
Abstract
This study reports on the development, reliability, and validity of a new instrument for obtaining respondents’ body image perception, the Brazilian Photographic Figure Rating Scale (BPFRS). This instrument consists of eight photographic images (seven distorted and one accurate) of respondents themselves in standardized poses, taken just prior to requesting respondents to make self-ratings on the instrument. Participants involved in developing and evaluating this instrument were 142 Brazilian women (age 21.8 ± 3.0 years). Ten experts assessed content validity and showed high agreement (defined by ratings of 4–5 on a 5-point scale) with items measuring underlying constructs and high (>70%) interrater agreement. A Pearson correlation demonstrated convergence between the BPFRS and other related scales; a positive correlation was also evident between actual and respondent-perceived body mass index. Both test–retest and Kappa confirmed temporal stability. These findings indicate that the BPFRS can accurately and reliably assess body image dissatisfaction and body perception in young women by deploying realistic, personalized images as stimuli for self-ratings. Implications for further research and treatment of body image problems are discussed.
Introduction
Body image is a multidimensional construct comprising perceptual (McCabe, Ricciardelli, Sitaram, & Mikail, 2006) and attitudinal dimensions (Pruzinsky & Cash, 2002). Adami et al. (2012) point out that alterations in body image can be considered a risk factor that may harm social, professional, emotional, and even psychological health through, for example, eating disorders (Cash, 2011; Gardner, 2011), depression (Johnson & Wardle, 2005), chronic dysphoria (Rosenström et al., 2013), and suicide (Rodriguez-Cano, Beato-Fernández, & Llario, 2006).
In recent years, interest in evaluating body image has stimulated the development of several tools, the most widely used being Silhouette Scales, which are quick, easy, and inexpensive to apply (Cash, 2011; Gardner & Brown, 2010a). However, weaknesses in these instruments have been identified in the literature, including (a) unrealistic images of the human body, (b) unrealistic values of body height and weight of the target population, (c) unverified psychometric qualities, and (d) a lack of silhouettes able to assess perceptions and attitudes simultaneously (Gardner & Brown, 2010a).
One strategy used to minimize potential errors is to use instruments developed from real anthropometric measures. Body mass index (BMI), one of the most commonly used measures, associates with body dissatisfaction (Austin, Haines, & Veugelers, 2009; Conti, Frutuoso, & Gambardella, 2005; Gardner & Brown, 2011; Graup et al., 2008; Kakeshita, Silva, Zanatta, & Almeida, 2009; Laus, Miranda, Almeida, Costa, & Ferreira, 2012; Pallan, Hiam, Duda, & Adab, 2011). Women tend to desire a slim body (Laus et al., 2012). Brazilian women, on average, wish to reduce body weight by 2 kg in order to feel content and beautiful (Alvarenga, Dunker, Philippi, & Scagliusi, 2010). Men, on the other hand, derive more body satisfaction from muscle gain (Kakeshita et al., 2009). In both cases, the body alterations are reflected in BMI changes. Other researchers have aggregated other anthropometric parameters in body image evaluation tools (Crossley, Cornelissen, & Tovée, 2012; Fran, Liu, Wu, & Dai, 2004), such as fat percentage (Corseuil, Pelegrini, Beck, & Petroski, 2009; Damasceno et al., 2012; Pallan et al., 2011) and waist–hip ratio (Graup et al., 2008).
Since the late 1970s, numerous technological devices have been developed to evaluate body perception and dissatisfaction (Gardner, Martinez, & Sandoval, 1987; Gardner & Moncrieff, 1988; Gardner, Morrell, Watson, & Sandoval, 1989). Guided by psychophysical tools, some authors have proposed such strategies to evaluate body image as the Method of Limits, Method of Constant Stimuli, and Adaptive Probit Estimation (Gardner & Boice, 2004; Gardner & Bokenkamp, 1996). Using processes of detection, discrimination, and assignment of magnitude, psychophysical tools seek to relate stimuli, sensations, and perceptions functionally (Gardner & Brown, 2010a); to express the internal organization of perceptive experience; and to generate results that can be systematically analyzed and interpreted (Da Silva & Ribeiro-Filho, 2006).
We sought to develop a more ecologically valid measure by introducing respondents to actual front- and side-view images of their own body, thus providing very personalized reference stimuli from which to solicit respondent self-perception ratings. We believe this measure will improve body image assessment by adding realism and eliciting a higher level of engagement from respondents while providing an accurate assessment of body dissatisfaction and body perception. Thus, this study aimed to first develop and then assess the psychometric properties of a new instrument, the Brazilian Photographic Figure Rating Scale (BPFRS), by using images of the subject’s own body to evaluate the subject’s body dissatisfaction and perception.
Method
Participants
A sample of 142 adult women (21.8 ± 3.0 years; BMI 23.76 ± 4.42) chosen from a university enrollment database were contacted via e-mail. Women have been identified as more susceptible than men to distorted and unhealthy body image. Young women may be more vulnerable to broad impact from their body-related feelings, beliefs, and behaviors (Laus et al., 2012; Runfola et al., 2013; Slevec & Tiggemann, 2011; Swami et al., 2010). The use of women in this study also enabled our results to be compared with those of similar studies in other countries (Swami, Salem, Furnham, & Tovée, 2008; Swami et al., 2012).
Following prior literature addressing influential factors in tests of perception such as physical exercise, mood, anxiety, and so forth (Cash & Pruzinsky, 2002; McCabe et al., 2006), we excluded people who had (a) exercised in the 3 hours before the test, (b) experienced atypical sleep (insomnia or altered sleep) the night before the test, or (c) suffered an emotional provocation on the day of the test (e.g., bad mood, anxiety, sadness, euphoria, muscle pain, or premenstrual tension). Each participant was questioned directly on these criteria before the test. All participants signed a Declaration of Informed Consent, in compliance with the ethical procedures required to perform the study, and the study was approved by the Ethics Committee of the Universidade Estadual Paulista—Rio Claro Campus/São Paulo, under Protocol No. 298 and Decision No. 071/2012.
Materials and Procedures
Each participant’s body weight and height were measured using, respectively, a Tannita digital platform scale (precision 0.1 kg) and a Sanny stadiometer with movable head (precision 1 cm). These measurements were used to calculate BMI, defined as the ratio of body weight to height-squared. Each participant completed two previously researched instruments for evaluating body image: (a) the Brazilian Silhouette Scale for Adults (BSSA) comprises 15 figures with characteristically Brazilian body shapes, with a test–retest correlation coefficient between actual BMI and perceived BMI of r = .84 (p < .01; Kakeshita et al., 2009); and (b) Stunkard’s Figure Rating Scale (SFRS), the original version of which was designed by Stunkard, Sorensen, and Schlusinger (1983) and, in validation for Brazilian women, returned good concurrent (r = .76; p < .0001) and discriminant, χ2(1) = 19.2; p < .005, validity. It comprises nine silhouettes, in order of increasing size, on a single card (Scagliusi et al., 2006). On both scales, dissatisfaction is defined by the difference between perceived and desired silhouettes. Non-zero values equated to dissatisfied individuals such that positive values indicated dissatisfaction with being overweight and negative values indicated dissatisfaction with being underweight.
To construct the BPFRS for this study, we involved participants in a series of steps as detailed below:
Image capture
Full-body photographs were taken of each participant in a laboratory previously prepared with suitable lighting and a dark backdrop. Each participant, wearing black shorts and a sleeveless top of Lycra-like adherent material (so as define body outline), was photographed from the front, with arms in a neutral position and, from the side, with shoulders slightly extended and legs spread apart to hip width. Photographs were prepared and displayed using a Sony Cyber-shot camera, HP Pavilion notebook with 14-inch screen, and Photoshop CS3 Extended (Adobe®) image manipulation software.
Construction of stimuli and preparation of tasks
Construction of the BPFRS was guided by existing human silhouette scales (Conti et al., 2013; Gardner, 2011; Gardner & Brown, 2010b; Gardner, Jappe, & Gardner, 2009; Kakeshita et al., 2009; Stunkard et al., 1983; Swami et al., 2008) and the theory of psychophysics (Da Silva & Ribeiro-Filho, 2006). Following guidelines from Gardner, Friedman and Jackson (1998), we opted for the minimum number of stimuli that gave the greatest number of possibilities for the chosen parameter (BMI, in our case), establishing a constant increment ratio with little distortion between stimuli and keeping the height of the silhouettes constant.
We chose eight stimuli (seven distorted images and an undistorted image) within the range 16.5 kg/m2 > BMI < 40 kg/m2, from extreme thinness to obesity (World Health Organization, 1995). To define the first stimulus in percentage terms, we used simple proportionality: The participant’s BMI represented 100%, and the lower limit (in our case BMI of 16.5) was the unknown variable in the equation. The same process was applied to establish the final stimulus, the upper limit (BMI of 40). As the feeling-stimulus ratio obeys the logarithmic law, the percentage values were converted into logarithms to specify the other stimuli. Thus, the logarithmic value of 65.5%, for example, is 1.81 (see Figure 1).
Calculation of increment ratio – for a subject with BMI 25.2 kg/m2. +final stimulus, CurrencySign initial stimulus, ¥number of stimuli, and °increment value.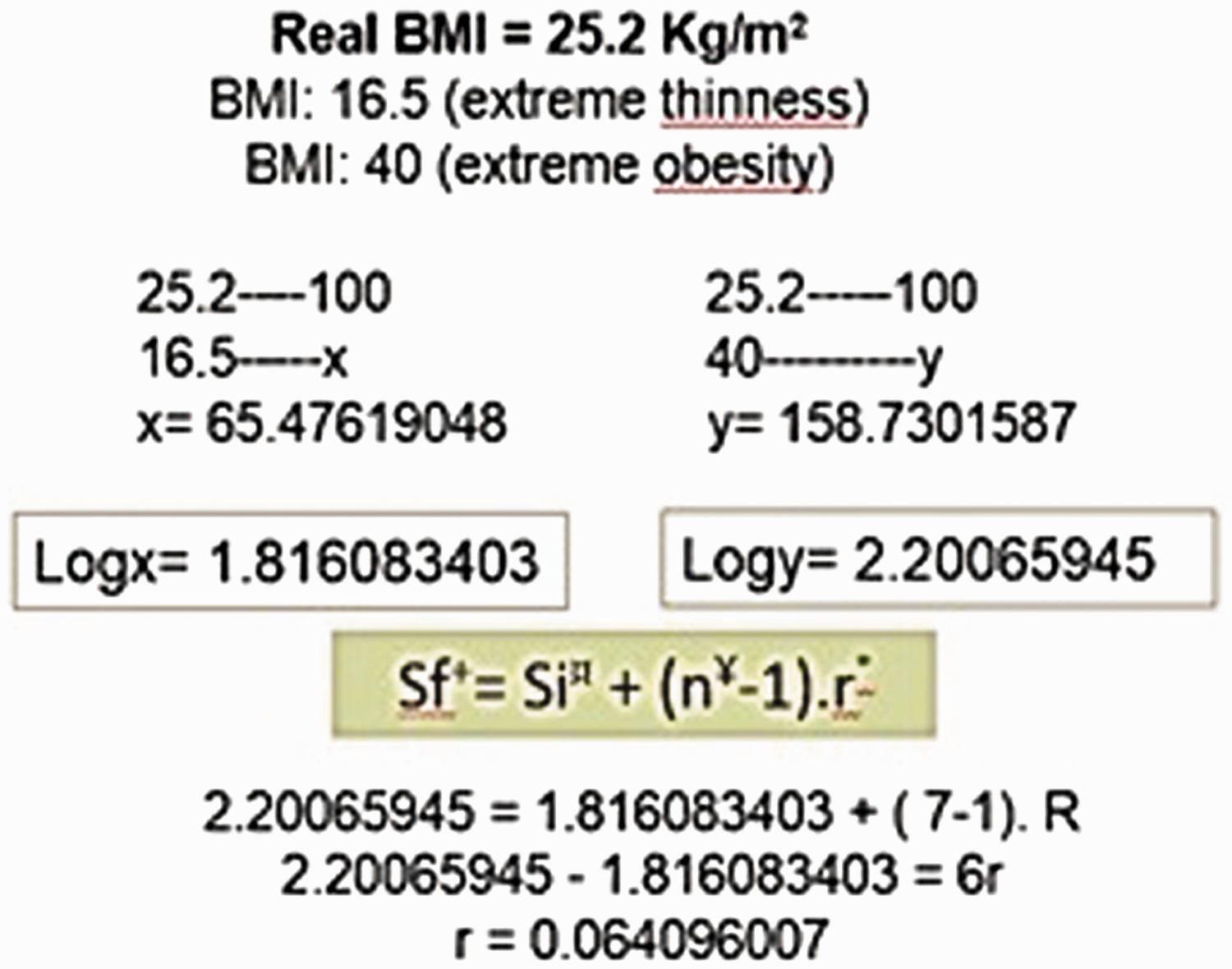
The increment ratio (r), the minimum change necessary for the difference to be noticeable, was calculated from the equation: Sf = Si + (n − 1) r (Da Silva & Macedo, 1983), where Sf is the value of the final stimulus (40 kg/m2), Si is the value of the initial stimulus (16.5 kg/m2), and n is the number of stimuli. The distortion increment value from one silhouette to another was 0.064 kg/m2 (Figure 2), equivalent to 1.57% (antilog). From the initial and increment ratio values, it is possible to calculate the other stimuli, which were converted to percentages, by calculating their antilog, indicating the distortion value for each photographic image (Figure 2).
Calculation of stimuli. *Stimuli.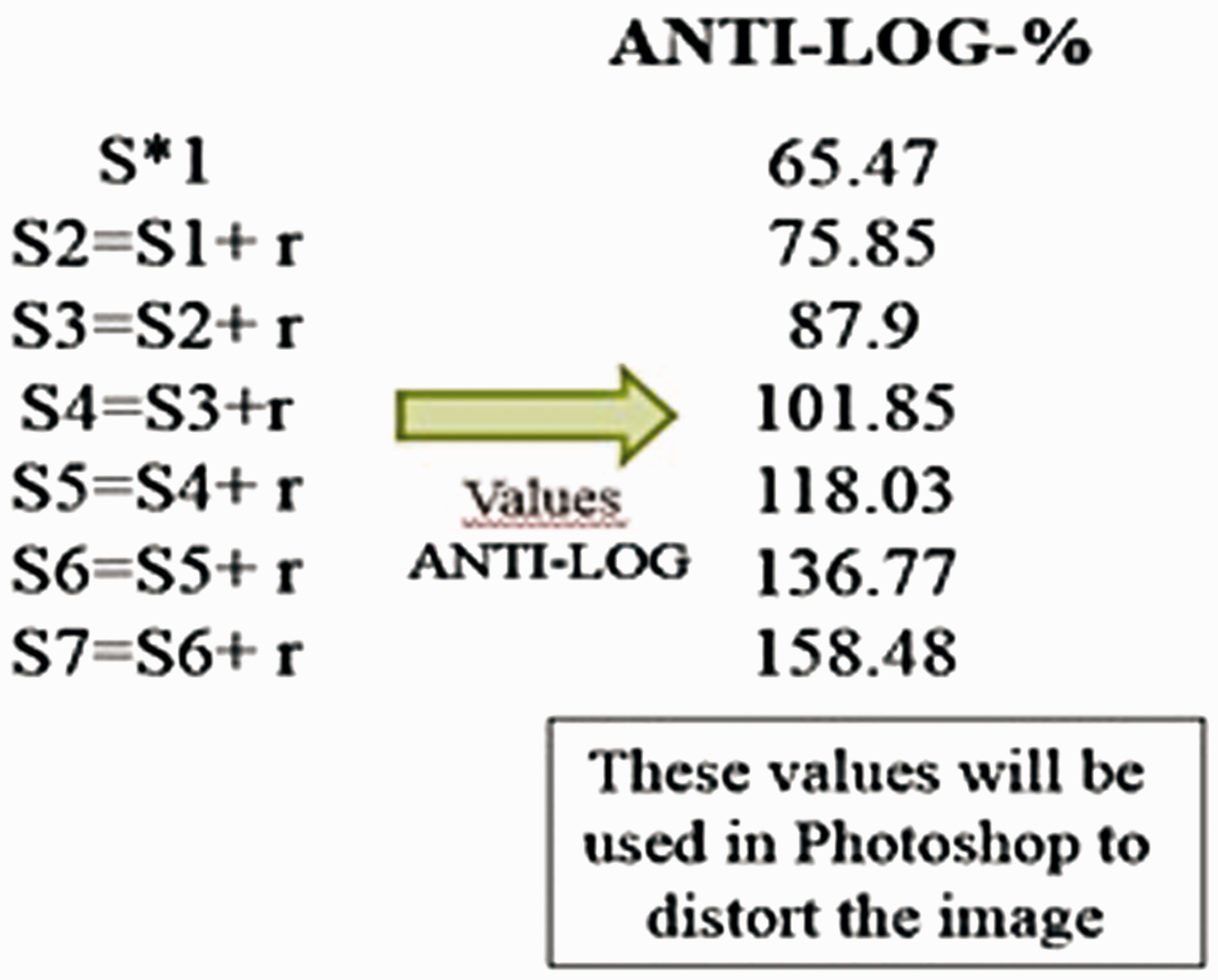
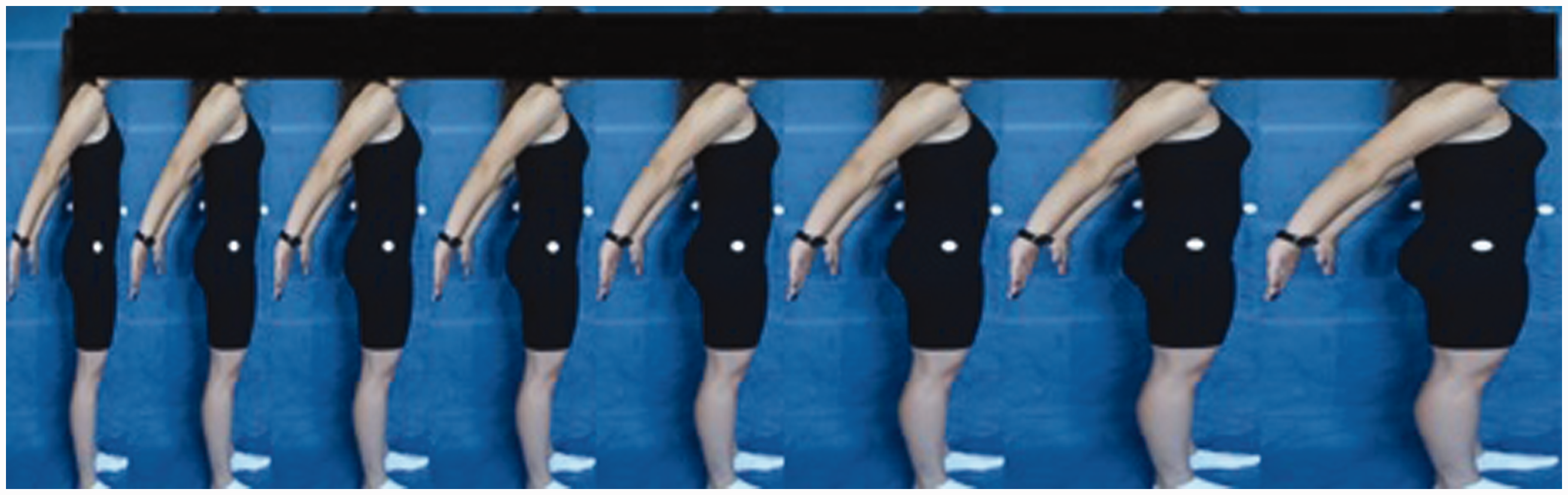
The undistorted image was treated using Photoshop CS3 Extended (Adobe®) software to compose seven distorted stimuli. These were arranged in ascending percentage order, with the participant’s undistorted image considered to represent 100%. Thus, the placing of the undistorted image depended on a participant’s BMI. In our example, the undistorted image was placed fourth. The eight juxtaposed stimuli form the front-view and side-view BPFRS, individualized for each participant (Figures 3 and 4). Preparation of each individual test, spanning the whole process described earlier, from calculation of the stimuli, manipulation (distortion) of the images, and their grouping in ascending order of size, took an average of 30 minutes.
BPFRS front view—The scale of distorted stimuli plus the image of the individual’s body without distortion. BPFRS side view—The scale of distorted stimuli plus the image of the individual’s body without distortion.
Application of the BPFRS
Each participant, after viewing their BPFRS, was asked to (a) “Choose the silhouette that best represents your real body” and (b) “Choose the silhouette that best represents the body that you would like to have.” Only one choice was allowed to apply to both front and side views. That is, for each question, if the participant wanted to choose a front-view option (for example, Image 3) and a different side-view option (Image 4), they were asked to choose only one of these options.
Body dissatisfaction was defined by the ordinal difference between the silhouettes representing the participant’s actual and desired bodies. Similarly, body size and shape perception index was calculated by subtracting the silhouette perceived as representing the actual body from the participant’s actual silhouette. Thus, dissatisfaction and the perception index may be considered as units from −7 to +7 and BMI values from −23.5 to 23.5. The value corresponding to zero was parameterized to represent satisfaction and precision in body perception. Any non-zero number indicated dissatisfaction and imprecision in body perception. Positive values indicated dissatisfaction due to excess weight and overestimation of body size. On the other hand, negative values denoted dissatisfaction due to low weight and underestimation of body size. The rating instrument took around five minutes to apply for each participant, as they were easy to understand.
Assessment of the Psychometric Qualities of the BPFRS
Validity and temporal stability are two requisites for a tool to be useful for research (Cash, 2011; Thompson, 2004) or clinical purposes. Accordingly, the BPFRS was examined for content validity, convergent validity, criterion validity, and temporal stability, following guidelines from Alexandre and Coluci (2011) and Pasquali (2003).
Content validity
Ten expert judges, each with at least 5 years’ experience in body image and psychometric research, were invited to assess BPFRS content validity, in terms of its capacity to evaluate body dissatisfaction and perception. The judges received a form on which they were required, after viewing the scale, to assign values of one (strongly disagree) to five (strongly agree), to indicate their level of agreement with five key affirmations: (a) the images of the scale are consistent with the human body; (b) the scale is visible, practical, and easy to apply; (c) the scale is capable of evaluating both the attitudinal dimension (specifically body dissatisfaction) and perceptual dimension of body image; (d) the scale represents the female body in a realistic manner; and (e) taken together, the front and side views enable an image to be formed with greater information content on the shape of the individual’s body. Data were analyzed descriptively. In keeping with the value commonly adopted in the literature (Hair, Black, Babin, & Anderson, 2009), we sought at least 70% interrater agreement (at least seven judges) with high ratings of instrument approval, ratings of 4 (agree) to 5 (strongly agree) for each BPFRS dimension assessed.
Convergent validity
Convergent validity was assessed with the two previously researched scales completed by participants, BSSA and SFRS. Each of these scales had been previously validated for the Brazilian female population, and significant positive correlations were expected between these instruments and the new instrument created in this study.
Criteria validity
Criteria validity was tested by examining the correlations between (a) participant’s actual BMI and the characteristic BMI of the silhouette the participant chose to represent her body; and (b) the silhouette chosen to represent the participant’s body and the body dissatisfaction index. Significant positive correlations were expected between these variables.
Temporal stability
To test the instrument’s temporal stability as regards the stability and reproducibility of results (Anastasi & Urbina, 2000), retesting was performed on 30% of the sample (45 women) as recommended by Thompson (2004). Note that the new scale was applied on different days, and the interval between test and retest was 35 days.
Statistical Analysis of the Data
Content validity testing entailed descriptive analysis of percentage of agreement. Convergent and criteria validity were assessed with Pearson correlations. The instrument’s temporal stability was analyzed using the Kappa coefficient of agreement (Agresti, 2013). All procedures were performed using SPSS software, version 18.0 (SPSS Inc., Chicago, IL) with a significance level of 5%.
Results
In the assessment of the scales’ performance in evaluating body image, content validity, judges’ scores reflected high approval ratings with interrater agreement in excess of the previously established criterion of 70% (Hair et al., 2009). Convergence was demonstrated, with significant results, between the BPFRS and both the BSSA (r = .82; p = 1e−5) and the SFRS (r = .73; p = 1e−4), indicating that the BPFRS evaluates body dissatisfaction reliably in young women. A significant positive correlation was found between participants’ actual and perceived BMI on the BPFRS scale (r = .88, p = 1e−4), demonstrating correspondence between these variables. Similarly, the correlation found between BMI and body dissatisfaction was high within the BPFRS (r = .81, p = 1e−4).
Temporal stability between test and retest scores was tested by significant positive correlations for both dissatisfaction (r = .79, p < .0001) and body perception (r = .77, p = 1e−4). The Kappa index indicated moderate temporal stability for the BPFRS (κ = .593; p = 5e−5) and BSSA (κ = .581; p = 5e−5) in assessing body dissatisfaction and for the BPFRS in assessing perception (κ = .6; p = 5e−5).
Discussion
This study aimed to develop and validate a new photographic scale to evaluate body dissatisfaction and body perception based on personalized images of the bodies of the respondents themselves. Kachani et al. (2013) point to the growing number of centers devoted to treating alterations in body image in Brazil. In that light, it is very important not only to refine the methodological apparatus used for evaluation but also to assess psychometric qualities of any tool (Gardner & Brown, 2011). The results of this study support the validity and temporal stability of the BPFRS (Agresti, 2013; Anastasi & Urbina, 2000; Pasquali, 2003) with findings that are in line with other studies in the area (Adami et al., 2012; Conti et al., 2013; Gardner & Brown, 2010a; Gardner, Jappe, & Gardner, 2009; Morgado, Ferreira, Campana, Rigby, & Tavares, 2013; Swami et al., 2008). Specifically, content validation was supported by over 70% agreement among the expert judges that each element of the scale was relevant and representative for the construct to be evaluated. The BPFRS met the essential test, when evaluating body image, that the parameters measured included real morphological characteristics of young women, as recommended by Swami et al. (2008, 2012). Criteria validation was supported by correlations between both real and perceived BMI (r = .88) and between BMI and body dissatisfaction (r = .88). Similar values have been reported by previous studies of women: r = .76 to .72 in Scagliusi et al. (2006), and .84 to .76 in Kakeshita et al. (2009). This trend has been widely evident in the literature, perhaps due to women’s preference for an ultra-thin body (Gardner et al., 2009). We agree with Swami et al. (2008) in their view that this strong correlation between a perceived silhouette and BMI provides evidence that the instrument in question (in this case, the BPFRS) can be used to evaluate both body dissatisfaction and perception. Convergent validity was demonstrated in that the BPFRS correlated with both BSSA (r = .82) and SFRS (r = .73). Similarly, Swami et al. (2008, 2012) used similar methodology to show good convergent validity for their PFRS instrument. Swami et al. (2012) also found that body dissatisfaction, as measured by the PFRS, is associated with body appreciation, internalization of media messages on appearance, and self-reported BMI. Of these factors, only the latter was tested in this study.
The BPFRS has added improvements and refinements to the methodological apparatus used in body image research to date in that it utilizes photographs of respondents themselves for rating stimuli and introduces the side-view profile stimuli. We believe this more individualized and realistic measure will improve respondent engagement in the task and yield more accurate and ecologically valid results, and future research on the instrument can now address those expectations. Meanwhile, this tool is able to assess body dissatisfaction in a similar manner to the PFRS, and it performed well in assessing body image perception.
Previous studies have reported poor reliability in most existing figure-rating scales (Gardner et al., 2009; Swami et al., 2008). In contrast, the BPFRS displayed strong test–retest reliability (r = .87) and temporal stability (κ = .581) in assessment of body dissatisfaction and perception. Swami et al. (2008) and Gardner and Brown (2010a) have pointed out that assessment of these parameters—the absence of which constitutes one of the major gaps in studies of body image—is very important to guaranteeing effective evaluation. Our findings are consistent with those of other studies of similar tools used with women, that is, r = .78 in Scagliusi et al. (2006); .84 and .76 in Kakeshita et al. (2009); .87 in Swami et al. (2008); and .85 in Swami et al. (2012).
Some limitations of the present study include its restriction to a particular age group and to female subjects, which may lead to bias and limit generalizations, given that age and gender factors are known to influence body image. In addition, some aspects of the preparation of the methodological apparatus for evaluating the perceptual dimension need to be refined. When validating the BPFRS, a normative value was not established. Another important factor in video distortion techniques is the lack of three-dimensionality, with image augmentation on the horizontal axis only, which mischaracterizes how human body composition changes in the natural way. Of course, other limitations are that this method of evaluation requires instrument respondents to be photographed (perhaps an aversive event for some subjects), it takes additional time, and it requires equipment and an involved process for generating and displaying distorted images.
The data obtained here have important theoretical and practical implications. The first relates to the need for multidimensional evaluations of body image that include actual physical characteristics of the individual evaluated. That approach to the study of body image is still uncommon in Brazil, hindering interventions in clinical and nonclinical samples for lack of precise information specific to local populations. Many research and clinical activities in this work are still based on studies carried out on other populations with different physical and cultural characteristics. As regards practical implications, this study (even if preliminarily) suggests an applicable and affordable methodological strategy, which can readily be incorporated into intervention and research work. The BPFRS can enhance the evaluation, diagnosis, and prophylaxis of body dissatisfaction and distortion of body perception. By considering undistorted images of participants, the BPFRS is a unique tool, specific to the evaluated individual. This tool respects and includes participant’s individual characteristics, and it may lend itself well to occasions when it is necessary to obtain periodic evaluations on the same subject. Other measures that rely on standardized images may introduce error variance from subject difficulty identifying with other body alterations. We would emphasize that researchers interested in using the BPFRS in future studies may do so, using the image manipulation programs free of charge, providing they follow the procedures set out in this manuscript.