
Abstract
This study examines women’s experiences of interacting with healthcare professionals after receiving serious prenatal information around gestational week 18 and through subsequent late pregnancy loss, including termination of pregnancy, intrauterine foetal death, or miscarriage. It focuses on medical guidance, emotional support, and post-birth care. A qualitative descriptive design was used. Five Norwegian women participated in individual in-depth interviews, providing insight into encounters with healthcare professionals across the care trajectory. Their experiences unfolded across four key moments: learning about the diagnosis, making a decision, giving birth, and leaving the hospital. Care was experienced as fragmented, intensifying emotional distress and uncertainty. Shifts between clinical and emotionally attuned language created cognitive dissonance, leading the women to question the legitimacy of their grief and maternal identity. These findings highlight the need for coordinated psychosocial and medical care that acknowledges maternal identity and affirms women’s right to grieve.
Keywords
Introduction
Pregnancy is experienced as a period of anticipation, attachment, and the emergence of maternal identity. For many women, the second trimester is when the pregnancy becomes increasingly embodied and socially acknowledged (Goksøyr & Økland, 2017). When serious foetal conditions are identified at this stage, the anticipated future with the unborn child may abruptly collapse, potentially transforming the pregnancy into an experience of loss.
Legal, institutional and clinical contexts and practices frame the experiences of late termination of pregnancy or miscarriage. At the time of this study self-determined abortion in Norway was permitted until the end of gestational week 12. Termination between gestational weeks 12 + 1 and 21 + 6 required approval by a regional abortion committee. Routine ultrasound screening was normally conducted around gestational week 18, meaning that serious foetal conditions were often identified within a relatively narrow period for further investigation, decision-making, and, where relevant, application for termination. These legal and organisational conditions form an important context for the women’s encounters with healthcare professionals.
Being informed of severe foetal anomalies often represents a profound turning point for expectant parents, fundamentally altering their understanding of the pregnancy and confronting them with decisions about the future and the possibility of continuation or termination (Heaney et al., 2022). The process of interpreting diagnostic information and reaching a decision has been described as emotionally demanding (Damm et al., 2025a), characterised by ambivalence, uncertainty, and inner conflict (Blakeley et al., 2019; Lafarge et al., 2019). Pregnancy termination due to foetal anomaly has also been described as a potentially traumatic experience, often associated with long-lasting emotional consequences (Jones et al., 2017; Lafarge et al., 2014).
Although termination following a serious foetal diagnosis shares features with miscarriage and stillbirth, it also involves distinctive emotional and psychosocial challenges. Women may grieve a wanted pregnancy while also coping with their involvement in the decision to terminate, often experiencing ambivalence, moral conflict, responsibility, grief, and relief simultaneously (Andersson et al., 2014; Goldblatt Hyatt, 2021; Heaney et al., 2022; Lafarge et al., 2013a, 2013b). In addition, abortion-related stigma and anticipated judgment may contribute to isolation and difficulties seeking support (Hanschmidt et al., 2016; Hendriks & Abraham, 2022). These findings suggest that grief following termination for foetal anomaly may differ from both spontaneous pregnancy loss and termination of an unwanted pregnancy, while also varying considerably between women (Lafarge et al., 2017).
Prior studies highlight substantial variation in parents experience and responses to pregnancy termination. Some express a need for solitude after receiving the diagnosis, while others seek active emotional support (Asplin et al., 2014). Furthermore, some parents emphasise the importance of creating memories and spending time with the foetus, others prefer to avoid reminders of the loss (Damm et al., 2025b; Heaney et al., 2022; Hodgson & McClaren, 2018). Beyond the decision and giving birth, the emotional and practical aftermath of termination has been described as an abrupt transition, often characterised by shock, social withdrawal, and insufficient follow-up (Heaney et al., 2022; Lafarge et al., 2014). Taken together, this illustrate that late termination of pregnancy involves a complex constellation of emotional, relational, and existential losses. Reproductive loss has been described as a complex and multifaceted form of grief, involving multiple layers of loss that may be both immediate and cumulative (Diamond & Diamond, 2017). It has been conceptualised as a form of disenfranchised grief (Doka, 1989, 2008). Such grief is often not openly acknowledged or socially validated and is characterised by few or no culturally sanctioned rituals through which it may be recognised or mourned. Consequently, parents may grieve in isolation, and the significance of the grief may remain unrecognised by both themselves and others, including healthcare professionals (Diamond & Diamond, 2016, 2017).
Within this context of emotional upheaval, uncertainty, and abrupt transition, parents facing the possible termination of a pregnancy are often unprepared for what lies ahead. Subsequently, there is a need for guidance, emotional support, and clear information throughout both the diagnostic process and the post-termination period (Brann et al., 2019; Cullen et al., 2018; Heaney et al., 2022). Encounters with healthcare professionals therefore become central to how the situation is experienced and understood.
Providing care in this context poses complex challenges for healthcare professionals. The emotional intensity of the decision-making process, combined with ethical complexity and clinical responsibility, may complicate the provision of consistent and responsive care (Andersson et al., 2014; Lafarge et al., 2017). The quality of care during and after pregnancy termination due to foetal anomaly has been found to influence women’s psychological adjustment and long-term well-being (Helps et al., 2020; Lafarge et al., 2013a). Healthcare professionals are often the first to communicate the diagnosis; they also support decision-making, are present during the birth, and frame the loss within medical and emotional narratives. How these encounters unfold may significantly shape parents’ memories and experiences of the event, and their understanding of what has occurred (Heaney et al., 2022). Variation in parents’ needs and preferences further underscores the importance of individualised care, continuity, and appropriate follow-up during and after termination (Giannatiempo et al., 2024; Kersting et al., 2013; Lafarge et al., 2017; Lotto et al., 2016).
Midwives and other healthcare professionals have been highlighted as particularly important providers of empathetic and individualised care during this process (Damm et al., 2025b; Heaney et al., 2022; Lyus et al., 2014). However, factors such as professional and clinical experience, personal opinions, institutional guidelines and routines, available resources, and opportunities for follow-up and reflection may influence the healthcare professionals’ responses and the care offered (Andersson et al., 2014; Heinsen et al., 2023). Previous research also suggests that healthcare professionals’ understandings of women’s coping and support needs do not always correspond with women’s own accounts (Lafarge et al., 2017). In this context, women may be sensitive to language, practices, or differences in care that they perceive as communicating judgment or as assigning less legitimacy to their loss. Such experiences should not necessarily be interpreted as evidence of explicitly judgmental attitudes among individual healthcare professionals. They may also arise from clinical terminology, organisational constraints, or institutional distinctions between termination, miscarriage, and stillbirth. Nevertheless, anticipated or perceived judgment, including abortion-related stigma, may influence women’s willingness to disclose their experiences, seek support, and understand their own entitlement to grieve (Hanschmidt et al., 2016). It is therefore important to examine not only the information and clinical care provided, but also how professional communication and institutional practices are experienced by women throughout the care trajectory.”
Within this context, the language used by healthcare professionals has been described as an important factor shaping how pregnancy loss is understood and emotionally processed (Jonas-Simpson & McMahon, 2005). When differences between health personnel’s clinical language and women’s own ways of understanding and articulating their experiences are not recognised, women may feel that the significance of the pregnancy and loss is not acknowledged (Kjelsvik et al., 2026; Kristiansen et al., 2026). Against this backdrop, this study explores how Norwegian women experienced their encounters with healthcare professionals after receiving serious prenatal information around gestational week 18 and through their late termination of pregnancy or miscarriage.
Materials and Methods
Study Context
At the time of the study, routine ultrasound screening around gestational week 18 was part of the Norwegian public antenatal care programme, providing information about gestational age, number of foetuses, placental position, and foetal anatomy and structural development (Norsk Helseinformasjon, 2025). Under the Abortion Act in force during the study period, self-determined abortion was permitted until the end of gestational week 12, while termination between gestational weeks 12 + 1 and 21 + 6 required approval from a regional abortion committee (Abortloven, 1975). 1 In 2022, a total of 193 committee-approved terminations of pregnancy were performed after gestational week 18 in Norway under the indications specified in the Abortion Act (Løkeland et al., 2023), compared with 52,026 live births (Thomsen et al., 2023).
Legal and organisational frameworks also shape women’s experiences of pregnancy loss. In Norway, women are not entitled to maternity leave until 12 weeks before their estimated due date, and pregnancy termination before gestational week 22 does not qualify for maternity leave or benefits in the same way as perinatal death (Folketrygdloven, 1997, §14–5, §14–9, §14–17). There are no national psychosocial guidelines for hospital care and follow-up for women who experience late termination of pregnancy or late miscarriage. These structural conditions may influence how loss is recognised, supported, and followed up within the healthcare system.
Study Design
This study employed a qualitative, descriptive, and interpretivist research design (Berger & Luckmann, 1966) informed by a process-oriented and narrative understanding of experience. Qualitative interviews are particularly suitable for exploring sensitive and under-examined experiences (Rapley, 2004). A semi-structured interview with initial open-ended questions allowed participants to reflect on their experiences while providing flexibility to explore emerging themes (Kvale & Brinkmann, 2015). User perspectives were integrated through an advisory group recruited from an interest organisation. This group, consisting of three women with lived experience of termination for foetal anomaly, contributed to the study planning, interview design, recruitment strategies, and participant information materials. The study is reported in accordance with the COREQ checklist for qualitative research (Tong et al., 2007).
Sample and Recruitment
Participants were recruited using criteria-based purposive sampling through the Norwegian SIDS and Stillbirth Society (Landsforeningen for uventet barnedød, LUB). The organisation offers bereavement support and peer fellowship for grieving parents and engages in preventive efforts and research to reduce child mortality in Norway (Landsforeningen for uventet barnedød, nd).
Eligibility criteria were as follows: • Received serious prenatal information at an ultrasound examination in or around gestational week 18 • Experienced miscarriage or termination of pregnancy between gestational weeks 18 and 21 + 6 • Experienced a first late pregnancy loss • Experienced the loss within five years prior to the interview
Due to the small number of potential participants with experience of late pregnancy loss within this specific gestational window, recruitment through LUB was considered appropriate. Moreover, they had likely already reflected on and articulated their thoughts on their loss, enabling them to make an informed decision about volunteering for the study. Given the small population, the inclusion criterion was set at a maximum of five years since the loss.
A recruitment email was distributed through the organisation, and 36 individuals volunteered for the study. Following screening conversations by telephone, five participants were found to meet all inclusion criteria and consented to participate. The participants ranged in age from 29 to 39 years (mean age 33.8), and all identified as Scandinavian.
Sample adequacy was considered in relation to the specificity of the study aim, the narrowly defined eligibility criteria and difficult-to-recruit study population, as well as the depth, adequacy and information richness of the interviews conducted.
Data Collection
Individual in-depth qualitative interviews were conducted online via Microsoft Teams by the first author and lasted between 90 minutes and 3 hours. Participants were interviewed in their homes to enhance their sense of safety, privacy, and autonomy.
A semi-structured interview guide (Supplemental file 1) was developed to allow a flexible approach enabling the participants to narrate their experiences in their own words. The guide consisted of broad, open-ended questions concerning the pregnancy and loss trajectory, encounters with healthcare professionals, decision-making, post-loss experiences, coping, and support needs. Suggested prompts were used flexibly to explore issues raised by each participant. They were invited to start with their present situation and then reconstruct the sequence of events surrounding the loss, including their interactions with healthcare professionals. The aim was not to establish a factual reconstruction of events but to explore how the encounters were experienced, interpreted, and remembered. No participants withdrew from the study.
Data Analysis
All interviews were transcribed verbatim by the first author, resulting in 119 pages of transcripts. The analysis was based on Braun and Clarke’s (2022) reflexive thematic approach, which treats researcher subjectivity as an analytic resource and emphasises an iterative process that enables in-depth engagement with the data.
The analysis proceeded through several stages. First, transcripts were read repeatedly to gain familiarity with the material, supported by field notes from the interviews. Initial codes were generated inductively through close reading, focusing on recurring meanings, experiences, and language use. Coding was first conducted within each interview as a vertical analysis, then across interviews as a horizontal analysis, to identify shared patterns and variations.
Codes and preliminary themes were discussed collaboratively among the authors and refined through iterative comparison with the data in several analytical workshops. Discrepancies in interpretation were resolved through dialogue and re-examination of transcripts. Analytic notes and reflexive discussions documented the development of codes and themes. The final analysis resulted in four theme clusters with associated sub-themes, representing participants’ experiences of key moments in their stories. Participants did not provide feedback on the findings.
Researcher Reflexivity
Reflexive thematic analysis acknowledges and values researchers’ impact on the research process (Braun & Clarke, 2022), necessitating a critical examination of the researchers’ roles. The four female authors have complementary experiential and professional backgrounds, contributing interdisciplinary insights related to pregnancy loss. The first author, Follestad, is a trained nurse with a master’s degree in mental health care and extensive counselling experience in reproductive care. The second author, Kalstad, is a trained grief counsellor and cognitive therapist with extensive experience in bereavement support and is employed by LUB. The third author, Christoffersen, is a professor with experience in social science methods and healthcare research and expertise in parental experience of loss. The fourth author, Berg, is an associate professor with a background in health and social sciences, particularly within medical sociology and qualitative studies of vulnerable groups’ life experiences.
Reflexive discussions were held throughout data collection and analysis to critically examine assumptions, emotional responses, and interpretive choices. This collaborative reflexivity functioned as a form of analyst triangulation, strengthening interpretive rigour and combining insider and outsider perspectives.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki (World Medical Association, 1964/2024) and approved by the Regional Committee for Medical and Health Research Ethics (REK) South East Norway (2021/288938). The collection and storage of personal data were approved by the Norwegian Agency for Shared Services in Education and Research (SIKT) (2022/742533), in accordance with the Norwegian Personal Data Act.
All participants received written and oral information about the study’s purpose and their rights as study participants, including confidentiality, and their right to withdraw from the study at any time. Written informed consent was obtained prior to participation. The participants have been given pseudonyms to ensure confidentiality.
Participation in research has been perceived as meaningful by many bereaved parents (Butler et al., 2018; Dyregrov, 2004). Nevertheless, given the emotional sensitivity of the topic, all participants were offered a follow-up conversation with a counsellor at LUB to ensure well-being after the interview.
Results
Themes and Sub-Themes
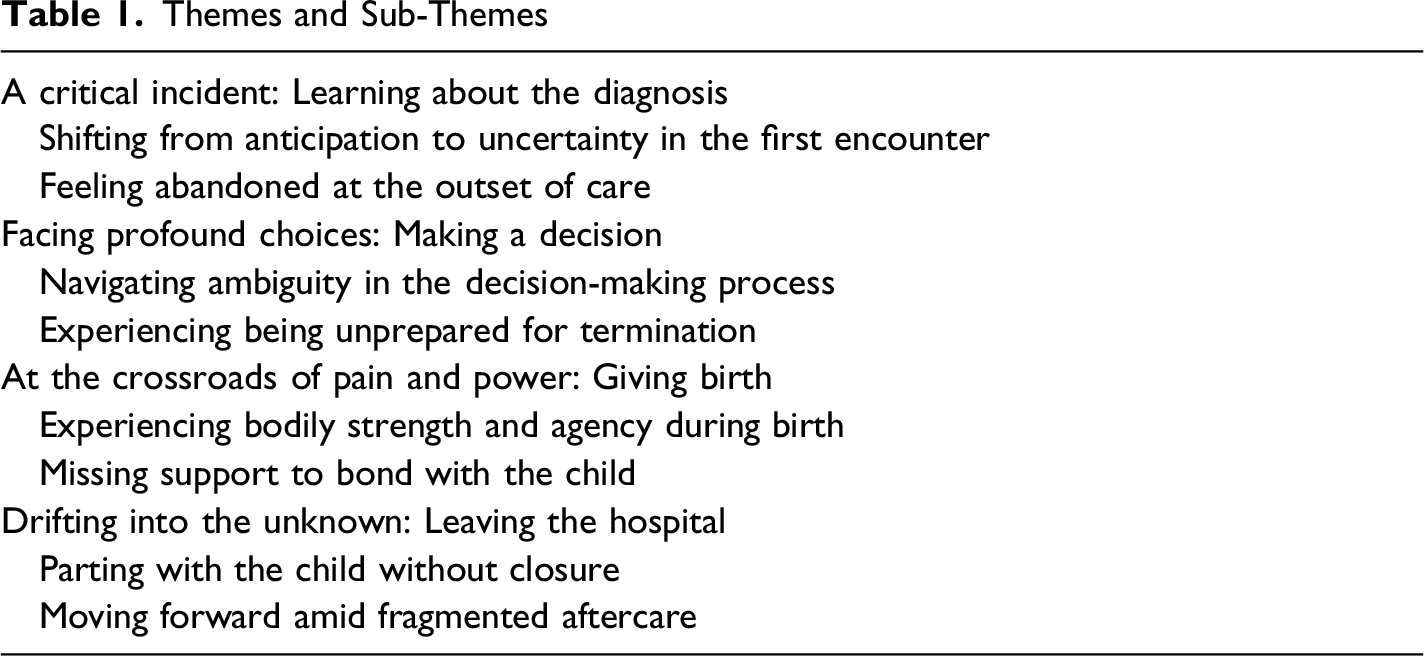
A Critical Incident: Learning About the Diagnosis
Shifting From Anticipation to Uncertainty in the First Encounter
The women in this study felt a strong attachment to the life growing within them. They approached the routine prenatal ultrasound at 18 weeks with anticipation, looking forward to meeting what they regarded as “their ‘babies’”. Expecting reassurance, they instead learned that something was wrong, sending them into a state of shock and emotional turmoil. The moment of diagnosis marked a profound rupture, transforming an anticipated confirmation into an experience of fear and uncertainty. It became the critical incident that initiated the subsequent care trajectory.
Sophia, whose baby was diagnosed with low amniotic fluid and foetal growth restriction, described how the experience overturned her sense of safety and their expectations: When we reached week 17, we were convinced nothing could go wrong, so we filled the house with baby equipment and built a baby crib. We were so happy and excited about the ultrasound… and leaving the hospital felt like our world had been turned upside down. (Sophia)
Similarly, Vera, who had experienced a miscarriage one year earlier, was devastated upon learning her baby had a heart defect, no kidneys, and no amniotic fluid: We thought everything was fine, because we went to four ultrasounds that showed nothing abnormal. I was in shock and could not comprehend what had gone wrong. (Vera)
All participants described this moment as an unreal, out-of-body experience. Their expectations of a normal family life were suddenly replaced by uncertainty and emotional upheaval, leaving them struggling to grasp the implications of the diagnosis.
Feeling Abandoned at the Outset of Care
As the participants attempted to absorb the unexpected diagnosis, they expected reassurance, guidance, or emotional support from healthcare professionals. Instead, they encountered a clinical environment in which medical terminology dominated the conversation, while their emotional needs remained largely unaddressed.
Vera expressed a strong sense of being left without support at the very outset of care: I wished they had something to offer me, someone to talk to. It was just a matter of ending the appointment and going home, left to digest everything that had been said on my own. (Vera)
The impersonal nature of these early encounters made participants feel like just another case within the system. Their transition from expectant mothers to patients facing possible miscarriage or termination occurred with little emotional scaffolding. This early lack of recognition and support contributed to feelings of abandonment and shaped how they approached the care that followed.
Participants described feeling disoriented and uncertain about what would happen next. They were referred for further investigations without receiving clear information. The shift from routine prenatal care to specialised foetal medicine thus unfolded as a continuation of an experience already marked by disruption and vulnerability.
Facing Profound Choices: Making a Decision
Navigating Ambiguity in the Decision-Making Process
After referral, hospital specialists confirmed or refined the initial findings, emphasising the severity of the diagnosis. Although extensive medical information was provided, participants experienced a lack of guidance on how to approach the termination decision itself. Being presented with life-altering choices without supportive discussion deepened their distress, as the ethical dimensions of the situation added a further emotional burden.
Struggling to navigate the complexity of the situation, participants expressed a strong need for certainty before making such a profound decision. They described feeling powerless in encounters with specialists, experiencing them as clinically detached and insufficiently responsive to their need for clarity and emotional support.
Some participants sought additional information independently. Mary and Sophia described turning to the internet and consulting external experts in an attempt to validate the information they had received and find reassurance. However, they encountered conflicting information, deepening their uncertainty. They found the emotional weight of the decision overwhelming as they struggled with the idea of ending a life that still might be viable.
Sophia captures the emotional impact of this period: When the doctor confirmed the news that our baby had a severe disease, our world seemed to spin out of control. I was on the verge of passing out, consumed by a sense of sheer panic. The doctor presented us with the choice of continuing the pregnancy or terminating it. He explained that due to the scant amount of amniotic fluid, a miscarriage was likely. Nevertheless, we held onto hope until the very last moment, grappling with mixed feelings and a tug-of-war between logic and the heart. (Sophia)
Mary described trying to envision her son’s prospective life and whether he had a realistic chance of survival. The burden of this decision felt crushing. While she clung to the hope of a ‘life worth living’, the phrase ‘incompatible with life’ echoed persistently, pushing her towards termination.
The notion of time emerged as a crucial factor for several participants. Although they appreciated the prompt referral to the hospital, they also felt pressured to decide before they were emotionally ready. They feared regretting a rushed choice yet simultaneously wanted to escape the painful situation. Ultimately, Mary, Vera, and Sophia decided to terminate their pregnancies, but all three reported a lingering sense of not having had enough time to fully process their emotions before proceeding.
For two participants, the pregnancy ended without an active decision. In Eliza’s case, the foetus died in utero, while Ruth experienced a miscarriage at 19 weeks after a period of indecision.
Eliza described this period as follows: I felt like I was being transported on an assembly line from one medical examination to another, receiving only technical and medical information at each stop, but no emotional support confirming the loss of a baby. (Eliza)
For the women who opted for termination, the legal requirement to seek approval from the Norwegian abortion committee initially provoked anxiety and fear of being judged. Contrary to their expectations, the committee meetings were experienced as respectful and supportive. Although the broader process was marked by isolation, the committee meeting provided a brief moment of reassurance and shared responsibility.
As Mary explained: I also felt that it was not only the two of us making the decision; in a way, they were part of it too, so we did not have to carry the decision entirely alone. It was not that I needed someone to take the responsibility away from me, but it felt reassuring not to be completely alone and to know that the professionals did not disagree with us. (Mary)
Committee members acknowledged the severity of their situation, adopted a neutral and non-judgemental stance, and provided clear, unbiased information. This recognition alleviated some of the ethical and emotional strain of decision-making and created a sense of shared responsibility. Although the broader process was marked by isolation, this encounter provided a brief moment of reassurance.
Experiencing Being Unprepared for Termination
Although the abortion committee’s validation provided a moment of relief, it did not lessen the emotional weight of the decision. As participants moved towards termination, they found themselves confronting new medical and emotional challenges.
They described the period between the final decision and giving birth as entering unfamiliar terrain, characterised by uncertainty and a lack of support to prepare for what lay ahead.
Eliza described her experience as this: I felt like I was being transported on an assembly line from one medical examination to another, receiving only technical and medical information at each stop, but no emotional support confirming the loss of a baby. (Eliza)
The participants noted a discrepancy between the clinical follow up, the language used in the care and their own understanding of the situation. Regardless of gestational age or prognosis, they viewed the foetus as their unborn child and a baby and compared their loss to stillbirth. Moreover, they perceived the seriousness of their loss as being measured by the duration of their pregnancy, leaving them feeling inferior to women who gave birth later in pregnancy. Mary perceived the clinical definition of viability as a threshold that resulted in different treatments for patients whose foetuses did not meet this threshold. She found it unfair that, in encounters with doctors and nurses, her termination was frequently referred to as a ‘late abortion’ rather than the birth of a baby. She felt deprived of the same rights and recognition as other bereaved mothers, despite experiencing a profound loss.
All participants felt positioned as patients yet desired to be treated more like expectant mothers, wanting to be recognised as women giving birth rather than as patients undergoing a procedure. Instead of prepared and guided, they experienced to navigate this transition largely on their own. The absence of clear information about labour and delivery heightened their anxiety and left them feeling unprepared for what lay ahead. As they approached childbirth, the need for recognition, guidance, and emotional support for an experience that held profound emotional and psychological significance became increasingly evident.
At the Crossroads of Pain and Power: Giving Birth
Experiencing Bodily Strength and Agency During Birth
In contrast to the turmoil of decision-making, childbirth offered a moment of clarity, shaped by the compassionate support of midwives who provided predictability and structure. The delivery room was perceived as a sanctuary where time seemed to stand still and events unfolded naturally under specialised care. During delivery, midwives used emotionally resonant words such as ‘baby’ and ‘birth’ rather than clinical terms such as ‘foetus’ and ‘abortion’. The participants felt that the midwives offered support, regardless of gestational age. They described giving birth as ‘a pause on the express train’: a precious opportunity to immerse themselves in the present and focus on a tangible task under the management of midwives. Eliza described this experience as follows: When I gave birth to my son, a wave of serenity washed over me, hormonally induced tranquillity that I had never experienced before. Despite the physical exhaustion and the mixed emotions, I felt a sense of joy and contentment. (Eliza)
The pain served as a catalyst, compelling participants to concentrate on the physical aspects of labour and reaffirming their identity as mothers. They attributed their heightened sense of control during childbirth to the plans, compassionate care, and support provided by the midwives. They felt that their identity as mothers going through labour and birth was legitimised, as opposed to feeling like patients undergoing medical procedures. For Sophia, giving birth became a turning point that fostered a sense of strength and resilience. The physical endurance required during labour seemed to momentarily restore a sense of control, offering respite from the emotional turmoil that had characterised the preceding period.
Despite knowing that their babies were unlikely to survive, the participants continued to hope for a different outcome. For some, this hope remained present until the moment of birth, when the reality of the loss became unavoidable. I had hope that until the baby was born, he would be healthy and alive, even though deep down I understood it would not happen. After he was born, I felt relieved it was over, before I slowly but surely realised that my baby was dead. In a way, this is how I would describe my existence at the time, moving in and out of reality and grief. (Mary)
Mary’s account highlights the tension between her rational understanding of the situation and the emotional attachment she continued to feel towards her child, particularly in light of the possibility of a live birth.
Missing Support to Bond With the Child
The transition from the deeply personal experience of giving birth to the impersonal nature of post-birth care felt stark and overwhelming. During labour and delivery, midwives played a key role in validating the participants’ identities as mothers who had lost their children. In those moments, participants were met with compassion and recognition, reinforcing their profound bond with their babies. However, this recognition was short-lived once the birth was over.
Mary’s account illustrates how small, embodied acts by midwives shaped opportunities for bonding: The midwife asked if she could place him on my chest while he was still warm… It felt strange emotionally during the circumstances. I felt happy, sad, and proud at the same time. During that precious time, I bonded with him. (Mary)
This moment of physical closeness affirmed Mary’s identity as a mother and created a tangible memory in an otherwise fragmented process. For most participants, however, such opportunities were not actively facilitated. They described how limited guidance after birth constrained possibilities for contact and memory-making, and some later regretted not having held their babies. Eliza expressed frustration over the hospital’s lack of initiative in offering simple mementoes, such as photographs, handprints, or footprints. As Ruth explained: They could have been more present, talked with us, and emphasised the importance of forming bonds, creating memories, and, well, everything… The only memory we have is his footprints. But no pictures. My best memory is from giving birth and seeing the baby again before the funeral. (Ruth)
Across the participants, opportunities to bond and create memories were perceived as more limited than those afforded to women who experienced loss later in pregnancy. This contributed to a sense of being treated differently, as if the legitimacy of their loss was implicitly linked to gestational age. The absence of these rituals and tangible memories compounded participants’ sense of loss and left them without visible proof of their motherhood.
Participants also described limited societal recognition of their need for connection and closure, which intensified their sense of isolation. The experience of the social legitimacy of their grief as being linked to gestational age. Sophia described how responses from others made her question whether her loss was considered sufficiently serious: I have struggled somewhat to accept my own grief because the pregnancy ended in week 21. People around us seemed very focused on how far along the pregnancy had been and on the idea that it could have been worse. But the grief is mine; I am the one who lost my child. (Sophia)
Rather than feeling supported in their grief, they were uncertain about whether their loss was acknowledged as worthy of mourning, leaving them emotionally disoriented and alone. This sense of devaluation was further reinforced by how some participants experienced their babies being handled. Acts such as placing babies in an aluminium bowl or wrapping them in a dirty towel were described as small yet deeply symbolic, intensifying participants’ pain and sense of invisibility.
Drifting Into the Unknown: Leaving the Hospital
Parting With the Child Without Closure
The parting with the child as an embodied experience of abrupt maternity as explained by Sophia: All these maternal feelings have been horrible. I had milk in my breasts, and for a while, I just wanted to run back… to find her again and have her on my chest. But I did not know where she was (Sophia).
Upon leaving the delivery room, the participants were immediately confronted with difficult emotions and decisions. They had to consider when to leave the hospital, whether to consent to a foetal autopsy, and how to arrange a funeral. Yet, healthcare professionals hesitated to provide clear guidance, leaving them unsupported and uncertain. Eliza asked for guidance about funeral arrangements but received none; she had to contact the church herself to discover her options.
After giving birth, participants experienced self-imposed pressure to leave the hospital, even though healthcare professionals did not explicitly ask them to do so. They perceived their losses as not warranting an extended stay. Although all five participants reported that they needed more time, this need was not actively recognised or accommodated, and they felt they were discharged too early, only a few hours after giving birth.
This premature departure left participants with a profound sense of losing control over the whereabouts of their babies and what would happen to them next. Three participants had to contact the hospitals to ask about the progress of the autopsy. This experience further reinforced their feelings of inferiority and the perceived disparity between their loss and that of others, intensifying their grief.
Mary and her partner were unwilling to leave their baby alone, and they sat in their car outside the hospital to remain near him. Similarly, Sophia struggled to come to terms with the separation from her baby: All these maternal feelings have been horrible. I had milk in my breasts, and for a while, I just wanted to run to the hospital… to find her again and have her on my chest. But I did not know where she was. (Sophia)
The early discharge and limited guidance surrounding the autopsy, funeral arrangements, and the whereabouts of their babies contributed to a profound sense of lost control. Rather than experiencing the separation as a supported transition, participants described leaving the hospital with unresolved questions and a lingering uncertainty about their role, rights, and connection to their child.
Moving Forward Amid Fragmented Aftercare
Participants’ felt that the aftercare they received was fragmented and fell significantly short of their needs. The lack of proactive and organised support further intensified the weight of their losses. Ruth described this experience as follows: I felt we were swimming in a full glass of chaotic bubbles. We were promised a call from the hospital after returning home, but no one called. We needed someone to talk to after the worst chaos had settled, but we had no one. It was easy to use alcohol and sleeping medication to endure the hollow, lonely feeling and get through the days and nights. (Ruth)
Participants felt that their grief was disregarded and that they lacked the attention and care they needed. Eliza described feeling abandoned when she approached healthcare professionals for follow-up: It was incredibly frustrating that no one seemed to fully understand my situation. It was like having three massive elephants perched on my chest, refusing to budge. They were heavy, stubborn, and suffocating, leaving me gasping for air. (Eliza)
In the absence of sufficient professional support, participants actively sought ways to legitimise their grief and maintain a connection to their child. They described constructing narratives around their loss, assigning their child a social and emotional status in an effort to integrate the loss into their lived experience. Through voluntary support networks, participants found a space where they felt understood, validated, and empowered to address their needs and cope with their grief.
Participants also described prolonged uncertainty related to the autopsy process. The wait of two to eight months for confirmation of the cause of death was experienced as emotionally taxing. For four participants, the autopsy confirmed the prenatal diagnosis, leaving them to question the necessity of such a long wait.
Having a grave to visit provided a tangible location through which the relationship with the child could be maintained. As Ruth explained: It was comforting simply to sit there and think about the life that did not happen. It was a place that was, in a way, ours. He is part of us, and he always will be. (Ruth)
A physical place of rest became central to regaining a sense of control and continuity. Vera regretted choosing a memorial garden, while Ruth rejected this option, emphasising the need to know her son’s exact whereabouts. For Eliza, a sense of closure only became possible after the funeral, when her baby was given a tangible resting place. As stated: “Knowing that my baby had a place to rest and proof of his existence was a great relief. It was comforting to have a physical location to visit and remember him by” (Eliza).
Discussion
Across the four key moments identified in the results – receiving the diagnosis, navigating the decision-making process, giving birth, and leaving the hospital – the participants’ experiences were shaped by variations in medical language, emotional support, guidance, and continuity of care. A central finding is that recognition of their loss and maternal identity was inconsistent across the care trajectory. Participants felt recognised as mothers in some encounters, particularly during birth, while later experiencing a lack of recognition through fragmented aftercare, unclear information, and limited institutional support.
The women’s interactions with healthcare professionals played a pivotal role in shaping their emotional adjustment. The abrupt transition from hopeful expectations to loss and grief was largely experienced as unsupported, leaving participants feeling without emotional support. This aligns with previous findings that healthcare communication can profoundly influence parental well-being following pregnancy termination for foetal anomaly and perinatal loss (Brann et al., 2019; Heaney et al., 2022; Lafarge et al., 2017).
The findings highlight language as a central mediating factor in the women’s experiences of care. A recurring theme across accounts was a linguistic tension between the women’s own understanding of the loss as that of a baby and the clinical and procedure-oriented language often used by healthcare professionals. This tension can be understood as a form of cognitive dissonance (Goldblatt Hyatt, 2021), in which conflicting interpretations of the loss coexist without being fully reconciled. Thus, language functioned not merely as a communicative tool but as a framework through which the loss, grief, and maternal identity were legitimised or undermined.
Importantly, the participants’ experiences illustrate that clinical language was not necessarily alienating in itself. Some encounters were characterised by healthcare professionals’ ability to combine clear clinical explanations with emotionally attuned language, fostering a sense of recognition and support. This finding aligns with previous studies demonstrating that effective and compassionate communication throughout the care trajectory crucially shapes the extent to which parents feel supported and able to adapt to their loss (Austin et al., 2021; Heaney et al., 2024). Where such acknowledgement was present, language served as a bridge between practice and lived experience.
Conversely, when clinical language dominated without corresponding emotional recognition, participants described increased feelings of alienation, uncertainty, and self-doubt. This linguistic mismatch appeared to amplify the perceived distance between the women’s own meaning-making and the healthcare system’s framing of loss. The contribution of clinical or procedural language to parents feeling that their grief was insufficiently recognised has been reported elsewhere (Atienza-Carrasco et al., 2020; Jones et al., 2017; Kjelsvik et al., 2026). In the present study, the failure of language to acknowledge the women’s emotional reality emerged as a key factor in undermining the perceived legitimacy of both grief and maternal identity.
The decision-making process itself emerged as ethically and emotionally complex. Participants sought clarity and certainty yet often encountered what they perceived as clinical detachment. While some described receiving clear and thorough medical information, it was frequently accompanied by a lack of emotional and psychological support during a phase marked by profound moral and existential considerations. This aligns with research showing that parents facing termination for foetal anomaly often receive conflicting medical opinions and insufficient decision-making support (Cullen et al., 2018; Heaney et al., 2022) and a lack of emotional and psychological support (Hanschmidt et al., 2016).
The findings also point to time as a central dimension of decision-making support. Participants needed time not only to understand medical information but also to emotionally comprehend the implications of the diagnosis and the decision ahead. The tension between clinical urgency and emotional readiness contributed to a sense of being rushed, even when referrals were prompt. This suggests that timely care should not be understood solely as rapid access to specialist assessment but also as the provision of sufficient time and support for emotional processing.
The women who contacted the abortion committee found the encounter validating, particularly through the shared or acknowledged responsibility for the decision, in line with findings reported by Kerns et al. (2018). However, this positive appraisal may be understood partly in light of contrary expectations: that the committee would act as a barrier rather than as a source of recognition. This appraisal thus appears closely related to participants’ need for moral and institutional legitimation during an especially vulnerable phase.
In contrast to earlier moments in the care trajectory, birth emerged as a moment in which participants could reclaim a sense of agency through the body. While decision-making was marked by uncertainty, moral ambiguity, and dependence on medical authority, labour offered a tangible task in which the women could act, endure, and be recognised as mothers. Midwives played a crucial role in this process by using affirming language, providing structure, and offering relational support. Birth after late termination or miscarriage should therefore be understood not only as a clinical endpoint but also as a potentially meaningful event in which maternal identity and the child’s reality may be affirmed. This aligns with previous studies highlighting the role of midwives in perinatal loss care (Helps et al., 2020; Lyus et al., 2014), as well as with Erato et al. (2022), who suggested that birth may reinforce maternal identity for some women.
However, this recognition was often short-lived. A key finding in this study concerns participants’ experiences of insufficient post-birth care. While support during labour was often described as attentive and compassionate, postnatal guidance and emotional care were largely absent. Participants described the absence of follow-up contact, information about grief reactions, and referral to support services as particularly distressing, leaving them feeling abandoned and emotionally unprepared after discharge. In line with Lafarge et al. (2017), our findings suggest that insufficient guidance limited the women’s opportunities to create meaningful memories and begin processing their grief. These experiences are consistent with studies linking inadequate bereavement care to prolonged psychological distress and adverse long-term outcomes (Hodgson & McClaren, 2018; Kersting et al., 2013).
The findings further show that post-birth care involved more than emotional follow-up. For several participants, uncertainty about the baby’s whereabouts, autopsy procedures, funeral arrangements, and opportunities for memory-making intensified the sense that their maternal role had been interrupted or disregarded. Bodily experiences, such as lactation, further reinforced maternal attachment in the absence of the child. These accounts suggest that the post-birth period is a critical phase in which recognition of motherhood, grief, and relational bonds may be either supported or undermined.
Memory-making practices appeared to serve a function beyond emotional coping. Photographs, handprints and footprints, time with the baby, funerals, and graves provided tangible confirmation that the child had existed and that the woman’s motherhood was real. When such opportunities were absent or insufficiently supported, participants were left with not only grief but also a lack of material and social evidence through which the loss could be recognised. In this sense, memory-making and ritualisation became central to legitimising both the child and the grief.
The participants’ accounts can be understood considering the concept of disenfranchised grief, where losses are insufficiently recognised or legitimised within institutional and social contexts (Diamond & Diamond, 2016; Hendriks & Abraham, 2022). Their frustration regarding limited legal and institutional recognition further illustrates how structural frameworks may contribute to experiences of invisibility. In Norway, late termination of pregnancy before the threshold of viability does not afford the same rights as stillbirth beyond 22 weeks, and some participants interpreted this distinction as undermining the legitimacy of their loss. Similar experiences have been reported in other studies, where women experiencing perinatal loss before viability often felt excluded from bereavement protocols (Giannatiempo et al., 2024; Ramdaney et al., 2015). At the same time, the significance attributed to legal status varied among participants, and not all expressed the same need for formal or legal recognition. These differences underscore how experiences of loss and grief are shaped through the interplay of institutional practices, legal frameworks, and individual meaning-making processes.
Beyond formal and material forms of recognition, participants also engaged in narrative and social forms of meaning-making. In response to limited institutional support, they sought to construct personal narratives and connect with bereavement networks to validate their experiences. Research suggests that meaning-making is essential for integrating perinatal loss into personal and social realities (Lafarge et al., 2013b; Neimeyer et al., 2006). In this study, these efforts appeared to compensate for gaps in professional follow-up and formal recognition.
Providing effective emotional support in situations of late pregnancy loss may, however, be particularly challenging for healthcare professionals. In a recent review, Lee et al. (2023) found that health professionals themselves reported a need for additional training to feel confident in knowing what to say, as well as a limited ability to provide sufficient, culturally appropriate, and individualised bereavement care and follow-up. Furthermore, these professionals identified emotional fatigue, time constraints, and organisational factors as barriers to holistic care. These findings align with the women’s experiences of fragmented and inconsistent care in this study, which may be understood in light of the complex and layered services in which healthcare is provided; the women often encountered multiple healthcare professionals across the care trajectory.
Although practical guidance on how to offer psychological support in such situations has recently become increasingly available (Fox et al., 2026), many women continue to report dissatisfaction with the emotional care they receive, as reflected in our findings and those of Kjelsvik et al. (2026) and Kristiansen et al. (2026). This apparent gap may suggest that, while there is broad agreement about the importance of emotional support, there is less clarity about how such support should be delivered. Interventions intended to be supportive may be experienced as inadequate or even distancing, particularly when not attuned to individual needs and contexts. Thus, the challenge may lie not in recognising women’s needs but in translating this knowledge into consistent, sensitive, and contextually appropriate care throughout the care trajectory. Furthermore, it may be questioned whether these needs can be adequately met within current healthcare structures, or whether complementary measures are needed, such as multidisciplinary approaches and individualised care plans, as suggested by Fox et al. (2026).
Overall, the findings suggest that late pregnancy loss following serious prenatal findings is shaped by both individual grief and the interpersonal encounters and institutional practices that determine which losses are recognised, supported, and ritualised. The variability of recognition across the care trajectory may help explain why the participants described their experiences as fragmented, isolating, and difficult to integrate into their lives.
Strengths and Limitations
By drawing on rich, descriptive interview data, the study illuminates how women experienced encounters with healthcare professionals at key moments across the care that informs both clinical practice and policy development. Although the sample was small, the interviews provided rich and detailed first-hand accounts that enabled an in-depth exploration of participants’ experiences. The integration of user perspectives through an advisory group of women with lived experience is another strength of the study.
The study also has limitations. First, recruitment relied exclusively on LUB, which may have introduced sampling bias. Participants had already sought contact with a bereavement organisation and may therefore have had more opportunities to reflect on and articulate their experiences than women without such support. Their accounts may also have been shaped by stories shared by other bereaved women, which could have contributed to more critical or elaborated descriptions of healthcare encounters.
Second, the interviews represent retrospective accounts of loss experiences, with time since loss ranging from several months to several years. While this may have influenced how events were remembered and narrated, such retrospective meaning-making was considered analytically relevant, as it highlights which encounters and forms of language remained salient over time.
Finally, including the perspectives of partners or healthcare professionals could have provided a more holistic understanding of encounters between parents and healthcare professionals following serious prenatal findings and late pregnancy loss.
Implications for Practice and Policy
The findings underscore the need for healthcare professionals to balance clear medical information with emotional support, recognising both the medical and existential issues involved. Healthcare professionals should receive training in how to integrate clinical and emotionally attuned communication to ensure that parents are both well-informed and emotionally supported as they grieve. This training should also address how healthcare professionals can support bereaved women in maintaining a connection with their baby, including practical guidance on memory-making after birth and information about funeral arrangements. Such practices may help parents integrate their baby into their family narrative and provide tangible recognition of the loss. Normalising women’s emotions by informing them about the range of feelings and reactions experienced by other parents in similar situations may also foster a stronger sense of security and autonomy.
Using more compassionate language and a more empathetic approach to care can empower women to feel entitled to grieve. Healthcare professionals should recognise women both as mothers who have lost a child and as patients in need of medical care. Validating this dual experience in healthcare could provide better support and understanding, enabling women to process their loss in a meaningful way.
The findings support the need for an integrated, compassionate, and continuous model of care for women experiencing late termination of pregnancy, intrauterine foetal death, or miscarriage after serious prenatal findings. This model should include national guidelines for psychosocial care and post-hospital follow-up to ensure trauma-informed care. Such guidelines could help bridge the gap between labour, and post-birth bereavement care. The findings also highlight the need for structured follow-up services, such as counselling and support groups, to ensure that women receive recognition and care beyond hospital discharge.
Conclusion
This study highlights the complex and often contradictory experiences of women receiving serious prenatal information around gestational week 18, followed by late termination of pregnancy, intrauterine foetal death, or miscarriage. Participants navigated a fragmented healthcare system, moving between medical and emotional narratives that shaped their understanding of the pregnancy, the child, and the loss.
A key insight is that recognition was not simply present or absent, but varied across the care trajectory. It was often undermined by fragmented aftercare, unclear information, and limited institutional support. This instability of recognition contributed to uncertainty about maternal identity, the legitimacy of participants’ grief, and their ability to integrate the loss into their lives. These findings underscore the need for a more integrated model of care that bridges medical and emotional support across the entire care trajectory.
The study contributes to existing literature by illustrating how fragmented communication, unstable recognition, and inadequate follow-up may affect women’s psychological well-being after late pregnancy loss. Addressing these gaps requires systematic improvements in bereavement care, as outlined in this study. Future research should include the perspectives of fathers and partners, as well as the impact of legal and institutional frameworks on parental grief.
Supplemental Material
Supplemental Material - The Right to Grieve: Norwegian Women’s Experiences of Care During Termination of Pregnancy in Second Trimester
Supplemental Material for The Right to Grieve: Norwegian Women’s Experiences of Care During Termination of Pregnancy in Second Trimester by Hege Sofie Follestad, Trine Giving Kalstad, Line Christoffersen, Anita Berg in Journal of Death and Dying
Footnotes
Acknowledgements
The authors would like to thank the participants for their time and stories from first-hand experience, and the advisory group for their comments and suggestions.
Ethical Considerations
The research was conducted in accordance with the World Medical Association Declaration of Helsinki Principles for Medical Research in Human Subjects (2024). Ethical approval was obtained from REK (REK 2021/288938). Personal data management was approved by the Norwegian Agency for Shared Services in Education and Research (SIKT 2022/743533).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Stiftelsen Dam (grant number 2020/HE2-337288). Stiftelsen Dam is one of Norway’s largest foundations financially supporting health and research projects. The foundation aims to improve public health through initiatives focused on participation, activity, and empowerment. The funding sources had no role in the study design, data collection, analysis, interpretation, or decision to submit the results for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, due to the sensitive nature of the research, so supporting data are not available. Underlying data can be made available upon reasonable request.
Disclosure
No generative AI tools has been used in the writing of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
Note
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.