
Abstract
Children’s perception of their own motor competence is an important correlate of their actual motor competence. The current study is the first to examine this association in British children and the first to use both product and process measures of actual motor competence. A total of 258 children (139 boys and 119 girls; aged 4 to 7 years, Mean = 5.6, SD = .96) completed measures of self-perceived motor competence using the Pictorial Scale for Perceived Movement Competence in Young Children. Children were classified as “Low,” “Medium,” or “High” perceived competence based on tertile analysis. Actual motor competence was assessed with the Test of Gross Motor Development-2 (a process measure) and a composite of 10-m sprint run time, standing long jump distance, and 1-kg seated medicine ball throw (collectively, a product measure). Data for process and product measures were analyzed using a 2 (sex) × 3 (high, medium, low perceived competence) analysis of covariance, with body mass index, calculated from height and mass, and age controlled. Boys obtained significantly higher scores than girls for both the process (p = .044) and product (p = .001) measures of actual motor competence. Boys had significantly (p = .04) higher scores for perceived competence compared to girls. Compared to children classified as medium and high self-perceived competence, children classified as low self-perceived competence had lower process (p = .001) and product scores (i.e., medium, p = .009 and high, p = .0001) of actual motor competence. Age (p = .0001) and body mass index (p = .0001) were significantly associated with product motor competence. Strategies to enhance actual motor competence may benefit children’s self-perceived motor competence.
Keywords
Introduction
Stodden et al. (2008) theorized that the development of good motor competence via fundamental movement skills (FMS) is important to children’s body weight and engagement in physical activity (PA). In subsequent years, an influx of data has strongly supported this idea (Robinson et al., 2015). Research with British children has further shown that higher motor competence is associated with lower body fat (Duncan, Bryant, & Stodden, 2016). Longitudinal data have further shown that children with better motor competence are more apt to become physically active and fit adolescents (Barnett et al., 2016) with stronger academic achievement (Jaakkola, Hillman, Kalaja, & Liukkonen, 2015).
Self-perceived motor competence has been shown to be an important correlate of actual motor competence (Barnett, Morgan, Van Beurden, Ball, & Lubans, 2011; Liong, Ridgers, & Barnett, 2015). The Stodden theory suggested that low motor competence would precipitate a negative spiral of PA disengagement that would strengthen as children matured (Stodden et al., 2008). Potentially contributing to this negative spiral, younger children have been particularly subject to forming less accurate self-perceptions, compared to their actual skills (Harter, 1987; Harter & Pike, 1984). A recent systematic review and meta-analysis supported the Stodden theory through research summary impressions of significant positive associations between PA and perceived motor competence in both children and adolescents (Babic et al., 2014). As this review included only one child study amidst 58 adolescent studies, there is a clear need for further research of this kind with younger populations.
Barnett et al. (2008) also called for more research investigating interrelationships between motor competence, children’s weight status, PA, and other health-related variables. However, because prior studies of actual motor competence and perceived physical competence have relied on measures that are not directly aligned (e.g., Goodway & Rudisill, 1996, 1997; LeGear et al., 2012; Robinson, 2011), Liong et al. (2015) called for researchers to better align these variables.
In answer to this call, Barnett and coworkers (Barnett, Ridgers, Zask, & Salmon, 2015; Barnett, Robinson, Webster, & Ridgers, 2015) developed the Pictorial Scale for Perceived Movement Skill Competence for Young Children (PMSC). The PMSC is based specifically on skills tested by the Test of Gross Motor Development-2 (TGMD-2; Ulrich, 2001) which, in turn, builds on earlier measures of perceived competence (Harter & Pike, 1984), yielding a user-friendly measure of perceived motor competence for children. Test retest reliability, internal validity, and face validity for the PMSC were initially established in a convenience sample of Australian children; subsequent work from the same researchers revealed differences in PMSC values between American and Australian children, leading these authors to recommend further PMSC research with diverse samples (Barnett, Robinson, et al., 2015). Lopes et al. (2016) demonstrated good face validity, internal consistency, and reliability of the PMSC with 5–10-year-old Portuguese children, and Valentini et al. (2017) validated the PMSC for use with Brazilian children.
This study sought to extend PMSC research with 4–7-year-old British children and is the first to use both process and product measures of actual motor competence to address perceived and actual competence correlates. There is high current interest in the topic of children’s motor competence and its relationship to health in the United Kingdom (Bryant, Duncan, & Birch, 2014; Duncan et al., 2017), and others have also advocated the more holistic assessment of both process and product measures of motor competence (Logan, Barnett, Goodway, & Stodden, 2017).
Method
Participants
A total of 258 children aged 4–7 years (139 boys, 119 girls; Mean = 5.6 years; SD = .96) from four central England primary schools participated in this study, following protocol approval from our institutional ethics committee and written informed parental consent. From school records, ethnic classifications of these participants were as follows: 72.5% Caucasian, 17.0% South Asian, 6.5%, Black, and 4.0% Other. The schools were selected using convenience sampling; they were located in areas ranked as 40–60% least deprived within England as a whole, using the Index of Multiple Deprivation (Association of Public Health Observatories, 2008).
Procedure
Within the school setting, following an orientation session, children rated their own motor skill competence on the PMSC. After 24–48 hours, we assessed the children’s actual motor competence (using both process and product measures) in small groups of 5-6 children. We assessed the children’s height (cm) and mass (kg) (with children bare-footed and wearing light shorts and t-shirt) using a SECA stadiometer and weighing scales (SECA Instruments Ltd, Hamburg, Germany). We calculated body mass index (BMI) as height/mass squared (kg/m2; Mean = 16.4; SD = 1.9) and found 81.8% (n = 211) to be classifiable as of healthy weight according to International Obesity Task Force criteria (Cole, Bellizzi, Flegal, & Dietz, 2000).
Process measures of motor competence (TGMD-2 Scores)
We assessed four motor skills (two locomotor and two object control) using the TGMD-2 (Ulrich, 2001): run, jump, catch, and overhand throw. These skills were selected because the physical education (PE) curriculum in England for children of this age focuses on mastery of these basic FMS (Department for Education, 2013). Each skill comprised three to four components, and skill mastery on the TGMD-2 requires each component to be present. We video recorded (Sony Handicam CX405b, Sony, UK) each skill and subsequently edited recordings into single-film clips of individual skills with Quintic Biomechanics analysis software v21 (Quintic Consultancy Ltd., UK). In this instance, the TGMD-2 scores were considered a process measure of motor competence as they reflect quality of movement, in line with recent distinctions between process and product measures of motor competence (Logan et al., 2017). We summed scores from two trials to create a total (scored 0–30) overall raw score following recommended TGMD-2 test administration guidelines (Ulrich, 2001). Two researchers experienced in the assessment of children’s movement skills analyzed the video clips after training in two separate 2–3-hour sessions by watching videoed skills of children’s skill performances and rating these against a previously rated “gold standard”. Congruent with prior research (Barnett, Minto, Lander, & Hardy, 2014), training was considered complete when each observer’s scores for the two trials differed by no more than one component per trial from the instructor's score for each skill (>80% agreement). We performed inter- and intrarater reliability analysis for all skills between the two raters on 10% of all the videos. Intraclass correlation coefficients for inter and intrarater reliability were .925 (95% CI [.87, .95]) and .987 (95% CI [.94, .98]), respectively.
Product measures of motor competence
Our three-product measures of motor competence were as follows: 10-m sprint time, standing long jump distance, and seated medicine ball (1 kg) throw distance. We timed each participant’s 10-m sprint using smart speed gates (Fusion Sport, Coopers Plains, Australia), and we tape-measured each participant’s standing long jump (distance from the take-off line to the back of the closest heel on landing). For these two measures (sprint time and long jump), we selected the best of two trials (fastest time in seconds and longest jump in centimeters). Both the sprint time and standing long jump distance are considered valid and reliable measures for children (Tambalis, Panagiotakis, Arnaoutis, & Sidossis, 2013). Our third-product measure was the seated medicine ball throw distance (measured in centimeters), using a 1-kg medicine ball, which has been found to be a reliable and valid measure of upper body strength in preschool aged children (Davis et al., 2008). Children sat on the floor before throwing the medicine ball forward like a chest pass three times, and we selected the furthest distance thrown (in centimeters) as assessed with a tape measure. Intraclass correlation coefficients for the three-product measures of FMS were .9 (CI [.86, .95]) for the 10-m sprint, .94 (CI [.9, .96]) for the standing long jump, and .86 (CI [.82, .91]), for the seated medicine ball throw indicating acceptable reliability. We calculated each participant’s Z-score for each of our three-product measures of motor competence and summed these Z-scores to create a composite product measure of motor competence. Recognizing that lower scores represent better performance on the 10-m sprint, scores on this task were made negative before creating the summed Z-score.
Perceived motor competence
As noted earlier, the children completed the PMSC (Barnett, Ridgers, et al., 2015) to provide their self-perceived movement skill competence scores in the same four skills as measured by the TGMD-2. The PMSC has been described extensively elsewhere, and prior research showed it to have good validity and reliability for this purpose (Barnett, Ridgers, et al., 2015). Briefly, for each skill, children were shown two, sex-specific illustrations of a child performing the skill competently and less competently and were then asked, “This child is pretty good at throwing, this child is not that good at throwing; which child is most like you?” From the selected picture, children were asked to further indicate their perceived competence by endorsing more specific descriptions with either competent or less competent picture, including, for the competent picture—4: Really good at… or 3: Pretty good at, etc.—and for the not so competent picture—2: Sort of good at… or 1: Not that good at. Possible scores for the entire scale ranged from 4–16. Following the children’s completion of these questions, we created tertiles from their scores for perceived motor competence in order to classify children as “high,” “medium,” or “low” in perceived competence overall. Within data for this sample, cut-offs were 4–11 for low, 12–14 for medium, and 15–16 for high, respectively. While these cut-offs may appear unequal in distribution, they represent cut-off scores to create three equal groups relative to the sample as a whole. This same procedure has been employed by previous researchers in the context of actual motor competence (Williams et al., 2008). Two-week test–retest reliability data, available in a subsample of children (n = 43; 22 boys, 21 girls; mean age = 5.6, SD = .48 years), indicated good agreement (intraclass correlation coefficient = .86, CI [.74, .92]) and internal consistency (Cronbach’s α = .89) for the total PMSC perception score based on these four items.
Statistical analysis
Pearson’s product moment correlations were also used to examine the relations between perceived and actual motor competence (as defined by both TGMD-2 scores and product measures) for both boys and girls. An independent samples t-test was used to examine any difference in perceived motor competence between boys and girls. To examine whether actual motor competence (via both TGMD-2 scores and product measures) differed by sex and the perceived motor competence classifications, we analyzed data using 2 (sex) × 3 (high, medium, low perceived competence) analysis of covariance (ANCOVA) models, controlling for both age and BMI. Where any significant differences were found, post hoc pairwise comparisons (Bonferroni adjusted) were employed to examine where the differences lay. Bonferroni adjustments were employed as they reduce the possibility of obtaining statistically significant results due to the testing of multiple hypotheses (Field, 2013). Partial η2 was used as a measure of effect size. Shapiro–Wilk tests confirmed all data were normally distributed (p > .05). In order to determine if there were different proportions of boys and girls within each tertile for perceived motor competence, the Kruskal–Wallis test for independent samples was also conducted. The Statistical Package for Social Sciences (SPSS, Version 20) was used for all analysis.
Results
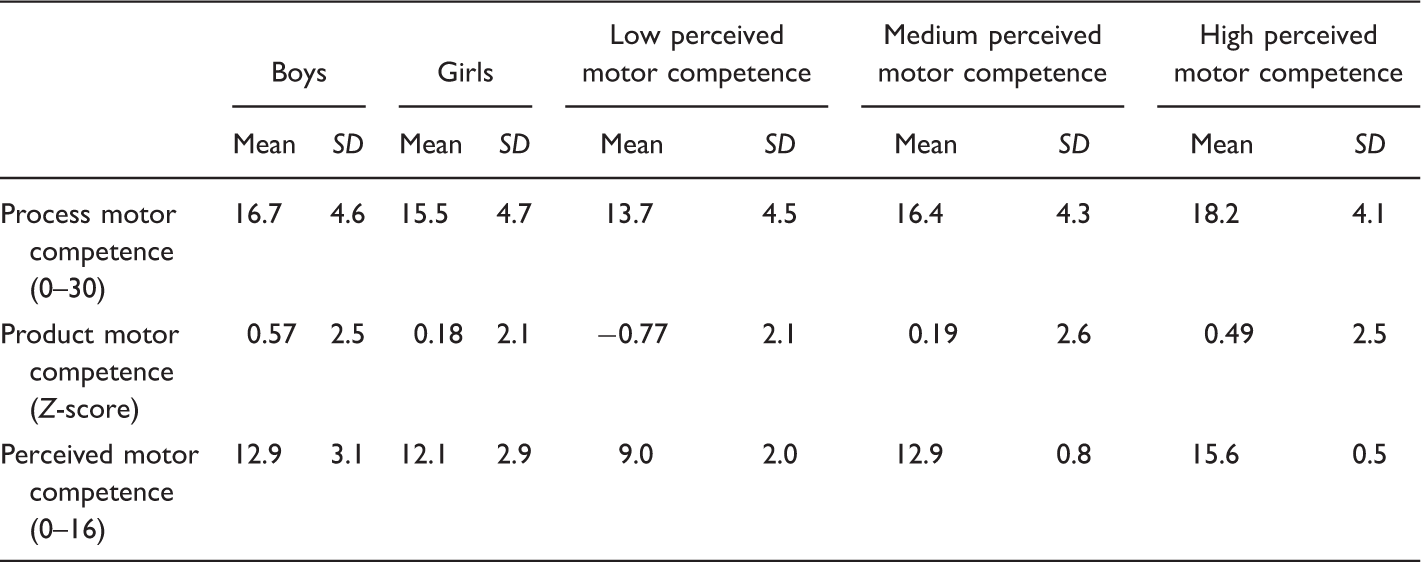
Descriptive Data (Mean, SD) for Process and Product Motor Competence and Perceived Motor Competence Scores Between Boys and Girls and Between Low, Medium, and High Perceived Competence Tertile.
After grouping participants into high, medium, and low self-perceived competence, analysis of process measures of motor competence (TGMD-2 scores) revealed no significant Sex × Perceived Competence Level interaction (p = .756), and neither age (p = .592) nor BMI (p = .849) were significant as covariates. We did find significant main effects for both sex (p = .044, Partial η2 = .018) and perceived motor competence level (p = .001, Partial η2 = .150). Bonferroni post hoc multiple comparisons further indicated that boys had higher TGMD-2 scores (p = .044, see Figure 1).
Mean ± SD of process motor competence (0–30) of boys and girls within the study sample.
Post hoc pairwise comparisons indicated that children classified as low perceived competence had lower TGMD-2 scores compared to children classified as medium or high perceived motor competence (both, p = .0001). Children classified as medium perceived competence also had lower TGMD-2 scores compared to children classified as high perceived motor competence (p = .043). Descriptive data (Means and SEs) for TGMD-2 scores as related to perceived motor competence classifications are presented in Figure 2.
Mean ± SD of process motor competence (0–30) of boys and girls in subgroups of low, medium, and high perceived competence.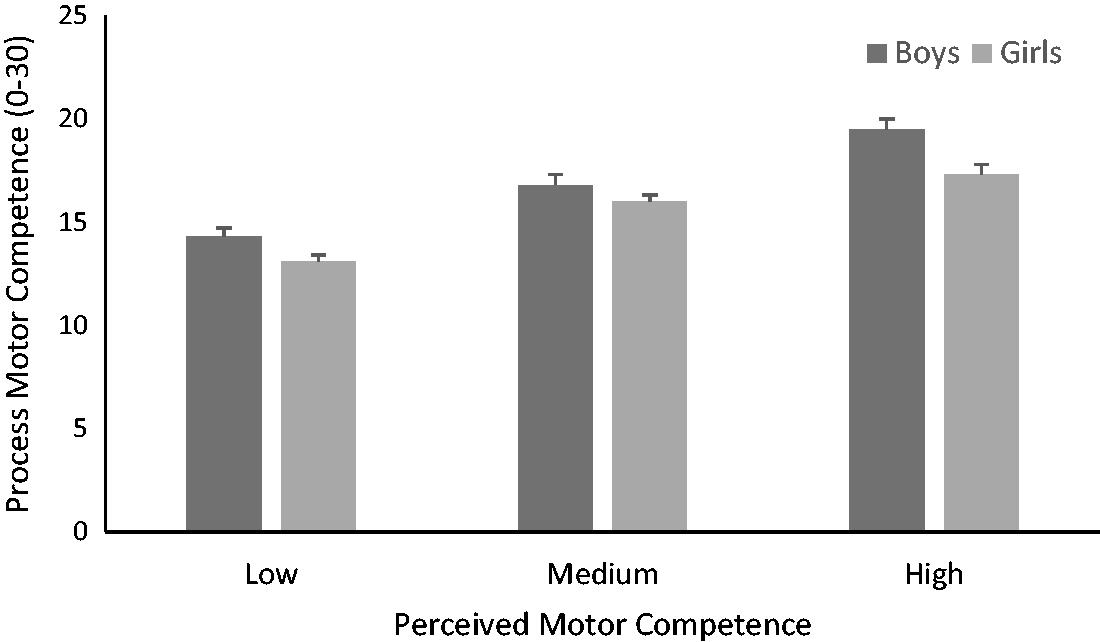
Through analysis of product motor competence, we again found no significant Sex × Perceived Motor Competence Level interaction (p = .368). However, in this analysis, both age (p = .0001, Partial η2 = .318, β = 1.519) and BMI (p = .0001, Partial η2 = .068, β = −.249) were significant covariates. Beta values indicated that a one year increase in age was associated with a 1.519 unit increase in TGMD-2 scores and a one kg/m2 increase in BMI was associated with a −.249 unit decrease in TGMD-2 scores. Similar to the results of process motor competence, for product motor competence, sex was significant as a main effect (p = .001, Partial η2 = .087), as was perceived motor competence (p = .001, Partial η2 = .072). Bonferroni post hoc pairwise comparisons indicated that boys had significantly higher product FMS scores (p = .001, see Figure 3).
Mean ± SD of product motor competence (composite Z-score) of boys and girls.
Post hoc analysis for perceived motor competence indicated that children classified as low perceived competence had poorer composite Z-scores for product motor competence, compared to those classified as medium (p = .009) and high (p = .0001) perceived competence. There was no difference between those classified as medium and high perceived competence (p = .99). Descriptive data (Means and SEs) of product motor competence in its association with perceived competence classifications are presented in Figure 4.
Mean ± SD of product motor competence (composite Z-score) of boys and girls subgroups of low, medium, and high perceived competence.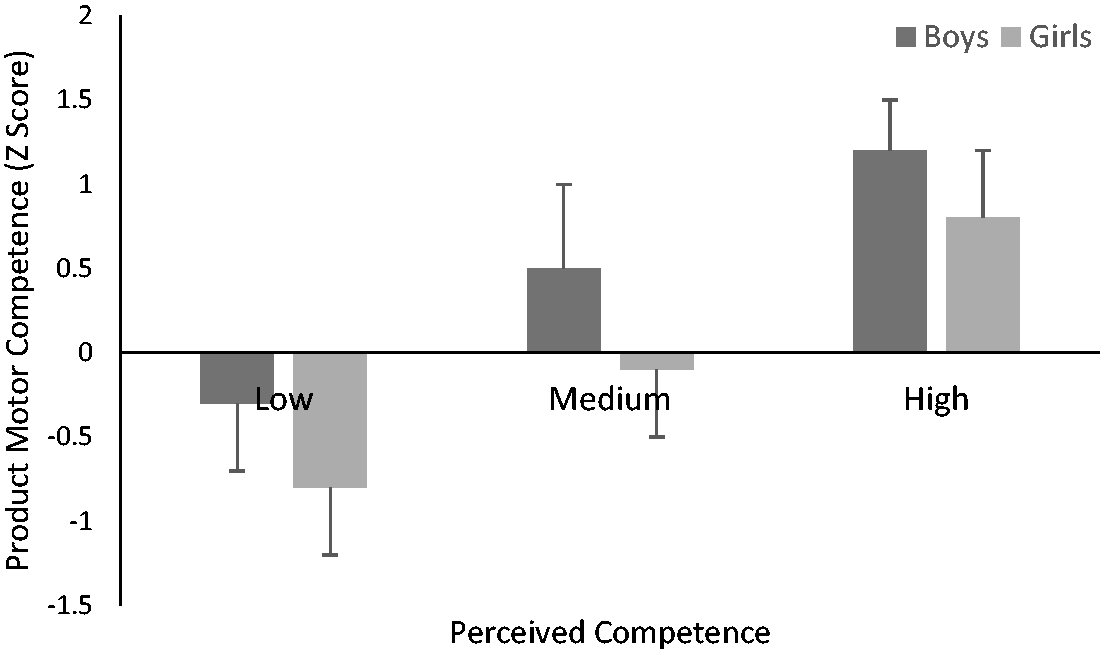
Discussion
This study compared self-perceived and actual motor competence in British school children aged 4–7 years. This is the first study to examine this relationship in this population and using both product (i.e., motor fitness) and process (i.e., TGMD-2 scores) measures. Our key finding was that actual motor competence, assessed with both TGMD-2 scores and product measures, was significantly poorer among children with low versus medium or high perceived motor competence (after controlling for age and BMI). Such results align with prior research that has only used TGMD-2 scores as a sole indicator of motor competence (DeMeester et al., 2016; Spessato, Gabbard, Robinson, & Valenitni, 2013). These aforementioned studies (DeMeester et al., 2016; Sepssato et al., 2013) also highlighted that weight status, assessed using BMI, influences the relation between perceived and actual motor competence. Likewise, Rudisill, Mahar, and Meany (1993) reported that age was a confounder when examining the relationship between actual and perceived motor competence in children. Hence, in the present study, both BMI and age were used as covariates within the statistical analysis.
Importantly, we found a direct alignment between the assessment of actual motor competence (via TGMD-2 scores) and perceived motor competence (via PMSC). While this has not always been the case in prior studies (e.g., LeGear et al., 2012; Robinson, 2011), prior research in this area has shown equivocal findings, with some studies (LeGear et al., 2012; Lopes et al., 2016; Robinson, 2011) reporting no association and at least one other study with Australian children (Liong et al., 2015) reporting variable associations between actual motor competence (assessed using the TGMD-2) and perceived motor competence (assessed using the PMSC) such that overall motor competence was not significantly associated, while boys’ actual object control skills were significantly associated with perceived competence. Another prior study (Barnett, Ridgers, et al., 2015) also observed these associations in object control skills. Similarly, Lopes et al. (2016) found that skill perceptions of locomotor and object control skill could be distinguished in a sample of Portuguese children aged 5 to 10 years. As the current study employed two object control and two locomotor skills into a combined motor competence score, it is difficult to identify which skills might be driving the comparisons noted here.
No study to date has used perceived competence tertiles to examine whether there are differences in actual motor competence according to varied classifications of perceived motor competence. Yet, this methodology has been suggested by other authors for understanding how motor competence may relate to such other variables as PA and weight (Williams et al., 2008). Prior research in this area has treated perceived motor competence as a linear variable (e.g., Barnett, Ridgers, et al., 2015; Liong et al., 2015). While this is valid, subgrouping children into a younger group, such as in the present study, may provide a better understanding of how perceived motor competence relates to other variables, since younger children are assumed to be less accurate in their perceived competence judgments (Harter, 1987; Harter & Pike, 1984).
The results of the current study also demonstrated sex differences in both TGMD-2 scores and product assessed motor competence, with boys demonstrating higher actual motor competence compared to girls, a finding that is consistent with prior studies in the United Kingdom highlighting motor competence differences between boys and girls (Bryant et al., 2014). The current results also support data collected on children from outside the United Kingdom (Goodway & Rudisill, 1997; Rudisill et al., 1993). Systematic review and meta-analysis have shown, more specifically, that boys tend to be better than girls in object control and motor coordination, but they are not necessarily better at all aspects of motor competence (Barnett et al., 2016).
There are of course important limitations to the current study. The use of tertiles in the current study was undertaken to create three equal groups to represent low, medium and high perceived motor competence. While dividing PMSC scores into tertiles can be useful, our classifications were limited to scores obtained by our relatively small sample, and the cut-offs we employed may not generalize to similar classification levels in other samples. Other research, with older children, has advocated cluster profiling in which grouping is based on combinations of low and high perceived and actual motor competence (Bardid et al., 2016). This technique is commonly performed, though groups formed are still unique to the PMSC responses of the researchers’ separate participant samples. Furthermore, the present study focused on a relatively narrow range of motor skills assessed by both the TGMD-2 and the corresponding PMSC, meaning that our results are restricted to this skill subset, limiting our ability to evaluate or make a full range of comparisons between actual and perceived object control or locomotor skills. Although Lopes et al. (2016) recently suggested that it may not actually be necessary to ask children their self-perception in all of the skills of the TGMD, skills such as running and jumping, compared to other skills (e.g., gallop), are more easily understood by young children. Finally, our findings are based on a relatively small sample of children from one geographical area of the United Kingdom. The results of the present study suggest that actual motor competence is significantly poorer in children who perceive their competence to be low compared to children with medium or high levels of self-perceived motor competence.