
Abstract
As the U.S. population ages and interest in community-based approaches to death and dying grows, end-of-life doulas (EOLDs) are reshaping how individuals, families, and communities experience dying. Drawing on 23 interviews with practicing doulas, we identify the FAME model: facilitator, advocate, mediator, and educator. As facilitators, doulas make end-of-life plans actionable through practical, emotional, and existential support; as advocates, they amplify the voices of dying individuals and their families within healthcare institutions; as mediators, they navigate interpersonal dynamics and emotional tensions; and as educators, they demystify death and clarify options that are often unknown or misunderstood. Beyond identifying these roles, the FAME model delineates role boundaries, conceptualizes doula work in functional rather than spatial terms, and provides clearer language for articulating the scope of practice within this emerging field. Ultimately, we explore how doulas bridge Mallon’s micro model, Abel’s circles of care, and compassionate communities frameworks through micro-level caregiving, meso-level community engagement, and macro-level social change.
Keywords
Introduction
In recent years, end-of-life doulas (EOLDs) have emerged as a growing presence in U.S. deathcare, particularly as healthcare systems struggle to meet the complex emotional, logistical, and social needs of individuals at the end of life (Incorvaia, 2022; Rawlings et al., 2018). Current end-of-life care in hospices and hospitals remains highly medicalized, often prioritizing physical dying while neglecting emotional and spiritual dimensions (Clark, 2002; Floriani & Schramm, 2012; James & Field, 1992; Puchalski, 2001, 2007). Care is frequently fragmented across families, hospice, and medical institutions, leaving many unprepared to navigate the dying process. At the same time, hospice programs can be overburdened and unevenly distributed geographically, limiting access to adequate support (Jawed & Comer, 2024; Wan et al., 2023).
While the role of EOLDs continues to evolve, existing research primarily describes doulas as holistic and flexible “jack-of-all-trades” providers without clearly defining what the role entails or how it is understood by doulas themselves (Rawlings et al., 2019; Thompson & Utz, 2024). At the same time, growing interest in compassionate communities and community-based deathcare practices has fueled demand for more systematic research on how doulas understand, navigate, and perform their role as complementary partners in end-of-life care (Abel et al., 2013; Mallon, 2021; Rawlings et al., 2019).
This study builds on previous work by offering a systematic analysis of how doulas conceptualize their role within compassionate community frameworks. Rather than focusing on spatial location or emotional proximity to the dying person (Mallon, 2021), or a comprehensive taxonomy of doula support roles (Krawczyk & Rush, 2020), our framework makes four key contributions. First, the FAME model delineates the boundaries of these core roles, clarifying where they begin and end. Second, it conceptualizes doulas’ work in functional terms, emphasizing what doulas do rather than where they are positioned. Third, it connects these roles to broader processes of professionalization by providing clearer language for articulating the scope of doulas' work. Finally, by situating the FAME model within compassionate communities frameworks, we show how doulas' roles bridge micro-level caregiving, meso-level community engagement, and macro-level social change efforts.
Literature Review
Compassionate Communities, Circles of Care, and Mallon’s Micro Model
In response to systemic gaps in formal healthcare systems, particularly those organized around biomedical models of care, an aging global population, and widespread fear and lack of knowledge surrounding death and dying, the compassionate communities model has emerged as a public health approach to end-of-life care (Abel, 2018; Kellehear, 1984, 2013, 2015). Compassionate communities promote a holistic understanding of health that extends beyond symptom management to include psychological, spiritual, and social well-being (Dumont et al., 2022). Central to this framework is the recognition that death, dying, and bereavement are not solely medical events, but shared social responsibilities distributed across families, neighborhoods, and civic institutions (Abel, 2018; Abel et al., 2013). The model emphasizes strengthening social capital, building community capacity, fostering mutual aid, improving death literacy, and mobilizing actors beyond the formal healthcare system, including schools, municipalities, community organizations, faith groups, and informal caregivers (Bakelants et al., 2023; Dumont et al., 2022; Kellehear, 2015).
Empirical research suggests that compassionate community initiatives can strengthen social networks, reduce isolation, enhance bereavement support, and in some cases decrease unplanned healthcare utilization by mobilizing trained volunteers and informal caregivers (Dumont et al., 2022; Horsfall, 2018; Quintiens et al., 2022; Rawlings et al., 2018). By normalizing conversations about death and promoting death literacy, these efforts reduce stigma and increase collective caregiving capacity (Kellehear, 2015; Patel et al., 2023). At the same time, scholars note that compassionate communities are often articulated at macro or meso levels—focused on public health policy, municipal frameworks, or broad community initiatives—without clearly specifying how care networks are organized and sustained within households and immediate family systems (Bakelants et al., 2023; Mallon, 2021). Implementation can also be uneven, particularly in marginalized communities where structural inequalities, limited resources, or distrust of institutions shape access to care (Dumont et al., 2022). Together, this shift toward shared responsibility for death and dying broadens who is recognized as a legitimate provider of end-of-life care and creates space for emerging roles, such as EOLDs.
Circles of care (Abel, 2018) operationalize community and family networks to provide EOL care. At the center is the person with a life limiting illness, surrounded by an inner network of close family and friends who provide direct care and emotional support. The outer network consists of less close family members, friends, and neighbors who aid with practical tasks, such as meal preparation or running errands. Though this model is beneficial, Mallon (2021) notes that it has limitations in addressing the small-scale, domestic networks that often play a critical role in EOL care. To complement and complete this larger framework, Mallon (2021) proposes a micro-level model specifically designed for home-based caregiving.
To link compassionate community care within the context of the family, Mallon (2021), drawing on qualitative interviews with death doulas, introduces a micro-model structured around three flexible caregiving roles: the intimate, the gatekeeper, and the peripheral. The intimate role involves close, personal care and emotional presence for the dying person. The gatekeeper manages access to the home and information, acting as a boundary-setter and communicator on the dying person’s behalf, a role that requires organizational skill and emotional sensitivity (Mallon, 2021). The peripheral role supports the household through logistical tasks such as meals, errands, and upkeep, allowing individuals who may be emotionally overwhelmed by direct caregiving to still contribute meaningfully to the care network. While Mallon’s model offers a valuable extension to the compassionate communities framework at the micro level, we ground the FAME model in specific role enactments rather than just relational proximity, which provides a complementary lens that illustrates how doulas shift their functions across different layers of the care network.
Emergence of Doulas in EOL Care
Alongside community-based models, EOLDs have emerged since the early 2000s as a response to persistent gaps in conventional EOL care. The International End-of-Life Doula Association (INELDA) (2025) defines an EOLD as a non-medical person who accompanies, educates, and advocates for individuals and their circles of care during terminal illness and dying. Their emergence is closely tied to the structural and regulatory limitations of hospice and the broader U.S. healthcare system. As Incorvaia (2022) notes, regulatory burdens constrain hospices’ ability to provide continuous, holistic, person-centered care, particularly round-the-clock presence for dying individuals and their families.
Hospice care under the Medicare Hospice Benefit covers clinical services, medications, and grief counseling but excludes room and board, 24-hour in-home care, and curative treatments, and eligibility is limited to patients certified as terminal within six months (Centers for Medicare & Medicaid Services, 2023). As a result, families frequently face significant gaps in support when providing care at home, contributing to caregiver burnout amid longer life expectancies, dispersed families, and rising costs of institutional care (Carlson et al., 2010; Rawlings et al., 2018). Doulas step into this space and provide care that hospices, hospitals, and families cannot always manage. Because doulas work outside the formal healthcare system and are not eligible for insurance reimbursement, they are usually paid directly by families or provide services on a voluntary basis. This independence allows doulas to take on certain care tasks and provide forms of support that formal care workers cannot.
Although EOLDs are not medical providers, they complement clinical care by addressing the physical, emotional, social, and spiritual dimensions that span the entire dying process (Fersko-Weiss, 2017; Fukuzawa & Kondo, 2017). Research documents that in planning for death, they may assist with advance care planning, legacy work, and education about the dying process (Dellinger Page et al., 2022). As death nears, doulas may offer emotional support, vigil sitting, respite care, and create peaceful environments through spiritual or cultural rituals (Donley & Fannin, 2024; Garces-Foley, 2022). After death, they often support families with grief resources, funeral planning, and continued check-ins that may last months or even years (Dellinger Page et al., 2022). To meet growing interest, the International End-of-Life Doula Association (INELDA), founded in 2015, and the National End-of-Life Doula Alliance (NEDA), established in 2017, have emerged to support training, professional networking, mentorship, and broader professionalization efforts meant to further establish the field.
Conceptualizing Doulas’ Roles
Existing studies have provided essential descriptive overviews of doulas' roles. Our study seeks to extend this work by providing a systematic analysis of specific functions doulas perform within EOL care (Krawczyk & Rush, 2020; Rawlings et al., 2018; Thompson & Utz, 2024; Yoong et al., 2022). Much of this literature emphasizes doulas’ flexibility, acting as a “jack of all trades,” or as a “human Swiss army knife” (Krawczyk & Rush, 2020, p. 6) to meet a wide range of client needs and appeal to diverse types of people (Rawlings et al., 2019). Though their flexibility enables doulas to provide forms of care that other professionals cannot, families, medical professionals, and even doulas themselves struggle to define where doulas fit within care systems or how their work differs from those of hospice volunteers and other deathcare professionals (Rawlings et al., 2019).
Efforts to develop clearer taxonomies of doula work have emerged in recent years in both academic and practitioner settings. Krawczyk and Rush (2020), for example, conducted interviews with 22 doulas across the UK, U.S., Australia, and Canada to produce the first comprehensive framework for describing doulas' roles. They asked respondents to describe the role, provide characteristics of the role, and describe the services they provide, could provide, and shouldn’t provide as well as the obstacles and barriers they face. From this data, Krawczyk and Rush (2020) identified three primary descriptors—support, educate, and empower—and several secondary descriptors, including companion and presence; advocate and champion; coordinate, collaborate, and facilitate; mediate and guide; and assess and plan. While Krawczyk and Rush (2020) provide a comprehensive taxonomy of the characteristics of doulas and services they provide, our model builds on this foundation by further delineating doulas’ most common role features, where roles begin and end, how they overlap, and how they are enacted across diverse social contexts.
Beyond academic research, practitioners and EOLD organizations have also worked to define guiding principles, models of care, and core competencies. These approaches vary across organizations and reflect broader differences in how EOLD practice is conceptualized within this emerging field. For example, “The INELDA Doula Approach” centers on three principles—self-awareness in care, autonomy of the dying person, and recognition of the individualized nature of dying—which directly inform the organization’s core competencies (INELDA, 2023). In contrast, Patty Brennan’s “Doula Model of Care,” adopted by NEDA, emphasizes non-medical and non-judgmental support, holistic family-centered care, empowerment in decision-making, and collaboration with end-of-life care teams, while NEDA’s core competencies focus more explicitly on communication, professionalism, technical knowledge, and ethics (NEDA, 2026). As training organizations have expanded in recent years, so too have differences in how doulas’ roles, competencies, and models of care are conceptualized and taught. Reflecting this growth, the Global Doula Project is currently compiling an international directory of EOLD training organizations (2026).
Beyond articulating EOLD roles, there is a growing body of research connecting EOLD roles to compassionate communities and circles of care frameworks in the death and dying literature (Mallon, 2021; Rawlings, Davies, & Tieman, 2021). Mallon (2021) did this by taking a more micro approach to Abel’s circles of care model by introducing the Mallon model, which incorporates the intimate, gatekeeper, and peripheral roles. While Mallon (2021) successfully connects EOLD roles with the compassionate communities and circles of care literature, there remains an opportunity to further specify the concrete roles and practices doulas engage in at the micro level. Her analysis also provides a useful starting point for linking these roles to the macro-level social change efforts supported by compassionate communities, which our research further extends.
While interest in EOLDs is increasing, it is not entirely clear how these roles might be incorporated into end-of-life care systems. Professionalization literature suggests that the process of becoming a recognized field involves developing clearer boundaries and role definitions—particularly when distinguishing doulas from adjacent professions such as hospice workers or social workers (Francis, 2022; Keshet et al., 2023; Young, 2019). In Australia, this shift is reflected in the introduction of nationally accredited pathways such as the Certificate IV in End-of-Life Doula Services, which signals growing formal recognition of the role even in the absence of full regulation. Similarly, in the United States, the National End-of-Life Doula Alliance (NEDA), in collaboration with the Hospice and Palliative Credentialing Center (HPCC), is exploring the creation of a voluntary, nationally recognized certification program for EOLDs, expanding on its existing Proficiency Assessment (Hospice and Palliative Credentialing Center, 2025). However, within the doula community, this standardization is a subject of ongoing debate, as some fear it may reproduce the very medical hierarchies doulas seek to resist (Francis, 2022).
Our study builds on and extends Mallon’s (2021) and Krawczyk and Rush’s (2020) work by analyzing how doulas themselves conceptualize their labor within EOL care. Drawing from in-depth interviews with 23 practicing doulas, we identify the FAME model and the four interrelated roles—facilitator, advocate, mediator, and educator—that connect micro-level caregiving with meso-level community advocacy and extend to macro-level social change. We believe the FAME model provides a more comprehensive framework for understanding doulas’ roles by situating them within compassionate communities frameworks and clarifying how role articulation contributes to doulas’ ongoing professionalization efforts.
Methodology
Data Collection
Respondents were recruited through a combination of snowball and purposive sampling. Through a colleague of the first author, we were able to connect with and recruit several doulas for this study. The remainder of the respondents were recruited through EOLD professional organizations in the United States, INELDA and NEDA. Leadership at both organizations shared a recruitment flyer on their social media pages and membership email listserv. Interested participants then directly contacted the first author. Data were collected through semi-structured qualitative interviews over Zoom, allowing for in-depth exploration of participants’ experiences with death and dying (Kallio et al., 2016). Interviews were conducted between the Spring of 2023 and the Spring of 2024 and on average lasted between 1 to 2 hours. An interview schedule was utilized for each interview that asked a standard set of questions about respondents’ work background, roles and services during the dying process, interactions with clients and families, day to day work experiences, changes in EOL care, personal perceptions of death, and demographic characteristics. The interview schedule was adapted from a study on women moving into funeral directing (Donley & Baird, 2017) as well as other studies involving qualitative interviews with EOLDs (e.g., Tumber, 2020). Interviews were recorded with permission, transcribed using Otter.ai, and checked for accuracy by the authors. Informed consent was obtained prior to interviews, participants were informed of the study purpose and their right to withdraw, and all data were deidentified with pseudonyms assigned to protect confidentiality. This project was approved by the authors’ university Institutional Review Board (03142024-02) and maintained ethical standards of human subjects research.
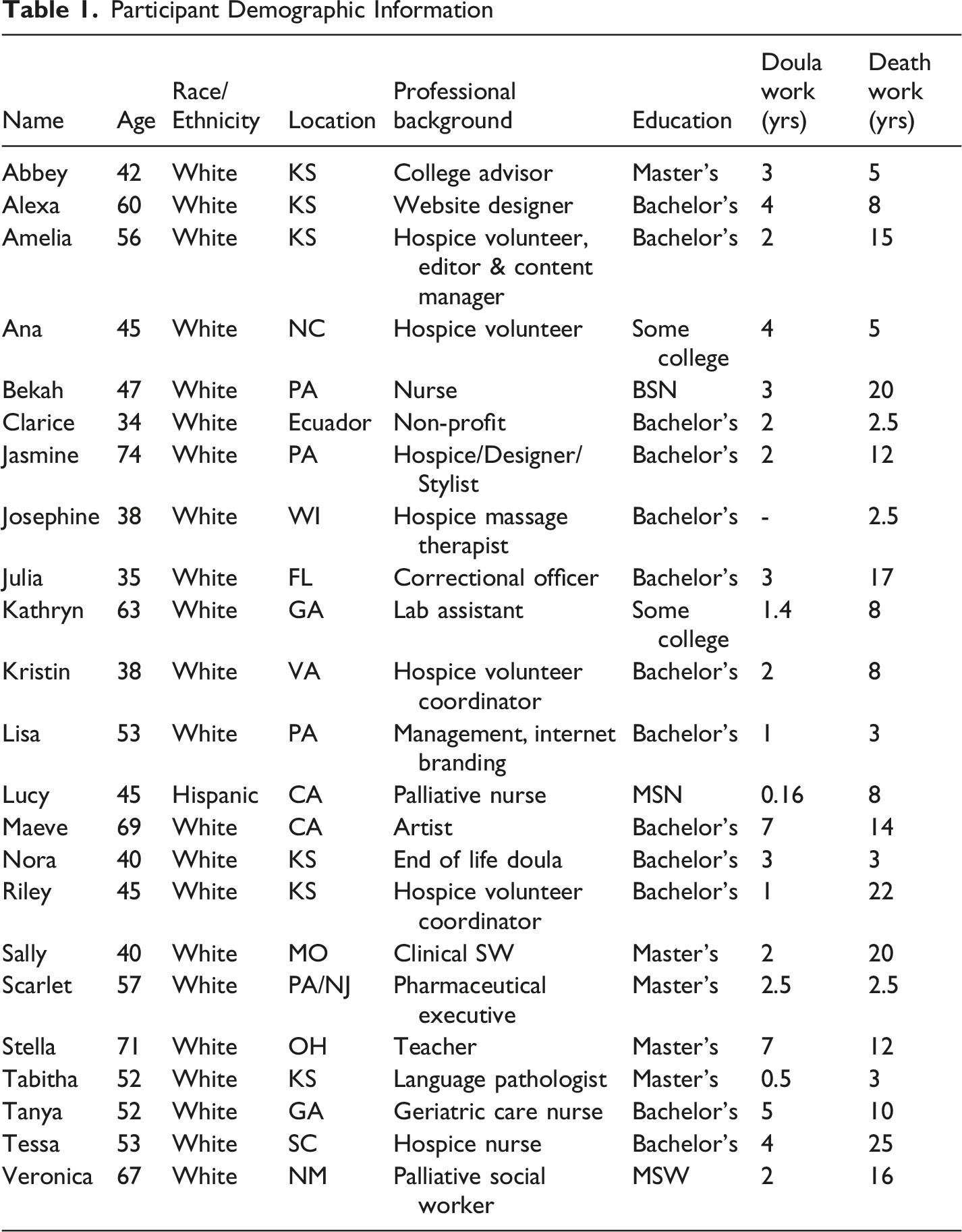
Sampling
Participant Demographic Information
Data Analysis
We used deductive thematic analysis which involves developing a coding frame prior to analyzing the data (Fereday & Muir-Cochrane, 2006). Our coding process was guided by the following research question: How do respondents conceptualize their role as an end-of-life doula? When we asked doulas, “How would you define an end-of-life doula?” or “What are the primary roles and responsibilities of an end-of-life doula?” many participants initially responded with some version of “we do everything,” similar to Krawczyk and Rush (2020). However, as they elaborated on their experiences of working as doulas, we began to see patterns in the verbiage used to describe their work. Thus, our data analysis began with coding how doulas described their role enactments in their day-to-day work across different social contexts, rather than relying on how they broadly characterized themselves as “advocates” or “facilitators.” In short, we coded their transcripts for when they described actually performing the role. In practice, this meant prioritizing narrative accounts of specific interactions, decisions, and situations over abstract role descriptors or aspirational statements about what doulas should do.
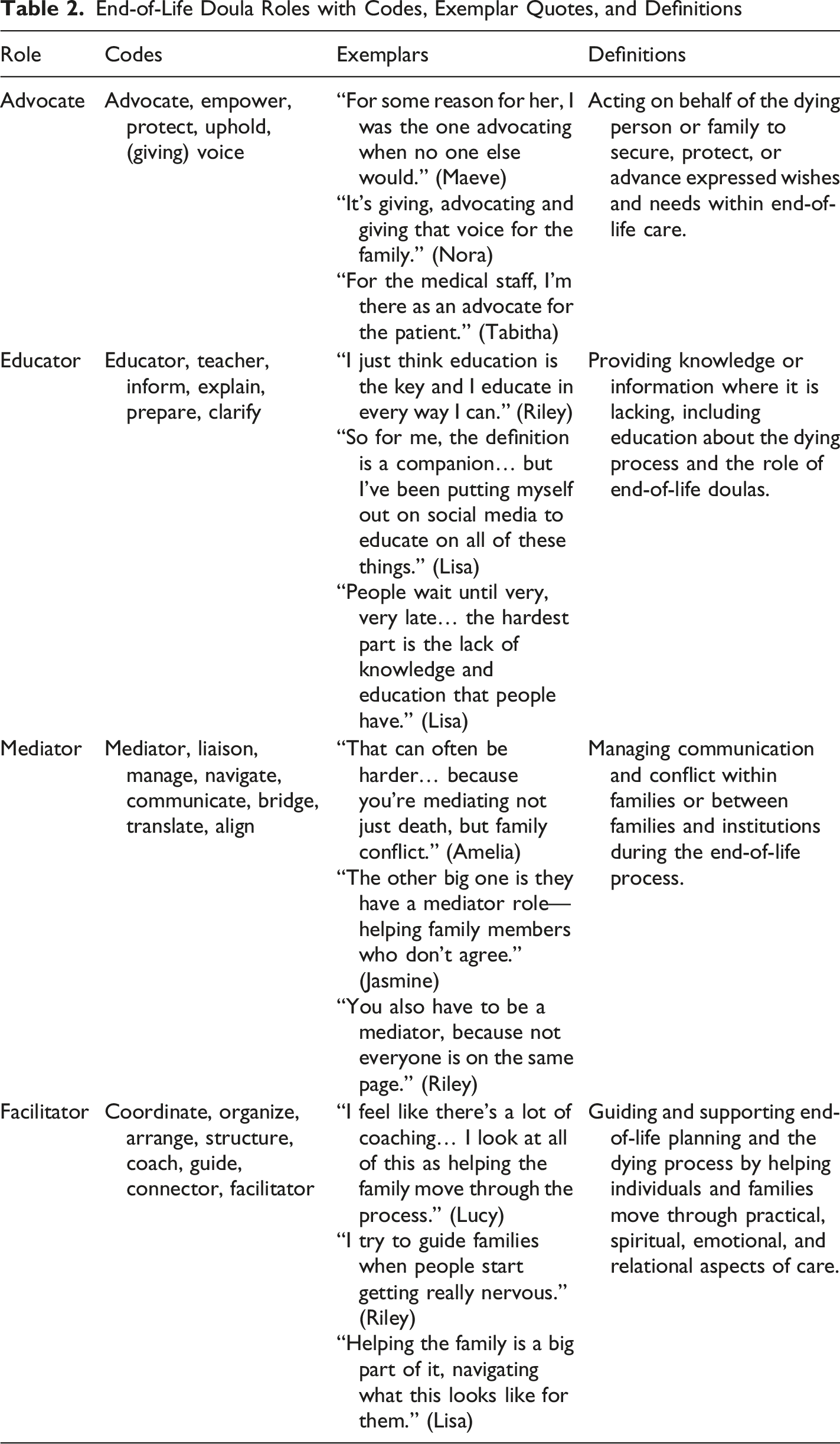
End-of-Life Doula Roles with Codes, Exemplar Quotes, and Definitions
Although the four roles of the FAME model were derived through a deductive coding process, the interpretation of our findings suggests strong theoretical alignment with the compassionate communities frameworks. Many respondents mentioned characteristics of compassionate communities throughout their interviews, such as improving death literacy, strengthening circles of care, connecting families across healthcare and community networks, and advocating around EOL care. Consequently, throughout the remainder of this paper, we situate the FAME model as a framework for understanding how doulas' roles bridge healthcare institutions, families, and community networks.
As qualitative sociologists, we approached this study as outsiders to end-of-life doula practice, as we do not have formal training or professional experience as doulas. This often prompted the first author to ask additional probing questions to clarify participants’ day-to-day work experiences. During analysis, this outsider perspective likely influenced how broadly we coded for roles to ensure we captured the full range of activities respondents described. By prioritizing verb-based descriptors of how doulas articulated their day-to-day functions, we developed a coding framework grounded in participants’ accounts.
The FAME Model
In the FAME model, doulas enacted four central roles—facilitator, advocate, mediator, and educator—that reflect how they address gaps across medical institutions and family caregiving. These categories therefore should be understood as ideal types that clarify distinct dimensions of the doula role rather than as exhaustive or rigid classifications. They are not mutually exclusive but rather highlight the multiple, overlapping forms of expertise doulas most commonly draw on in their work. Although all four roles were present across interviews, educators and facilitators were enacted most frequently, followed by mediators and advocates. The prominence of the educator role likely reflects the fact that doulas remain relatively unfamiliar and only partially integrated within end-of-life care systems. As the field becomes more widely recognized, the salience of these roles may shift. Doulas emphasized these roles differently across interviews, enacted them discretely depending on context, and at times these roles intersected.
Facilitating the End of Life (Care)
Doulas often described their role as facilitators—helping people prepare for death and then assisting in the dying process itself. Doulas described helping with everything from practical tasks to emotional prep and advance care planning. Much of this practical support depends on the client and family’s personal preferences. Lisa explained, “Helping the family is a big part of it,” and talked about gathering care options, organizing appointments, and just making sure people have what they need. Kristin shared how she pulled together a team to clean a client’s house. According to Kristin, this kind of preparation isn’t just about logistics and practical domestic support, it’s about helping people understand what’s coming and making sure the person dying has what they need. Other doulas talked about the importance of demystifying the legal and planning side. Nora said, “It doesn’t have to be expensive [...] you can get your advanced care directives, a legal document, for $5,” and focused on helping people feel less overwhelmed. Clarice described helping expats navigate systems across countries and how the end-of-life laws differ between countries. These forms of facilitation often overlapped with education and advocacy, as planning conversations became opportunities to clarify options, reduce fear, and reinforce client preferences. Respondents offered services on a sliding scale or on a purely volunteer basis primarily for close friends or family in the absence of being covered by health insurance.
Doulas also facilitate the actual dying process and this is perhaps the part people don’t always see, but sitting vigil is essential to doulas' work. They help families stay grounded, talk through what’s happening, and make the experience as close as possible to what the dying person wanted. Abbey said, “Do you need your dog on your lap? [...] Who do you want there, and who don’t you?” Tabitha put it simply: “I make it as peaceful and beautiful as I possibly can.” Lisa talked about walking families through what death will look like—how the body changes, how to keep someone comfortable, and how to create a space that actually reflects what the person wants: “How do we keep out the ones you don’t want here? [...] What do you want? It’s your day,” she said. Riley talked about how getting families to talk and share memories as someone is actively dying is “the best soundtrack you could have at the end of life.” Alexa described helping families create small rituals and intentional spaces during the dying process, explaining that “there’s little human things you can do” to help families “start to kind of set a stage for what’s actually happening.” Rather than focusing solely on medical decline—“the heart rate’s going down”—she encouraged families to share stories, write reflections, listen to music, use comforting objects such as blankets to create more peaceful and personalized experiences. These examples show how facilitation extends beyond logistical coordination (who is/isn’t in the room) to include emotional, spiritual, and ritualizing support, making the dying process more intentional and meaningful. By bringing together families, friends, and care providers, doulas facilitate care across formal and informal care networks.
Advocating for Voice and Autonomy
EOLDs recognize that at the end of life, many people lose autonomy and a sense of control over what happens to them. While both advocacy and mediation involve communication across the care network, advocacy is about acting on behalf of the client or family while mediation is about managing communication within the care network. Doulas intervened on behalf of clients while also building families’ capacity to advocate for themselves. Tessa explained, “I just want them to always know that they are in control still, because they’ve lost, typically they’ve lost a lot of independence, and a lot of decision making.” Amelia said it’s about “keeping the patient’s wishes and desires forefront [...] being the patient’s advocate when they’re unable to [speak], just to make sure that stays part of a conversation.” The role of advocate is thus twofold: advocating for client autonomy while clients maintain some level of control but it can eventually shift to a proximal form of advocacy. Here, the doula’s labor becomes a safeguard for the client’s wishes, ensuring ‘good care’ is maintained even when the individual can no longer make decisions for themselves. What made doulas especially effective in this role is that they occupy an outsider role compared to family members. Ana explained, “You’re in such a high emotional state that your thinking and logic brain aren’t able to process all of that [...] it’s so important to have somebody [...] kind of like the outside observer just taking notes.” That distance gives doulas a more objective approach to make sure clients’ wishes do not get overlooked in the process.
Doulas also advocated for families, especially when navigating medical systems that were confusing, dismissive, or too fast-paced to explain things clearly. Doulas described themselves as translating information, asking questions, or helping families communicate concerns when they did not feel able to do so themselves. Tabitha described being that go-between: “You push that button [for a nurse] and you might wait 20 minutes [...] whereas I can walk down to the nurse’s station and talk and ask a question and bring it back to the family.” Tabitha’s role as a 'go-between' is defined by her ability to act as a proxy for the family, taking on the practical responsibility of retrieving information from medical staff. At times, this advocacy meant empowering families and clients to speak up for themselves and ask medical staff questions. Respondents often described families feeling uncertain about their role in end-of-life decision-making and hesitant to ask questions. Nora framed advocacy as helping families recognize that they still “have a voice.” In her interview, she discussed the “humongous train of end of life” and the assumption that this is simply “how it’s always been done,” even though not everyone “wants it that way.” For Nora, doula advocacy involves “advocating and giving that [decision making] back to the people.” Reflecting on a situation in which a family expressed concern that repeated administration of morphine caused a dying grandmother to sleep during periods when she was otherwise “alert and engaged in conversations,” Nora explained that many relatives assume “if hospice and these doctors and nurses are telling me that this is what has to be,” then they have little choice in the matter. In response, Nora encouraged the family to share their concerns with medical staff, reminding them that “nobody is gonna know what their [grandmother's] needs are and what they want and what they like more than you.” Part of doulas' work involves supporting families in recognizing that they have a voice and that their understanding of their loved ones’ needs is important. For doulas, advocacy is both protective action (ensuring wishes are respected) and empowerment (teaching families to speak up for themselves). These examples illustrate how doulas engage in direct advocacy while also supporting clients’ and families’ capacity to advocate for themselves.
Mediating Conflict and Communication
Doulas often described themselves as mediators—especially when families do not agree about end-of-life decisions or are emotionally scattered. Mediation, according to our respondents in this study, means acting as a neutral bridge, centering the client while navigating family conflict, cultural differences or misunderstandings with medical staff. Riley said, “You have to be a mediator with family [...] Sometimes you have to be that equalizer to calm things down.” Julia noted that conflict can get more intense when there are cultural or religious differences, especially if the client and their family don’t share the same beliefs: “The family thinks that they know what’s best [...] but that’s not exactly the case. [...] Whatever the client says, that’s the law.” Doulas talked about holding firm on that point—centering the client—while also helping families adjust to what that means in practice. Kristin talked about taking the time to understand family dynamics and “bridge the gap” between them and hospice or medical staff. Jasmine’s example shows how sometimes roles intersect, explaining, “We’re the liaison, we’re advocating for the families, getting information from the medical team; we’re part of the team but not medical.” Riley, also enacting multiple roles at once, described a strategy of redirecting when things start to escalate, saying, “Sometimes you need to kind of split people up [...] educate, and then reconvene.” For doulas, managing conflict is not about resolving disputes but about creating conditions that allow families to remain focused on the dying person.
Moreover, doulas describe navigating these situations as akin to walking a tightrope. Nora put it bluntly: “A tightrope walker is my number one. Families and end of life are all over the map.” She explained how some family members try to pull her into their side of the story or unload their frustrations about others. Her job, she said, is “being that neutral party [...] just walking that tightrope.” Other doulas used similar metaphors. Tessa described it as “tiptoeing” through conversations that require both honesty and sensitivity, especially when trying to help families catch up to where the client already is in the dying process. She elaborates: “It's just everybody else catching up…the hardest part about bringing people to the same page of where the dying person typically is…if I were to say a challenge, it would be tiptoeing and gently delivering the, the urgency, the timeline, we're talking days or weeks.” Veronica added that most families come in with “unresolved issues [...] hurts or fears” that can get in the way of communication and planning. And while doulas don’t try to resolve conflict, they act as steady guides—neutral, calm, and focused on the client. Amelia elaborates on how her role as a mediator means she must act as an information gatekeeper at times: “If you’re in the patient’s confidence, you do have to be careful about getting their permission to share anything they share with their family.” Doulas in their role as mediators make it clear to the family that their loyalty is to the person who’s dying—not to managing everyone else’s expectations. These examples illustrate how doulas manage conflict and communication in ways that help maintain focus on the needs of the dying person and the overall experience of dying.
Educating for Death Literacy
Doulas consistently described themselves as educators. Their role as educators took three forms: informing the public about their role as EOLDs, providing community death education, and demystifying the death process. The role is still unfamiliar to most people and that makes it harder for doulas to justify why their work is needed. Nora put it plainly: “We’re so new, we’re trying to first of all, educate; educate people on who we are, what we can do.” Riley described being dismissed by medical staff who didn’t understand the doula role, saying, “You’re gonna think that a doula is a nobody, they’re just in the way.” These reflections highlight a central challenge: not simply invisibility, but questions of professional legitimacy. Educating others on their role and how they are different and necessary for EOL care is an important strategy for countering this perception and legitimizing their expertise (Francis, 2022).
Community death education represents a central component of how doulas describe their work, extending beyond individual clients to broader public and professional audiences. This work takes many forms. Most notably, doulas discussed developing curricula or classes for a range of audiences. For example, Riley explained that she offers a three-session “Death Doula 101” course covering preparation, the active dying phase, and what happens after death. Abbey, Alexa, and Kristin described designing continuing education courses for nurses and social workers. Ana discussed organizing workshops for younger adults on “getting your affairs in order,” while others developed sessions for palliative care teams and oncologists on how to discuss final wishes with patients. Some hosted local Death Cafés. Doulas further described giving guest lectures in social work college classes and offering public talks to community organizations and groups (such as libraries, churches, retirement communities, funeral homes and adult education programs), contributing to broader death literacy efforts.
Finally, doulas described how they demystified the death process for families. Many doulas describe how families contact them very late, and are unfamiliar with EOL options, hospice policies, how to plan for death, and what a good death entails. Lisa explains this in more detail, “People wait until very, very late [...] The hardest part is the lack of knowledge and education that people have.” Maeve added that families often don’t even know how to interact with the person who’s dying: “Most family members have never been into death. And they’re freaked out by it.” Maeve then goes on to explain how she teaches families how to communicate with dying loved ones—another example of the intersection of doulas’ roles. Tabitha also noted that families often want guidance in real time: “Sometimes they’re like, yes, tell us everything.” This lack of preparation can be a detriment to families. Veronica shared a story about a woman whose husband died without help because she didn’t know she had a choice in providers. “She tried doing it all on her own,” Veronica said. “It was very traumatic.” Respondents described these situations as particularly difficult and emphasized how earlier involvement might have changed the experience for families.
Discussion
The purpose of this study was to better define the roles of EOLDs through in-depth interviews with 23 doulas working across a range of settings. Importantly, we sought not only to articulate a clearer framework for these roles but also to examine how they intersect with the broader framework of compassionate communities (Abel, 2018; Kellehear, 2013, 2015). While prior studies generally describe how doulas provide flexible, holistic care across the dying process (Krawczyk & Rush, 2020; Rawlings et al., 2018; Thompson & Utz, 2024), fewer studies have systematically conceptualized how doulas themselves define and understand their roles. Our findings identify the FAME model consisting of four core roles—facilitator, advocate, mediator, and educator. The FAME model extends prior models by 1. Delineating the boundaries of what the core roles are while clarifying areas of overlap, 2. Conceptualizing doulas’ roles as functional rather than spatial, 3. Connecting the conceptualization of doulas’ roles to ongoing professionalization projects, and 4. Demonstrating how doulas' roles bridge Mallon’s micro model, Abel’s circles of care, and the macro-level social change efforts of compassionate communities.
The FAME model refines prior typologies by synthesizing overlapping descriptors into functional mechanisms. While Krawczyk and Rush’s taxonomy offers a valuable descriptive account of doulas' roles, there remain opportunities to further clarify role boundaries and how they can inform the emerging professionalization of EOLD work. For example, in our model, empower, advocacy, and champion are collapsed into Advocate; and coordinate, collaborate, facilitate, assess and plan, ritualizing for meaning making, and after-death care and funeral planning are collapsed into our category Facilitator. Instead of addressing the full scope of doulas’ work, we clarify the most common functions through which they coordinate EOL care in practice. Moreover, the FAME model offers clearer boundaries for each role, where they begin and end, as well as the functions attached to each. Because Krawczyk and Rush’s (2020) study was international in scope, drawing on a small number of participants across multiple countries, it is less focused on how doulas perform their roles within specific contexts. The FAME model builds on these frameworks by further delineating doulas' role boundaries and the specific labor involved in each role within a U.S. context, though the enactment of these roles may vary across international healthcare systems and cultural contexts.
Second, our model also contrasts with Mallon’s (2021) micro model, which categorizes doulas as intimate, gatekeeper, or peripheral based on their relational and physical proximity to the dying person. While Mallon’s typology is valuable for mapping the relational positioning of doulas within care networks, our research provides a complementary lens by further specifying functions and tasks doulas perform within those spaces. By grounding our model in functions rather than relational proximity, our model highlights how doulas fluidly adopt and shift roles in response to contextual needs. These frameworks are not incompatible. Our role-based typology could complement Mallon’s micro model by linking relational positioning within family, community, hospice, and healthcare networks to the specific dimensions of care provided by doulas (Abel, 2018; Kellehear, 2015). For example, doulas who operate in the “intimate” zone might most frequently act as facilitators or advocates, while those situated more peripherally may primarily perform educational functions or coordinate practical forms of support. Likewise, the gatekeeping role Mallon describes can be better understood through the concrete functions of mediation that doulas engage in to manage family conflict and interpersonal dynamics (DeDiego et al., 2023; Fukuzawa & Kondo, 2017). Our findings suggest that doulas could enact the same core roles—facilitation, advocacy, mediation, and education—across different spatial and relational contexts. In other words, they may enact the same role at varying distances from the dying person, depending on client needs, family dynamics, and care settings. This reinforces the idea that proximity does not always determine function, and that doulas contribute meaningfully whether at the center or periphery of care. Together, these frameworks provide a more holistic and comprehensive account of EOLDs’ work by recognizing both where doulas are situated within circles of care and the specific dimensions of care they provide. In doing so, they highlight how doulas’ roles shift across relational contexts while still maintaining similar core functions.
Third, the move toward role definition is tied to ongoing debates within the doula community about professionalization, as many doulas expressed frustration with the ambiguity surrounding their role and having to educate families, institutions, and professionals about who they are and what they do. Because EOLD work remains unregulated, ambiguity is built into both practice and the way organizations describe doulas’ work. INELDA defines doulas as non-medical companions providing emotional, spiritual, and practical support (2025), while NEDA notes there is “no all-inclusive or definitive list” of services (NEDA, 2025). Such open-ended language mirrors the way many participants initially described their role as “doing everything.” Moreover, families often face needs beyond what hospice or medical staff can provide, and doulas’ flexibility makes them appealing.
While the unregulated nature of the work means boundaries between roles are porous, the FAME model captures how doulas in their own words describe their work without imposing rigid job descriptions. Doulas' clearly (and consistently) articulating the scope of their roles would be a helpful step toward legitimacy and perhaps greater integration and collaboration in institutional settings (Dellinger Page & Husain, 2023; Young, 2019). Although EOLD care is not currently covered by private insurance, Medicare, or Medicaid, an increasing number of states have begun allowing birth doula services to be reimbursed through Medicaid, and in some cases private insurance plans (Herbert, 2025). These policy developments suggest emerging pathways for formal integration of EOLDs work into healthcare systems. The FAME model provides a useful heuristic for understanding how doulas describe and enact their roles across end-of-life care settings. Furthermore, the model is intended as a flexible and evolving framework rather than a prescriptive or de facto account of doula practice, allowing it to adapt as additional research emerges and doula practices continue to develop across international healthcare systems and cultural contexts.
Still, some doulas expressed concern that narrowing the scope too much would replicate the rigidity of the systems they were trying to resist, or that excessive standardization risks over-professionalizing a role that is defined by its flexibility and relational nature. This ambivalence echoes what professionalization scholars have noted—namely, that setting boundaries is part of becoming a recognized field, but those boundaries can also limit autonomy and exclude people whose practices don’t conform (Francis, 2022; Keshet et al., 2023; Young, 2019). While ambiguity can create challenges for role clarity and professional recognition, it can also function as a strength by allowing doulas to adapt to the diverse needs of dying individuals and their families. The flexibility of the FAME model therefore allows doulas to retain that adaptability while simultaneously offering clearer ways to articulate doulas' work. Our model offers a middle path between the “jack-of-all-trades” model that dominates current descriptions and the highly specialized, formalized roles found in the medical model that many doulas resist.
Finally, situating doulas' roles within the compassionate communities framework highlights how doulas translate community-based ideals into everyday EOL care (Kellehear, 2013, 2015). The goals of compassionate communities—to normalize death, promote death literacy, strengthen community capacity for care, and integrate health, social, and civic systems (Abel, 2018; Kellehear, 2013, 2015)—are enacted through the roles identified in this study. As educators, doulas normalize death and build death literacy by demystifying the dying process and facilitating open conversations about EOL care. As advocates, they strengthen community capacity by empowering clients and families to articulate wishes, communicate with medical providers, and maintain control over end-of-life decisions. Through facilitation, doulas coordinate care across families, hospice, and community networks, helping reduce fragmentation between social and medical systems of care. As mediators, they sustain relationship cohesion by navigating conflict, cultural differences, and communication breakdowns, ensuring that care remains centered on the dying person. Importantly, research notes that compassionate communities are difficult to operationalize across diverse cultural, institutional, and family contexts (Horsfall, 2018). Our findings suggest that doulas could help address this challenge through their flexible, relational, and context-specific role enactments tailored to the specific needs, values, and constraints of particular families, various healthcare settings, and ultimately communities. Doulas operate across micro, meso, and macro levels of care as on-the-ground actors who make compassionate communities actionable rather than abstract. Notably, the FAME model offers healthcare systems and organizations a framework for understanding and articulating doulas' roles within end-of-life care.
Implications, Limitations, and Future Research
This study has several practical implications, along with limitations that point to areas for future research. Although multiple major U.S.-based professional doula networks offer training for EOLDs, core competencies vary, ranging from process-oriented, relational frameworks to more task-based and skills-driven models. As a result, there is no standardized framework defining the core competencies and skills required for practice. More systematic role categories could help structure certification content and promote greater consistency across this emerging profession. For healthcare systems, clarifying these roles may help identify where doulas can be integrated into existing models of care. For doulas themselves, having clearer language to describe their work could help families, medical professionals, and the general public better understand where they fit in end-of-life care.
Situating the FAME roles within Mallon’s micro model, Abel’s circles of care, and the broader compassionate communities framework highlights how doulas enact community-based end-of-life care in practice. Rather than centering support solely within medical institutions, the FAME model shows how doulas help organize, stabilize, and extend care by linking families, hospice services, and broader community networks. However, a full evaluation of how these roles operate within and across compassionate community systems remains an important direction for future research.
At the same time, this work is not without limitations. The sample consisted primarily of white women in the U.S., which reflects broader demographics in doula work. Because compassionate communities emphasize shared caregiving and collective responsibility rather than a professionalized role alone, the FAME model could also inform doula-like care enacted by individuals who do not fit the “typical” demographic or professional profile reflected in existing samples. This shifts the focus to community embedded care practices rather than professional roles. Future research should therefore examine how diverse caregivers—including doulas of color, queer doulas, and culturally specific community death workers—engage in forms of care that align with compassionate community frameworks. Because existing research relies on doulas’ own accounts of the care they provide, more research is needed to examine how clients and families experience and interpret doulas' roles.
Our findings are highly contextualized by the structural conditions of the U.S. end-of-life care system, which shaped how participants described their roles—particularly the emphasis on advocacy, mediation, and providing continuous support where formal services fall short. Because international hospice and healthcare systems are often structured differently across nations, doulas' roles may shift subtly in response to those specific institutional environments. Beyond structural variations, the FAME model is also influenced by U.S. cultural perspectives on death. In other places, where death is more communal or less medicalized, the necessity for roles like the “advocate” or “mediator” may be less pronounced than in the individualistic and death-avoidant U.S. context. Moreover, EOLD movements are taking distinct shapes in the UK, Canada, and Australia. Compassionate communities as a public health approach is more salient in the UK and Europe compared to the U.S., so other roles might be more relevant in those contexts. Thus, while the FAME model offers a systematic framework, it may require adaptation, and future research should examine how doulas’ roles are enacted across diverse healthcare and cultural contexts.
Conclusion
This study and the FAME model presented in it provide a more systematic framework for understanding the roles of EOLDs compared to earlier models. The FAME model offers an alternative to vague or overly generalized portrayals of doulas as endlessly flexible by providing a clearer picture of the actual functions they perform to anchor families, hospice, and community care networks. Moreover, situating these roles within the compassionate communities framework highlights how doulas bridge community-based end-of-life care by connecting families, communities, and institutions in everyday practice. In doing so, the FAME model contributes to ongoing efforts to articulate the scope of doula practice more clearly, particularly within broader processes of professionalization.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.