
Abstract
How a scholarly community organizes knowledge about the deaths of marginalized populations is itself a question for death studies. This bibliometric review maps the global literature on end-of-life and palliative care for adults with intellectual and developmental disabilities, drawing on 919 English-language articles from 1990 to 2025. Only 5.5% of papers appeared in palliative care journals; the evidence base has accumulated in disability-specialist venues largely invisible to scholars and clinicians of dying. Topic modeling on 423 core documents shows staff training has dominated this scholarship for three decades, while the perspectives of dying people themselves remain peripheral, a pattern that speaks to long-running concerns about awareness contexts and the social organization of dying. Citation analysis reveals a field whose intellectual architecture rests on a single author. The literature mirrors the marginalization of the population it studies; this review offers death scholarship a structural map and an agenda for diversification.
Keywords
Introduction
How a society and its scholarly disciplines organize knowledge about the deaths of marginalized populations is a question with a long history in death studies (Glaser & Strauss, 1965; Walter, 1994). Bibliometric methods, defined broadly as quantitative approaches to the analysis of scientific publications using bibliographic data (Broadus, 1987), are increasingly being deployed to interrogate the structural conditions under which professional knowledge about dying is produced, accumulated, and transmitted. This study applies these methods to one such literature: the global research on end-of-life (EOL) and palliative care for adults with intellectual and developmental disabilities (IDD), a population whose dying has historically been rendered peripheral both in clinical practice and in scholarly accounts of death.
Equitable access to EOL and palliative care (World Health Organization, 2020) remains elusive for adults with IDD, despite a well-documented and growing burden of life-limiting illness in this population (Tuffrey-Wijne et al., 2007; Coppus, 2013). As people with IDD live longer than at any prior point in recorded history, with life expectancy now approaching that of the general population for those without severe comorbidities (Lauer & McCallion, 2015), the prevalence of dementia, cancer, and cardiovascular disease in this group has increased markedly (Heslop et al., 2014; Lauer & McCallion, 2015). IDD, characterized by significant limitations in intellectual functioning and adaptive behavior originating during the developmental period (American Association on Intellectual and Developmental Disabilities, 2021), affects an estimated 1–3% of the global population. The convergence of increasing longevity and high burden of life-limiting illness generates an urgent clinical and policy imperative for evidence-based EOL and palliative care tailored to the specific communication, cognitive, and support needs of this population.
Despite this imperative, adults with IDD have historically been excluded from mainstream palliative care research and clinical practice (Ryan et al., 2011; Tuffrey-Wijne & McEnhill, 2008). Barriers to equitable EOL care operate at multiple levels: clinician unfamiliarity with IDD-specific communication needs, diagnostic overshadowing, difficulties with advance care planning, inadequate training of both specialist IDD and generalist palliative care staff, and systemic failures in the transition between IDD and palliative care services (Adam et al., 2020; Bekkema et al., 2014). These barriers have attracted increasing scholarly attention since the 1990s, producing an expanding body of literature spanning nursing, social work, medicine, ethics, and disability studies. Qualitative studies of staff experiences have mapped the barriers to good EOL care for people with IDD in residential and community services (Todd, 2013; Wiese et al., 2012). However, the structural characteristics of the broader scholarship that has accumulated around it, including its geographic distribution, thematic organization, citation dynamics, and relationship to mainstream palliative care and death studies, have never been systematically examined.
Such an examination matters for death scholarship in two specific ways. First, the dissemination architecture of a literature reveals which professional and scholarly communities are positioned to act on its findings; the absence of this evidence base from the venues where palliative care clinicians read is therefore a substantive feature of how the dying of cognitively marginalized adults is constructed as a clinical problem. Second, the thematic structure of a literature reveals whose voices are organized as authoritative within it; when a body of scholarship about dying is dominated by the perspectives of those who care for the dying rather than by the dying themselves, that pattern speaks to long-running death studies concerns about awareness contexts and the social organization of dying (Glaser & Strauss, 1965).
Bibliometric reviews have characterized the intellectual structure of the broader developmental disabilities literature (Carollo et al., 2021; Cavallaro et al., 2025; Fong et al., 2023; Lim et al., 2023) and mapped global palliative care research (Abu-Odah et al., 2022), but no such analysis has been conducted at their intersection. The present study addresses this gap by conducting the first comprehensive bibliometric review of the global literature on EOL and palliative care for adults with IDD published between 1990 and 2025. Specifically, the study aims to: (1) characterize publication trends, geographic distribution, and journal dissemination patterns; (2) identify the thematic structure of the field and examine how research priorities have shifted over time; (3) map the citation architecture of the field, identify its most structurally influential papers, and characterize open access trends; and (4) situate this evidence base within death studies scholarship on how professional knowledge accumulates around marginalized dying populations. Together, these analyses provide the first empirical mapping of this field and offer an evidence base for future research prioritization, funding decisions, and the broader project of making visible whose deaths matter to scholarly and professional communities.
Methods
Search Strategy and Data Sources
Bibliographic data were retrieved from OpenAlex, an open-access scholarly database indexing more than 250 million works across all disciplines (Priem et al., 2022). OpenAlex was selected on two grounds. First, as a fully open database with a public application programming interface requiring no institutional subscription, it enables complete methodological transparency: the search queries, filters, and corpus used in this study can be independently verified and replicated by any researcher without licensing barriers, addressing a well-recognized reproducibility constraint in bibliometric research (Culbert et al., 2025). Second, OpenAlex provides broader coverage of open access journals and of social science and health-related disciplines than either Scopus or Web of Science (Maddi et al., 2025), making it particularly well suited to a literature that spans nursing, social work, disability studies, and medicine across multiple geographic contexts. Reference coverage has been shown to be comparable to both proprietary databases for recent journal article corpora (Céspedes et al., 2025; Culbert et al., 2025). Reporting follows the BIBLIO bibliometric reporting checklist. A PRISMA-style flowchart is used for visual clarity in presenting the screening process.
Two thematic blocks were constructed to capture the intersection of interest. The EOL and palliative care block comprised terms including: palliative care, end-of-life care, hospice, terminal care, advance care planning, do not resuscitate, goals of care, life-limiting illness, treatment withdrawal, and good death. The IDD block comprised eight sub-queries covering: intellectual disability, developmental disability, learning disability, Down syndrome, Fragile X syndrome, autism spectrum disorder, mental retardation, intellectual handicap, and mental handicap (included as historical search terms to capture literature predating contemporary terminology). Autism spectrum disorder was included as an IDD sub-query because of its frequent co-occurrence with intellectual disability in the clinical and research literature (American Association on Intellectual and Developmental Disabilities, 2021). Papers addressing autism spectrum disorder without confirmed intellectual disability comorbidity were not excluded at the filtering stage, as title and abstract screening cannot reliably distinguish this at scale. Inspection of the corpus identified 52 papers with autism-related terms in the title, of which approximately 50 did not include co-occurring IDD terminology at the title level, representing 5.4% of the final corpus. Of these 50 papers, 6 met Tier 1 and 44 met Tier 2 criteria, and all were retained in the full corpus; 23 entered the 423-document topic-modeling core (3 of the 6 Tier 1 and 20 of the 44 Tier 2 papers), while the remaining 27 did not meet the core’s relevance-score and minimum-token thresholds. This represents a boundary limitation, with the effect on the topic structure examined in the Limitations section. Each IDD sub-query was paired with the full EOL block using a Boolean AND operator, yielding eight separate queries that were subsequently merged. The search was restricted to English-language journal articles and was conducted on March 1, 2026, using the pyalex Python library (van Eck, 2023). Three articles with a publication year of 2026 were retrieved and retained, as they had been indexed by OpenAlex prior to the search date and met all eligibility criteria; these are represented in the 2025 bar of Figure 2.
Eligibility Criteria and Relevance Filtering
Records were included if they (a) reported original research, a review, or a commentary on EOL or palliative care for adults with IDD, (b) were published between 1990 and 2025, and (c) were written in English. No restriction was placed on study design or disciplinary origin. Records were excluded if they concerned exclusively pediatric populations, animal subjects, or conditions outside the IDD spectrum.
A three-tier relevance filtering strategy was applied to all retrieved records. Tier 1 required both IDD and EOL terminology to appear in the title, representing the highest dual-relevance confidence. Tier 2 required IDD terminology in the title and EOL terminology in the abstract, or vice versa. Tier 3 required both IDD and EOL terminology to appear in the abstract only. Records meeting none of these criteria were excluded. Records were subsequently deduplicated by OpenAlex identifier and then by digital object identifier. A numerical relevance score was assigned to each record using a weighted term-frequency scheme: title matches were weighted 3 points per match; abstract matches were weighted 1 point per match, applied separately to core IDD and EOL terminology patterns. Tier 1 and Tier 2 records with a relevance score below 4 were excluded from the topic modeling core subset as likely tangential matches, reducing the Tier 1 and Tier 2 pool from 573 to 508 documents prior to preprocessing. The search and eligibility process is summarized in Figure 1. PRISMA flowchart illustrating the systematic search and eligibility process. Records were identified via the OpenAlex database (search date: March 1, 2026), screened using a three-tier title and abstract matching strategy based on co-occurrence of IDD and EOL terminology, and deduplicated to yield a final corpus of 919 articles published between 1990 and 2025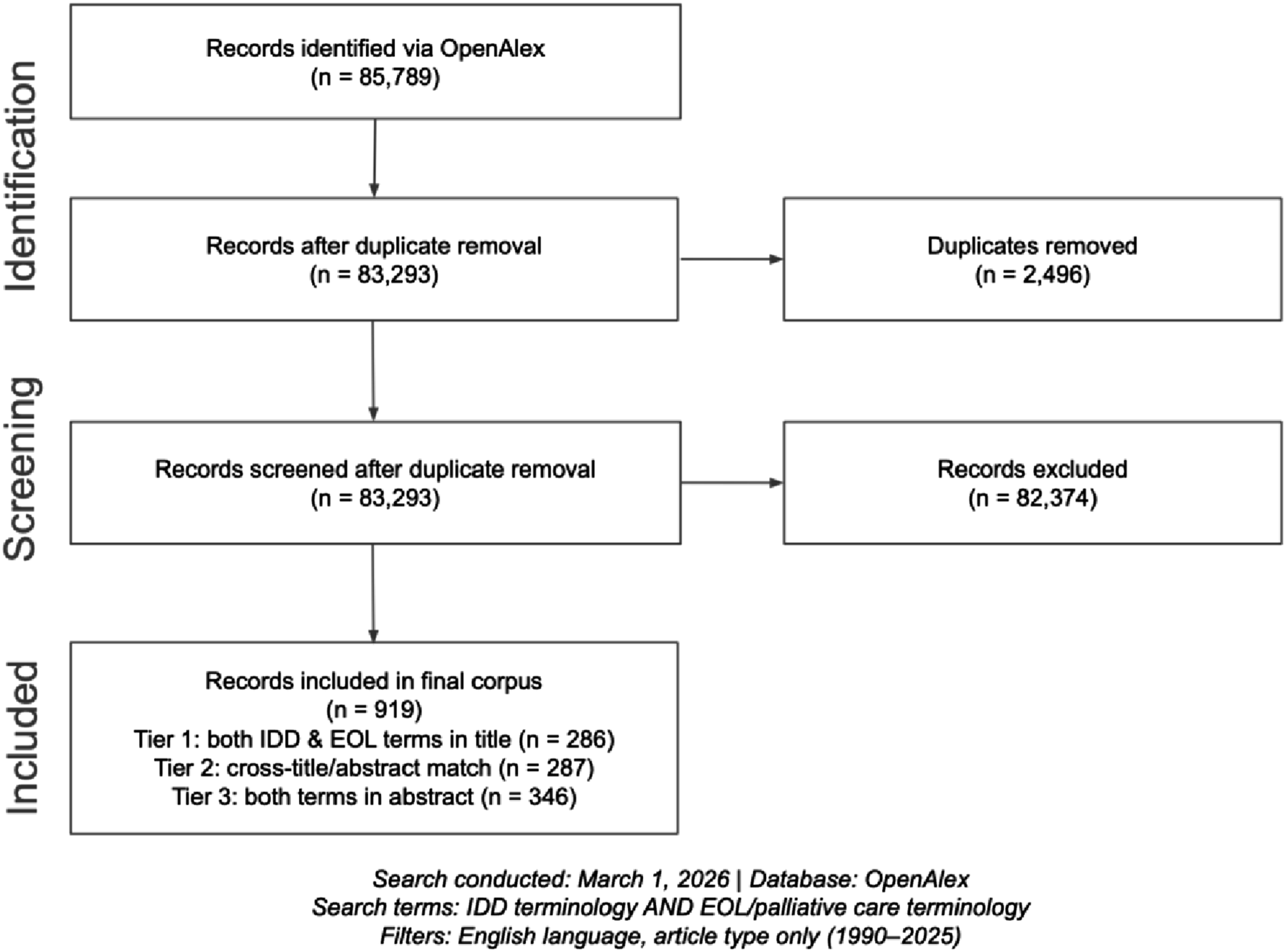
Bibliometric and Network Analyses
ublication trends were examined by plotting annual output from 1990 to 2025 and fitting both a linear regression and a polynomial trend line. Growth phases were identified through visual inspection of the annual trend, with boundaries placed at points of sustained directional change and contextualized against documented policy events. Journal and country productivity were assessed by counting the number of corpus papers attributable to each source, with country assignment based on author affiliation data extracted from OpenAlex. Country-level counts are not additive with respect to the 919-paper corpus, as multi-country papers are attributed to each contributing country. The h-index was computed for each journal and country appearing in the top 15 by output, using the standard definition: the maximum value h such that h papers have each received at least h citations (Hirsch, 2005). Bradford’s Law analysis was conducted by ranking all journals by output in descending order and identifying zone boundaries at successive thirds of total output (Bradford, 1934); the Bradford multiplier was computed as the ratio of journals required per zone. Open access status was classified per OpenAlex metadata and summarized across six time periods. The proportion of uncited papers was computed as the share of corpus articles recording zero global citations in OpenAlex as of March 1, 2026.
Two co-occurrence networks were constructed using NetworkX (Hagberg et al., 2008): a keyword co-occurrence network (nodes: keywords appearing in 6 or more papers; edges: co-occurrence in 2 or more papers) and an international collaboration network (countries contributing to 6 or more papers; pairs collaborating on 2 or more papers), with synonym normalization applied to keyword variants.
Topic Modeling
Topic modeling was performed using Latent Dirichlet Allocation (Blei et al., 2003) on a core subset of 508 documents meeting Tier 1 or Tier 2 eligibility with a minimum relevance score of 4. Text was preprocessed by lower-casing, removing punctuation and numerals, and applying an extended domain-specific stopword list that excluded both generic academic terms (study, results, methods) and universal domain terms (palliative, care, disability) to maximize discrimination between topics. Documents with fewer than 12 tokens after preprocessing were excluded, yielding a final modeling corpus of 423 documents and a vocabulary of 1,768 terms. The model was fitted using the Gensim implementation (Řehůřek & Sojka, 2010) with six topics, 30 passes, 300 iterations, asymmetric document-topic priors, and a fixed random seed for reproducibility. Coherence scores (c v ; Röder et al., 2015) were computed for models specifying 4 to 8 topics, yielding scores of 0.363, 0.351, 0.352, 0.341, and 0.359 respectively. The coherence curve was flat across this range (range = 0.022), with the four-topic solution yielding the marginally highest score. c v coherence for well-formed topic models in comparable social-science corpora is often reported in the 0.5 to 0.6 range; the lower values here are consistent with a smaller, lexically heterogeneous interdisciplinary corpus and reinforce the exploratory reading of the topic structure adopted throughout. However, manual inspection of top-weighted terms revealed that the four-topic solution produced one dominant topic absorbing 40% of documents with incoherent term mixtures, while six topics produced the most thematically distinct and interpretable groupings. Six topics was therefore selected on the basis of interpretability, consistent with recommended practice when coherence curves are flat (Chang et al., 2009). Topic labels were assigned based on inspection of the ten highest-probability terms per topic. Topic evolution was examined by computing mean topic probability per document across the six time periods.
Document Co-Citation Analysis
Document co-citation analysis was conducted to map the citation architecture of the field and identify its most structurally influential papers. For each of the 919 corpus papers, the full reference list was retrieved via the OpenAlex application programming interface, yielding 15,528 total reference links. A co-citation pair was defined as two papers cited together within the same corpus document. Papers cited five or more times by the corpus were retained as network nodes (n = 187); co-citation pairs occurring three or more times were retained as edges (n = 2,007), producing a weighted undirected network. Nine isolated nodes were removed. Betweenness centrality was computed for each node using NetworkX, quantifying the extent to which each paper bridges otherwise disconnected regions of the network (Freeman, 1977). Conventional community detection algorithms yielded low modularity scores (Q = 0.268), below the threshold typically associated with reliable cluster identification (Newman & Girvan, 2004). Accordingly, co-citation frequency and betweenness centrality are reported as complementary descriptive indicators of structural influence, without inferring discrete thematic communities from network partitioning.
Cohort-Normalized Citation Intensity Analysis
To identify papers gaining disproportionate attention relative to their publication cohort, a cohort-normalized citation intensity score was computed for each paper in the core corpus. The score was defined as the ratio of a paper’s global citation count to the mean citation count of all papers published in the same time period. This metric is not equivalent to formal burst detection algorithms such as Kleinberg’s burst detection (Kleinberg, 2003), but provides a straightforward cohort-adjusted measure of relative citation attention. Cohort periods correspond to those used in the topic evolution analysis. Papers with fewer than 10 global citations were excluded. The 15 papers with the highest scores were initially identified; two falling outside the IDD and palliative care intersection were subsequently excluded, yielding 13 papers reported in Table 5.
Results
Publication Trends, 1990–2025
A total of 919 English-language articles addressing EOL and palliative care for adults with IDD were identified in the final corpus, spanning the period 1990 to 2025. Annual output is presented in Figure 2. Three phases of growth were identified. A dormant phase (1990–2002) was characterized by sparse and irregular publication, with annual output rarely exceeding five articles. An emergence phase (2003–2011) saw sustained growth from single figures to approximately 30 publications per year, coinciding with landmark reports documenting premature and preventable deaths in this population, including the Mencap Death by Indifference report (Mencap, 2007) and the United Kingdom Confidential Inquiry (Heslop et al., 2014), which catalyzed policy and research attention across the IDD and palliative care fields. An acceleration phase (2012–2023) saw output increase sharply, reaching a peak of 75 publications in 2023. The overall linear slope across the full period was +2.01 papers per year. The apparent decline in 2024–2025 reflects database indexing lag rather than a true reduction in scholarly activity. Annual publication output for end-of-life and palliative care research in adults with intellectual and developmental disabilities, 1990–2025 (N = 919). The dashed curve represents a polynomial trend line. Three phases of growth are identified: dormant (1990–2002), emergence (2003–2011), and acceleration (2012–2023). The apparent decline in 2024–2025 reflects database indexing lag. Three papers indexed in 2026 are included in the 2025 bar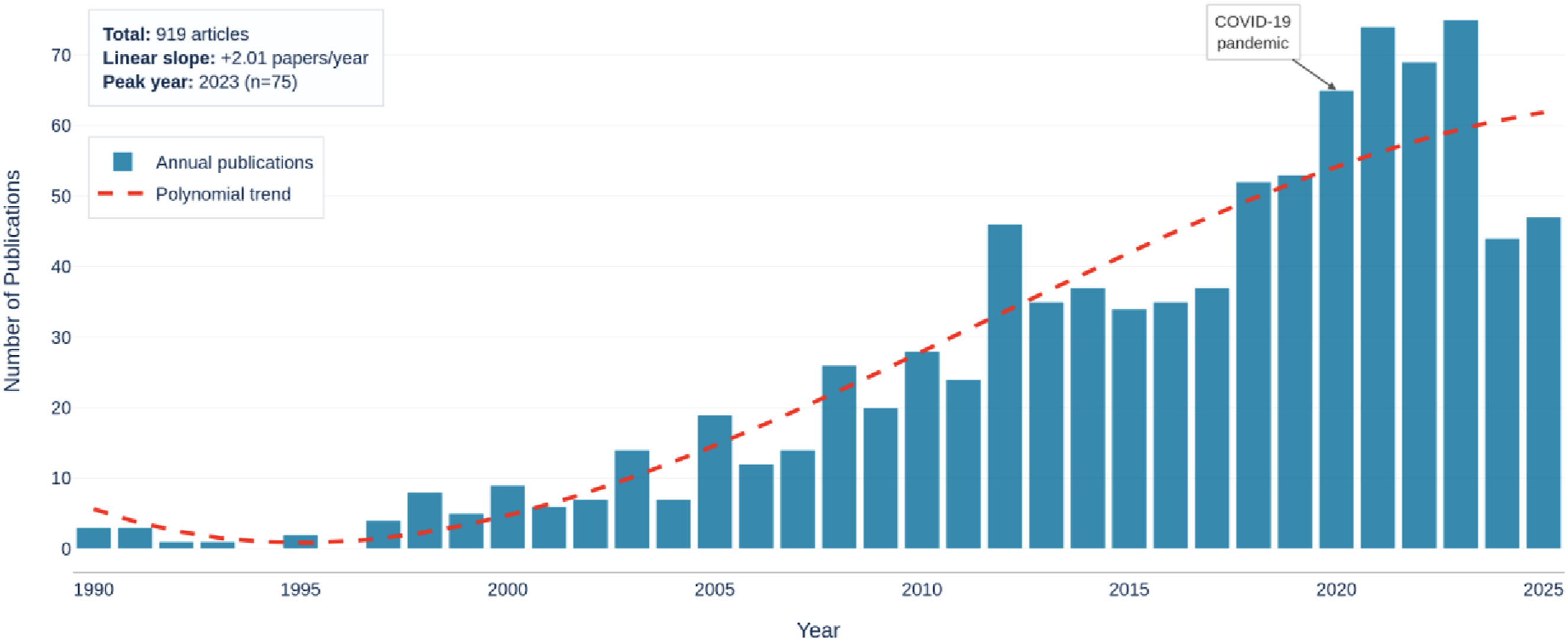
Citation counts across the corpus were highly skewed: 392 papers (42.7%) recorded zero global citations in OpenAlex as of the search date, while the remaining 527 papers accounted for the full citation load. The zero-citation rate varied markedly by period, rising from 25.9% in 1990–1999 to 47.5% in 2020–2025, suggesting that recency and indexing lag account for a substantial share of uncited papers rather than genuine scholarly neglect. Among papers published before 2020, the uncited rate was 39.3%, compared with 47.5% for papers published from 2020 onwards.
Journal Productivity and Citation Impact
Top 15 Journals by Publication Output With h-Index and Citation Metrics
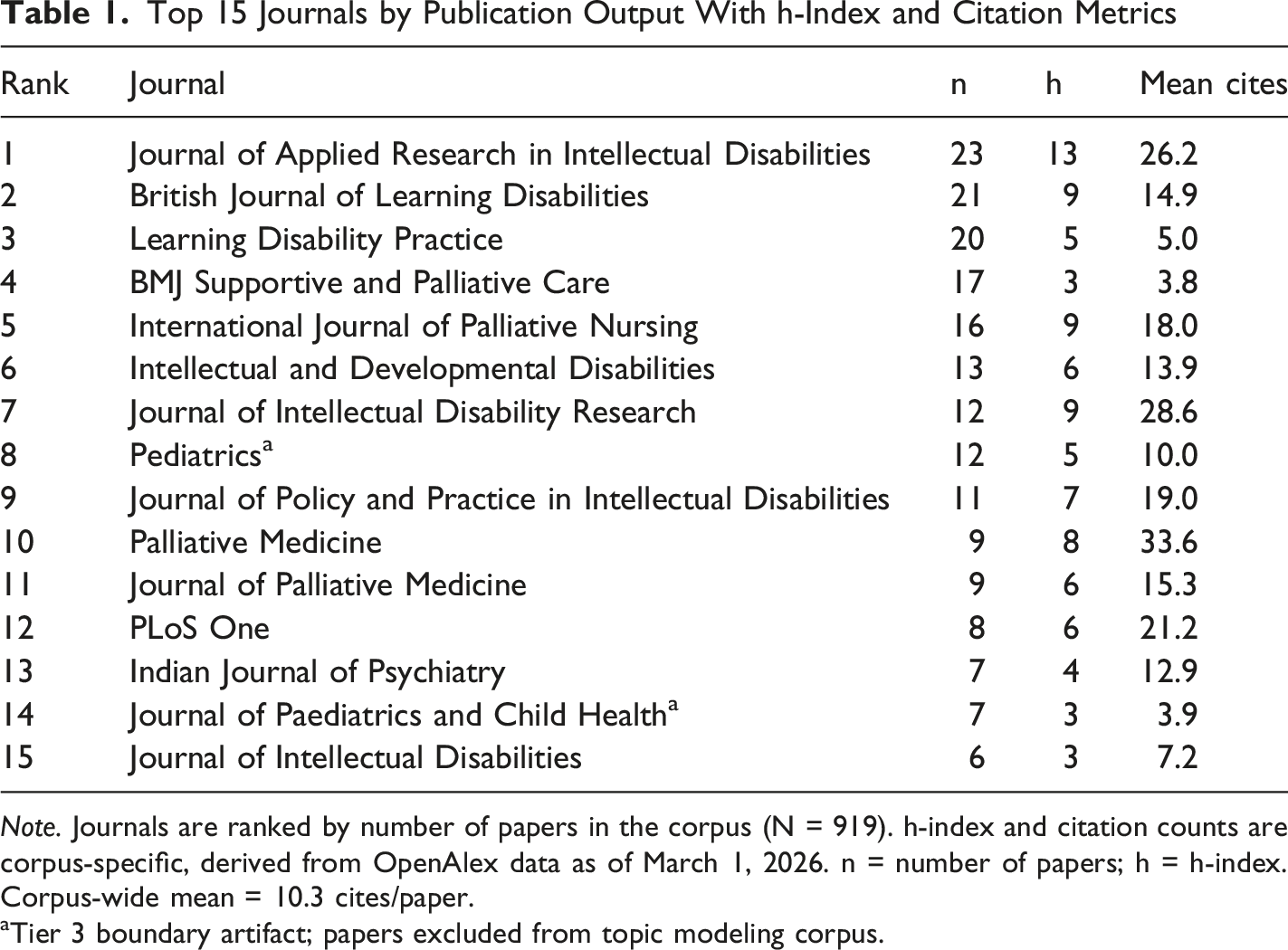
Note. Journals are ranked by number of papers in the corpus (N = 919). h-index and citation counts are corpus-specific, derived from OpenAlex data as of March 1, 2026. n = number of papers; h = h-index. Corpus-wide mean = 10.3 cites/paper.
aTier 3 boundary artifact; papers excluded from topic modeling corpus.
H-index analysis revealed important distinctions between volume and citation impact. Palliative Medicine recorded the highest mean citations per paper (33.6), substantially exceeding the corpus-wide mean of 10.3 citations per paper, despite ranking 10th by output. The Journal of Applied Research in Intellectual Disabilities recorded the highest h-index among individual journals (h = 13), consistent with its dominant volume. These findings indicate that while IDD-specialist journals publish the greatest volume of relevant research, palliative care journals confer substantially greater citation impact per paper, reflecting the broader readership of those venues. The appearance of Pediatrics (rank 8, n = 12) and Journal of Paediatrics and Child Health (rank 14, n = 7) in the top 15 reflects boundary artifacts of the relevance filtering strategy; all 19 papers from these journals were classified as Tier 3 and none met the threshold for inclusion in the topic modeling corpus, so their presence did not influence the topic modeling results.
Country Productivity and International Collaboration
Top 15 Countries by Publication Output With h-Index and Citation Metrics
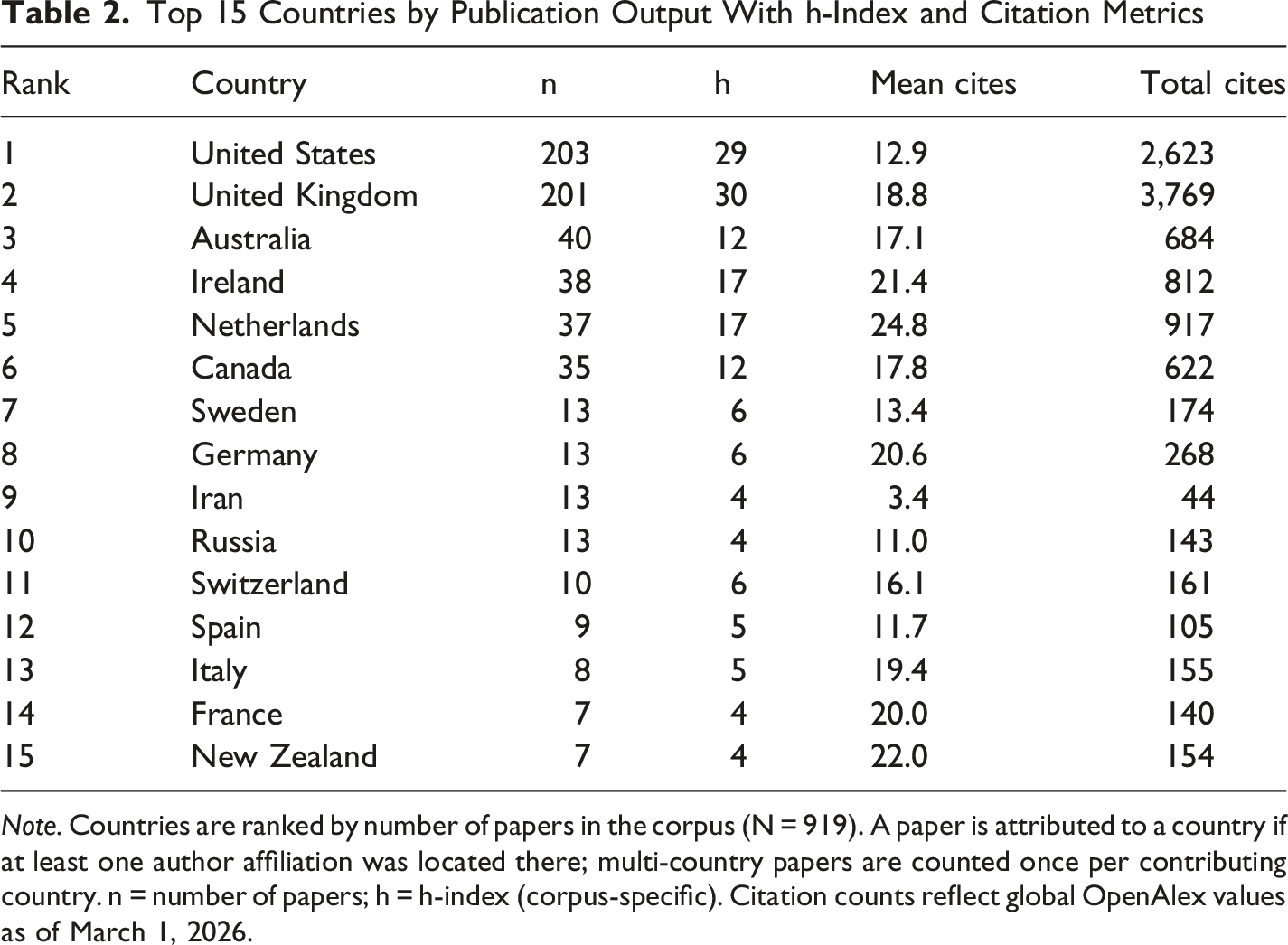
Note. Countries are ranked by number of papers in the corpus (N = 919). A paper is attributed to a country if at least one author affiliation was located there; multi-country papers are counted once per contributing country. n = number of papers; h = h-index (corpus-specific). Citation counts reflect global OpenAlex values as of March 1, 2026.
H-index analysis indicated that the United Kingdom recorded the highest h-index among contributing countries (h = 30), followed closely by the United States (h = 29), despite near-identical output volumes. The United Kingdom also recorded a higher mean citation count per paper (18.8 vs. 12.9 for the United States), suggesting greater average impact per publication. Country-level h-index values reflect the citation distribution of each country’s contribution to this specific corpus rather than a general indicator of research quality; cross-country comparisons are further confounded by differences in corpus output volume (Hirsch, 2005). The Netherlands recorded the highest mean citations per paper of any country in the top 15 (24.8), despite relatively modest output, indicating a concentrated body of high-impact work. The appearance of Iran and Russia (n = 13 each) in the top 15 reflects primarily low-citation output (mean citations 3.4 and 11.0 respectively), suggesting limited integration into mainstream international citation networks.
Of the 919 corpus papers, 101 (11.0%) involved authors from more than one country, indicating that the field is substantially nationally siloed. Because each multi-country paper is attributed to every contributing country, the per-country counts in Table 2 inflate national output. Across the top 15 countries the summed counts exceed the papers they represent by about 16% (647 attributions for 558 distinct papers). This inflation is small for the two leading producers, with 19% of United States papers and 23% of United Kingdom papers jointly authored internationally, but larger for several smaller contributors, including Ireland (58% of its papers) and the Netherlands and Canada (49% each). The international collaboration network is presented in Figure 3. The United Kingdom functioned as the primary hub of international collaboration, appearing in 9 of the 14 strongest bilateral partnerships. The strongest collaboration pairs were Ireland–United Kingdom (n = 12 jointly authored papers), United Kingdom–United States (n = 11), and Canada–United States (n = 10). Collaboration between non-Anglophone countries was sparse, with most partnerships involving at least one Anglophone nation. Countries from the Global South were absent from the collaboration network entirely, reinforcing the geographic insularity identified in the productivity analysis. International collaboration network for end-of-life and palliative care research in adults with IDD. Nodes represent countries contributing to ≥6 corpus papers; edge width is proportional to the number of jointly authored publications. Node size is proportional to total publication count. Nodes are grouped by world region as shown in the legend. Only 11.0% of corpus papers (101 of 919) involved multi-country authorship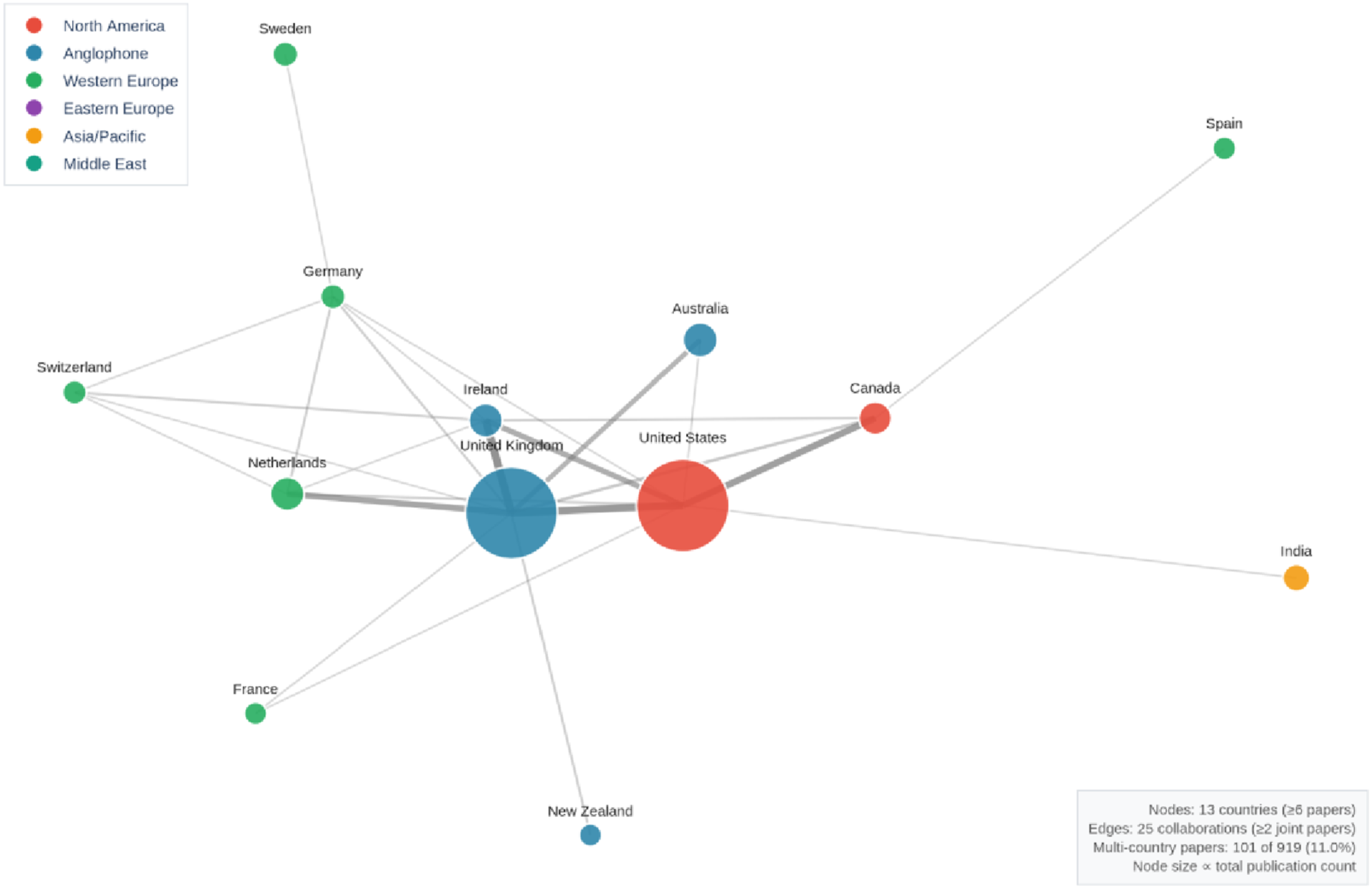
Keyword Co-Occurrence Network
The keyword co-occurrence network comprised 21 nodes and 110 edges, presented in Figure 4. The network revealed a dense central cluster anchored by the terms palliative care, end-of-life care, intellectual disability, nursing, and learning disability. The strongest single edge in the network connected nursing and palliative care (co-occurrence weight = 282), confirming nursing as the dominant disciplinary lens through which this literature is produced. A distinct qualitative methods sub-cluster was identifiable, grouping qualitative research and focus group, consistent with the field’s reliance on qualitative inquiry. Terms associated with patient experience and autonomy, including advance care planning, decision making, and quality of life, occupied peripheral positions in the network. These are themes that sit at the heart of contemporary death studies and palliative care practice, yet their marginal positioning in this literature suggests the field has not yet fully engaged with the patient-centered values that define modern EOL care or with the awareness contexts long central to death studies inquiry (Glaser & Strauss, 1965). Keyword co-occurrence network for end-of-life and palliative care research in adults with IDD. Nodes represent keywords appearing in ≥6 corpus papers; edges represent co-occurrence in ≥2 papers. Node size is proportional to keyword frequency; edge width is proportional to co-occurrence strength. Nodes are grouped by domain category (IDD/disability; Palliative/end-of-life; Research methods; Clinical/general) as shown in the legend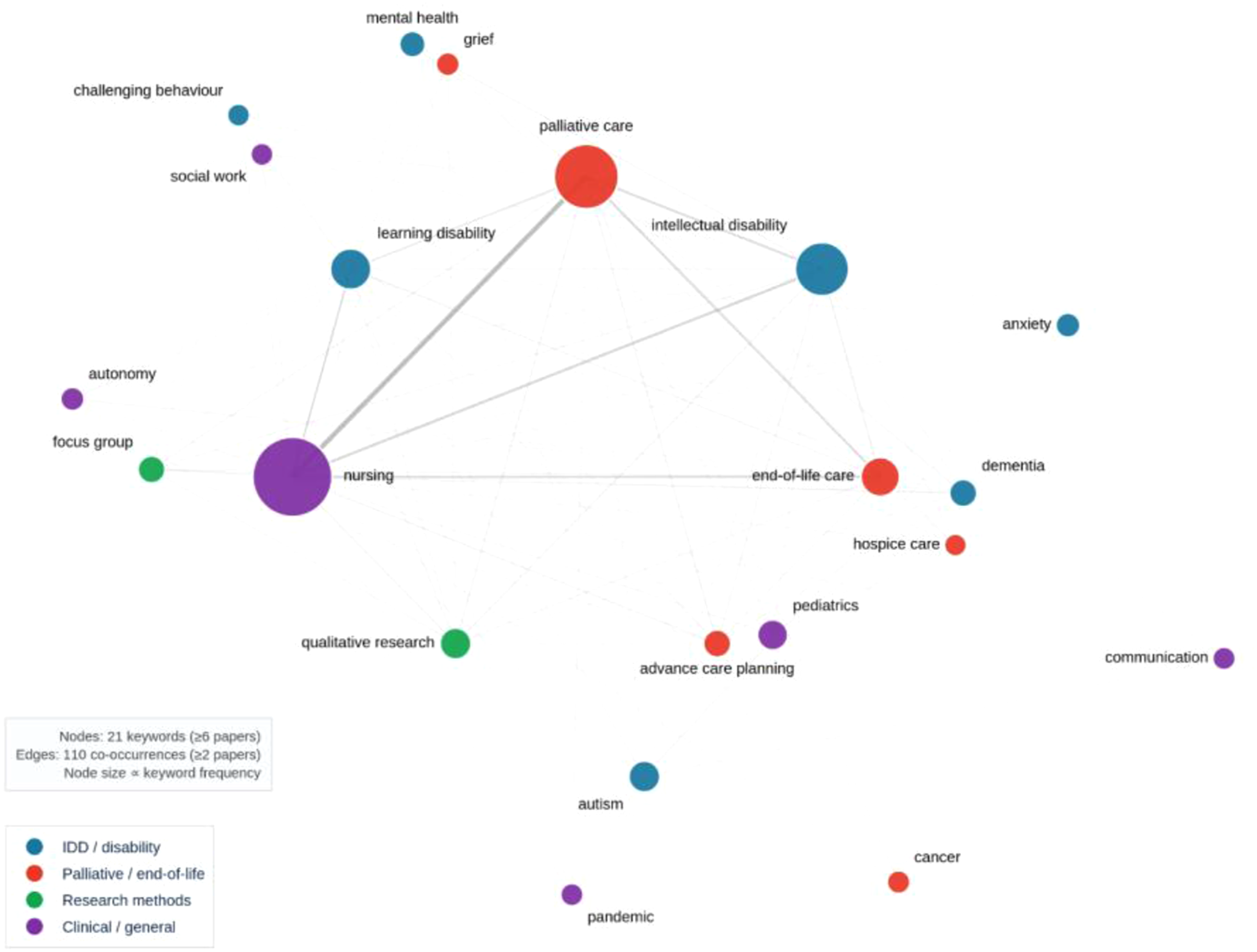
Bradford’s Law and Open Access Trends
Bradford’s Law zone analysis confirmed a concentrated output core: Zone 1 comprised 28 journals producing one-third of all corpus output, while Zones 2 and 3 required 140 and 254 journals respectively for equivalent volumes, consistent with the output concentration characteristic of an emerging interdisciplinary field (Egghe, 2005). Zone 1 contained an estimated three to four journals appearing to reflect indexing artifacts, a known consequence of broad Boolean search strategies.
Open access adoption increased markedly over the study period, rising from 14.8% in 1990–1999 (4 of 27) to 22.6% in 2000–2005 (14 of 62), before dipping to 16.9% in 2006–2011 (21 of 124). The most substantial increase occurred between 2006 and 2011 and 2012 and 2015, rising to 47.4% (72 of 152), consistent with the introduction of mandatory open access policies by the Wellcome Trust and Research Councils UK. Adoption continued to accelerate, reaching 67.8% in 2016–2019 (120 of 177) and 77.3% in 2020–2025 (289 of 374). The high open access rate represents a positive development for equity, particularly given the potential for practitioners in low- and middle-income countries to access findings without institutional subscriptions.
Thematic Structure: Topic Modeling
Topic Model Results: Six Thematic Domains Identified From 423 Core Documents
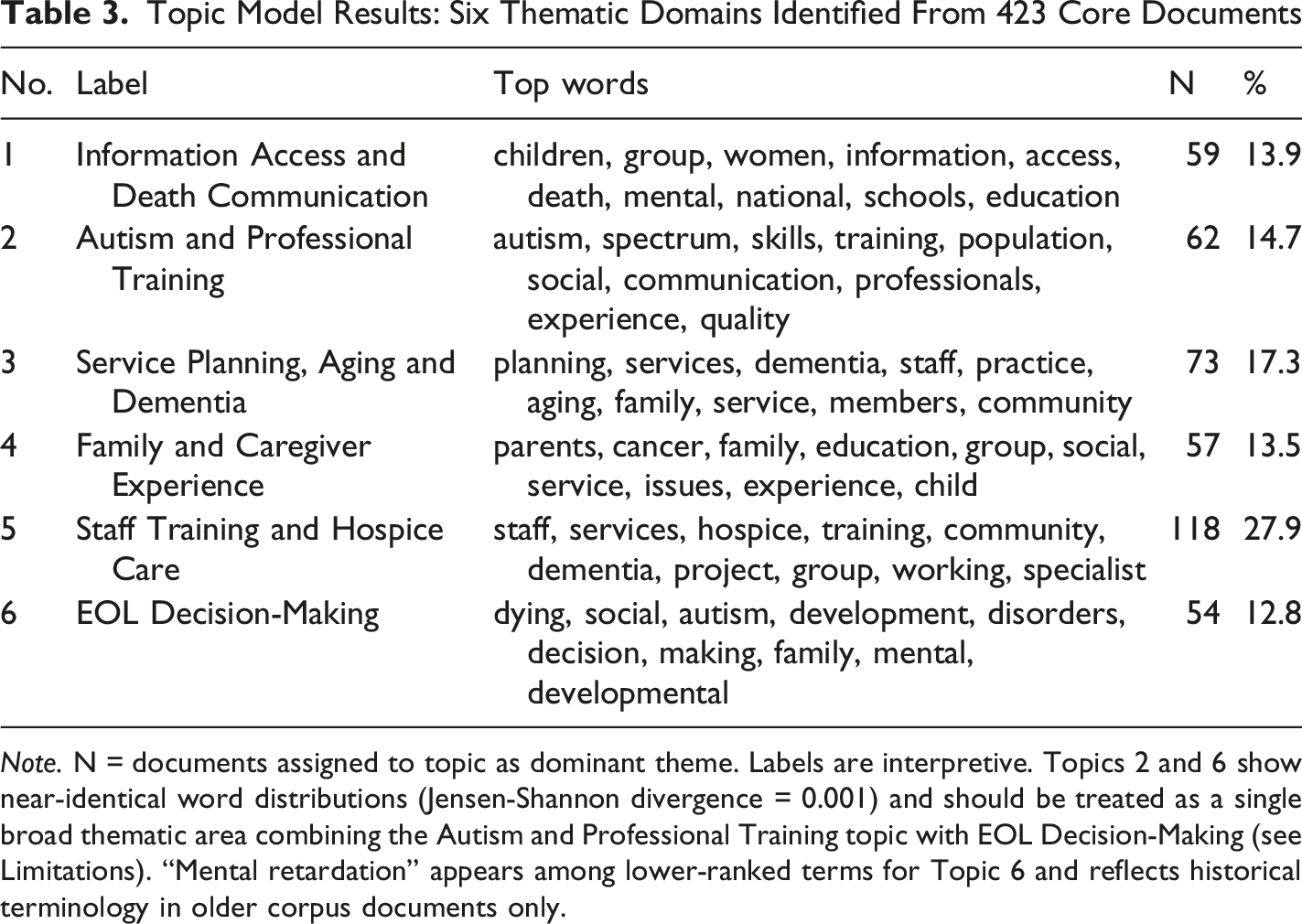
Note. N = documents assigned to topic as dominant theme. Labels are interpretive. Topics 2 and 6 show near-identical word distributions (Jensen-Shannon divergence = 0.001) and should be treated as a single broad thematic area combining the Autism and Professional Training topic with EOL Decision-Making (see Limitations). “Mental retardation” appears among lower-ranked terms for Topic 6 and reflects historical terminology in older corpus documents only.
Topic evolution over the six time periods is presented in Figure 5. The Staff Training and Hospice Care topic was dominant throughout the study period, peaking in the 2006–2011 phase (mean probability = 0.36). Service Planning, Aging and Dementia dominated in the earliest period (2000–2005), consistent with early policy concerns about the aging IDD population. Information Access and Death Communication showed a modest increase in the 2020–2025 period, possibly consistent with heightened attention to remote communication during the COVID-19 pandemic, though causal attribution cannot be established from topic probability data alone. Pre-2000 values should be interpreted with caution given the small number of documents in that period. The thematic interpretation offered here is exploratory, given the flat coherence curve across topic numbers and the non-trivial inter-topic overlap between Topics 2 and 6 discussed in the Limitations section. Evolution of six thematic domains identified by topic modeling across six time periods, 1990–2025. Values represent mean topic probability per document within each period (N = 423 core documents). Topic labels are interpretive summaries derived from top-weighted terms. Pre-2000 values should be interpreted with caution owing to small document counts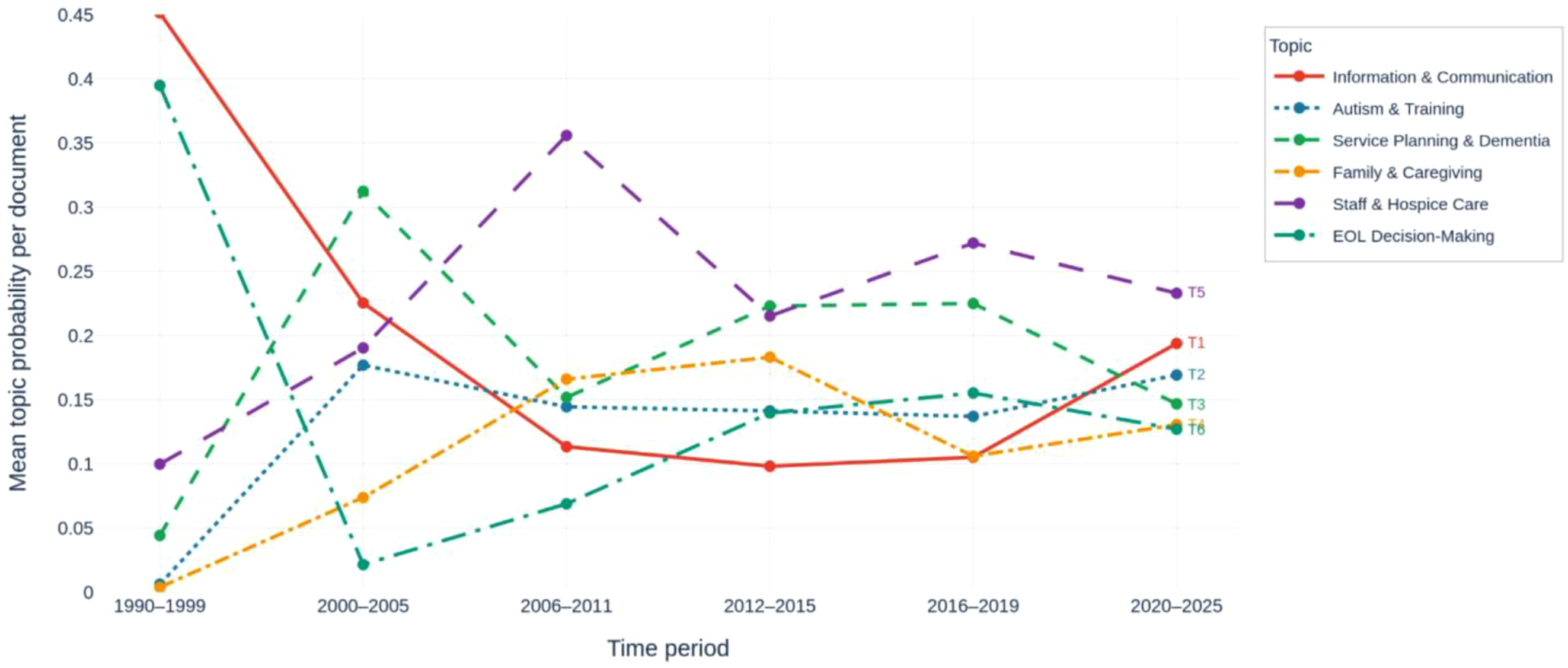
Citation Architecture: Document Co-Citation Analysis
Top 20 Most Co-Cited Papers in the Document Co-Citation Network
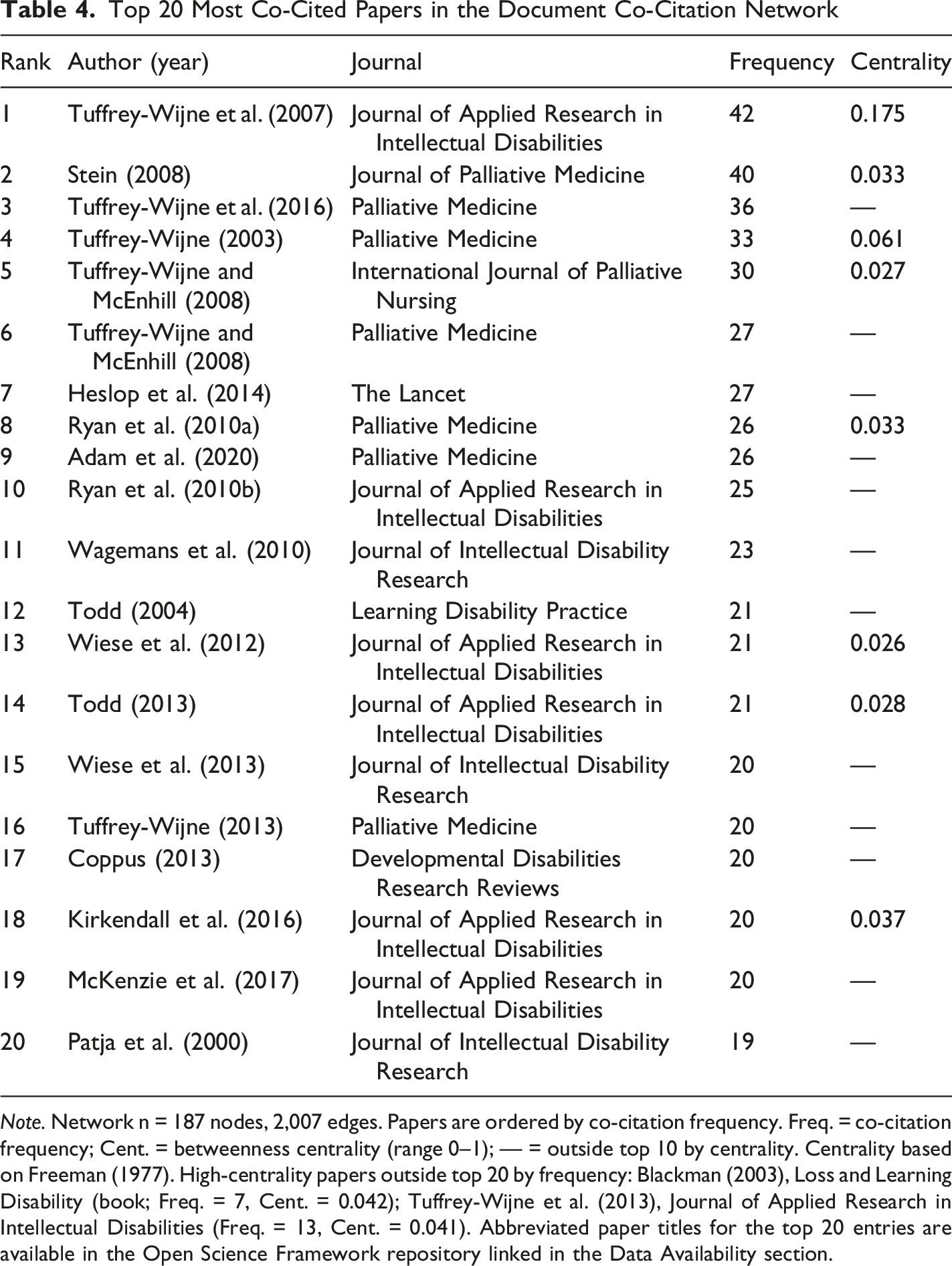
Note. Network n = 187 nodes, 2,007 edges. Papers are ordered by co-citation frequency. Freq. = co-citation frequency; Cent. = betweenness centrality (range 0–1); — = outside top 10 by centrality. Centrality based on Freeman (1977). High-centrality papers outside top 20 by frequency: Blackman (2003), Loss and Learning Disability (book; Freq. = 7, Cent. = 0.042); Tuffrey-Wijne et al. (2013), Journal of Applied Research in Intellectual Disabilities (Freq. = 13, Cent. = 0.041). Abbreviated paper titles for the top 20 entries are available in the Open Science Framework repository linked in the Data Availability section.
Kirkendall et al. (2016), a review of EOL decision-making in people with IDD, ranked fifth for centrality (0.037) despite ranking 18th for co-citation frequency, identifying it as a structurally important bridge paper disproportionate to its raw citation count. Blackman (2003), a text on loss and learning disability, ranked third for centrality (0.042) despite relatively low co-citation frequency (7 times), reflecting its role connecting the bereavement literature with the mainstream clinical EOL corpus. Taken together, these findings confirm that the intellectual foundation of this field rests on a narrow base of anchor papers, with a single author occupying both the most co-cited and the most structurally central position across three decades of literature. Because the network’s modularity falls below the level associated with reliable community detection (Q = 0.268), the bridging roles and regional descriptions reported here derive from co-citation frequency and betweenness centrality rather than from validated clusters, and should be read as descriptive indicators rather than discrete intellectual communities.
Cohort-Normalized Citation Intensity
Top 13 Papers by Cohort-Normalized Citation Intensity Score
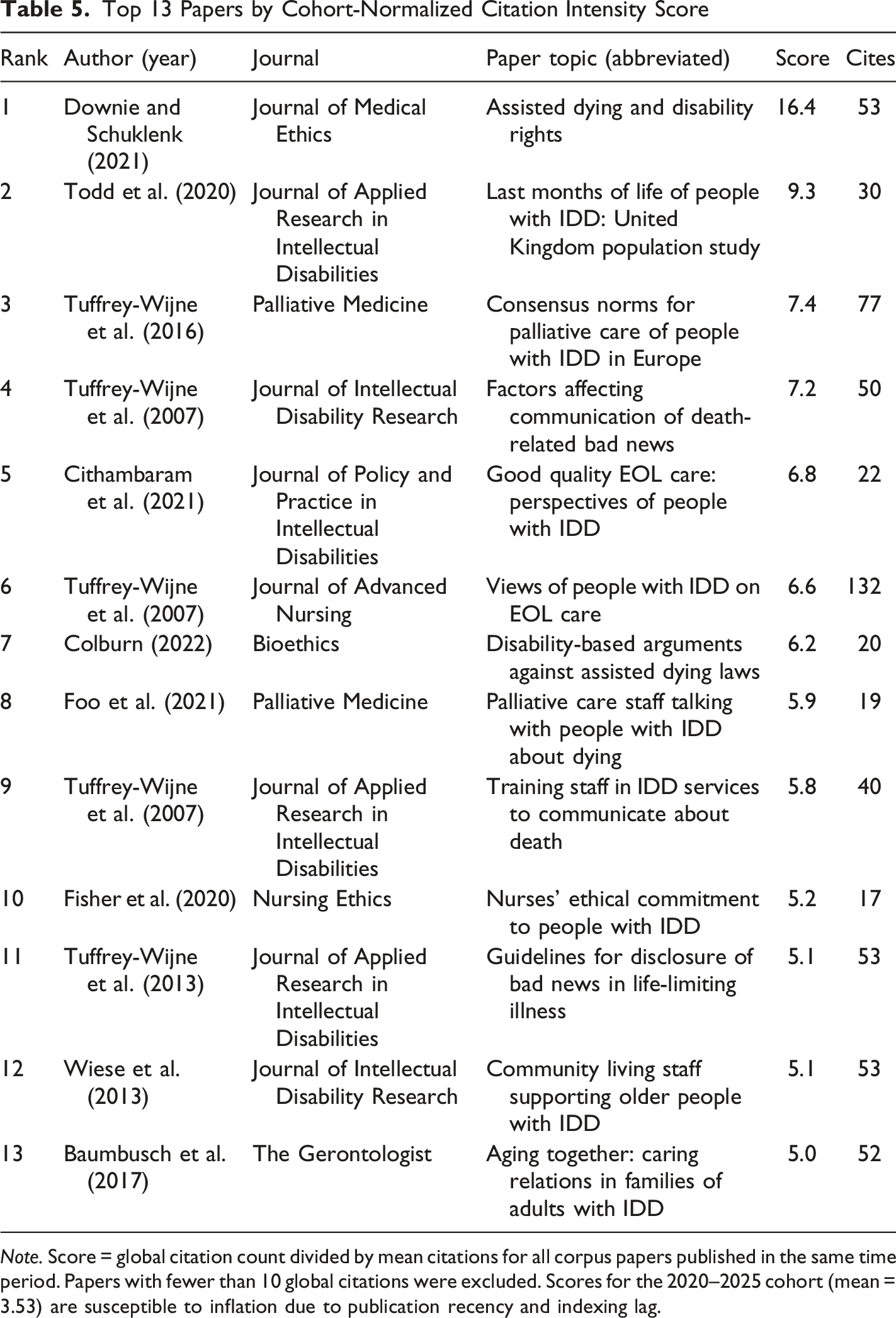
Note. Score = global citation count divided by mean citations for all corpus papers published in the same time period. Papers with fewer than 10 global citations were excluded. Scores for the 2020–2025 cohort (mean = 3.53) are susceptible to inflation due to publication recency and indexing lag.
Discussion
This study provides the first comprehensive bibliometric map of the global literature on EOL and palliative care for adults with IDD, drawing on 919 publications spanning 35 years. The findings describe a literature that has grown substantially since 2003 but remains structurally constrained: geographically concentrated, nationally siloed, thematically narrow in particular ways, and largely invisible to the mainstream palliative care and death studies communities it ought to inform. Read together, these findings raise questions that belong in death scholarship as much as in clinical palliative care: about how professional knowledge organizes itself around marginalized dying populations, whose voices come to count as authoritative within such knowledge, and what the structural conditions of that knowledge production reveal about the social organization of dying more broadly.
The Dissemination Gap as a Sociology of Knowledge
The most empirically striking finding of this review is the systematic mismatch between where this literature is published and where its findings would most plausibly inform practice. Of the top 15 journals by output, eight were IDD-specialist publications and only four were palliative care venues, accounting together for 51 of 919 corpus papers (5.5%). A hospice nurse, a palliative medicine consultant, or a community EOL team reading within their own professional literature will not encounter this evidence base through routine professional reading. This pattern is conventionally framed as a clinical communication problem, and at one level it is: it helps explain why barriers to equitable EOL care for people with IDD persist despite more than three decades of relevant research (Bekkema et al., 2014).
Read through a death studies lens, however, the dissemination gap is also a finding about the structural organization of knowledge. The siloing of scholarship on the deaths of cognitively marginalized adults within IDD-specialist venues is not merely an inefficiency in scholarly communication. It can also be read as a feature of how professional knowledge gets organized around populations that are themselves marginalized within broader healthcare and cultural systems. The IDD population’s invisibility in the journals that mainstream palliative care clinicians read mirrors the IDD population’s invisibility in the clinical encounters those clinicians manage. On this reading, the structure of the literature reproduces the structure of the marginalization it is ostensibly trying to address. This is the death studies argument the empirical pattern supports: who is positioned to know about whose deaths is itself a structural feature of how dying is socially organized. The bibliometric data document the dissemination pattern itself; the siloing of academic communities and the absence of institutional recognition are inferred causes, not measured ones.
This finding gains additional weight when set against the broader palliative care bibliometric landscape. Abu-Odah et al. (2022) mapped global palliative care research between 2002 and 2020 and identified seven major research clusters; IDD did not appear among them, not because the literature did not exist, but because it was not reaching palliative care journals in sufficient volume to register. The contrast between journal output and citation impact sharpens the point: Palliative Medicine ranked 10th by output in the present corpus but first by mean citations per paper (33.6 vs. a corpus-wide mean of 10.3), confirming that papers reaching a mainstream palliative care audience attract substantially greater scholarly attention. Strategic targeting of palliative care venues is not merely a matter of scholarly visibility; it is the most direct mechanism for closing the gap between what is known and what is practiced.
Awareness Contexts and the Marginal Position of Patient Voice
The dominance of the Staff Training and Hospice Care topic (27.9% of documents) across the full study period reflects a field that has been preoccupied with preparing paid caregivers for the practicalities of EOL care rather than centering the experiences and preferences of adults with IDD themselves. The comparatively small Family and Caregiver Experience topic (13.5%) and the peripheral positioning of advance care planning, decision making, and quality of life in the keyword network reinforce this interpretation. While staff training is undeniably important, an evidence base that consistently prioritizes institutional and professional concerns over the lived experiences of the people most affected risks producing guidance that is practically useful but ethically incomplete.
This finding speaks directly to one of the foundational concerns of death studies: the social organization of awareness around dying. Glaser and Strauss’s (1965) classic analysis of awareness contexts identified the closed and suspicion contexts that dominated mid-twentieth-century dying as configurations in which information about death was systematically withheld from the dying person. Subsequent death studies scholarship has tracked the partial movement toward more open awareness contexts but has also documented the persistence of older patterns in settings where the dying are deemed incapable of, or shielded from, knowledge of their own deaths. The empirical pattern observed in the present corpus, in which scholarship about the deaths of people with IDD has organized itself for three decades around the perspectives of those who care for the dying rather than the dying themselves, suggests that closed and suspicion awareness contexts have remained durable features of the IDD palliative care field. The relative growth of Information Access and Death Communication as a topic in 2020–2025 is encouraging and may signal a slow reorientation. But the structural pattern across three decades is striking: the dying have been the subject of this literature without being its informants. Open awareness is not a universal norm, however. In many non-Western settings, indirect or family-mediated communication about dying is preferred even for people who are not cognitively marginalized, and Glaser and Strauss’s framework was developed in a Western context; advocacy for centering the dying person’s voice should therefore be read alongside the literature’s Anglophone concentration rather than as a culturally neutral prescription.
Death studies as a discipline brings established methodological resources for addressing this gap, particularly traditions of qualitative inquiry developed to capture the perspectives of people with serious illness, including those with communication difficulties. These methodological strengths have been underutilized in the IDD and EOL literature, where qualitative inquiry predominates but has concentrated on staff and carer perspectives rather than those of people with IDD themselves. The distinct Autism and Professional Training cluster reflects the growing recognition that autism spectrum conditions, which frequently co-occur with intellectual disability, present specific challenges for EOL communication and planning that require tailored approaches (Tuffrey-Wijne et al., 2016). The identification of assisted dying and disability rights as an emerging citation intensity sub-theme deserves particular attention from death studies scholars, as assisted dying legislation places debates about cognitive capacity, safeguarding, and the rights of marginalized dying populations directly within the field’s intellectual remit.
Structural Fragility of the Knowledge Base
The co-citation analysis revealed a strikingly narrow intellectual foundation. A single author, Tuffrey-Wijne, occupied the most co-cited position (42 times), the highest betweenness centrality (0.175), and appeared six times in the top 20 most co-cited papers and five times among the top 13 citation intensity papers. While this reflects genuinely exceptional and sustained scholarship, such concentration of structural influence in a single researcher carries risks. A knowledge base that routes a disproportionate share of its intellectual traffic through one node may be more susceptible to conceptual narrowing than a more distributed knowledge base, and may inadvertently constrain the diversity of theoretical and methodological approaches in the field. These conclusions rest on descriptive network indicators rather than formally validated communities (modularity Q = 0.268) and should be regarded as indicative rather than definitive.
The high proportion of uncited papers (42.7% of the corpus) reflects a small number of anchor papers accumulating the majority of citation attention, a pattern common in emerging interdisciplinary fields lacking the dense citation networks of mature research communities. The pattern is also one death studies scholarship can think productively about. Marginalized dying populations tend to generate marginalized knowledge communities: small in size, dependent on individual carriers, vulnerable to disruption when those carriers retire or shift focus. The structural fragility of the IDD palliative care literature is not a critique of any individual scholar but a description of how knowledge about marginalized dying has historically been sustained. Building a more robust and interconnected knowledge base will require deliberate cross-disciplinary diversification, including engagement between IDD specialists, palliative care researchers, and death studies scholars.
Growth, Geographic Concentration, and Open Access
The three-phase growth trajectory reflects the field’s dependence on policy shocks rather than sustained research investment. The dormant phase (1990–2002) corresponds to a period when EOL care for people with IDD was absent from clinical guidelines and largely invisible to policymakers. Growth did not begin in earnest until landmark reports forced the issue onto the agenda, and the acceleration phase from 2012 onwards reflects the downstream effects of those shocks rather than an independently developing research program. This pattern of reactive rather than proactive growth has consequences for the coherence and cumulativeness of the evidence base, and is itself an argument for dedicated funding streams that do not depend on crisis to generate momentum.
The concentration of output in the United States and United Kingdom (44% of all papers) raises important questions about transferability. EOL care for people with IDD is not culturally neutral: care models, legal frameworks governing advance directives and assisted dying, family structures, and cultural attitudes toward death and disability vary substantially across regions. A literature generated predominantly in two high-income Anglophone countries cannot be assumed to speak to the EOL needs of the majority of people with IDD, who live in low- and middle-income countries where palliative care infrastructure, disability services, and legal frameworks differ fundamentally (Carollo et al., 2021). The near-complete absence of Global South countries from the collaboration network is an absence from the English-language indexed literature, which is not the same as an absence from the literature itself. Brazilian, Spanish-language, and Francophone African scholarship on IDD and end-of-life care may exist but would not be captured by an English-only search. The gap this review documents is therefore one of representation in the indexed, English-language evidence base that mainstream palliative care and death studies communities read, rather than necessarily a gap in the world’s scholarship. This concentration is not unique to the IDD subfield: Abu-Odah et al. (2022) found the United States and United Kingdom to be the two most productive countries in global palliative care research, so the Anglophone skew documented here reflects palliative care scholarship broadly rather than a signature specific to this population. A fuller comparison against other marginalized groups, such as people experiencing homelessness or imprisonment, is constrained by the scarcity of comparable bibliometric profiles for those populations.
The acceleration of open access adoption, reaching 77% of papers in 2020–2025, represents the most unambiguously positive structural trend identified in this review. Open access is particularly consequential in this field because the practitioners most in need of this evidence, including disability support workers, community nurses, hospice staff, and family caregivers, are frequently employed outside academic institutions and lack access to subscription-based journals. The marked increase coinciding with funder mandates from the Wellcome Trust and Research Councils UK is consistent with a policy lever interpretation, though causal attribution cannot be established from observational data alone. The convergence of high open access rates and an accelerating publication trend means that the evidence base is both growing and becoming more accessible. The remaining challenge is ensuring it reaches the right journals, and therefore the right audience.
Limitations
The findings of this review should be interpreted in light of several limitations, which fall broadly into three categories: data and search limitations, analytical limitations, and interpretive limitations.
Regarding data and search, bibliographic data were retrieved from a single database. While OpenAlex provides broad disciplinary and geographic coverage and supports full methodological reproducibility (Culbert et al., 2025; Maddi et al., 2025), its metadata quality continues to be evaluated and some inconsistencies have been identified, particularly in reference matching and institutional affiliation data (Culbert et al., 2025). OpenAlex reference coverage is less complete for older publications, with corpus papers from the dormant phase (1990–2002) returning a median of one reference each against a median of nine for papers from 2012 onward. The co-citation network, which draws on these reference lists, therefore reflects the earliest corpus papers less fully. The absence of an early foundational cluster in the network may partly follow from this, and should not be read as firm evidence that no early foundational work exists. This qualification is confined to the network’s treatment of the dormant phase. It does not bear on the publication-trend, dissemination, thematic, or geographic findings, which derive from publication and affiliation metadata rather than reference lists, nor on the network’s well-supported findings about the more recent literature, which rest on far denser reference data. Additionally, the restriction to English-language publications may have systematically underrepresented contributions from non-Anglophone countries, compounding the geographic concentration observed in the productivity analysis and potentially overstating the dominance of United Kingdom and United States research.
Regarding analytical decisions, the three-tier relevance filtering strategy introduced author-defined thresholds that, while applied consistently, involve a degree of subjectivity. Tier 3 records (both IDD and EOL terms in abstract only) make up 37.6% of the corpus and may include papers in which the intersection of IDD and palliative care is tangential rather than central. These records are excluded from the topic-modeling core, so the thematic findings do not depend on the Tier 3 threshold. Restricting the full-corpus analyses to the higher-confidence Tier 1 and Tier 2 records raises the share of papers in palliative care venues only modestly, from 5.5% to 8.2%, and leaves the central dissemination finding intact; the higher uncited rate among Tier 3 records (48.0% against 39.4% for Tier 1 and Tier 2) is consistent with their more peripheral relevance.
The inclusion of autism spectrum disorder as a search term may have introduced papers addressing autism without co-occurring intellectual disability, given that autism spectrum disorder alone does not meet the American Association on Intellectual and Developmental Disabilities or DSM-5 definitions of IDD (American Association on Intellectual and Developmental Disabilities, 2021); at the title level this represented approximately 5.4% of the final corpus. Within the topic model, these papers did not concentrate in the Autism and Professional Training topic. They split across that topic (6 papers, 26%) and the EOL Decision-Making topic (10 papers, 43%), the two domains already shown to be near-identical (Jensen-Shannon divergence = 0.001), and they accounted for only 10% of documents assigned to the Autism and Professional Training topic. Refitting the six-topic model with these papers excluded from the core, leaving 400 documents, left the substantive findings unchanged: staff training and hospice care remained the single dominant theme (44.2% of documents), with patient, family, and decision-making themes secondary. The autism boundary therefore does not materially affect the thematic conclusions. Historical disability terminology including ‘mental retardation’ appears in the OpenAlex metadata of older corpus documents and consequently in the topic model’s term distributions; its presence reflects the language of the historical literature and not the author’s terminology.
Topic modeling labels are interpretive summaries based on inspection of top-weighted terms, and alternative labelings remain possible. The number of topics (six) was selected on the basis of interpretability after inspection of models from four to eight topics; the coherence curve was flat across this range, providing no clear quantitative basis for model selection (Chang et al., 2009). Examination of the five-topic solution showed that the Service Planning, Aging and Dementia and EOL Decision-Making topics collapsed into a single diffuse topic combining service planning, dementia, decision making, and dying, while the staff-training topic remained distinct and dominant and the autism cluster persisted. This reduced the interpretability of the planning and decision-making distinction, so six topics was retained. To test whether the substantive findings depend on this choice, the model was also refitted at five and seven topics. The preponderance of staff training and the peripheral position of patient and family perspectives held in both solutions: the staff-training topic was the single largest theme at five topics (30.3% of documents), and the two largest topics at seven topics were both centered on services and staff, while topics centered on patient decision making and family experience remained minority themes. The thematic conclusions are therefore not an artifact of the number of topics selected. Post-hoc inter-topic distance analysis revealed a Jensen-Shannon divergence of 0.001 between Topics 2 and 6 (natural logarithm base, range 0 to ln 2 ≈ 0.693), indicating near-identical probability distributions. Users of the topic modeling findings should treat Topics 2 and 6 as reflecting a single broad thematic area combining the Autism and Professional Training topic with EOL Decision-Making rather than two empirically distinct categories, and should regard the full topic structure as exploratory rather than as validated discrete thematic categories.
Regarding interpretive limitations, the co-citation network modularity score (Q = 0.268) fell below the threshold for reliable community detection (Newman & Girvan, 2004). Co-citation frequency and betweenness centrality are therefore reported as descriptive indicators of structural influence rather than evidence of formally validated clusters. Two features of the dissemination pattern also lie beyond what bibliometric data can show. The choice of publication venue may reflect the fit between a study’s research questions and a journal’s scope rather than structural siloing alone, and the data contain no record of manuscripts submitted to and rejected by palliative care journals, which would bear on whether the pattern reflects authors’ submission choices or editorial gatekeeping. These are interpretive boundaries on the structural account offered in the Discussion, not challenges to the observed distribution itself. Finally, all citation counts and open access classifications reflect OpenAlex data as of March 1, 2026 and will change as indexing continues; the apparent decline in output in 2024–2025 and the elevated zero-citation rate for recent papers both reflect this indexing lag rather than genuine reductions in scholarly activity or impact.
Conclusions
This study provides the first empirical map of the global literature on EOL and palliative care for adults with IDD, drawing on 919 publications spanning 35 years. Four conclusions emerge with implications for both clinical palliative care and death studies. First, three decades of relevant research have accumulated almost entirely outside the journals where palliative care clinicians read, what this review interprets as a structural feature of how scholarly knowledge about the deaths of cognitively marginalized adults has been organized and a plausible explanation for why barriers to equitable EOL care for this population persist. Second, the field is geographically concentrated in a small cluster of Anglophone countries, with only 11.0% of papers involving multi-country collaboration, raising serious questions about the generalizability of findings to the majority of the world’s population with IDD who live in low- and middle-income countries. Third, topic modeling reveals a persistent preoccupation with staff training and institutional care over three decades, with patient and family perspectives comparatively underrepresented; the dying have been the subject of this literature without being its informants, a pattern that connects directly to long-running death studies concerns about awareness contexts and the social organization of dying. Fourth, the citation architecture of the field rests on a narrow intellectual foundation concentrated in a single author’s body of work, suggesting structural fragility characteristic of marginalized knowledge communities and the need for deliberate cross-disciplinary diversification.
Three concrete actions follow. Researchers should submit EOL and IDD work to palliative care and death studies journals, ensuring it reaches the clinicians, hospice staff, and scholars of dying most positioned to act on it and to integrate it into broader scholarship on death and dying. This recommendation is constrained by a structural disincentive: tenure criteria and departmental journal hierarchies in disability studies and special education often reward field-specific publication over palliative care outlets, so closing the dissemination gap will require change to these incentive structures and not only individual submission choices. Funders should support investigator-led studies in low- and middle-income countries, where IDD prevalence is highest and research output lowest. Future research should place adults with IDD at its center, treating them not as the subject of proxy accounts but as the primary informants of their own dying. Such work will call for methods that bring people with IDD and their families directly into the research, with care for the bereavement these conversations can carry. It will also need to attend to awareness in its fuller register, as something expressed through emotion and behavior, and sometimes held inwardly, rather than through spoken disclosure alone. Open access adoption has reached 77% in 2020–2025; the evidence is increasingly findable. The remaining task is making it speak across the disciplinary boundaries that have so far constrained it, and to the question that ought to organize death studies’ engagement with marginalized populations: whose deaths come to matter to scholarly and professional communities, and on what terms.
Footnotes
Acknowledgments
The author thanks K. Gulati for assistance with the bibliometric analysis pipeline and manuscript preparation.
Consent to Participate
This study analyzed publicly available bibliographic metadata retrieved from the OpenAlex database and did not involve human participants, human data, or human tissue. No ethical approval was required.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset and complete analysis pipeline supporting the findings of this study are available via the Open Science Framework at https://doi.org/10.17605/OSF.IO/2SDVX. (Myung, 2026)