
Abstract
Advance care planning (ACP) completion rates remain modest in the United States despite the benefits of ACP to patients’ quality of end of life. This mixed methods study explores adults’ (N = 203) perspectives on ACP and the potential use of artificial intelligence chatbots to facilitate this process. Participants identified as either living with life-limiting illnesses (N = 75) or as healthy (N = 128), and were mean age 64.02 (SD = 11.09); 48.8% men, 48.3% women; 55.7% disabled; and racially, socioeconomically, and religiously diverse. Participants were open to engaging with chatbots for logistical and informational ACP tasks but strongly preferred human communication for more personal or emotional conversations. Comfort with chatbot-facilitated ACP increased when chatbots were transparent, text-based, and used in conjunction with healthcare providers. Findings underscore the continued primacy of human connection in ACP and highlight design considerations—including transparency and human integration—under which chatbots may responsibly supplement this process and gain public acceptance.
Keywords
The question of how individuals wish to be cared for at the end of life (EOL) is fundamentally one of dignity, autonomy, and respect for personal values. Despite broad consensus on the ethical imperative to honor individuals’ preferences (Akdeniz et al., 2021), these preferences are not always honored, compromising the quality of care and the overall patient and family experience during the final stages of life. Approximately 13–21% of patients in the United States receive EOL care that is inconsistent with their expressed values, for example, with respect to treatment (e.g., life extension versus comfort care) and preferred place of death (Khandelwal et al., 2017; Modes et al., 2020).
Advance care planning (ACP) practices are intended to prevent such harms. ACP refers to practices and processes related to clarifying and communicating decisions about the care an individual prefers to receive at EOL, particularly in the event they become incapacitated. ACP includes formal and informal conversations as well as medical and legal documentation. A patient’s documentation of their values and treatment goals through an advance directive, for example, increases the likelihood that the patient will receive the care they desire at EOL (Sudore & Fried, 2010). Unfortunately, fewer than one in three adults in the United States has completed an advance directive (Yadav et al., 2017).
At its best, the goal of ACP is to ensure that the medical, spiritual, and psychological care a person receives throughout the duration of an illness or at EOL aligns with their personal values, goals, and preferences. Both the process of engaging in ACP and the tangible outcomes of ACP reduce stress and decisional burden on family and loved ones (Yeun, 2021) and improve satisfaction with care and bereavement outcomes (Scherer & Holley, 2015). ACP is associated with reducing unnecessary hospitalizations and aggressive treatments, increasing use of palliative and hospice services, and lowering healthcare costs (Molloy et al., 2000; Teno et al., 2007; Wright, 2008). For example, Brown et al. (2025) analyzed data from nearly five million patients with chronic neurodegenerative diseases and congestive heart failure. They found that patients who had documented ACP discussions had 20–30% fewer emergency department visits than those without documented discussions. In addition, patients who had previously shown increasing rates of emergency department visits and hospitalizations showed declining rates after ACP. Study authors indicated that their findings may be explained by prior research suggesting that ACP may reduce healthcare utilization by improving patients’ understanding of their illness, prognosis, and personal care preferences. When documented through ACP, patient clarity is often associated with preferences for less aggressive treatment at EOL and with better alignment of provider care with patients’ goals. Yet despite these demonstrated benefits, rates of engagement in ACP conversations in the United States remain low (Malani et al., 2021), and there is room for ACP to be made more effective.
Low ACP Rates and Areas for ACP Improvement
People report avoiding ACP discussions for many reasons, including fear of EOL and emotional discomfort with EOL topics, a lack of knowledge about ACP, mistrust of the healthcare system, and concerns about harming the provider-patient relationship (Bernard et al., 2020; Schrader et al., 2010; West & Hollis, 2012). Physicians also sometimes hesitate to initiate ACP conversations out of concern that such discussions could cause emotional distress, diminish a patient’s sense of hope, or feel inappropriate in certain clinical contexts (Curtis, 2000; Morrison et al., 1994). Both patients and providers approach conversations related to EOL with verbal and non-verbal cues indicating the topic is extremely sensitive, and tend to use language replete with ambiguity (Parry, 2024). In addition, ACP does not always result in tangible products, such as advance directives and the assignment of healthcare proxies, that provide evidence of what treatments a patient would prefer when they are no longer able to communicate for themselves (Beck et al., 2002; Hooper et al., 2020).
Current ACP processes and tools tend to be simplistic, emphasizing a binary view of legal document completion versus non-completion—rather than regular revisiting of one’s goals and preferences—and a narrow set of decisions related to opting in or out of life-extending treatments. Therefore, ACP documents may be outdated (Forrow, 1994), ambiguous or lacking in practical details (Lynn, 1991), or unintentionally restrict surrogates’ flexibility in responding to unforeseen circumstances (Hawkins et al., 2005). Further, the wording of advance directive templates may influence individuals’ decision-making about EOL care preferences, raising concerns about the reliability of completed forms (Park et al., 2020). Finally, completed advance directives may simply fail to reflect a person’s true values, goals, and healthcare preferences because they prioritize specific treatment decisions over broader conversations about values and decision-making processes. These varied problems highlight the need to find new avenues to facilitate effective, dynamic ACP conversations and to produce personalized documentation to improve EOL outcomes.
Can ACP Be Improved With the Help of AI Chatbots?
There have been calls to use different forms of media to improve ACP conversations (Tenzek et al., 2025). In response, researchers and healthcare professionals have developed self-guided ACP aids in easy-to-follow formats such as conversation booklets, video tutorials, and even card games, in order to reduce emotional discomfort, simplify complex topics, and encourage meaningful dialogue about EOL preferences (Phenwan et al., 2023; Sedini et al., 2022). Such tools have demonstrated effectiveness in motivating individuals to move beyond intention and take real action—for example, after engaging with an ACP card game, up to 75% of participants took concrete ACP-related actions such as discussing their wishes with family or appointing a healthcare proxy (Van Scoy et al., 2017). However, one of the key limitations of these ACP aids is their static nature: they offer broad, predetermined scripts and cannot adapt in real time to the user’s emotions, preferences, or readiness to engage.
In contrast, artificial intelligence (AI) chatbots can produce fluid, responsive conversation and adjust tone, pacing, and content based on user input (Jiang et al., 2023), allowing for a more personalized and supportive experience. Chatbots are computer-based systems designed to replicate human dialogue through text, voice, or multimedia interactions. With recent advancements in AI and digital technologies, their capabilities have significantly expanded and are now widely applied across diverse healthcare settings (Al-Amin et al., 2024; Laymouna et al., 2024). Related research in the realm of ACP is rapidly evolving, but some studies suggest patients may be especially willing to engage with chatbots on sensitive topics (Miles et al., 2021), such as EOL care. In addition, chatbots have the potential to address existing barriers to ACP: little time in healthcare appointments, limited access to providers, and a lack of EOL and ACP knowledge. New AI chatbot ACP tools would presumably be accessible to patients at any time and on any day, be free or low-cost for patients, and be equipped to provide basic and advanced information on EOL care and ACP according to patients’ needs.
Early research on AI chatbots in the context of palliative care demonstrates that such tools can be effective in dispelling misconceptions, improving patient awareness and education, and producing human-like conversations that resemble meaningful dialogue (Gondode et al., 2024; Srivastava & Srivastava, 2023). This research has also revealed certain limitations, such as chatbots’ excessive repetition of phrases and expressions of strong, potentially inappropriate opinions on sensitive topics like religion, death, and the afterlife. Palliative care experts have also raised concerns about AI chatbots being positioned as replacements for human interaction (García Abejas et al., 2025), which could progressively weaken and ultimately diminish the patient-provider relationships that are fundamental to effective medical practice (Akingbola et al., 2024). Laypeople are concerned about privacy and security in AI chatbot conversations (Li, 2023). Finally, there are concerns about the potential for biased chatbots, which could lead to harm to marginalized groups (Alowais et al., 2023). Though the use of AI chatbots in this sensitive context presents challenges, given that decades of research seeking to improve ACP have made only marginal gains (Curtis et al., 2022; Morrison, 2020; Szmuilowicz et al., 2023), innovative approaches are needed. Seeking input from potential users is an important first step.
Purpose of the Present Study
The present study contributes to the existing literature on ACP communication by examining U.S.–dwelling adults’ openness to integrating AI chatbots into ACP conversations. Chatbots are already being implemented as communication aides in other healthcare settings (Al-Amin et al., 2024; Laymouna et al., 2024), and are currently being assessed for implementation in the ACP communication process (Gondode et al., 2024; Srivastava & Srivastava, 2023). However, there is no present literature on patients’ perspectives on communicating with AI chatbots in the emotionally sensitive context of EOL care, nor on their imagined preferences for such communication.
In response to this literature gap, we surveyed two demographic groups we believed would have considered EOL care preferences and ACP. The first group was comprised of adults over the age of 18 who self-identified as having a life-limiting illness (LLI), or a medical condition that is expected to significantly shorten lifespan and/or reduce quality of life, as such individuals may be more likely to have considered care preferences and mortality. We also surveyed adults over the age of 50 who may not identify as having a LLI, as age is associated with increased awareness of mortality (Charles & Carstensen, 2010). Our primary objective was to assess participants’ general perceptions and attitudes toward the integration of AI chatbots into ACP, with the aim of identifying barriers and opportunities for this application. Our secondary objective was to gather participant input to inform the future development of ACP AI chatbot technology designed to support individuals in identifying and communicating their care preferences.
Materials and Methods
Ethics
This study was deemed Exempt by the University at Buffalo Institutional Review Board (STUDY00008612). Detailed informed consent information was provided as page one of the online survey. Participants who indicated their consent were advanced to the study survey.
Recruitment and Participation
Participant Recruitment
Data was collected from February through June of 2025. Participants were recruited via an email campaign to leaders of 87 local organizations serving diverse constituencies, posting flyers in local community spaces and businesses serving minoritized and older populations, and through research registries. Research registries were the Buffalo Research Registry, a volunteer database managed by the University at Buffalo Clinical and Translational Science Institute, and ResearchMatch, a national volunteer registry established by numerous academic institutions and supported by the U.S. National Institutes of Health as part of the Clinical Translational Science Award program. We attempted to oversample for adults with LLI, as this population is difficult to reach for research recruitment (Brickey et al., 2022; O’Mara et al., 2009).
Inclusion and Exclusion Criteria
To be eligible, individuals had to be able to read and respond to the survey in English and to currently reside in the United States for at least one year. Adults who identified as living with a life-limiting illness (“LLI”)—living with a serious, terminal, or progressive condition such as cancer, organ failure, chronic obstructive pulmonary disease, or neurological disorders—had to be at least 18 years old. Adults who identified as not living with an LLI (“healthy”) had to be at least 50 years old. Individuals were included in the present sample if they had progressed through at least 95% of the survey, as our primary questions of interest were located at the end of the survey.
Sample
Participant Demographics
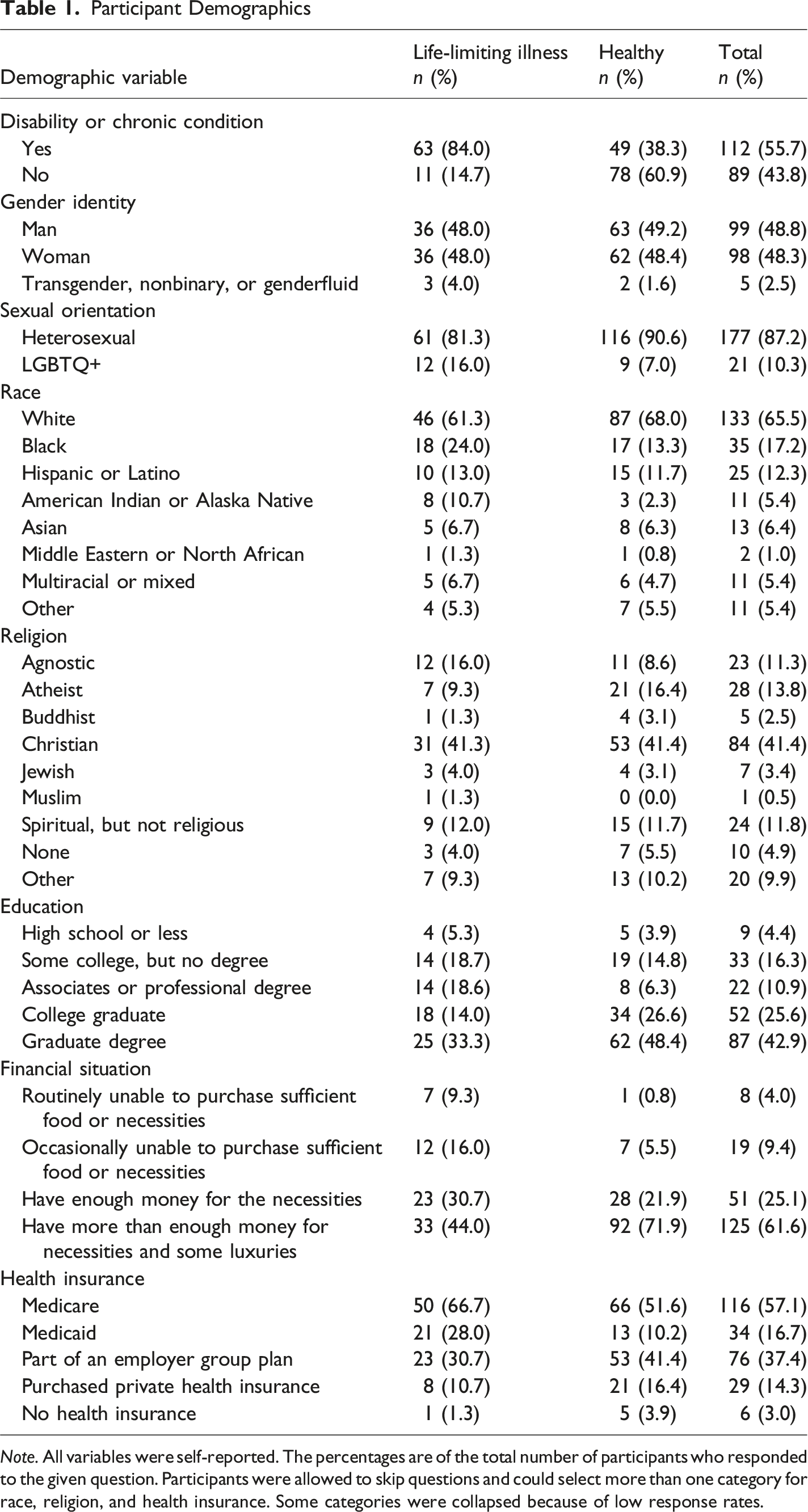
Note. All variables were self-reported. The percentages are of the total number of participants who responded to the given question. Participants were allowed to skip questions and could select more than one category for race, religion, and health insurance. Some categories were collapsed because of low response rates.
Survey Measure
The questions analyzed in the present study were collected as part of a larger survey examining preferences, concerns, desires, expectations, and beliefs related to EOL care, ACP communication and documentation, and AI chatbots. Each section included multiple-choice and open-ended questions, prompting both quantitative and qualitative responses.
Procedure
Eligible participants were directed to a consent form and survey hosted on the University at Buffalo Qualtrics secure platform. The full survey was estimated to take approximately 20–30 minutes to complete. Participants had the option to skip questions and, in some cases, choose multiple responses. Participants were given the option to enter a drawing for one of 10 $25 digital rewards at survey close.
Analyses
The study employed an exploratory design involving a self-administered online survey; we did not make hypotheses. Descriptive statistics were used to summarize participant responses. When appropriate, group comparisons between healthy adults and adults with LLI were conducted using t-tests and chi-square tests. Of note, group differences are noted in Results only when statistically significant. All quantitative analyses were performed in R (R Core Team, 2023). Qualitative thematic analysis was conducted on open-ended survey responses to identify patterns, themes, and key insights (Braun & Clarke, 2006). Themes were generated through multiple rounds of coding to ensure reliability and validity in interpretation.
Results
Descriptive Statistics
As shown in Table 1, the sample was evenly distributed between men and women. Most participants identified as White and as heterosexual. The sample was religiously diverse, with Christianity reported most often. The sample was more educated than the general U.S. population (U.S. Census Bureau, 2025), with nearly half holding a graduate degree. The healthy group was significantly older (M = 65.42, SD = 8.50) than the LLI group (M = 61.60, SD = 13.70), t(107.95) = 2.18, p = .031, d = 0.36 and fewer healthy participants identified as having a disability or chronic condition, χ2(1, N = 203) = 39.20, p < .001, Cramer’s V = 0.44. In addition, financial situation differed significantly by group, χ2(2, N = 203) = 20.37, p < .001, Cramer’s V = 0.32; participants with LLI more often reported financial difficulties, whereas healthy participants more often reported having more than enough money for necessities and luxuries. Finally, healthy participants were more likely to have completed college or graduate degrees than participants with LLI, χ2(2, N = 203) = 9.51, p = .009, Cramer’s V = 0.22.
EOL Care Consideration
A substantial portion of participants indicated they had given their future EOL care at least some thought, with 85.5% selecting either somewhat or quite a bit of thought. A chi-square test of independence revealed a significant association between group and the extent to which participants had thought about their EOL care, χ2(2, N = 203) = 6.33, p = .042, Cramer’s V = 0.18. Participants in the LLI group were more likely to report having thought about it quite a bit (41.3%) compared with the healthy group (33.6%) and were less likely to report having thought about EOL care not at all (6.7%) compared to the healthy group (19.5%).
Perspectives on AI Integration into Healthcare and ACP
Slightly more than half of the sample (58.9%) had previously interacted with a chatbot. Participants were prompted to provide yes/no ratings of 11 categories of health-related support in response to the question, “In what healthcare contexts do you think a chatbot could provide accurate information?” As illustrated in Figure 1, AI chatbots were perceived as potentially accurate for tasks such as helping users to find treatment locations or prepare questions for medical appointments. However, when it came to more complex tasks such as diagnosing conditions based on symptoms and providing emotional support, chatbots were viewed as less accurate, for example endorsing “Providing me with comfort and emotional support” significantly less frequently than would be expected if all options were equally likely to be chosen, χ2(1, N = 836) = 36.91, p < .001, Cramer’s V = 0.21. The only significant difference between LLI and healthy groups was for the item “Helping me find the right specialist,” χ2(1, N = 203) = 4.26, p = .039, Cramer’s V = .15, such that LLI participants were more likely than healthy participants to trust a chatbot with this task. Healthcare contexts for which patients perceived artificial intelligence chatbots to provide accurate information. Healthy = participants without life-limiting illness; LLI = participants with life-limiting illness.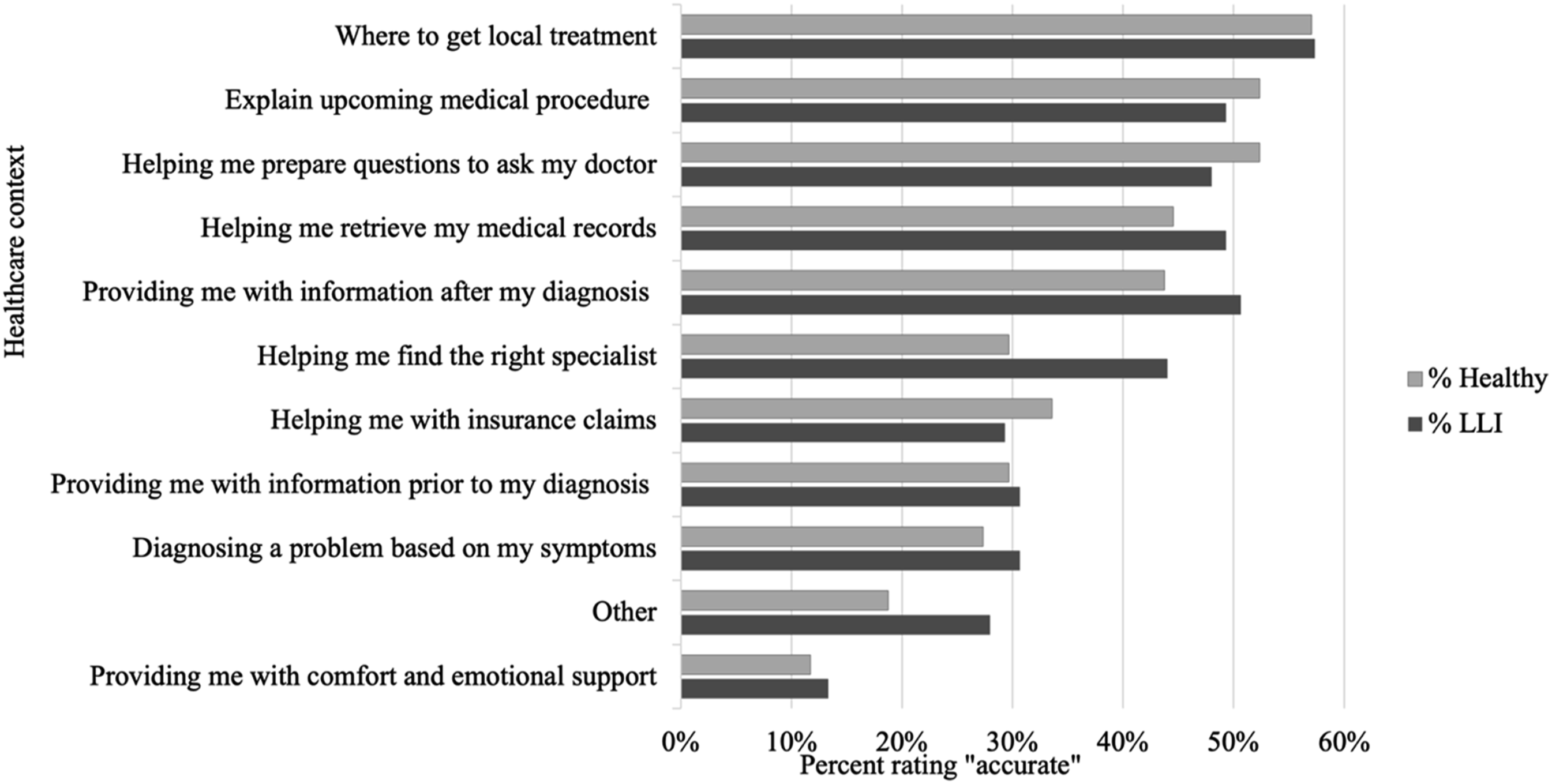
Figure 1 Bar graph displaying the percentage of participants endorsing artificial intelligence chatbots as potentially accurate in each of 11 healthcare contexts. Healthy participants are represented by light gray bars, and participants with life-limiting illnesses by dark gray bars.
Openness to the Use of AI Chatbots in ACP
Themes From Participant Reflections on Artificial Intelligence Integration in Advance Care Planning and End-of-Life Discussions
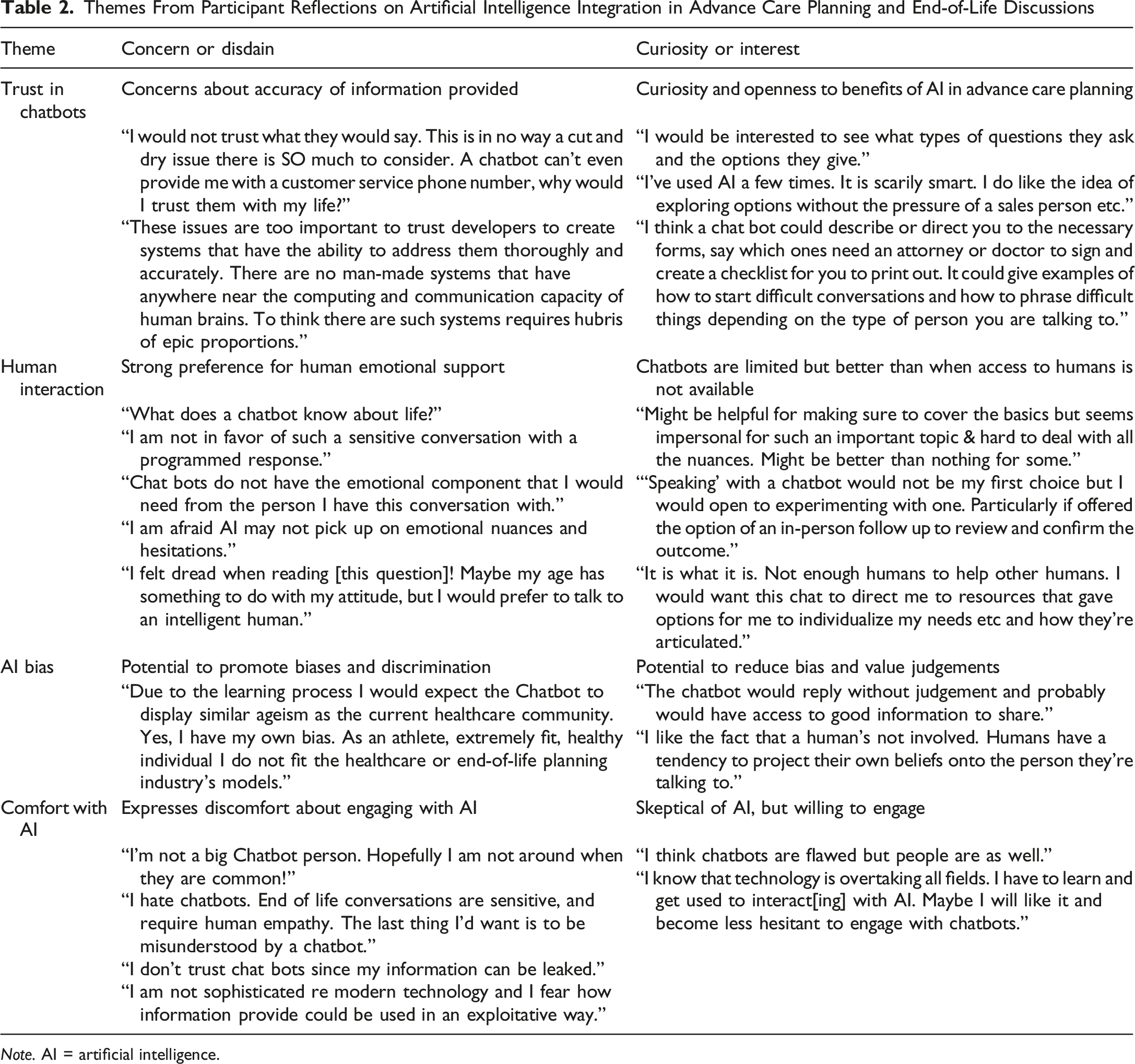
Note. AI = artificial intelligence.
Overall, participants expressed curiosity about chatbot conversations as well as concerns regarding patient privacy and chatbot bias. Participants often expressed that they believed chatbots were severely limited in their ability to provide emotional support. However, even those participants who preferred human interaction tended to acknowledge that chatbots could bridge gaps in access when human support is unavailable or ineffective.
Participants were also asked whether they would prefer to have ACP conversations virtually with a chatbot or in person with a medical professional. The majority preferred a medical professional (73.9%). Only 7.4% preferred a chatbot; 23.6% selected I’m not sure or have no preference. Participants were also prompted to explain their reasoning behind their choice. In their open-ended explanations, participants who selected medical professionals emphasized the importance of expertise and believed professionals were better equipped to handle emotionally challenging ACP conversations. As one participant explained: Advance care planning is a sensitive topic and should include the care of a human being who can hold space for the depth of emotions and complexity of humanity in the conversation. An unfeeling robot cannot provide the psychological, mental, or emotional touch necessary for these types of conversations.
A few participants described having a trusting and valued relationship with their healthcare provider: “I…have a very caring and compassionate [primary care provider] that I believe would give me true and accurate information, especially since he has been my physician for over 10 years.” In one notable case, a participant clarified that while they preferred to converse with a medical professional, this choice was likely unrealistic due to concerns about the fragility of the healthcare system: [A medical professional] would be ideal. There just isn't time though. I have Medicaid. It's not a doctor’s fault they don't have time for lots of extras. Not in the [United States]. I'm just grateful to have care. I'm scared with current politics I'll lose this care that I have.
Some participants who selected not sure described the complexity contained within the choice, for example, pointing to a desire for the conversation partner—whether a medical professional or a chatbot—to “understand what is involved with your particular medical condition because generic, one size fits all answers would be frustrating…It could be awkward or uncomfortable discussing such things in person, especially with a professional who doesn’t really know you.” Some said that their choice depended on the situation: “I think the choice would have to do with the urgency of need to have the discussion and the type of info needed to pass between me and the provider.” Others were “open to discuss[ing] advance care with anyone, even [a] chatbot.”
A small proportion of participants preferred a chatbot. These participants believed that a chatbot would provide a private and non-judgmental environment (“No judgement by bot on silly questions or repeat questions. The bot does not act like [it’s too] busy or [you’re] bothering [them]”) or be more accessible and available than providers (“I don’t think medical professionals have time for things like [ACP conversations]”). Overall, a portion of the respondents who selected no preference or a chatbot preference believed that chatbots could potentially fulfill psychosocial and practical needs they perceived as unlikely to be met through interactions with medical providers.
Preferred Characteristics of an ACP AI Chatbot
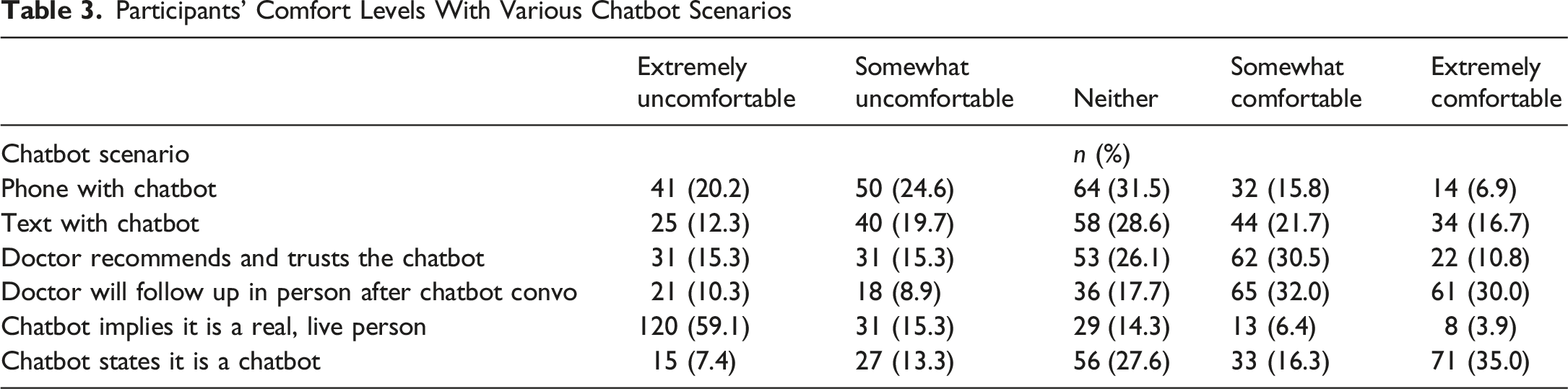
Participants were asked to rate their comfort with a potential chatbot interaction based on six key scenarios: (a) “I can have a phone conversation with the chatbot”; (b) “I can have a text conversation with the chatbot (typing on a cell phone or computer)”; (c) “If my doctor told me they trust and recommend the chatbot”; (d) “If my doctor told me we would have a follow-up face-to-face conversation based on my chatbot conversation”; (e) “The chatbot states right away that it is a chatbot”; (f) “The chatbot implies they are a real, live person.”
Participants’ Comfort Levels With Various Chatbot Scenarios
Discussion
The purpose of this study was to explore adults’ beliefs about integrating AI chatbots into the ACP process. We analyzed responses from 203 participants, including 128 who identified as healthy and 75 who identified as living with an LLI. Participants across both groups represented a range of racial, religious, and socioeconomic backgrounds. Most participants had given at least some thought to their own EOL care, with those identifying as having an LLI more likely to have considered it in depth. Additionally, more than half of the sample reported prior experience interacting with an AI chatbot, suggesting a baseline familiarity with the technology relevant to the study’s focus.
Utility of AI in Healthcare and ACP
We first examined participants' beliefs about the use of AI chatbots in healthcare broadly. Participants endorsed the use of chatbots for emotional support significantly less often than they did for the other categories. While we note that there may have been some variability in participants’ interpretations of the meaning of “accuracy” with regard to emotional support, participants’ open-ended responses indicated that they tended not to view chatbots as well-suited to providing comfort or empathy in medical contexts. This finding reinforces existing concerns about technological dehumanization in healthcare (Akingbola et al., 2024) and suggests that while chatbots may be viewed as useful for logistical or informational tasks, they are not perceived as appropriate substitutes for emotional or relational aspects of health communication. The only significant group difference was in the domain of specialist referrals, where participants with an LLI were more likely than healthy participants to believe that a chatbot could help them find the right specialist. This difference may reflect the LLI group’s more frequent navigation of the healthcare system and use of specialist care; however, due to the number of group comparisons made, we interpret this result with caution.
Participants’ views of using AI chatbots for ACP specifically also reflected both openness and ambivalence. Some participants were curious or cautiously optimistic, highlighting AI’s ability to offer general information, guide reflection, and improve access to planning tools. A few mentioned chatbots’ potential to reduce human bias or judgment, appreciating the objectivity AI might bring to sensitive conversations. Others pointed to chatbots’ convenience and scalability, especially in situations where human support is limited. However, not all participants were open to the idea of AI integration into ACP. Participants voiced doubts about the accuracy and reliability of chatbot-generated content and questioned whether such tools could adequately address the emotional, ethical, and contextual complexity of ACP communication. Preference for human connection and emotional support was a recurring theme, with some respondents asserting that chatbots lack the empathy, nuance, and understanding required for meaningful ACP conversations. One participant provided a concise summary of a perspective expressed by many: I would be somewhat open to chatting with a chatbot for learning about end-of-life care and clarifying my values around advance care planning. A chatbot could provide helpful general information, prompt reflection, and offer resources. However, I would prefer to discuss deeply personal or complex concerns with a human professional, as these topics require empathy, nuance, and individualized guidance.
Concerns about data safety and privacy were also prevalent, particularly regarding how information might be shared or exploited by corporations. Several participants expressed discomfort with the motives driving AI development, citing fears of corporate greed, cost-cutting, and the dehumanization of healthcare. As one participant starkly put it: I know the corporate world is trying to save money and boost the profits of the one percent and corporate owners, but I wish not to play their games and live in the world controlled by software. I would prefer to speak with a real human being on matters such as life and end of life care.
These findings suggest that while some users are open to experimenting with AI in ACP contexts, many are not convinced that the technology is ready, or appropriate, for such deeply human matters—as one participant wrote, “What does a chatbot know about life?”
The Role of Health Care Providers
Our findings underscore the central role that healthcare providers continue to play in ACP communication. Nearly three-quarters of participants indicated a preference for in-person ACP conversations with a medical professional over virtual conversations with an AI chatbot, citing trust in their healthcare provider’s expertise and a strong desire for emotional support. Participants who were neutral or unsure about their preferences tended to recognize the benefits and limitations of both human and AI-facilitated conversations, and explained that their preferences would depend on factors such as medical urgency, provider familiarity, or the complexity of their condition. Some participants noted that longstanding, trusting relationships with their providers made them feel more comfortable discussing their EOL preferences, consistent with research suggesting that patient-provider relationships are fundamental to effective ACP and effective medical practice more broadly (Akingbola et al., 2024; Forrow, 1994). Provider-offered ACP consultations have been found to significantly boost advance directive completion rates. One retrospective chart review study found that patients who were directly offered ACP consults ended up completing advance directives at extraordinarily improved rates: 65.9% completion in primary care settings compared with 1% of controls and 28.1% completion in the hematology/oncology setting compared with 3% of controls (Leak et al., 2021).
At the same time, some participants who preferred medical providers acknowledged that these ideal patient-provider relationships are not universally accessible. A few responses reflected concerns about limited appointment length, which is a known deterrent to patient-initiated ACP conversations (Bernard et al., 2020). Concerns were also raised about strained provider capacity and inequitable access to care due to insurance or other systemic barriers. Indeed, among the small subgroup of participants who preferred a chatbot, several cited practical convenience and ease of access as key reasons. Our findings suggest that although healthcare providers may be seen as the gold standard for ACP conversations, structural limitations in healthcare access may require the development of supplemental tools such as AI chatbots if ACP participation rates are to improve.
Participant responses revealed that comfort with AI chatbots in ACP conversations is highly dependent on the interaction context and the chatbot’s transparency. Participants were especially open to chatbot interactions when a face-to-face follow-up encounter with a physician was promised. Transparency also played a pivotal role: participants were very uncomfortable when the chatbot implied it was a real person and most comfortable when it clearly identified itself as a chatbot, which may be related to participants’ preference for text-based over voice-based chatbot interactions. Together, these results suggest, first, that human oversight is critical to chatbot acceptability, and second, that a chatbot that obfuscates its identity (by implying it is human) is particularly off-putting, perhaps because this suggests the tool cannot be trusted more broadly. ACP AI chatbot tool development in this context must therefore incorporate input from healthcare providers (Shevtsova et al., 2024), language training that produces emotionally attuned and empathetic language (Lederman & D’Alfonso, 2021) and incorporates bias mitigation language, and strong cybersecurity protocols (Mohsin Khan et al., 2025).
Study Strengths and Limitations
We successfully recruited participants who had given some thought to EOL care preferences and had some exposure to AI chatbots, supporting the appropriateness of the target participant groups. We did not recruit adults 18–49 without LLI, and only eight participants with LLI under age 50 participated, limiting our ability to generalize to adults under age 50. In addition, this survey was administered online via Qualtrics, which means participation required a basic level of digital literacy. While this was helpful in our goal of recruiting an audience with exposure to AI, those without internet access or who struggle with technology may have been excluded. Our sample was diverse across several domains, including a balance of men and women, a strong representation from those with federally administered insurance, and some notable diversity in race, religion, and income levels. However, these latter groups were not sizable enough to conduct group comparisons, which will be important in future research given that preferences for virtual healthcare assistance may vary by identity characteristics such as race (Vilaro et al., 2022). We were also limited in our ability to generalize our findings to individuals from some racial groups (e.g., Asian, Middle Eastern), with minoritized gender identities, with low educational attainment, struggling with financial insecurity, or without insurance, all of whom often face greater barriers in EOL equity (Jawed & Comer, 2024; McCune et al., 2025; West & Hollis, 2012). These factors should be considered when interpreting the findings and their implications for broader ACP and AI chatbot implementation.
Practice Implications
The responsible integration of AI chatbots into ACP could improve engagement, completion, and quality of ACP. Chatbots are not constrained by time as human providers are and may therefore enable increased ACP engagement at a patient’s preferred time, duration, and pace. AI chatbots have access to tremendous knowledge bases and can provide education tailored to individuals’ needs, offer key questions for consideration, and elicit details not feasibly generated in a brief patient-provider encounter. Further, as the worldwide population ages, those with lifelong exposure to digital generative AI tools are increasingly likely to expect its presence in healthcare throughout their lives. Indeed, AI is rapidly being integrated into healthcare communication, at a rate likely outpacing empirically based best practices to inform its development and deployment. Not only is there no prior research on patients’ views of the potential for AI chatbots to facilitate ACP communication, but there is also relatively little conversation analytic research on human provider-patient ACP communication on which to build (Parry, 2024). Continued research on human and AI-assisted ACP communication is imperative. Establishing foundational knowledge about potential users’ preferences when the technology is still nascent increases the likelihood that these tools will be developed with crucial user input.
This study highlights the complex perspectives adults hold regarding the integration of AI into ACP conversations. Participants in both healthy and LLI groups recognized the potential utility of AI chatbots in ACP, particularly for increasing access, providing information, and guiding reflection. However, they conveyed substantial skepticism about whether AI chatbots could or should replace the emotional depth, empathy, and contextual awareness of human professionals. While the vital role of healthcare providers in ACP remains clear, structural barriers in the healthcare system point to a space where thoughtfully designed AI tools could serve as a supportive bridge or supplement to human care. For AI chatbots to gain acceptance in such sensitive domains, program design must reflect a deep understanding of emotional nuance, prioritize transparency, and function in partnership with human providers rather than in place of them. Future efforts should focus on co-designing AI ACP tools with input from diverse users to ensure they meet the psychological, ethical, and relational needs of patients navigating EOL decisions.
Footnotes
Acknowledgements
We thank Katie Johnson and Sydney Kosnik for assistance with survey design and recruitment.
Ethical Considerations
This study was reviewed and deemed Exempt by the University at Buffalo Institutional Review Board.
Consent to Participate
Participants provided electronic confirmation of informed consent prior to survey completion.
Author contributions
Both authors contributed to study conceptualization and design. Data collection, analysis, and writing were led by NMK and supported by HNR. HNR provided critical revisions. Both authors agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Partial financial support was received from the American Psychological Association Summer Undergraduate Psychology Experience in Research (APA SUPER) Fellowship.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request, but restrictions apply due to participant privacy concerns.