
Abstract
Bereavement may trigger a variety of psychological reactions, including prolonged grief disorder (PGD), depression, and loneliness. This study aimed to explore the co-occurrence patterns of these symptoms among Chinese bereaved university students. Using latent class analysis (LCA), four distinct classes were identified: a high symptom class (22.2%), a predominantly grief class (21.9%), a moderate symptom with prominent anhedonia class (23.3%), and a low symptom class (32.6%). Individuals with poorer physical condition, rural residence, unexpected loss, or lack of opportunity to say goodbye were more likely to belong to the high symptom class, whereas chronic disease-related loss was linked to lower odds of this membership. Additionally, the class membership significantly predicted functional impairment six months later (n = 159). Predominantly grief class (M = 11.61) and moderate symptom with prominent anhedonia class (M = 14.33) showed significantly higher impairment. These findings highlight the heterogeneity of bereavement responses and inform targeted interventions.
Introduction
Bereavement is a significant life event universally experienced by humans (Stroebe et al., 2007; Thimm et al., 2020). Among university students, bereavement is particularly prevalent and is one of the most frequently reported stressors (Balk et al., 2010; Hay et al., 2026; Huang et al., 2025): approximately 35–55% of students experience such a loss within a two-year period (Balk et al., 2010; Cousins et al., 2017; Varga et al., 2021). In addition, since the start of their freshman year, 60% of senior students have experienced at least one bereavement (Huang et al., 2025). Grief is a common response that individuals exhibit following the loss of a significant other (Stroebe & Schut, 1999). Prolonged grief disorder (PGD) is diagnosed when grief extends beyond culturally expected timelines and is marked by intense yearning or preoccupation with the deceased—such as intrusive memories or persistent longing (Killikelly et al., 2025; Simon & Shear, 2024). PGD is officially included in both the Diagnostic and Statistical Manual of Mental Disorders, fifth edition, text revision (DSM-5-TR) and the 11th edition of the International Classification of Diseases (ICD-11). According to the DSM-5-TR criteria, PGD symptoms must persist for over 12 months (American Psychiatric Association, 2022), while ICD-11 criteria require a duration exceeding 6 months (World Health Organization, 2022a). In a population-based sample, the point prevalence of PGD among the bereaved varied between 4.7% and 6.8% (Treml et al., 2024), while this rate reached 14.2% among bereaved university students in mainland China (Jiang et al., 2025).
Grief is frequently accompanied by depressive symptoms (Cox et al., 2015), which may significantly impair the cognitive functioning and academic performance of bereaved college students (Balk, 2008). An estimated 63% of individuals with prolonged grief symptoms also experience co-occurring depressive symptoms (Komischke-Konnerup et al., 2021). Depression involves a depressive mood (such as sadness, irritability, feelings of emptiness) or loss of pleasure, along with other cognitive, behavioral, or neurovegetative symptoms that severely impact an individual’s functioning ability (World Health Organization, 2022b). Although PGD and depression share overlapping features, such as sadness, guilt, and difficulty concentrating, numerous studies have demonstrated they are distinct psychological constructs (Boelen & Lenferink, 2020; Malgaroli et al., 2018; Robinaugh et al., 2014). The primary distinguishing feature of PGD is the presence of intense yearning or longing for the deceased and a persistent desire to seek proximity to the deceased person, whereas depression is defined by a pervasive depressed mood and a marked loss of interest or pleasure in most activities (Shear, 2015; World Health Organization, 2022a).
Prolonged grief symptoms also represent a distinct factor contributing to loneliness (Eisma & Buyukcan-Tetik, 2025; Vedder et al., 2022). Although intense loneliness is explicitly included in the DSM-5-TR criteria for PGD but not in ICD-11, loneliness represents a broader interpersonal construct that is conceptually distinct from PGD and may show different patterns of co-occurrence with grief (American Psychiatric Association, 2022; World Health Organization, 2022a). Therefore, the aim of this paper is to investigate whether loneliness accompanies grief among bereaved university students. Moreover, a recent study suggests a mutually reinforcing relationship between the two: loneliness may perpetuate grief reactions, while persistent grief may, in turn, intensify feelings of loneliness (Eisma & Buyukcan-Tetik, 2025). Loneliness is characterized by a subjective sense of dissatisfaction stemming from the perception that one’s social network lacks adequate size or meaningful engagement (Hawkley & Cacioppo, 2010). Research has shown that self-adjustment and social support can alleviate loneliness, whereas the absence of these protective factors may intensify it (Nisa & Lestari, 2023). However, in the aftermath of the global pandemic, pandemic-related burnout has contributed to psychological distress (Sun et al., 2022), and social isolation has intensified (Sun et al., 2024). Recent studies have highlighted loneliness as an increasingly concerning issue among contemporary university students (Fletcher et al., 2025; Lv et al., 2025; Wu et al., 2024). This vulnerability to loneliness may further complicate students’ adjustment to bereavement. As a prevalent outcome of bereavement, loneliness poses a serious risk to the psychological and physical well-being of the bereaved (Vedder et al., 2022), impairing daily functioning and increasing the risk of suicidal ideation (Hawkley et al., 2010; Leigh-Hunt et al., 2017). Importantly, loneliness has been shown to be significantly associated with both depression and prolonged grief symptoms in bereaved populations (Burger et al., 2020; Eisma & Buyukcan-Tetik, 2025; Lee, 2019). Loneliness has been regarded as a gateway symptom following bereavement, potentially triggering subsequent mental health issues such as depression (Fried et al., 2015). Network analysis has further revealed that loneliness functions as a bridge symptom between depression and prolonged grief symptoms (Eisma & Buyukcan-Tetik, 2025; Robinaugh et al., 2014). In conclusion, PGD, depression, and loneliness may frequently co-occur following bereavement, and the interactive dynamics among their symptoms warrant further empirical investigation.
Latent class analysis (LCA) is a person-centered statistical approach that categorizes individuals into distinct, non-overlapping subgroups by analyzing their responses to a series of categorical indicators (Lanza et al., 2007). By identifying subgroups with distinct symptom patterns, LCA can suggest whether different predictors are associated with different comorbidities. Such associations may then indicate that each subgroup would benefit from tailored interventions. (Boelen et al., 2016). Several studies have classified individuals into distinct subgroups based on the co-occurrence of PGD and depressive symptoms. For instance, Maccallum and Bryant classified bereaved individuals into three subgroups: a combined PGD and depression group, a depression-only group, and a low-symptom group (Maccallum & Bryant, 2018). Parallel findings were found among a non-Western sample of bereaved young and middle-aged adults: a resilient class (low PGD and depression symptoms), a PGD class (primarily PGD symptoms), and a combined PGD and depression class (high levels of both symptoms) (Kokou-Kpolou et al., 2021). Beyond depression, some studies have also extended the analysis to include posttraumatic stress symptoms (PTSD). Three distinct subgroups were also identified among bereaved adults within the first six months (Boelen & Lenferink, 2020) and in suicide-bereaved populations (Boelen & Lenferink, 2020; Grafiadeli et al., 2022). However, the symptom patterns involving PGD, depression, and loneliness have not yet been systematically examined among bereaved college students, especially in non-Western contexts such as China.
Previous LCA studies on bereaved people have predominantly focused on adult samples with an average age between 35 and 56 years (Heeke et al., 2023). However, bereavement experiences among university students have received scant research attention. University students aged 18 to 24 are in a critical developmental stage of emerging adulthood (Jiang et al., 2025). During this stage, they have to balance academic performance, occupational development, identity exploration, and increasing responsibilities, which may amplify the challenges brought on by bereavement (Glickman, 2020). This gap necessitates further research to clarify the manifestation and severity of bereavement in this population (Balk et al., 2010). For bereaved college students, the loss of a loved one may not only lead to academic crises (Balk et al., 2010) but also trigger emotional, physical, and interpersonal distress (Varga, 2015). Bereavement may activate the attachment systems of bereaved students (Shear & Shair, 2005), increasing the need for family support (Cousins et al., 2017). In the Chinese cultural context, university students typically reside on campus (Huang et al., 2024). Therefore, due to geographic separation from family and childhood friends, many students become disconnected from their original support networks and struggle to access the adequate support they need (Arnett, 2000). Moreover, the lack of understanding from peers at school may further intensify their feelings of isolation (Servaty-Seib & Taub, 2010). Notably, in the post-pandemic era, university students have experienced prolonged social isolation and increased reliance on social media. Even after daily life has returned to normal, this excessive online usage may have weakened opportunities for high-quality interpersonal connection, further exacerbating feelings of loneliness (Wu et al., 2024). At the same time, some students have begun confiding their thoughts and feelings to artificial intelligence chat-bots as a means of alleviating psychological distress (Kim et al., 2025; Lai et al., 2025). Taken together, investigating the psychological and behavioral patterns of bereaved university students against this specific temporal and cultural background holds significant research value. Furthermore, although bereaved college students express a strong desire for support soon after the loss, they may encounter obstacles when seeking help (Tureluren et al., 2022). Financial difficulties and insufficient support have been identified as practical challenges for bereaved university students, suggesting the need for more accessible bereavement assistance (Fletcher et al., 2025; Terry, 2024). In the Chinese context, these challenges may be further complicated by limited public knowledge and insufficiently established norms regarding bereavement support for caregivers (Lu & Liu, 2025). These persistent challenges underscore the necessity for greater attention to this under-served population and for the development of tailored support mechanisms.
In addition, adjustment processes and bereavement outcomes may differ across cultural contexts, particularly between Eastern and Western societies. Influenced by traditional philosophies (e.g., Confucian filial piety and Daoist thought), Chinese individuals are generally less inclined to process grief through social sharing (Chow et al., 2007). Instead, they tend to suppress feelings of grief, deny the reality of death (Yuan et al., 2024), and exhibit higher levels of deliberate grief avoidance (Bonanno et al., 2005). One longitudinal study revealed a contrasting pattern: bereaved-Chinese report more intense grief and poorer health perceptions in the early stage of bereavement, but demonstrate better psychological adaptation and health outcomes than Americans 18 months after the loss (Bonanno et al., 2005). Taken together, distinctive Chinese bereavement experiences relative to Western contexts underscore the need for expanded research within this cultural setting.
Therefore, the current study, using a longitudinal design and LCA method, aimed to identify subgroups among bereaved Chinese college students based on symptoms of grief, depression, and loneliness. While prior research has largely focused on Western bereaved adults (Heeke et al., 2023), examining symptom patterns in Chinese college students may provide critical culturally relevant insights into bereavement outcomes during emerging adulthood. Moreover, identifying subgroups with homogeneous symptom profiles could inform the development of targeted, population-specific interventions. Additionally, while loneliness and depression are commonly viewed as accompanying conditions with PGD (Eckholdt et al., 2018; Robinaugh et al., 2014; World Health Organization, 2022a), it remains unclear whether these symptoms consistently co-occur as an inseparable pattern or can present independently. Another aim was to examine differences in demographic variables and loss-related characteristics across the identified subgroups, which would provide guidance on which populations should be prioritized for support following bereavement. Finally, this study investigated whether subgroup membership predicts functional impairment six months later. Establishing such predictive utility would support the importance of early identification for students.
Method
Participants and Procedure
The current study was a two-wave longitudinal survey with an interval of 6 months. Participants were recruited online and were eligible if they met the following two criteria: (1) the time since the death of a loved one was less than 36 months; (2) they were currently enrolled in higher education (i.e., undergraduate or graduate programs) and aged 18 years or above. The 36-month cutoff was selected to focus on students who were still relatively close to the loss and potentially undergoing grief adaptation (Nielsen et al., 2019), and is consistent with prior bereavement studies using a similar within-three-years criterion (Boelen & Eisma, 2015; Huang et al., 2025). The duration of the survey was approximately 25 minutes. Prior to participation, individuals were informed of the benefits they would receive: 30 yuan for completing the first wave (Time 1) and 40 yuan for completing the second wave (Time 2). Data were collected via the Qualtrics platform, and electronic informed consent was obtained before starting the survey.
At Time 1, a total of 402 students were enrolled in the research, and 37 were excluded (30 for insufficient response effort, 6 for exceeding loss time, and 1 was excluded owing to missing data). Ultimately, 365 valid questionnaires were collected. Time 1 participants (N = 365) included 187 females (51.2%) and 178 males (48.8%), with a mean age of 21.34 years (SD = 1.71). The majority were college/university-educated (92.0%) and reported a close relationship with the deceased (96.2%). Over half of the population were urban residents (51.8%). The time since loss averaged 10.87 months (SD = 7.37), and their self-rated physical health averaged 3.95 (SD = 0.74) on a 5-point scale (1 = very poor, 5 = very good). Deaths resulted from acute diseases (43.3%), chronic diseases (40.8%), or accidents (15.9%). The deceased were respectively the bereaved individuals’ parents (9.3%), grandparents (61.1%), other family members (17.8%), or other relationships (11.8%, such as intimate friends). Only 32.6% anticipated the death, and 65.2% reported having no opportunity to say goodbye beforehand.
At Time 2, a total of 159 valid questionnaires were obtained, comprising 54.7% females (n = 87) and 45.3% males (n = 72), with an average age of 22.03 years (SD = 1.92). College/university education was reported by 73.6%, 59.1% lived in urban areas, and 66.0% had experienced grandparent loss. The majority of participants (91.2%) described their relationship to the deceased as close. The mean physical health score was 3.82 (SD = 0.78). Regarding cause of death, acute illnesses (45.9%) and chronic conditions (42.1%) were most common, followed by accidents (12.0%). The deceased included the participants’ parents (10.1%), grandparents (66.0%), other family members (17.6%), and other relationships (6.3%). While 33.3% of participants had anticipated the death, 66.7% reported that they were unable to bid farewell prior to it.
Sociodemographic Information for the Total Sample and For Each Latent Class at Time 1
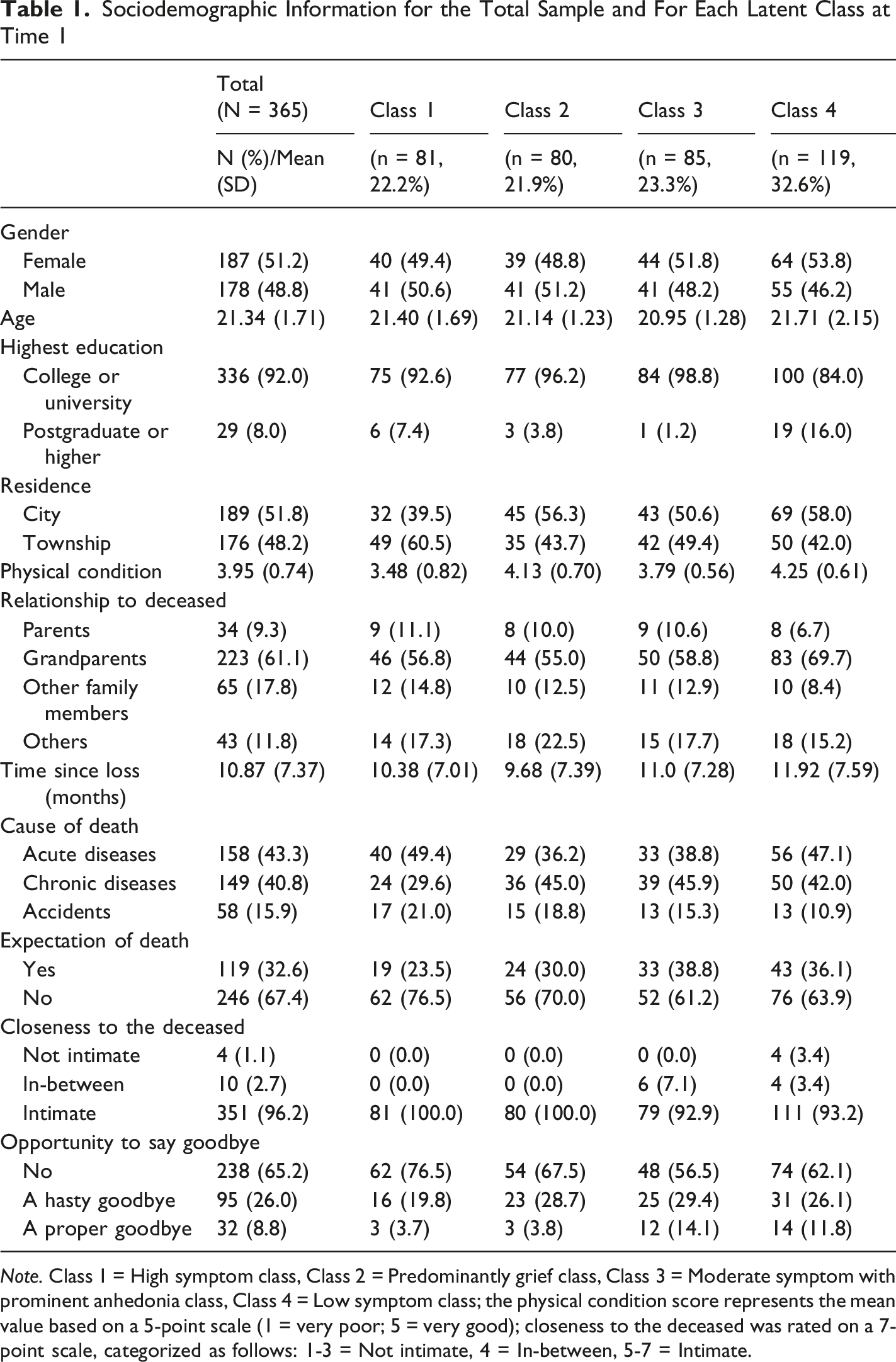
Note. Class 1 = High symptom class, Class 2 = Predominantly grief class, Class 3 = Moderate symptom with prominent anhedonia class, Class 4 = Low symptom class; the physical condition score represents the mean value based on a 5-point scale (1 = very poor; 5 = very good); closeness to the deceased was rated on a 7-point scale, categorized as follows: 1-3 = Not intimate, 4 = In-between, 5-7 = Intimate.
Measures
Self-Developed Demographic Information Questionnaire
This study collected participants’ basic information using a self-developed demographic information questionnaire, including gender, age, education level, residence, physical condition, relationship to the deceased, time since death, cause of death, expectation of the death, closeness to the deceased, and the opportunity to say goodbye to the deceased.
Prolonged Grief Scale–Revised (PG-13-R)
Prolonged Grief Scale-Revised (PG-13-R) (Prigerson et al., 2021) is a revision of the PG-13 scale (Prigerson et al., 2009). It contains 13 items, of which 10 symptom items correspond to the PGD symptoms in the DSM-5-TR criteria (yearning, preoccupation, identity disruption, disbelief, avoidance, intense emotional pain, difficulty with reintegration, emotional numbness, feeling that life is meaningless, and intense loneliness) (American Psychiatric Association, 2022). These items are rated on a 5-point Likert scale from “1 = not at all” to “5 = overwhelmingly”, with higher scores indicating greater severity of grief symptoms. A total score of 30 or above is considered indicative of probable PGD (Prigerson et al., 2021). In the present study, Cronbach’s alpha for the scale was α = 0.90 at Time 1 and α = 0.91 at Time 2.
Patient Health Questionnaire-9 (PHQ-9)
Patient Health Questionnaire-9 (PHQ-9) is used to assess the severity of depression during the past two weeks (Kroenke et al., 2001). It consists of 9 items, each scored from 0 (not at all) to 3 (nearly every day), with a total score ranging from 0 to 27. Total scores of 5, 10, 15, and 20 on this scale represent the thresholds of mild, moderate, moderately severe, and severe depression, respectively. The Cronbach’s alpha of the PHQ-9 in this study was α = 0.89 at Time 1 and α = 0.90 at Time 2.
UCLA-Loneliness Scale
The UCLA-Loneliness Scale is a widely recognized instrument for measuring loneliness (Russell, 1996), with various versions differing in the number of items (Vedder et al., 2021). The original version comprises 20 items (Russell et al., 1980), while the 6-item version was used in this study (Xu et al., 2018). Each item is scored from 1 (never) to 4 (often), with total scores ranging from 6 to 24. Higher scores indicate greater levels of loneliness. The Cronbach’s alpha of the UCLA scale in the present study was α = 0.88 at Time 1 and α = 0.93 at Time 2.
Work and Social Adjustment Scale (WSAS)
The Work and Social Adjustment Scale (WSAS) is used to assess functional impairment due to bereavement and grief (Mundt et al., 2002). It consists of 5 dimensions (work, household management, social leisure, private leisure, and relationships), and each is scored from 0 (no impairment at all) to 8 (very severe impairment). Total scores above 20 appear to indicate a moderately severe or worse condition of functional impairment (Mundt et al., 2002). In this study, Cronbach’s alpha for the scale at two time points was 0.91 and 0.94, respectively.
Data Analysis
Initially, dichotomous indicators were generated for each symptom item. Specifically, for PGD symptoms, a rating of 1 (not at all), 2 (slightly), or 3 (somewhat) indicated absence, while a rating of 4 (quite a bit) or 5 (overwhelmingly) was coded as presence. For depression, a rating of 0 (not at all) or 1 (several days) meant absence, and a rating of 2 (more than half the days) or 3 (nearly every day) meant presence. For loneliness, a rating of 1 (never) or 2 (rarely) was considered absence, while a rating of 3 (sometimes) or 4 (often) signified presence.
LCA was conducted among participants at Time 1 (N = 365). Several fit indices were computed: (1) Akaike Information Criterion (AIC), the Bayesian Information Criterion (BIC) and the sample size adjusted Bayesian Information Criterion (ssBIC), with lower values indicating better fit; (2) entropy, with a value ≥0.80 being acceptable; (3) Lo-Mendell-Rubin (LMR) test and the bootstrap likelihood ratio test (BLRT), where a significant p value indicates that the k class model is better than the (k – 1) class model (Nylund et al., 2007). Regarding conditional probabilities, if the indicator value exceeded 0.60, it was regarded as a high likelihood that the symptom was experienced by the members of that class. A value ranging from 0.15 to 0.59 signified a moderate probability, while a value below 0.15 indicated a low probability of endorsement (Burstein et al., 2012). In addition to statistical indicators, parsimony and interpretability were also considered in determining the optimal number of latent classes (Boelen et al., 2019). Once the optimal model was selected, associations between class membership and demographic and loss-related variables were explored using the robust three-step method, also called the ML three-step approach. The three-step method takes the classification error into account. It uses the method of maximum likelihood estimation and yields a logistic regression model estimation (Asparouhov & Muthén, 2014; Vermunt, 2010).
To examine whether latent class membership at Time 1 predicted functional impairment at Time 2 (n = 159), we applied the BCH method. The BCH method uses weighted ANOVA while accounting for classification error. Statistical differences across classes were evaluated using a chi-square test difference analysis derived from the BCH procedure (Bolck et al., 2017).
All analyses in the current study were conducted using Mplus v.8.
Results
Latent Class Analysis
Goodness-of-Fit Statistics For One-to Five-Class Models
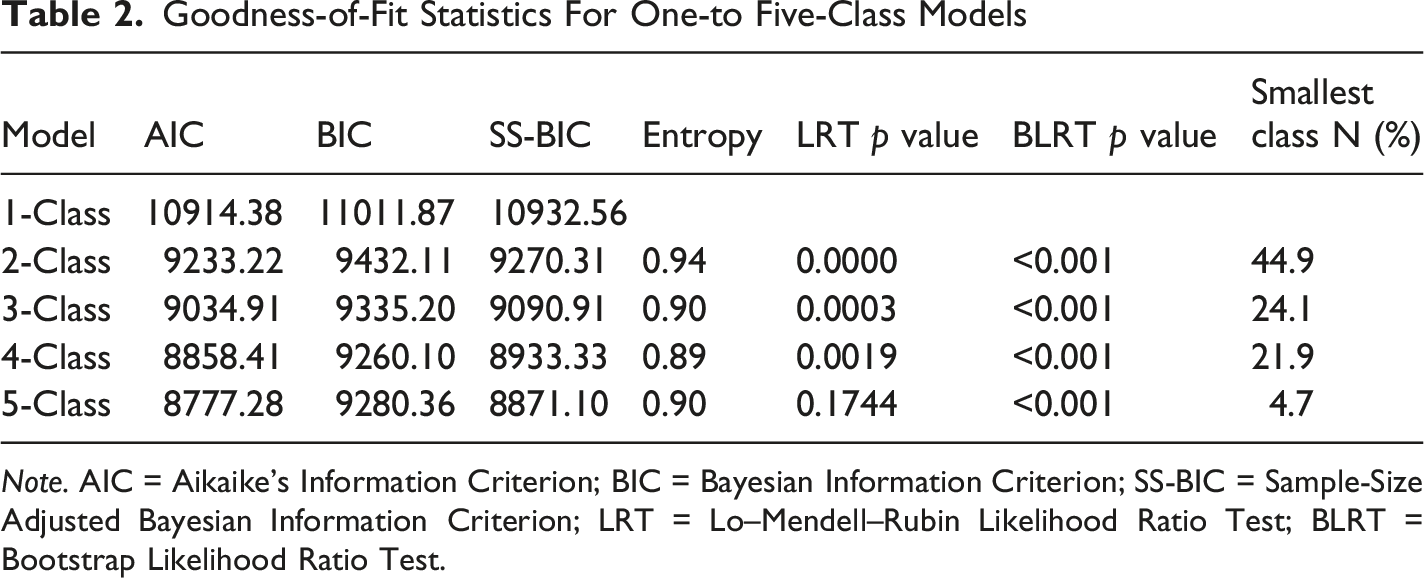
Note. AIC = Aikaike’s Information Criterion; BIC = Bayesian Information Criterion; SS-BIC = Sample-Size Adjusted Bayesian Information Criterion; LRT = Lo–Mendell–Rubin Likelihood Ratio Test; BLRT = Bootstrap Likelihood Ratio Test.
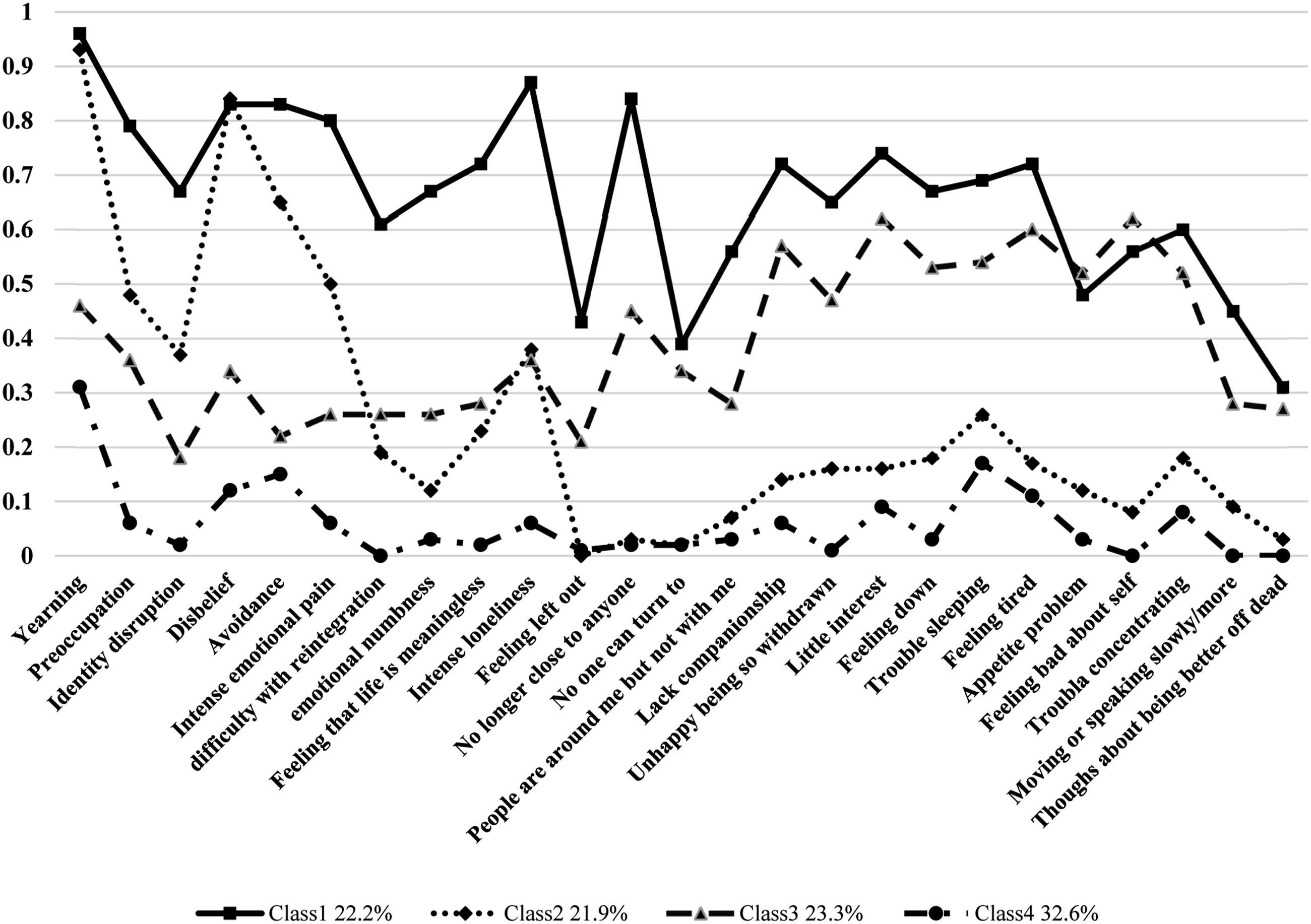
Probability estimates for the four-class solution
Probability of Symptoms of PGD, Depression and Loneliness Endorsement for the Overall Sample and Each Class (N = 365)
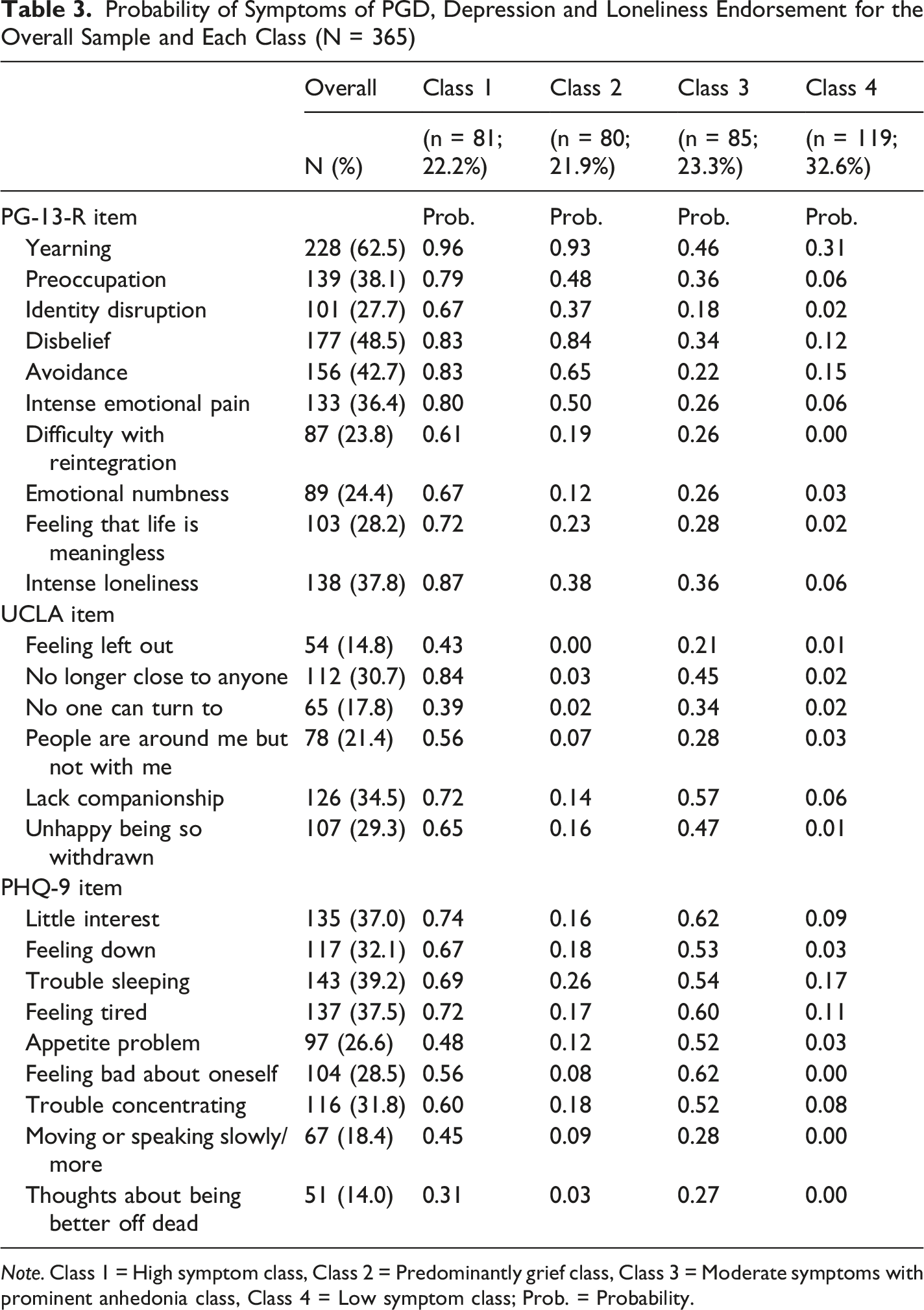
Note. Class 1 = High symptom class, Class 2 = Predominantly grief class, Class 3 = Moderate symptoms with prominent anhedonia class, Class 4 = Low symptom class; Prob. = Probability.
Class 1 consists of participants with a high probability of endorsement for most symptoms across the three domains, except for moderate probabilities of three loneliness symptoms (“I feel left out”, “There is no one I can turn to” and “People are around me but not with me”) and four symptoms in depression (“Appetite problem”, “Thoughts about being better off dead”, “Feeling bad about self”and “Moving or speaking slowly/more”). This class was accordingly labeled as “high symptom class” (22.2%). Class 2 was named as “predominantly grief class” (21.9%), which exhibited high or moderate probabilities for grief symptoms and slightly moderate or low probabilities for symptoms of loneliness and depression. Class 3 showed moderate probabilities across most symptoms, with high probabilities for three depression symptoms (“Little interest”, “Feeling tired”, and “Feeling bad about self”). Thus, this class was labeled as “moderate symptom with prominent anhedonia class” (23.3%). Class 4 was characterized by generally low probabilities for most symptoms, except for moderate probabilities for two grief symptoms (“yearning” and “avoidance”) and one depression symptom (“Trouble sleeping”). Therefore, this class was labeled as “low symptom class” (32.6%).
Associations of Class Membership With Demographic and Loss-Related Variables
Associations of Class Membership With Demographic and Loss-Related Variables
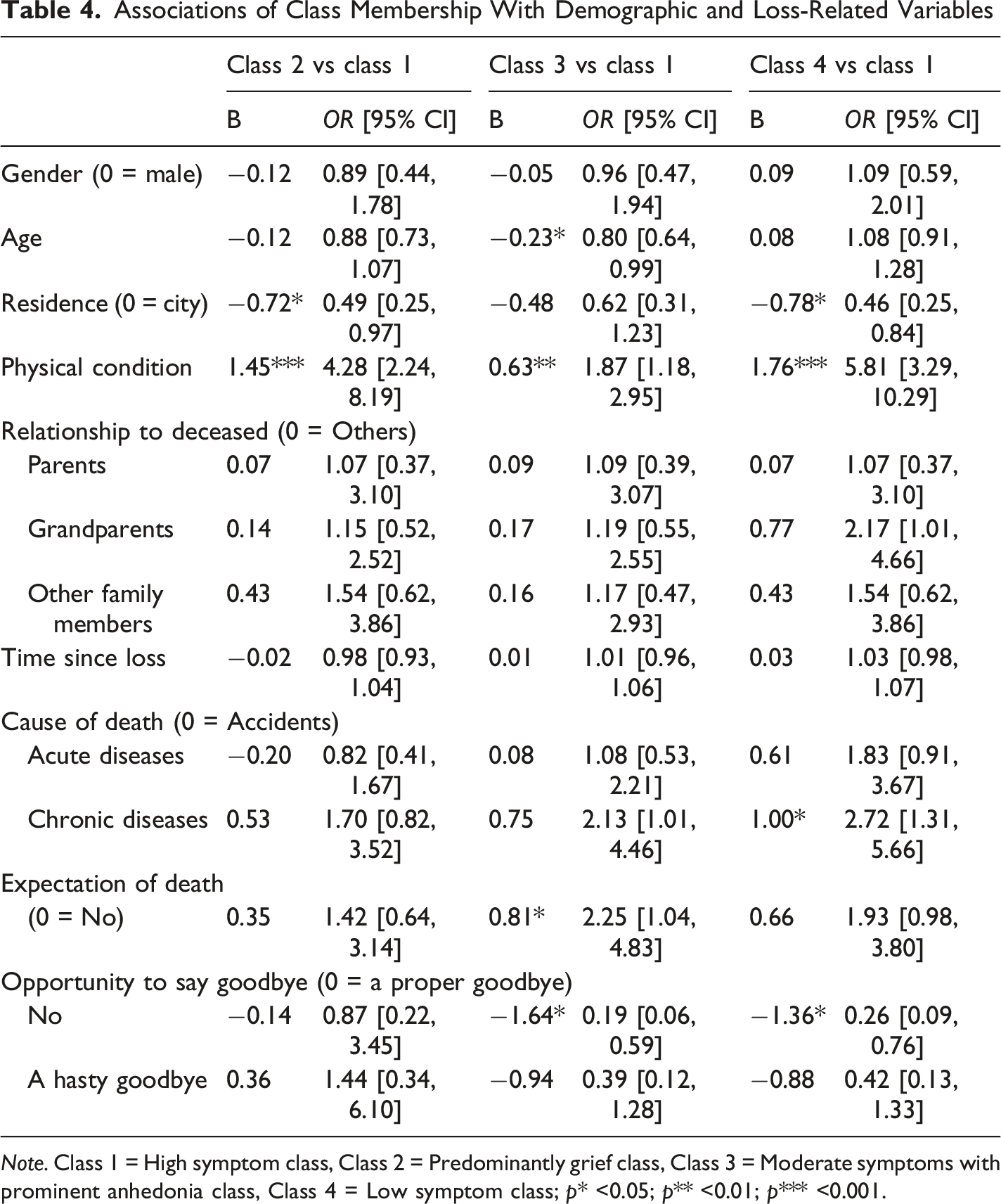
Note. Class 1 = High symptom class, Class 2 = Predominantly grief class, Class 3 = Moderate symptoms with prominent anhedonia class, Class 4 = Low symptom class; p* <0.05; p** <0.01; p*** <0.001.
Predictive Effect of Class Membership on Functional Impairment at Time 2
Differences in Functional Impairment at Time 2 Between the Classes
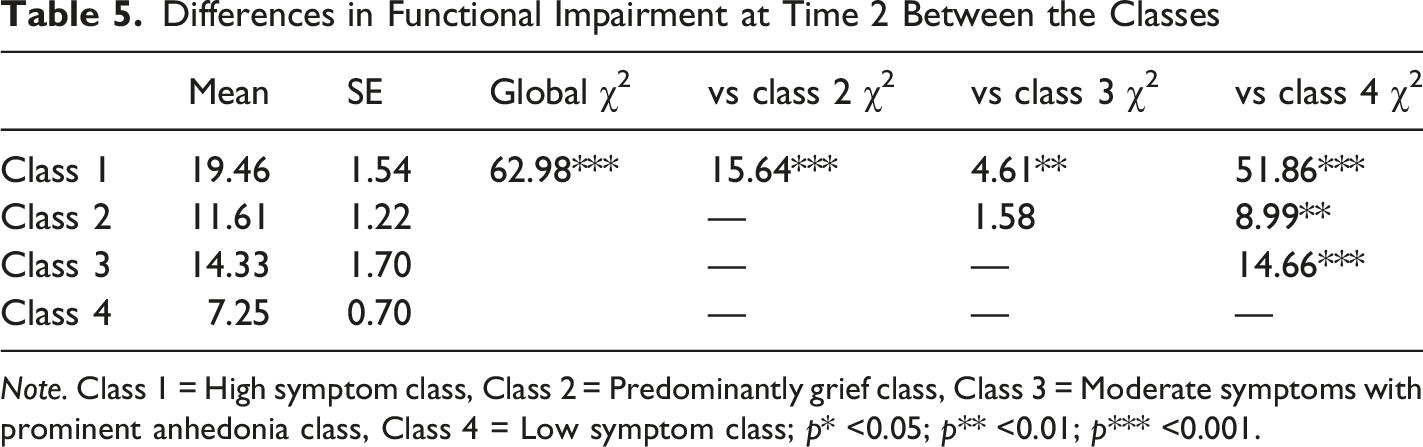
Note. Class 1 = High symptom class, Class 2 = Predominantly grief class, Class 3 = Moderate symptoms with prominent anhedonia class, Class 4 = Low symptom class; p* <0.05; p** <0.01; p*** <0.001.
Discussion
This study investigated the co-occurring symptom patterns of grief symptoms, depression, and loneliness among Chinese college students following bereavement. Four distinct classes were identified: a high symptom class, a predominantly grief class, a moderate symptom with prominent anhedonia class, and a low symptom class. Bereaved individuals who were older, resided rurally, reported poorer physical health, experienced an unexpected death, or were unable to say goodbye were more likely to be classified into the high symptom class. Conversely, bereavement due to chronic disease was associated with a lower likelihood of being in the high symptom group. Furthermore, class membership significantly predicted functional impairment six months later, providing support for the prognostic utility of the identified subgroups.
Four latent subgroups emerging from the analysis revealed distinct patterns of symptom co-occurrence. In addition to the high symptom class exhibiting grief symptoms, depression, and loneliness simultaneously, there existed a unique subgroup primarily characterized by grief symptoms. This finding suggested that depression and loneliness may not necessarily occur in conjunction with grief reactions consistently. The four-class pattern shares some similarities with previous studies investigating PGD, depression, and PTSD. For instance, three classes remained largely consistent: a high-symptom class (combined PGD/depression class in previous study), a predominant PGD symptom class, and a low-symptom class (often labeled the resilient class in previous study) (Boelen & Lenferink, 2020; Heeke et al., 2017; Maccallum & Bryant, 2018).
However, our findings diverged from prior research in two aspects. First, compared with the three-class classification, our study identified an additional group—moderate symptom with prominent anhedonia class (Class 3). When compared to the same four-subgroup classification, our Class 3 aligns with their “predominantly PTSD class” in structure—both exhibit one highly probable symptom (depression) alongside other symptoms with high probabilities (Nickerson et al., 2014; Tay et al., 2019). However, Class 3 in the current study only included three symptoms with slightly elevated probabilities.
Additionally, the proportion of symptomatic individuals in our sample (67.4%) was lower than in previous studies, which reported proportions ranging from 74.7% to 84% (Boelen et al., 2016; Grafiadeli et al., 2022; Kokou-Kpolou et al., 2021). This discrepancy might be related to differences in sample characteristics. In our study, a larger proportion of losses were due to non-violent death, such as illness, rather than accidents. Additionally, the deceased were predominantly grandparents—losses that are often perceived as more normative or expected. Both factors potentially facilitated better psychological preparedness among bereaved individuals (Miyabayashi & Yasuda, 2007).
Another potential explanation lies in Chinese cultural practices. In this collectivist society, individual needs are often secondary to maintaining group harmony (Tsai et al., 2006). As a result, people may feel compelled to control their emotions and suppress overt expressions of their grief (Yuan et al., 2024). This tendency is reinforced at home, where talking about death and grief is often taboo (Cheng et al., 2019; Hu et al., 2025). For Chinese university students, this means even fewer opportunities to process their loss. Within Chinese culture, mourning rituals serve as a substitute for direct verbal or emotional disclosure (Woodward et al., 2023). These rituals are considered the most important way to show care and respect for the deceased (Qin & Xia, 2015). This cultural inclination, however, can lead the bereaved to mask their intense yearning and painful emotions for the deceased. Consequently, they may report lower levels of grief and fewer symptoms of PGD.
The second aim of this study was to explore associations between class membership and demographic and loss-related variables. Findings revealed that older bereaved university students were more likely to be classified into the high symptom class. This is potentially due to dual pressures of demanding academics and career preparation faced by upper-year students (Mu et al., 2022; Wu et al., 2020), complicating bereavement adaptation. Students residing in rural areas were also more likely to belong to the high symptom class. Adequate mental health services and grief interventions are known to facilitate post-loss adjustment (Rotzal, 2024). However, rural regions typically have more limited healthcare and social services compared to urban counterparts (Downing & Jack, 2012; Hansford et al., 2023), hindering recovery for the bereaved. Physical condition emerged as another important factor associated with class membership. Specifically, bereaved individuals in worse physical condition demonstrated a greater likelihood of being categorized into the symptomatic subgroup compared to those in good physical health. Previous studies have indicated that physical deterioration is a consequence of bereavement (Stroebe et al., 2007) and demonstrated that bereavement-related challenges significantly predict lower physical quality of life (Trevino et al., 2018). The current findings extend previous work by suggesting that physical condition not only reflects the consequences of bereavement but also actively shapes its symptom patterns. Additionally, high-symptom conditions were less common in those whose loved ones passed away from chronic illnesses. This aligned with prior research indicating that bereavement following deaths from chronic illnesses is associated with better adaptation and reduced adverse impacts (Sanders, 1983; Shah et al., 2013). Furthermore, unexpected death was associated with a higher likelihood of belonging to the high symptom class, which is consistent with findings from both Chinese (Liang et al., 2024) and European samples (Treml et al., 2021). Lastly, a lack of opportunity to say goodbye to the deceased also increased the likelihood of high symptomatology, compared to the low symptom class. Pre-death communication, particularly farewells, benefits the bereaved by reducing regrets, supporting adaptation to bereavement (Worden, 2009). The other reason might be that the absence of a goodbye may lead to an ambiguous loss, making it difficult for the mourning process to proceed normally (Hernández-Fernández & Meneses-Falcón, 2022).
The third aim of this study was to examine the predictive effect of classification at Time 1 on functional impairment at Time 2. The results revealed that the functional impairment levels across different classes at Time 2 were ranked from highest to lowest as follows: high symptom class, moderate symptom with prominent anhedonia class, predominantly grief class, and low symptom class. This pattern is consistent with prior research showing that individuals in the high grief symptom class reported the most severe functional impairment at Time 2, followed by the separation distress class with relatively fewer symptoms, and the lowest in the low symptom class (Boelen et al., 2019). These findings indicated that bereaved individuals with higher initial symptom severity continue to exhibit elevated functional impairment six months later. However, Boelen’s study primarily focused on PGD symptoms. Our study further demonstrated that the co-occurrence of multiple symptoms appeared to result in more severe functional impairment compared to isolated grief symptoms. Previous studies demonstrated functional impairment’s association with most disorders, particularly the strongest independent link with depression (Hussain et al., 2011; Kristensen et al., 2009). This may explain the heightened impairment observed in multisymptomatic groups. The findings of this study emphasized the importance of identifying high-risk individuals for targeted interventions to mitigate functional impairment after bereavement.
Several limitations of this study should be mentioned. Firstly, the use of convenience sampling constrains the generalizability of conclusions. Secondly, the limited sample size restricted the exploration of more meaningful associations between demographic and loss-related variables and classes. For example, more than half of the deceased were grandparents, which may constrain the applicability of findings to populations with different kinship relationships to the deceased. Thirdly, the reliance on self-report measures for assessing grief symptoms, depression, and loneliness meant the findings reflect co-occurring symptoms rather than clinically verified comorbid disorders. Finally, a significant dropout rate at Time 2 in the longitudinal design may affect the external validity of the research outcomes.
Despite these considerations, the results of this study indicated that bereaved Chinese college students can be meaningfully classified into four classes based on their symptoms of grief, depression, and loneliness. In addition, the observed associations between demographic variables, loss-related variables and class membership offer valuable clinical implications. For example, healthcare professionals may encourage family members to maintain open communication with terminally ill patients, especially to have an appropriate farewell, which will be beneficial for bereavement recovery. Moreover, the classification at Time 1 can predict the functional impairment at Time 2, which reminded clinicians that they could implement early interventions by identifying at-risk populations in advance, thereby reducing the risk of long-term functional disruptions among bereaved students.
Footnotes
Acknowledgements
The authors acknowledge all the participants who participated in this study.
Ethical Consideration
The present study was approved by the Ethics Committee of Soochow University (No. SUDA20231213H03).
Consent to Participate
Written informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Social Science Fund of China [grant numbers: 25CSH033]. The funding agency had no role in the study design, data collection, analysis, or interpretation, or manuscript preparation or submission.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data used in the current study are available from the corresponding author upon reasonable request.