
Abstract
Cerebral Palsy (CP) is a common physical disability that is managed with a variety of strategies. One non-invasive intervention for people living with CP is a type of video self-modelling (VSM) referred to as positive self-review (PSR). PSR involves watching a video of oneself performing only the best examples of a desired task; this technique has been associated with improved performance and learning for people without disabilities and for those in various clinical populations, including children with spina bifida and stroke patients. PSR may have similar benefits for people living with CP. In this study we examined the effectiveness of PSR for improving a self-selected movement task among individuals living with CP. In this case study approach, eight participants completed a pre-, post-, and second post-test measuring and recording well-being, movement self-consciousness and tendency to consciously monitor movements. Results were mixed, with some participants improving their movement time, well-being ratings and tendency toward self-consciousness and conscious monitoring of movements and others showing no changes or regressions. The effectiveness of VSM appears to depend upon the match between type of task and disability and/or the length of practice. More study is needed.
Introduction
Individual differences in motor learning refer to variations in the ability to perform and improve various motor skills in varied contexts (Ackerman, 1987, 2014; Magill & Anderson, 2020; Pancheco & Newell, 2018a; 2018b). The capacity to learn skills can be influenced by several factors including underlying ability, brain structure and function, and environmental context, among many others (Ferre & Gordon, 2017). Of interest in this study were individuals living with a disability who are often underrepresented in research because of (a) the heterogeneity of their symptoms and specific disability classifications and (b) the difficulty recruiting sufficient numbers of participants for experimental research designs and inferential statistics. The heterogeneity of symptoms among people with disabilities also creates challenges for designing interventions, since generic interventions are often less efficacious than specifically targeted treatments. To illustrate the challenges associated with generic interventions, in the current study, we investigated motor skills learning among individuals living with cerebral palsy (CP) – a classic example of a single classification of a disability group with heterogeneous symptoms. Each person with CP has unique challenges that can compromise the process of skill acquisition; these separate challenges must be better understood for researchers and clinicians to best help individuals with CP manage their symptoms (Dune, 2011).
Cerebral palsy (CP) defines a group of enduring movement and postural disorders related to a developmental brain injury, with changes in brain structure and function that affect motor development and behavior through links to cognition, communication, and neurosensory abilities (Tofani et al., 2020, Vila-Nova et al., 2020). CP encompasses a group of non-progressive (National Center on Birth Defects and Developmental Disabilities, 2020) and non-contagious motor conditions that create physical impairments during human development, primarily in regards to mobility (Beukelman & Mirenda, 1999). Individuals with CP experience permanent but changing motor impairments (Rosenbaum et al., 2007), with complications attributed to disturbances in the developing fetal or infant brain.
Motor disorders associated with CP may be accompanied by problems with spatial perception, behavior, epilepsy, sensation disturbances, and secondary musculoskeletal problems (National Center on Birth Defects and Developmental Disabilities, 2020). As such, individuals with CP may be diagnosed with learning difficulties. Sometimes, however, it is the magnitude of the problems caused by underlying brain injury that prevents the individual from expressing their cognitive abilities (Pennington et al., 2004).
CP is most often characterized by abnormal muscle tone, poor reflexes, and decreased motor development and coordination (Bevans & Tucker, 2020). Tight muscles and joints are often reported, due to permanently fixed joints and bone deformities (Rosenbaum et al., 2007). Classical symptoms also include muscle spasms, involuntary facial movements, unsteady gait, problems with balance, and decreased muscle mass (Himmelmann & Panteliadis, 2018). The effects of CP fall on a continuum of motor dysfunction and may range from mild clumsiness to impairments so severe that they render coordinated movement virtually impossible (Dune, 2011). Spastic CP is by far the most common type, occurring in 70–80% of all cases, and may accompany other types of CP (the remaining 30% of all cases) (The Cerebral Palsy Alliance, 2020). Spastic CP is further classified by the region of the body most affected (see Figure 1).
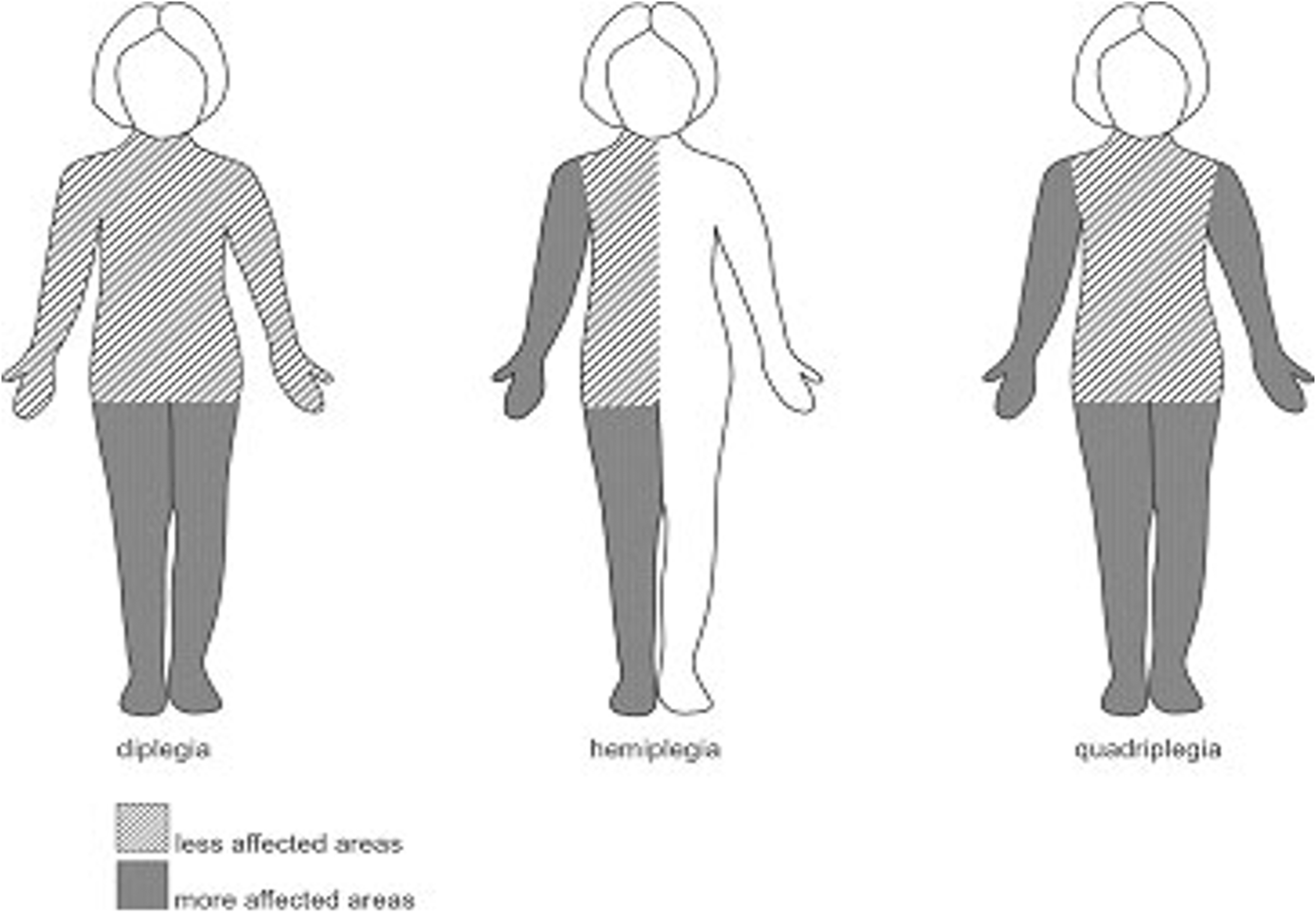
Regional Classifications of Spastic Cerebral Palsy.
Presently, individuals living with CP often engage in conventional management of their physical concerns. Interventions aim to reduce muscle tone and spasticity and increase voluntary motor control. They include splinting and motor training incorporated into a neurodevelopmental approach to rehabilitation. These approaches comprise constraint-induced movement therapy, bimanual training, and virtual reality (Shierk et al., 2016), all of which aim to facilitate “normal” motor development and function and prevent muscle contractures and joint and limb deformities. However, some of these conventional rehabilitation approaches are problematic because they require invasive surgery and its attendant risks, cause pain, or lead to short and long-term complications. These approaches may also be too generic in nature, given the heterogeneity in the degree and type of symptom manifestations associated with CP.
A non-invasive intervention with potential benefit for individuals living with CP involves a combination of physical practice and Video Self Modelling (VSM). Modelling is a type of observational learning that involves watching another person perform a task prior to attempting the task or watching a replay; normally modelling involves no manipulation of the video footage or any prior attempt at performing a skill (Anderson et al., 2014). In contrast, however, a form of VSM referred to as Positive Self-Review (PSR) presents footage of oneself performing only positive examples of the desired skill or behavior. Modelling can be presented in the form of a future performance in a technique referred to as feedforward (FF) video self-modelling. In the FF technique, the video footage is edited to show the person performing the skill at a level not yet achieved (Anderson et al., 2014). VSM has been applied extensively in domains such as education (Hitchcock et al., 2003), with growing interest in its use, amongst other observational techniques, for movement and rehabilitation domains (Coulson et al., 2006; Holmes, & Calmels, 2008; Rymal & Ste-Marie, 2019; Steel et al., 2018; Wrightson et al., 2016).
Skills explored in the education domain have often been associated with reading, especially for individuals on the autism spectrum or persons from low-socioeconomic areas (Dowrick et al., 2006; Rao et al., 2012); these uses of VSM may involve either PSR or FF. More recently, there has been greater use of VSMs by researchers in the field of human movement science to improve movement skill execution in sporting and rehabilitation settings. For example, Coulson et al. (2006) used the PSR method to increase the likelihood that individuals with facial nerve palsy would perform a symmetrical smile. This method had the additional effect of increasing confidence and well-being. Further, Steel et al. (2018) used this method for individuals post-stroke event, with the objective of improving their reach and grasp capability. The participants in this study demonstrated a significant improvement in the forward motion (but not the backward or toward the body motion) while displacing a weighted cup with their preferred hand, compared to their non-preferred hand. The participants also showed significant increases in their well-being scores and improvements in their movement self-confidence and movement self-consciousness scores as measured by the Movement Specific Reinvestment Scale (Masters & Maxwell, 2008).
Given significant heterogeneity among individuals in special populations exposed to interventions for improving performance or learning, consideration must be given to difficulties identifying group changes over time or comparing experimental and control groups. While physical practice has been described as the most important variable in skill acquisition, VSM is known to be a particularly effective way to facilitate skill acquisition in both typical and atypical populations (Dowrick & Dove, 1980; Dowrick & Raeburn, 1995; Ste-Marie et al., 2012). Moreover, VSM provides a customizable approach that provides an individualized focus on the learner’s unique strengths and needs, and its effectiveness is not dependent on the individual’s ability to engage in repeated bouts of physical practice.
We aimed, in the current study, to create a customized practice context using the PSR variation of VSM that would likely promote skill acquisition in a diverse group of people living with CP. Since providing choice to the learner increases autonomy over the learning process and motivation to learn and has been shown to promote skill acquisition (Ste-Marie, Carter, et al., 2020; Wulf & Lewthwaite, 2016), we had participants self-select a skill they wanted to learn. We hypothesized that participants would complete self-selected tasks in a faster time and with higher automaticity, as measured by their reductions in movement self-consciousness and conscious monitoring of performance (which would also result in improved well-being) (Adie et al., 2012; Wulf & Lewthwaite, 2016), following a customized VSM intervention.
Method
In this study, we used a case series approach with eight participants in light of the challenges associated with recruiting a larger participant group and because of difficulty comparing averaged improvements across groups of individuals with widely varying initial abilities. In addition to its potential contribution to these participants’ ability to learn, we considered participant autonomy in selecting the movement task to be important because participants best know which skill improvements might create the greatest benefit to them in their work, social or home lives.
Participants
We invited individuals living with CP to participate in this study, giving a specific emphasis to those with spastic hemiplegic CP (though other classifications were also encouraged) who demonstrated deficits in their ability to perform a self-selected functional goal-oriented movement skill. Recruitment was through advertisements placed on notice boards in physiotherapy clinics and hospitals in Sydney, New South Wales, Australia. Further, online advertisements were posted on a CP Alliance website, employment websites and social media platforms associated with the university and on general websites such as Facebook and Twitter so as recruit participants even outside of the Sydney metropolitan area. The advertisements detailed the tasks within the study and the participant reimbursement for time and travel per test session of $20AU. While thirty individuals expressed initial interest in the study, only 18 engaged in an initial contact; and, of these, only eight individuals aged 18-51 years (M age = 32.1, SD = 12.6 years) gave informed consent to participate in the study. We did not request medical reports from the participants, though each participant provided their CP classification and any relevant details as to their abilities. Six of the participants had spastic hemiplegia while two had spastic quadriplegia. All participants were highly independent in their day to day living and engaged in work (n = 6) or study (n = 2). Four participants (two with hemiplegia and two with quadriplegia), occasionally required assistance with tasks such as transportation. All participants were cognitively able to understand the study.
Procedure
Once each participant gave fully informed consent to participate in the study, based on the research protocol that received ethical approval from the governing university (H11453), they were asked to complete the Canadian Occupation Performance Measure (COPM)© (Law et al., 2014), which assisted us with the identification of the participants’ preferred learning task for the study and their perceived importance of those activities in their lives (e.g., self-care, productivity and/or leisure). The questionnaire also captured participants’ satisfaction with their performance at each stage of testing, measured on a 1–10 scale with 1 being the lowest rating and 10 the highest. The COPM is considered a reliable and validated performance measurement tool for clinicians working with individuals with various disabilities (Lalor et al., 2019; Roe et al., 2019; Thyer et al., 2018).
Participants also completed a five-item well-being survey created by the researchers for this study, in order to gauge changes in mood via open ended items (see Appendix). They also completed the Movement Specific Reinvestments Scale © (Masters & Maxwell, 2008) which has ten items designed to examine movement self-consciousness (MSC) in addition to conscious motor processing (CMP). This scale was validated by Kal et al. (2016). MSC items measure how the person feels about themselves as they move while CMP items measure how much attention the person directs toward performing a skill. Each item required a response from one of six options ranging from strongly agree to strongly disagree. Individuals who score high on both measures are presumed to perform skills with a lower degree of automaticity. These variables can be high in those living with movement disorders (e.g., stroke), and they have been associated with anxiety and poor confidence in relation to completing tasks (Masters, 2013). Therefore, the inclusion of this questionnaire provided a tool that captured data on movement specific psychological processes that may be impacted by an intervention that uses the PSR variation of VSM and physical practice. Overall, the questionnaire section of each testing session took approximately 15 minutes to complete.
All participants were filmed by the researchers while completing 10 trials of their self-selected movement task as quickly as possible. Filming and testing took place in the participant’s home environment, except for one participant who chose to attend the university of the lead researcher for this activity. Filming was completed in less than twenty minutes. The footage was then examined by a member of the research team (the same researcher for all participants), to determine which trials provided the most efficient (shortest time taken in addition to smoothness of path) examples of performance for that individual. These trials were edited into a training sequence. Participants were then asked to watch the training video once daily in addition to physically practicing the skill in their home environments 10 times a day as quickly as possible, for three weeks, with compliance to the training protocol recorded at both the post tests. All participants indicated that they had complied with the training instructions.
After the intervention period of three weeks of daily training, the testing procedure was repeated (post-test 1) using the same questionnaires and physical tests. Two weeks later, the tests were completed again after a retention period without practice (post-test 2). We did not include a further period of physical training or VSM as we determined five weeks was a substantial time commitment for a group who routinely combined rehabilitation with school and/or work.
Results
We used a mixed-method case study approach to explore changes in key variables, including movement time, satisfaction and performance, movement self-consciousness and conscious motor processing (see Figure 2) and well-being (see Appendix). In line with this approach, the results for each case are presented and contrasted below (see Figure 2, Table 1). Even a cursory inspection of Table 1 reveals the large degree of heterogeneity in the participants’ responses to the intervention. No individual showed improvement on all the variables assessed at each test period, no individual showed regression on all variables at each test, and no individual showed a pattern of stasis across all variables and tests. Instead, each individual demonstrated a unique profile of improvement, regression and stasis across the different variables and tests. While the mean data across this small group, as presented in Table 2, show slight improvements in movement time, mean satisfaction and performance and mean movement self-consciousness from pre-test to post-test 1 to post-test 2 and slight improvements in conscious motor processing from pre-test to post-test 2, none of these changes at the group level were statistically significant when analyzed using a one-way ANOVA and paired-sample T-test, nor did they appear clinically meaningful. Moreover, detailed inspection of each case demonstrated that it was not possible to cogently summarize group findings or to posit variables such as task or type of disability as mediators of the participants’ different responses to the intervention. In the remainder of the results section, we describe each individual’s response pattern.
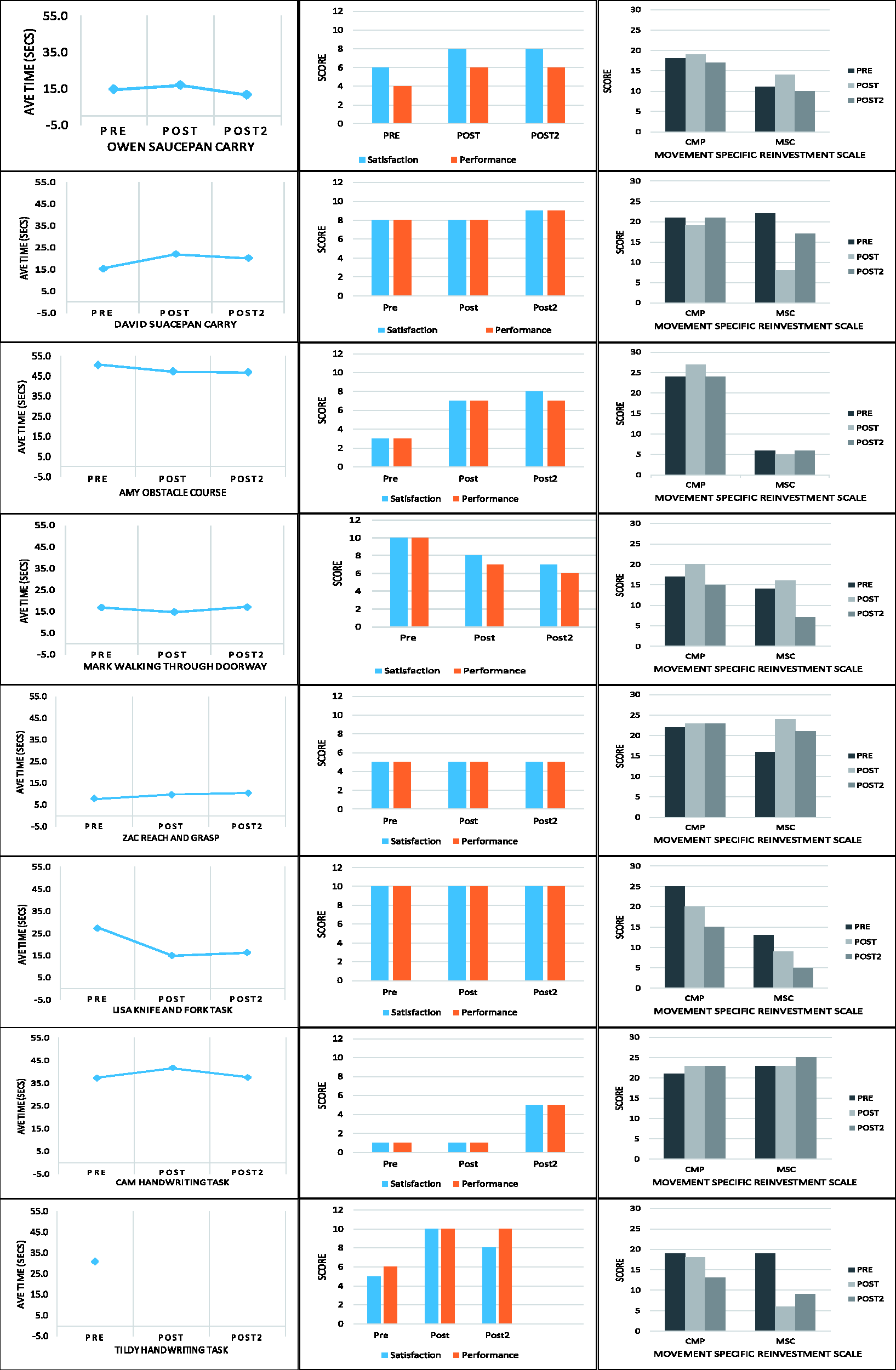
Participant Test Results.
Summary of Learning Outcomes for Each Participant, on Each Variable, Between Pre-Test, Post-Test 1 and Post-Test 2.
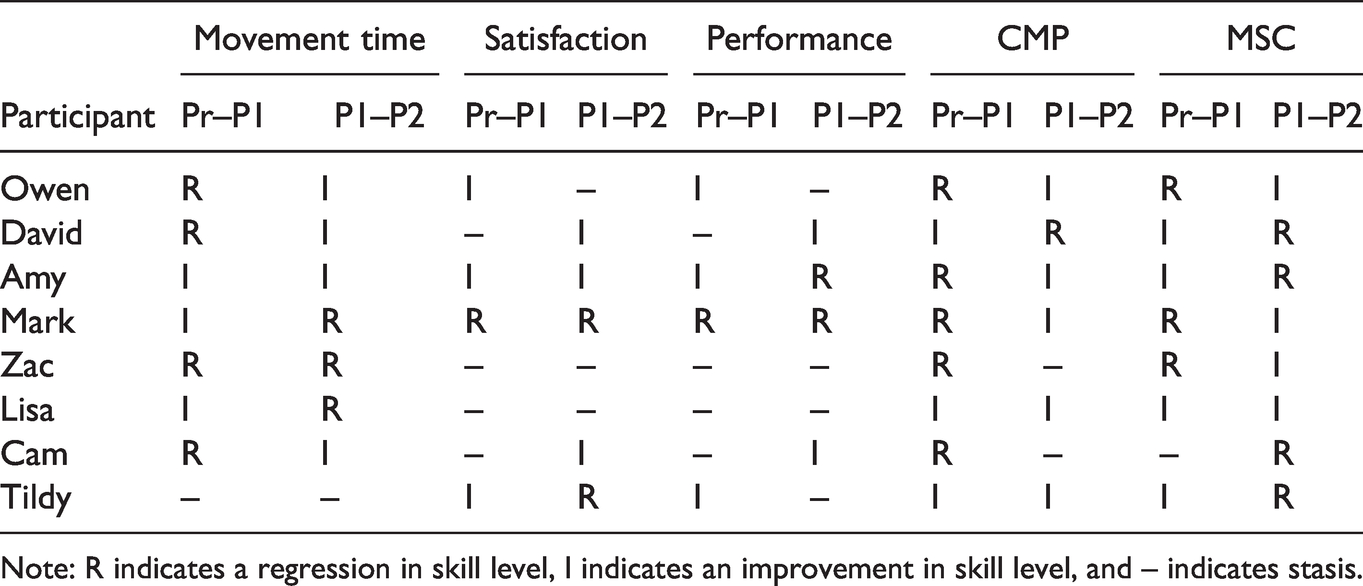
Note: R indicates a regression in skill level, I indicates an improvement in skill level, and – indicates stasis.
Group (n = 8) Means (and SDs) for Each Variable From Each Testing Session.
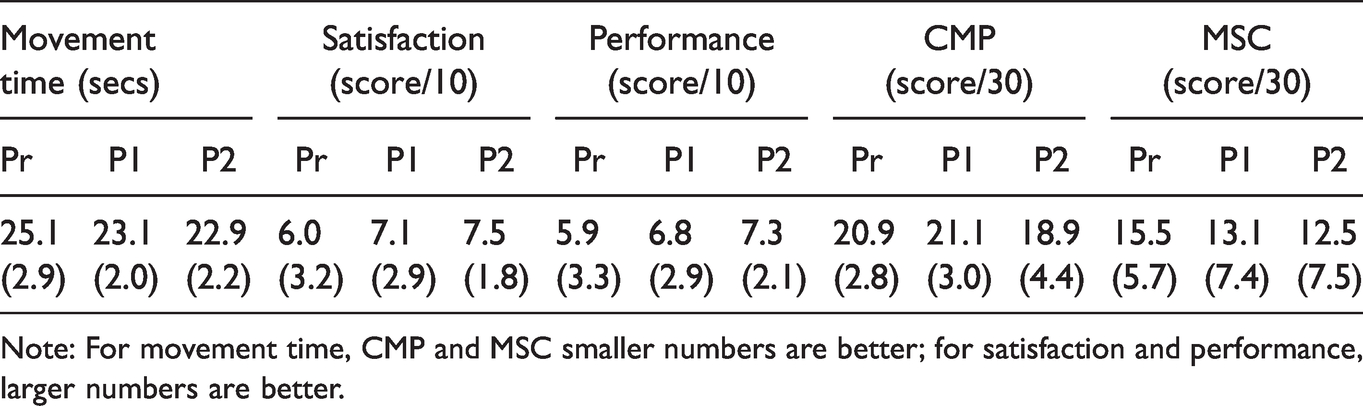
Note: For movement time, CMP and MSC smaller numbers are better; for satisfaction and performance, larger numbers are better.
On the COPM questionnaire, many participants verbalized that the ability to perform tasks at comparable speeds to their peers was very important in different spheres of their lives, and that their productivity and self-care was more important than their leisure time on the COPM questionnaire. For example, Cam (writing task) stated that he wished to be involved in the study because he wanted to become faster at writing notes at work. While he said his employer was very supportive, he felt less competent than his workmates, and this affected his self-esteem and confidence. Despite his adherence to the intervention, neither Cam’s movement times (Table 2, Figure 2) nor his CMP and MSC (MSRS) scores improved (Table 3). However, there were positive changes in the psychological variables that measured skill execution satisfaction and performance (Table 4). His responses to well-being items suggested minimal, if any, changes in his well-being though he did suggest ‘more training may be required’ to observe any changes.
Individual Percentage Differences for Participant Movement Times Between Pre-Test and Post-Test 1 and Between Pre-Test and Post-Test 2.
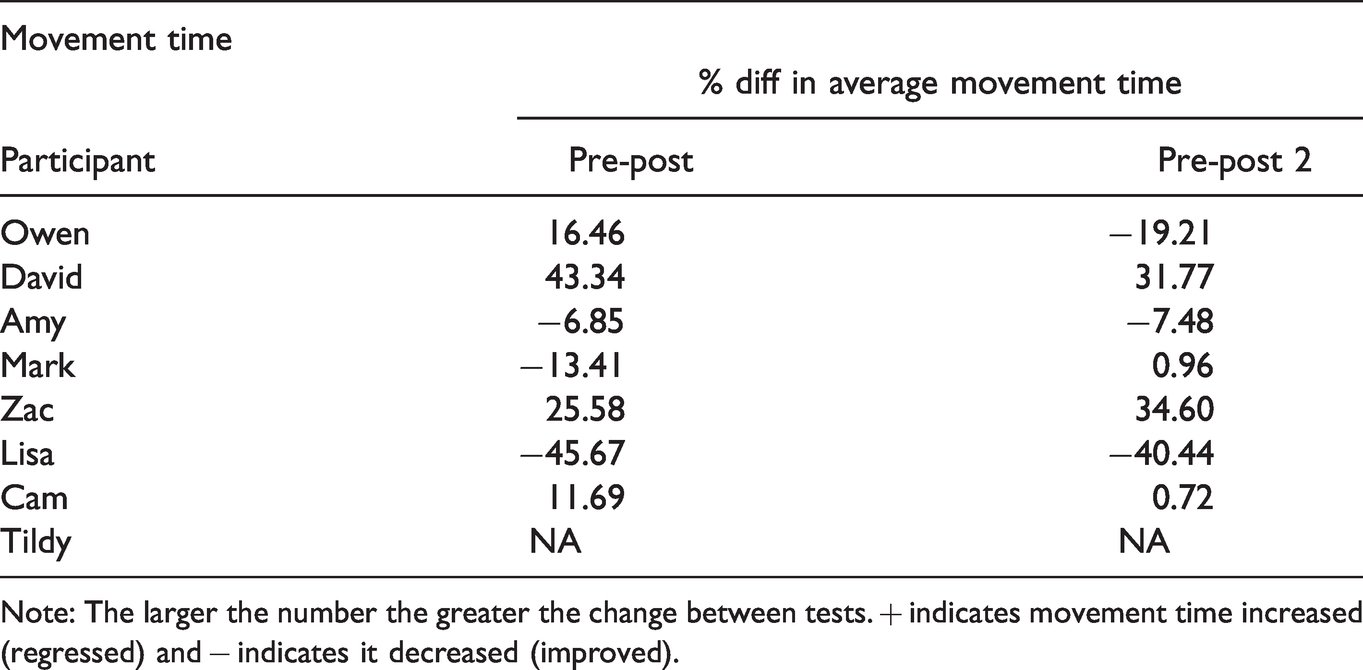
Note: The larger the number the greater the change between tests. + indicates movement time increased (regressed) and − indicates it decreased (improved).
Individual Participant Scores (Percentage Differences) on Canadian Occupational Performance Measure (COPM).
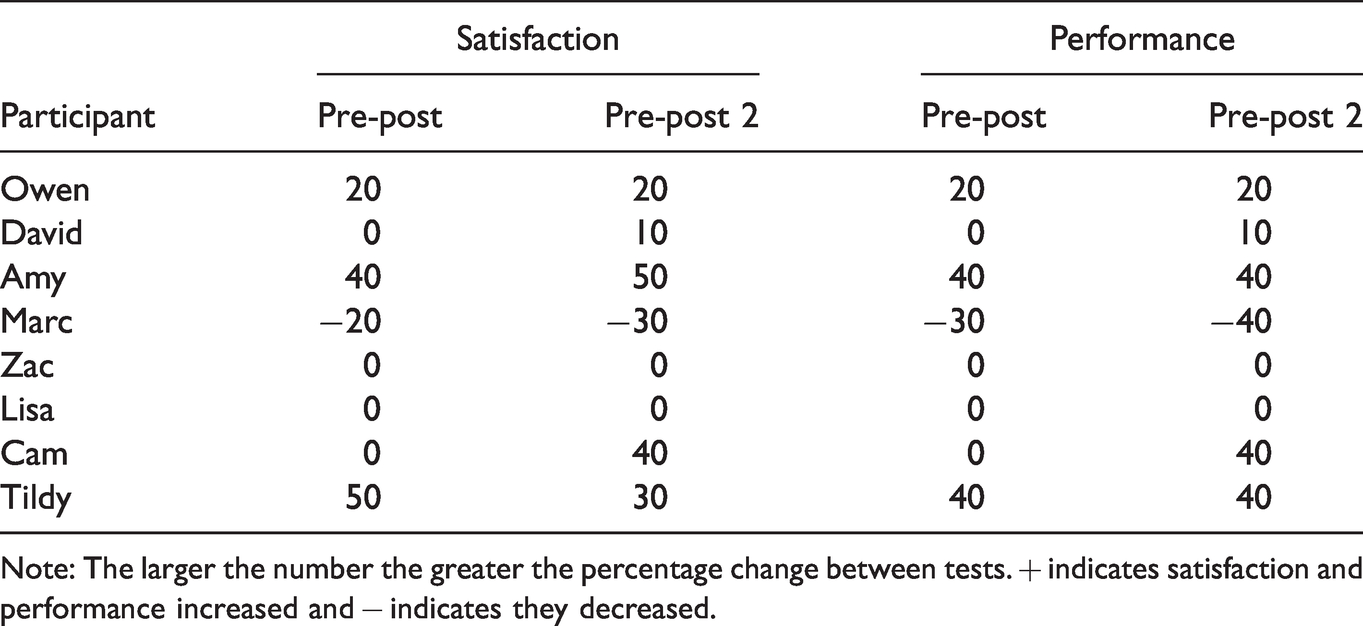
Note: The larger the number the greater the percentage change between tests. + indicates satisfaction and performance increased and − indicates they decreased.
In contrast to Cam, Amy improved her movement time throughout the study for her chosen task (a self-designed obstacle course), self-selected to help her improve her ability to navigate objects while in motion. She also demonstrated consistent increases in satisfaction and performance scores between testing sessions, though her MSC and CMP scores remained stable throughout (Table 5). Amy’s responses to well-being items showed that she felt the training improved both her movement ability and an awareness of her movement patterns, though she did not comment on whether this improved her mood.
Individual Participant Scores (Percentage Differences) on Movement Specific Reinvestment Scale Test.
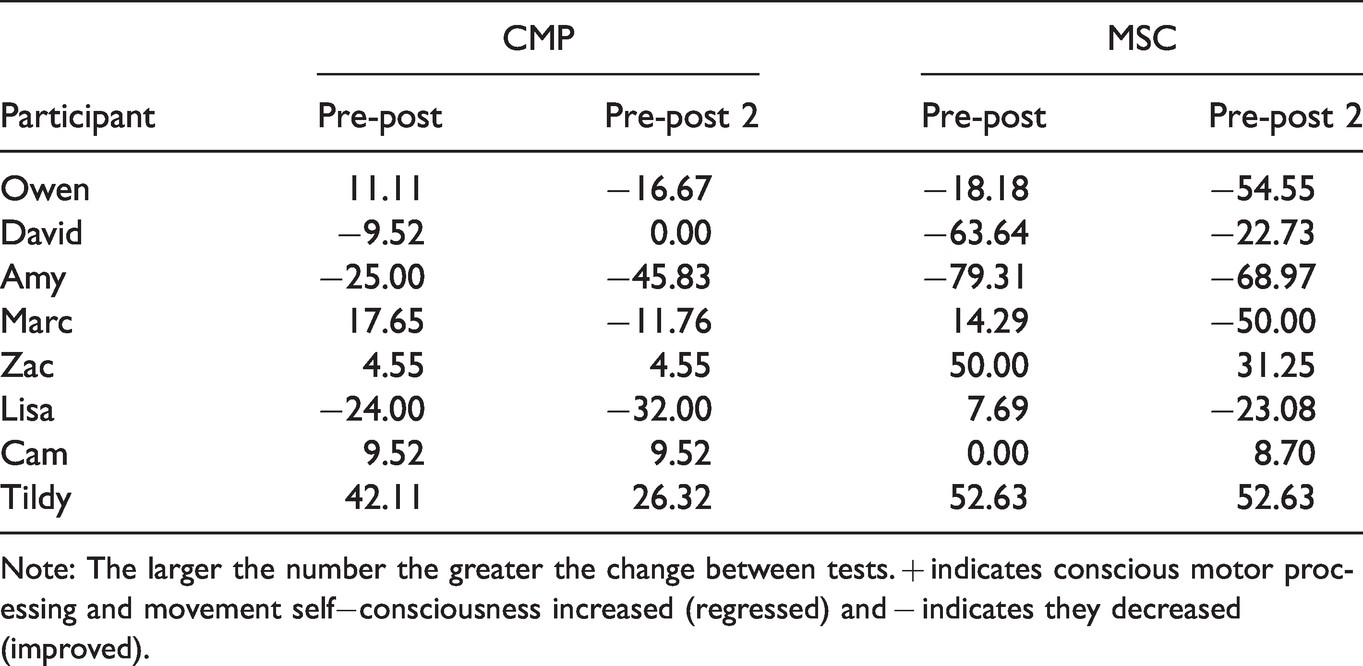
Note: The larger the number the greater the change between tests. + indicates conscious motor processing and movement self−consciousness increased (regressed) and − indicates they decreased (improved).
Mark (walking through a doorway) and Lisa (knife and fork manipulation) also improved their movement times between the pre-test and post-test; however, like Cam, some of their improvements were lost during the post to post-test 2 period (more so for Mark than Lisa). This may suggest that continued training was important for these participants (Table 3). While Lisa said that her mood did not change during the course of the study, her response to the well-being items and her anecdotal comments suggested that she became more likely to initiate tasks rather than ask for assistance (previously her normal practice), suggesting some changes that were below the level of her conscious awareness. Mark also reported no changes in mood but commented that the study intervention was working, and he had fewer injuries (from bumping into objects). He rated his satisfaction and performance with his skills as being lower than at baseline (Table 4), whereas Lisa indicated no change in these variables. Both demonstrated substantial improvement in MSC and CMP scores (Table 5).
Participants Owen and David (who filled a saucepan with water which was then carried while walking to a stove top), and Zac (reach and grasp task with a liquid filled cup) showed slower movement times between pre-test and post-test; however they improved during the post to post-test 2 period. Zac and David, remained relatively stable on all other measures throughout the study except CMP, whereas David improved between pre and post-test and Zac regressed (Table 3). Owen improved his satisfaction and performance ratings from pre to post-test, and he improved his MSC and CMP from pre to post-test2 (Tables 4 and 5).
Further, on well-being items, Owen indicated that the method used in the study improved his ability and would result in increased confidence with additional training. In contrast, Zac felt the intervention had not worked and did not believe, given his age (43 years), that this method would yield improvements in the long-term. David expressed the same sentiment, noting that, while the intervention may have led to some improvement, more conventional physical therapy techniques were more useful.
Tildy, who also chose a handwriting task, was the only participant tested via a video conference call. Due to glitches with the video conference technology, the recorded video footage from post and post-test2 was of insufficient quality to gain consistent measurements. Despite the absence of this information, she had substantial improvements in her satisfaction and performance scores in addition to her scores on the MSC and CMP (Tables 4 and 5). She also indicated that she thought the intervention had improved her ability and she felt happier because she was more confident.
Discussion
The purpose of this study was to examine the effectiveness of the PSR variation of VSM combined with physical practice as a customizable strategy for improving motor skills of individuals living with CP. We used a mixed-method case study approach to explore changes in key variables, including movement time, satisfaction and performance, movement self-consciousness, conscious motor processing and well-being. Motor learning research has shown that physical practice and modelling are effective methods for improving movement skills (Rymal & Ste-Marie, 2019; Ste-Marie, Lelievre, et al., 2020), and we considered this combination a particularly useful strategy in the current study because the capacity to endure extended periods of physical practice is often hindered by physical limitations associated with CP.
Most of the eight participants in this study demonstrated improvements in at least one of the variables we examined, while some demonstrated relatively stable performance across the study and, notably, others regressed in performance on some measures. Our findings highlighted challenges associated with the variability in this population and the associated difficulties designing general interventions to help participants with physical challenges improve performance on a specific task. Even when participants self-selected the movement tasks to promote their autonomy and motivation and facilitate their learning, outcomes were highly variable. These findings help to explain why so few studies have examined the effects of modelling on performance and learning in clinical populations (e.g., Ste-Marie et al., 2012).
Although our PSR VSM intervention yielded mixed results, we believe it has potential value in clinical settings based on evidence for its effectiveness with special populations (e.g., Dowrick & Raeburn, 1995; Steel et al., 2018) and its theoretical utility for facilitating skill acquisition when specific strategies and individual needs can be matched. For example, following the discovery of a mirror neuron system in the brains of monkeys, several investigators (Di Pellegrino et al., 1992; Rizzolatti et al., 1996) showed that action observation is associated with increased cortical excitability in the primary motor cortex and in brain areas involved in movement planning, anticipation and execution (e.g., Gangitano et al., 2001; Gonzalez-Rosa et al., 2015; Holmes & Calmels, 2008; Loporto et al., 2013; Wrightson et al., 2016). Action observation appears to prime the neural structures that underlie action execution, leading to adaptations in the CNS that facilitate action production.
If action observation does prime neural structures and facilitate action production, why did the current PSR VSM intervention produce such inconsistent effects? Perhaps the PSR version of VSM provided a relatively weak type of intervention for learners attempting to improve a strong habit that is resistant to change. It is important to note that most experimental studies of motor learning focus on the acquisition of novel skills rather than the refinement of existing skills (Magill & Anderson, 2020). The FF variation of VSM may be more effective for the refinement of existing skills because it provides participants with the illusion they are capable of performing a skill that is actually beyond their current capabilities. In contrast, the PSR version simply highlights for the learner the best performance they are capable of demonstrating at the current time. In other words, the FF method draws learners into the future by showing them a more skilled version of themselves, whereas the PSR method may reinforce the learner’s present less-skilled self-perception. A recent study by Nuara et al. (2019), showing that children with CP were more likely to benefit from an action observation intervention when they were paired with a more skilled peer seems to provide support for the benefits of observing more skilled models. Of course, it is also possible that the current intervention was too short to have clear effects when learners attempted to improve well established skills. Further research is needed to determine whether the FF variation of VSM and/or a longer intervention might prove more efficacious than the current intervention for people living with CP.
A number of other factors unique to each participant likely contributed to our finding of inconsistent effects of PSR VSM intervention among this participant sample. Researchers have studied individual differences in learning for well over a hundred years (e.g., Ackerman, 1987). Researchers have documented large variations in the rate at which learners acquire skills, retain them and transfer them to novel variations or new contexts (e.g., Pacheco & Newell, 2018a, 2018b), to a wide variety of factors, including the learner’s physiology, morphology, aptitudes, needs, attitude, and personality (Ackerman, 2014). Differences in working memory capacity and speed of information processing (e.g., Ackerman & Cianciolo, 2000) as well as motivation and attention (e.g., Wulf & Lewthwaite, 2016) are particularly important contributors to differences in motor learning. Though not measured in the current study, variations in these factors, combined with variations in each participant’s level of disability, likely made major contributions to our findings of inconsistency in the effects of PSR. Future research might measure some of these factors to provide an individualized understanding of what factors may affect each participant. In addition, researchers may consider addressing the heterogeneity in participants’ response to PSR by giving learners control over the way in which VSM is delivered to them. Researchers have reported considerable individual differences in learners’ desire for control over their practice context, their practice schedule, and the schedules by which demonstrations and augmented feedback are provided (see Ste-Marie, Carter, et al., 2020 for an overview). However, regardless of these differences, providing learners with control over these aspects of practice appears to facilitate motor learning (Ste-Marie et al., 2020b).
Limitations and Directions for Further Research
Chief among this study’s several limitations was our small sample size, as dictated by recruitment difficulties. Of course, this problem dictated the individualized nature of our case study approach, and, across this multiple case study series, eight cases helped demonstrate the heterogeneity our study highlighted. Several potential participants demonstrated initial enthusiasm for the study, but the time commitment made it difficult for them to fit this protocol into their already busy schedules. The same time commitment also prohibited extending the length of the study for those who agreed to participate. Future researchers should collect multiple baseline measurements in order to assess the participants’ pre-test skill stability. Another limitation connected to the time commitment issue was the length of the training in this study design. As noted above, considerably more practice and exposure to the PSR variation of VSM may have been necessary to ensure the types of improvements seen in previous PSR VSM studies with special populations. A final limitation concerned the procedures used to ensure compliance. Based on the participants’ initial enthusiasm for the study, we assumed that we could adequately assess compliance through self-report at the post-tests. In hindsight, daily compliance data should have been collected by video recording the training sessions or having participants/caregivers keep diaries of their training sessions. A further question for future researchers is whether permitting participants to self-select motor learning skills contributed in some cases to participants choosing skills that were particularly resistant to change over short intervention periods. With this type of multiple case study training experience, overseers of this type of motor learning in working with specific populations might be better able to gauge what motor learning skills to target for optimal gains so as to best motivate continued learning with early successes and build upon skill improvements.
Conclusion
Through an eight person case study series, this paper highlighted difficulties associated with designing motor skill training interventions for individuals living with CP. The heterogeneity of symptom presentation in our small participant sample and the self-selected tasks our participants practiced was mirrored by participant heterogeneity of responses to the combined physical practice and PSR VSM intervention. Several factors might explain the heterogeneity in these outcomes, and these factors warrant further study. Our findings highlight the need to consider individual differences when designing interventions to improve motor skill performance and learning among individuals with motor impairments. Much more research is needed to identify what interventions are likely to work for which individuals. Meanwhile, clinicians are encouraged to combine knowledge of prior research with individualized trial and error experimentation to identify what strategies are likely to work best for each client.
Footnotes
Appendix
Author Contributions
Kylie A. Steel contributed to every aspect of the study and wrote the first draft and subsequent versions of the manuscript. David I. Anderson contributed significantly to the conceptualization of the study, data analysis, and manuscript development. Caroline A. Smith was involved in the conceptualization of the study, the grant application which funded this study, and reviews of the manuscript. Eathan Ellem, Karen P.Y. Liu, Andrew Morrison-Gurza, Tinashe Dune, Lauren Fairley contributed to aspects such as recruitment, data entry, and manuscript editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a Western Sydney University Women’s Fellowship grant awarded to the first author.