location. Parental satisfaction with actual LOD is likely to have a lasting impact, with less decisional regret about the LOD (Dussel et al., 2009) and better bereavement outcomes (Jaaniste et al., 2017).
In light of the significant proportion of families unable to achieve their preference for a home death, there is a need to examine local barriers further. Such barriers may include a desire for more healthcare support in the home (Barlund et al., 2021; Wahid et al., 2018), level of trust in community healthcare providers (Brouwer et al., 2020), and access to medical supports at home to decrease the need to travel for inpatient treatment (Barlund et al., 2021). Strategies used to overcome these barriers, such as better healthcare service coordination or upskilling staff (Wahid et al., 2018), may be evaluated by comparing future preferred and actual LOD congruence figures with the benchmark figures reported in the current study.
Further research into how families prefer to have difficult discussions, such as those around LOD, could inform the creation of educational or clinical tools to help healthcare workers engage in sensitive and timely conversations about end-of-life and LOD planning.
Conclusion
This study found that the most common LOD for expected pediatric deaths was hospital, followed by home and then hospice. As end-of-life approached, the documented preference for death at home decreased, while the preference for a hospital death increased. Families who chose hospital as the desired place of death were more likely to achieve congruence between their preferred and actual location of death. However, nearly one-fifth of families who preferred a home death did not achieve that preferred location. The current study underscores the need to improve how LOD preferences are recorded and to explore and address local barriers that prevent achieving a preferred home death.
Supplemental Material
Supplemental Material - Actual and Preferred Location of Death for Children Known to a Palliative Care Service
Supplemental Actual and Preferred Location of Death for Children Known to a Palliative Care Service by Victoria Sun, Sandra Coombs, Nicole Armitage, Meaghan Dowling, and Tiina Jaaniste in OMEGA - Journal of Death and Dying
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.