
Abstract
Autistic individuals often struggle developmentally, even in areas that are not explicit diagnostic criteria, such as motor skills. This study explored the relation between early motor skills, assessed retrospectively, and current pragmatic language skills. Caregivers of neurotypical and autistic children, matched on gender and age, completed assessments of their child’s early motor development and current language abilities. Early motor skills were correlated with later pragmatic language skills, and autistic children exhibited fewer motor skills than neurotypical children. In fact, motor skills were a better predictor of an autism spectrum diagnosis than were scores on a measure of current pragmatic language. These results highlight the important role of motor skills in autism spectrum disorders.
Introduction
Early motor milestones, such as sitting, crawling, and walking, are tied to the development of perceptual (Ross-Sheehy, Perone, Vecera, & Oakes, 2016), social (Karasik et al., 2014; Walle, 2016), and cognitive abilities (Libertus & Violi, 2016; Walle & Campos, 2014) in typical infants and toddlers. Furthermore, various motor milestones have been found to relate to the development of language skills; for example, sitting skills predict subsequent receptive language skills in infants (Libertus & Violi, 2016), and the transition from crawling to walking is associated with an increase in communicative behaviors, specifically gestures (Clearfield, 2011). More generally, motor skills are positively correlated with concurrent language skills in toddlers (Alcock, 2006; Alcock & Krawczyk, 2010; Wang, Lekhal, Aaro, & Schjolberg, 2014). This relationship not only exists between oral motor skills and expressive language (Alcock, 2006) but also between fine or gross motor skills and both receptive and expressive language skills (Alcock & Krawczyk, 2010). In fact, one large-scale longitudinal study reported that early motor skills (at 18 months) also predicted later general language skills (36 months; Wang et al., 2014).
The relationship between motor skills and language skills is of particular interest for such developmental conditions as autism spectrum disorder (ASD), characterized by atypical communication. Individuals on the autism spectrum, or autistic individuals as they prefer to be called (see Dunn & Andrews, 2015; Kenny et al., 2015; Sinclair, 2013, for why identity-first terminology is preferred over person-first terminology), are diagnostically distinguished in the Diagnostic and Statistics Manual, 5th Edition (DSM-5; American Psychiatric Association, 2013) from non-autistic or neurotypical individuals in their social communication, interests, and behaviors.
Motor Skills in Autistic Children
Although not part of the diagnostic criteria for ASD, motor challenges are a cardinal concern in this diagnostic group. A meta-analysis addressing a continuum of motor skills, ranging from motor planning to balance, describes large differential effect sizes between autistic and neurotypical individuals across the lifespan (range: 0.92 in adulthood to 1.36 in childhood; Fournier, Hass, Naik, Lodha, & Cauraugh, 2010). Autistic children exhibit delayed or atypical early motor skills, beginning in infancy and toddlerhood (Baranek, 1999; Gernsbacher, Sauer, Geye, Schweigert, & Goldsmith, 2008; Landa & Garrett-Mayer, 2006; Teitelbaum, Teitelbaum, Nye, Fryman, & Maurer, 1998). For example, the ability to execute early oral-motor actions (e.g., blowing raspberries at six months) and manual-motor actions (e.g., grabbing a dangling toy at six months) distinguishes neurotypical infants and toddlers from those subsequently diagnosed with autism (Gernsbacher, Sauer, et al., 2008).
Many studies investigating early motor delays in autistic children rely on their younger siblings due to their increased likelihood of receiving an ASD diagnosis (Ozonoff et al., 2010). Studies of at-risk younger siblings who later receive an autism spectrum diagnosis have not generally reported significant delays in motor skills prior to 12 months (Landa & Garrett-Mayer, 2006; LeBarton & Iverson, 2013; Leonard et al., 2014; Ozonoff et al., 2010), but individual studies vary in reports of the age when a delay is first noted, ranging from 14 months for both fine and gross motor skills (Landa & Garrett-Mayer, 2006) to 36 months for fine motor skills only (Leonard et al., 2014). A motor skill delay may differentiate at-risk children who subsequently receive or do not receive an ASD diagnosis. More specifically, one study found that motor control at 18 months distinguished younger siblings of autistic children who received an autism spectrum diagnosis from younger siblings of autistic children who did not receive an autism spectrum diagnosis at 36 months (Brian et al., 2008). Another study reported that parental concern over motor development at six months differentiated younger siblings of autistic children who later received an autism spectrum diagnosis from both younger siblings of neurotypical children and younger siblings of autistic children who later did not receive an autism spectrum diagnosis (Sacrey et al., 2015).
The Relation Between Motor and Language Skills in Autistic Children
Similar to findings with typically developing children, motor and language skills were found to be linked in autistic children for concurrent expressive language (Hsu et al., 2004; Kim, 2008; Luyster, Kadlec, Carter, & Tager-Flusberg, 2008; McDuffie, Yoder, & Stone, 2005; Mody et al., 2017; Stone & Yoder, 2001) and, to a lesser extent, for receptive language (Kim, 2008; McDuffie et al., 2005; Mody et al., 2017). This relationship has also been found for motor imitiation (Luyster et al., 2008; McDuffie et al., 2005; Stone & Yoder, 2001), fine motor skills (Hsu et al., 2004; Mody et al., 2017), and gross motor skills (Hsu et al., 2004; Kim, 2008; Mody et al., 2017).
Motor skills may also predict language skills in autistic children. More specifically, motor imitation in autistic preschoolers predicted receptive language six months later after controlling for cognitive ability (McDuffie et al., 2005), intentional communication a year later after controlling for initial intentional communication (Sandbank et al., 2017), and expressive language two years later after controlling for initial expressive language (Stone & Yoder, 2001). Similarly, gross motor skills predicted the rate of expressive language development from age 2 – 9 years in autistic children (Bedford, Pickles, & Lord, 2016) and expressive language development from 7 – 36 months in younger siblings of autistic children who subsequently receive an autism spectrum diagnosis (Leonard, Bedford, Pickles, Hill, & the BASIS team, 2015). Furthermore, the ability to execute early oral- and manual-motor actions between six and 24 months of age predicted subsequent speech fluency in autistic children (Gernsbacher, Sauer, et al., 2008). Finally, in an intervention-based study, change in oral-motor skills correlated with change in receptive and expressive language skills in young autistic children (Belmonte et al., 2013).
Motor Skills and Autistic Characteristics
Emerging literature suggests that motor skills are related to autistic characteristics and not just an autism spectrum diagnosis. For example, motor skills have been negatively correlated with the degree of autistic traits in autistic children (Hilton, Zhang, White, Klohr, & Constantino, 2012) and have predicted autism severity scores in autistic toddlers (MacDonald, Lord, & Ulrich, 2014) and school-age autistic children (MacDonald, Lord, & Ulrich, 2013). Motor skills have also been associated with specific diagnostic characteristics. Age at sitting predicted restricted and repetitive behaviors in one study (Uljarević, Hedley, Alvares, Varcin, & Whitehouse, 2017), and fine motor, but not gross motor, skills predicted social skills in a second study (Mody et al., 2017).
The Present Study
As shown, there is a growing body of research suggesting that motor skills not only distinguish autistic and neurotypical individuals but may also predict language skills in autistic children. While research examining the relationship between motor and language skills has focused on receptive and expressive language, autistic individuals diagnostically differ in social communication, for which research has been sparse and limited to documenting a relationship between motor skills and autism severity scores (MacDonald et al., 2013, 2014; Mody et al., 2017). No prior study on motor skills has assessed pragmatic language skills specifically. Therefore, the present study aimed to elucidate the relationship between early motor skills and pragmatic language in autistic children. More specifically, we hypothesized that, in retrospective motor skills assessments, autistic children would have performed significantly fewer early motor skills than neurotypical children and that early motor skills would be positively correlated with later pragmatic language skills. Additionally, we hypothesized that the number of autistic traits would be negatively correlated with early motor skills and that retrospectively assessed early motor skills would better predict an autism spectrum diagnosis than currently assessed pragmatic language skills.
Method
Participants
Participants were recruited via announcements through local autism service organizations, fliers posted at local businesses, and word of mouth. A total of 76 caregivers of neurotypical (n = 31) and autistic (n = 45) children between the ages of 3 – 18 years enrolled in the study between June 2012 and March 2015. All participating caregivers provided informed consent and received a $15 gift card for completing the study. This study was approved by the institutional review board at Ursinus College.
To verify an autism spectrum diagnosis, we used a 15-point cut-off on the Social Communication Questionnaire (SCQ; Berument, Rutter, Lord, Pickles, & Bailey, 1999). A total of 13 children (two neurotypical and 11 autistic) were excluded from further data analysis due to inconsistencies between parent report of a community diagnosis on the autism spectrum (most often made by a pediatrician or psychologist) and the child’s score on the SCQ. An additional 14 children (nine neurotypical and five autistic) were excluded from further data analysis due to medical conditions suggesting possible non-idiopathic autism or an early motor development confound such as known chromosomal anomalies, history of seizure disorder, diagnoses involving cardiac or nervous system dysfunction, major sensory impairments (e.g., hearing loss), premature birth, or speech delay in neurotypical children. Thus, the sample was narrowed to 20 neurotypical children and 29 autistic children. Because neurotypical and autistic groups of children significantly differed in their gender ratios (neurotypical: 11 females, nine males; autistic: four females, 25 males; χ2(1) = 9.46, p = .002) and age at caregiver interview (neurotypical: M = 7.45 years, SD = 3.85; autistic: M = 10.70 years, SD = 4.51; t(47) = −2.62, p = .01), participants were carefully selected for the final sample to create comparable groups with respect to gender ratios and age. The final sample comprised 13 neurotypical (four females, nine males; M age = 7.97 years, SD = 4.24) and 13 autistic children (four females, nine males; M age = 7.98 years, SD = 4.11). None of the neurotypical children had a developmental or language disorder. In terms of developmental disorders, five autistic children also had a diagnosis of Attention Deficit/Hyperactivity Disorder (ADHD) and two autistic children had a diagnosis of intellectual disability. In terms of language disorders, 11 autistic children experienced a speech delay and one of those had a diagnosis of dyspraxia.
Materials and Measures
Primary caregivers completed a questionnaire to assess their child’s present-day language ability: the Children’s Communication Checklist (CCC; Bishop, 1998). Analyses using the CCC focused on the pragmatic composite score which includes statements related to inappropriate initiation, coherence, stereotyped conversation, use of context, and rapport. Parents were also asked to complete the MacArthur Communicative Development Inventory (CDI; Fenson et al., 1994); however, based on the average age of the current sample and a limited range of scores in the neurotypical children, CDI scores were not analyzed.
Primary caregivers completed an interview about their child including a series of questions about current medical and educational diagnoses and motor development, and they completed two questionnaires to assess autistic characteristics (see later). This was mostly a landmark-based retrospective interview to assess the children’s motor development between six and 24 months (Gernsbacher, Sauer, et al., 2008). The first author was trained by Gernsbacher in how to administer the landmark-based retrospective interview, and the first author then trained all interviewers in this study. The primary caregiver was asked to recall a salient event at each age (6, 12, 18, and 24 months) before answering yes or no questions about oral- and manual-motor skills. While some have questioned the use of retrospective assessment methods (e.g., Ozonoff et al., 2010), Gernsbacher, Sauer, et al. (2008) verified this interview approach with home videos. A total of 20 motor skills were assayed over the four ages. Two items from the original interview were inadvertently omitted during the creation of the retrospective interview: makes animal sounds (oral, 18 months) and points proximally on request (manual, 18 months).
Descriptive Statistics and t-tests Group Difference Probability Finidngs on Measures of Communication Behavior and Autistic Traits for Autistic and Neurotypical Samples.
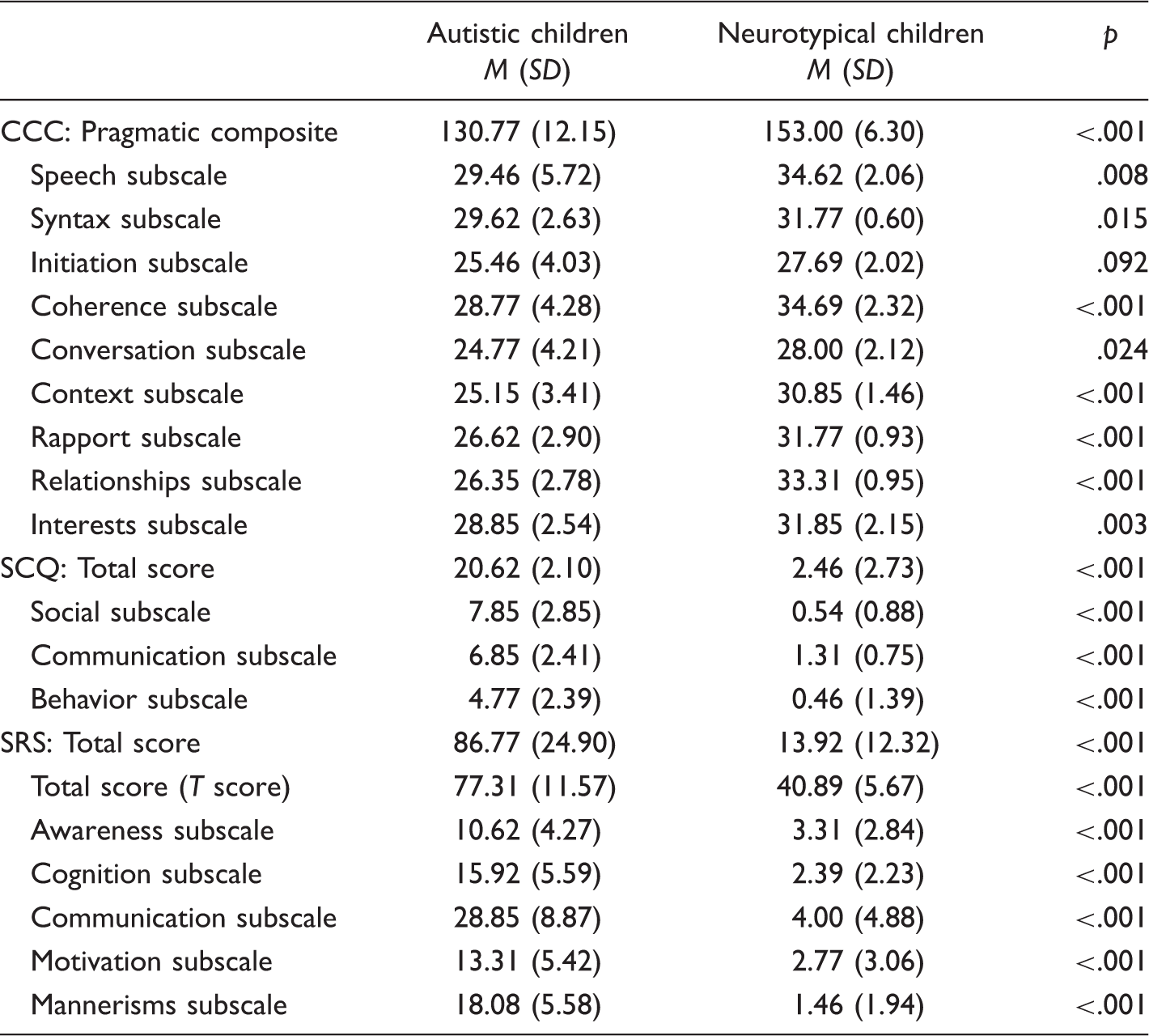
Note. All scores are raw scores unless otherwise specified.
Procedure
Interested primary caregivers received an information packet with details about the study, an informed consent form, and the language questionnaires by postal mail. After caregivers returned the informed consent and language questionnaires, caregivers were contacted by phone or electronic mail to schedule a phone interview which comprised questions about the child’s medical history and diagnoses, the retrospective interview about motor development, the SCQ, and the SRS (in that order).
Results
Early Oral- and Manual-Motor Skills and Developmental Milestones in Neurotypical and Autistic Children.
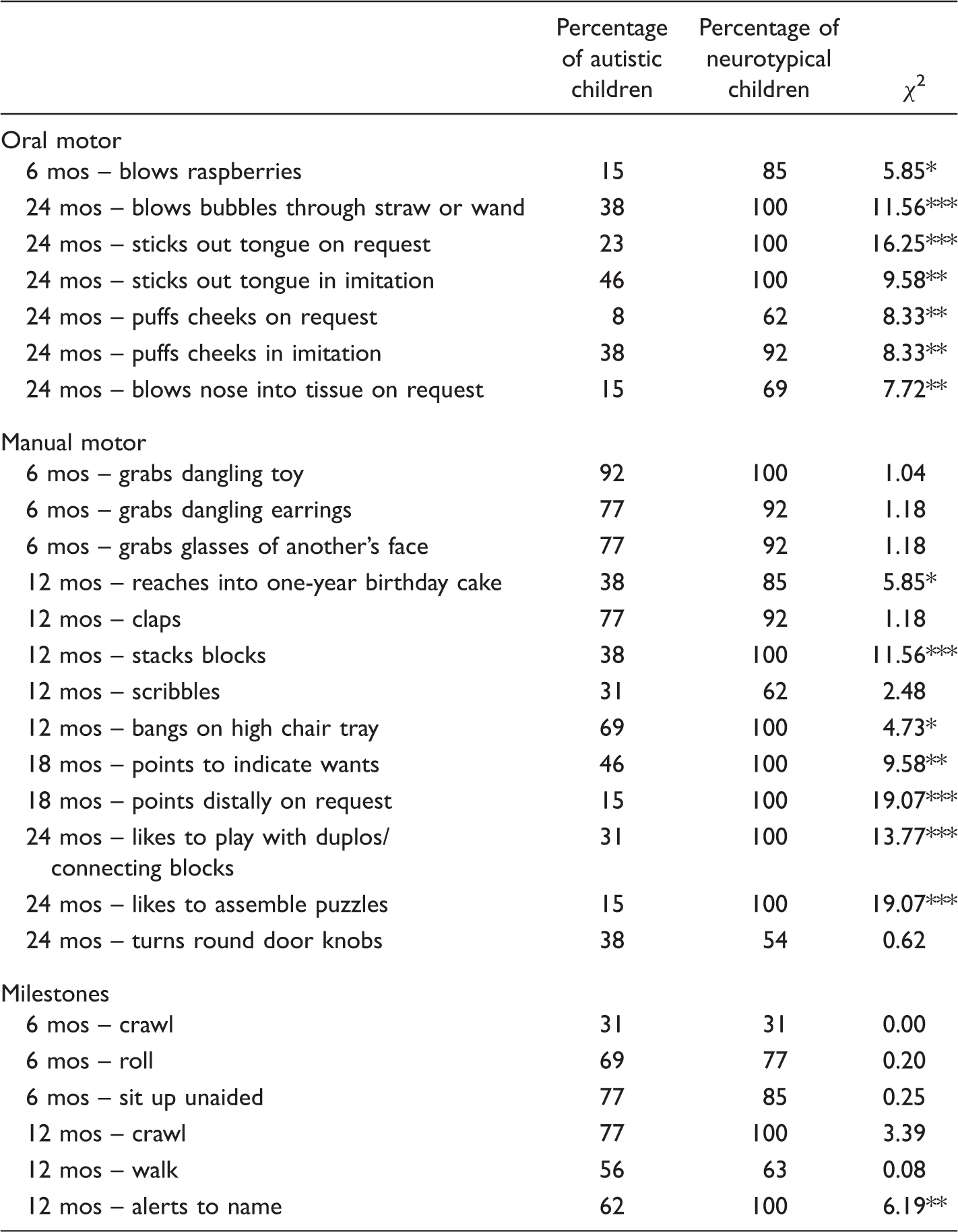
p ≤ .05. **p ≤ .01. ***p ≤ .001.
Composite motor skills scores were created for each participant by computing the percentage of motor skills performed. All additional analyses used these composite percentage scores. To investigate the effects of type of motor skill (oral or manual) and group (autistic or neurotypical) on the percentage of motor skills performed, we used a 2 × 2 mixed-design analysis of variance (ANOVA). There was a significant main effect of type of motor skill, F(1, 24) = 5.98, p = .02, Percentage of oral-motor and manual-motor skills performed by autistic and neurotypical children. Error bars represent ±1 SE.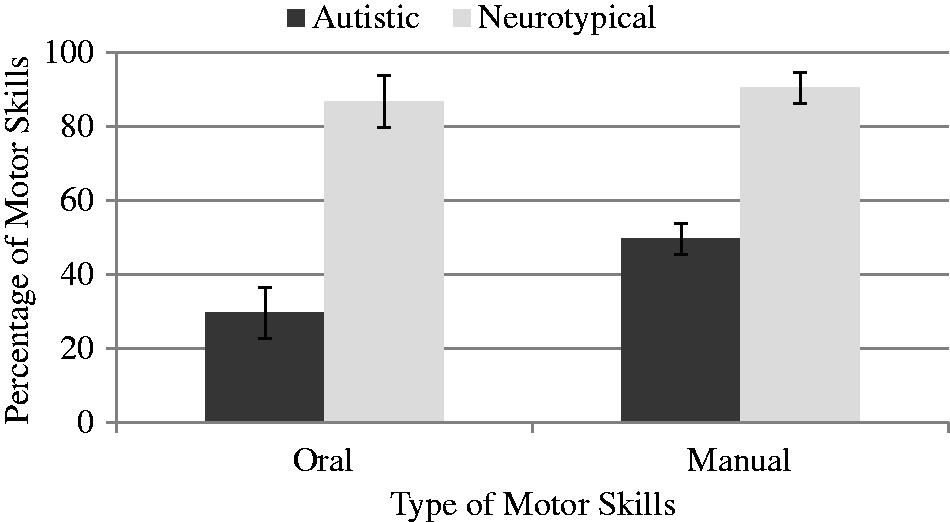
To investigate the effects of age of motor skill (6 months, 12 months, 18 months, or 24 months) and group on the percentage of motor skills performed, a 4 × 2 mixed-design ANOVA was conducted. There were significant main effects of age of motor skill, F(3, 72) = 8.33, p < .001, Percentage of 6-, 12-, 18-, and 24-month motor skills performed by autistic and neurotypical children. Error bars represent ±1 SE.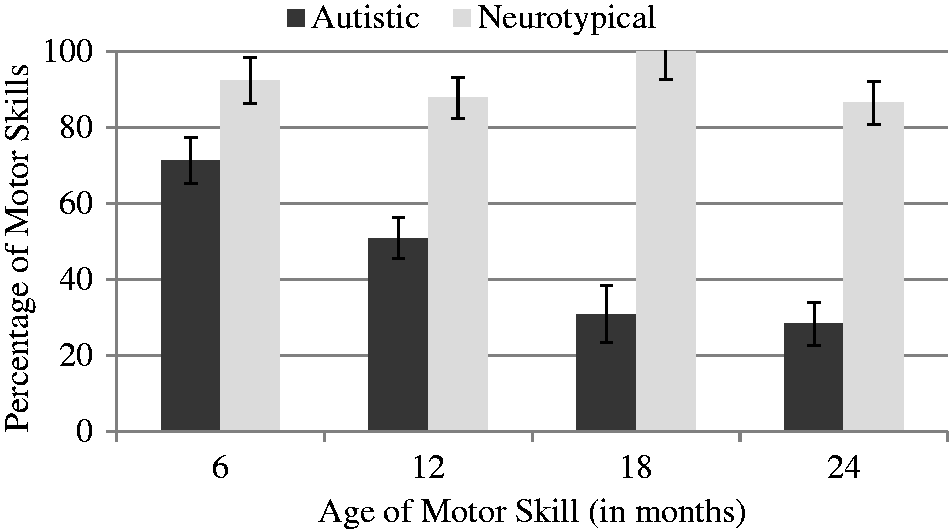
Pearson correlations were calculated between percentage of oral-motor skills performed and percentage of manual-motor skills performed with child’s age at caregiver interview, number of autistic traits (T scores on the SRS), and pragmatic language (pragmatic composite score on the CCC) in all children (i.e., both autistic and neurotypical children). A Bonferroni correction was applied to correct for multiple comparisons (i.e., six comparisons, α = .008). Neither oral- nor manual-motor skills were related to child’s age (r(24) = .15, p = .47 and r(24) = −.06, p = .76, respectively). However, both oral- and manual-motor skills were negatively correlated with autistic traits (r(24) = −.77, p < .001 and r(24) = −.75, p < .001, respectively) suggesting that the fewer motor skills performed, the more autistic traits the child exhibited. Furthermore, both oral- and manual-motor skills were positively correlated with pragmatic language (r(24) = .62, p < .001 and r(24) = .59, p = .002, respectively). Correlations were not significant when considering each group separately (all ps > .10) and the results were comparable with the full sample.
Finally, a forward stepwise logistic regression was conducted to predict group membership using total number of motor skills performed and pragmatic language as predictors. A model using only the number of motor skills performed was statistically significant, indicating that the number of motor skills performed reliably distinguished autistic and neurotypical children (χ2(1) = 27.55, p < .001). There was a strong relationship between number of motor skills performed and group membership (Nagelkerke R2 = .87) with a prediction success of 88.5% (92.3% for neurotypical participants and 84.6% for autistic participants). Addition of pragmatic language did not significantly improve the model (χ2(1) = 3.32, p = .07). When using the full sample, a model using both pragmatic language and number of motor skills was statistically significant (χ2(2) = 58.04, p < .001). In this model, number of motor skills significantly improves a model using only pragmatic language (χ2(1) = 9.46, p = .002).
Discussion
The present study replicated previous research in showing that early oral- and manual-motor skills were correlated with later language quality and that early oral- and manual-motor skills distinguished autistic and neurotypical children (e.g., Gernsbacher, Sauer, et al., 2008). Furthermore, the present study demonstrated that early oral- and manual-motor skills were negatively correlated with the number of autistic characteristics and were, in fact, such effective predictors of an autism spectrum diagnosis that measures of later pragmatic language added no predictive power. As autistic and neurotypical children did not generally differ in their attainment of developmental motor milestones (e.g., crawling), these results were not driven by a negative halo effect in which caregivers of autistic children simply rated their children as more delayed in all areas, compared with ratings from caregivers of neurotypical children.
Researchers have proposed that at least in neurotypical children, motor development facilitates communication development. For instance, Campos et al. (2000) proposed that locomotion, in particular, facilitates development in multiple domains ranging from perceptual skills to cognitive and social skills. Similarly, Iverson (2010) posited that motor development from birth to 18 months is important for communication development as new motor skills allow for new types of social interaction, thus facilitating communication development. Despite acknowledgement that delays in communicative development in at-risk infant siblings of autistic children later diagnosed on the autism spectrum may be related to delays in motor development (see Tager-Flusberg, 2016, for a review) and a similar theory that motor delays within the first 2 years play a role in the development of social communication in the autism spectrum (Bhat, Landa, & Galloway, 2011), there is a continued need for a research focus on social communication delays and challenges.
Beyond evidence of motor development as one possible mechanism for communication development, motor and communication have overlapping neural systems which may contribute to the relationship between motor and communicative behaviors seen in the autism spectrum. More specifically, motor-related brain regions are important for language comprehension tasks as evidenced by patient studies and research with multiple neuroimaging techniques (i.e., functional magnetic resonance imaging or fMRI and transcranial magnetic stimulation or TMS) in neurotypical participants (see Pulvermüller & Fadiga, 2010, for a review). Further, Glenberg and Gallese (2012) recently applied a model of motor control to various aspects of language from acquisition to comprehension and production.
These findings have potential implications for the diagnosis of ASD and understanding communication skills in individuals on the autism spectrum. In terms of diagnosis, because oral- and manual-motor skills as early as six months of age are predictive of an autism spectrum diagnosis, early motor skills (e.g., blowing raspberries and grabbing a dangling toy at six months) may serve as early identifiers of ASD that might lead to earlier diagnosis and interventions. Because measures of both social communication (e.g., joint attention) and receptive language depend on manual-motor skills such as pointing and manipulating objects (noted by Gernsbacher, Sauer, et al., 2008), early motor skills may be useful as diagnostic screeners.
Additionally, as previously mentioned, our current understanding of autistic individuals’ communication difficulties highlights challenges in social interaction. This is most notably observed in the merging of social interaction and communication diagnostic categories to form the new social communication disorder in the latest version of the DSM (American Psychiatric Association, 2013). Recent research highlights that autistic individuals’ challenges are consistent with dyspraxia, or difficulty in planning or executing motor movements (e.g., Bodison, 2015; Dowell, Mahone, & Mostofsky, 2009; Dziuk et al., 2007; Mostofsky et al., 2006; Stieglitz Ham et al., 2011). Autistic individuals’ dyspraxia is a promising explanation for their challenges in social communication. In one study, autistic children’s praxis performance predicted diagnostic social interaction and communication scores (Dziuk et al., 2007). Furthermore, gaze dyspraxia is a possible explanation for atypical joint attention seen in autism (Gernsbacher, Stevenson, Khandakar, & Goldsmith, 2008). Finally, motor interventions can improve social and communication skills in autistic children. More specifically, interventions can target motor gestures (e.g., sign language training) or use physical prompts of mouth and hands (e.g., Prompts for restructuring oral muscular phonetic targets or PROMPT) to improve communication (see McCleery, Elliot, Sampanis, & Stefanidou, 2013 for a review).
The present study only addressed whether motor skills distinguished autistic and neurotypical children. Additional research is needed to assess whether early motor skills also distinguish neurotypical infants and toddlers from infants and toddlers with other types of developmental disabilities (e.g., Developmental Coordination Disorder), especially as past research suggests motor challenges may be similar between autistic children and children with other developmental disabilities in later childhood (McPhillips, Finlay, Bejerot, & Hanley, 2014; Noterdaeme, Mildenberger, Minow, & Amorosa, 2002; Perry, Flanagan, Geier, & Freeman, 2009; Provost, Lopez, & Heimerl, 2007; Sumner, Leonard, & Hill, 2016). Likewise, motor and language skills are similarly related in autistic children and children with other developmental disabilities (Hellendoorn et al., 2015; McPhillips et al., 2014), though at least one study reported motor skills in toddlerhood distinguished autistic children from children with atypical development. More specifically, fine motor skills distinguished autistic toddlers from toddlers with atypical development and gross motor skills distinguished a subset of autistic toddlers (i.e., those with a diagnosis of Autistic Disorder) from toddlers with atypical development (Matson, Mahan, Fodstat, Hess, & Neal, 2010).
The current study relied on small convenience samples of autistic and neurotypical children but did not assess, for example, intelligence, socioeconomic status, or home environment. Therefore, the current sample may not be representative of the larger population with respect to other relevant variables, perhaps limiting the generalizability of these results. Future research should report on larger, representative samples so that variables can be investigated variables can be investigated as potential moderators. The current study also relied on data collected via caregiver report via mailed questionnaires and a phone interview, and it was not possible to obtain in-person assessments of the child’s motor or pragmatic language skills. Because in-person assessments of children’s skills are generally preferred over caregiver report, future research should improve on this methodology.
Despite its limitations, the present study is the first to consider the relationship between early motor skills and later pragmatic language in both autistic and neurotypical children. These results add to the growing literature, suggesting that the earliest atypicalities in the autism spectrum are in the motor domain, not in social communication. These results also support the idea that motor challenges or delays may play a role in autistic communication, highlighting the value of further exploring the role of dyspraxia in autistic communication.
Footnotes
Acknowledgments
The authors are grateful to the participating children and caregivers. The authors also thank student research assistants including Kaitlyn Cherry and Kathryn Siti for their assistance with data collection and data entry.