
Abstract
Balance problems have been found among 57% of adults with Intellectual Developmental Disorder (IDD). Moreover, these adults have only partially participated in conventional activity programs. There is a clear need for new interventions that will enhance these individuals’ interest and motivation toward improving their balance skills. Virtual gaming training experiences are a promising prospect in that regard. The purpose of this study was to examine the effect of virtual reality games on improving balance for adults with IDD. We recruited 31 individuals with mild-moderate IDD who had fallen at least twice in the year prior to initiating this intervention, and we evaluated these participants using the Timed Up and Go (TUG) test. The participants were randomly assigned to control and experimental groups, and only the latter group took part in a series of twelve 30-minute bi-weekly virtual game sessions, designed to improve balance using the SeeMe virtual game system. We found significant (p < .001) pre-post improvements in balance abilities in the experimental group and no significant pre-post change in the control group (p < .77). These data suggest that virtual game technology is a viable tool for improving balance among adults with IDD.
Introduction
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013), three criteria must be met to diagnose Intellectual and Developmental Disorder (IDD): (a) deficits in intellectual functioning; (b) deficits in three domains of adaptive functioning including conceptual (academic), social, and practical abilities; and (c) symptom onset occurring during the developmental period. The prevalence of IDD in the general population has been reported to vary from 1-3% (Harris, 2006; King et al., 2009; Maulik et al., 2011). In a review of 52 articles, Maulik et al. (2011) found that the overall prevalence of IDD was 1.37%, regardless of age or gender.
Of relevance to the IDD population (see below) are falls. A fall is defined as, “An unplanned descent to the floor (or to an extension of the floor) …” (Currie, 2008, p. 3). Fall prevention requires adequate balance, which is a complex ability entailing continually adapting reactions to incoming sensory information from the visual, proprioceptive and vestibular systems (Hsieh et al., 2001; Katz & Lazcano-Ponce, 2008; Rubenstein & Josephson, 2006). As individuals with IDD present an array of disabilities (e.g., ataxia, paresis, movement disorders, epilepsy, sensory limitations), they are more prone to falls than peers without IDD (Willgoss et al., 2010). The incidence of falls within the general older adult population is around 33%, while the incidence of falls among older adults with IDD is about 57% (Willgoss et al., 2010). Thirty-two percent of all falls by individuals with IDD result in injury or death (Chiba et al., 2009; Willgoss et al., 2010). Moreover, falls are associated with fall-related psychological concerns for both the individual at risk (Payette et al., 2016) and family members and caregivers. Fall-related psychological concerns lead to activity avoidance that, in turn, reduces physical fitness and increases the likelihood of a sedentary lifestyle that tends to be typical of individuals with IDD (Chang et al., 2004; Chiba et al., 2009; Harlein et al., 2009; Rubenstein & Josephson, 2006). Efforts to prevent falls through intensive physical activity training for individuals with IDD may be impeded by difficulty persuading them to cooperate willingly with these interventions, meaning that encouragement and highly motivating programs are often needed (Lotan, 2007; Temple, 2007). For all these reasons, virtual gaming as a motivating physical activity has been proposed (Yalon-Chamovitz & Weiss, 2008).
Since the mid-1990s, daily life for many adults has become permeated with technology-driven activities, especially due to the wide availability of mobile devices and of low-cost personal computers that can run relevant software for a variety of rehabilitation populations (e.g., Standen et al., 2001). Virtual game technology, and more specifically, virtual gaming, has become commonplace, and it is now part of a clinician’s repertoire of available rehabilitative tools. As numerous clinicians and researchers continue to examine ways to increase physical activity participation and reduce the sedentary lifestyle of individuals with IDD (Oppewal et al., 2018), virtual game technology represents new means of achieving both goals.
Virtual gaming may be described as the use of computer-based interactive simulations to present users with practice opportunities for engaging in realistic activities through artificial environments (Rizzo & Kim, 2005; Weiss et al., 2006). Virtual games provide players with an experience in two or three-dimensional simulated virtual environments (VEs) with which they can interact and respond at different levels of motor and cognitive ability to perform tasks that are motivating, meaningful and purposeful (Eden & Bezer, 2011; Parsons & Mitchell, 2002; Rheingold, 1991; Tam et al., 2005; Weiss et al., 2003).
To date, a number of VEs have been used for people with IDD, permitting an examination of the potential of virtual reality and virtual games for teaching life skills, such as route learning (Mengue-Topio et al., 2011), street crossing (Wright & Wolery, 2011), preparation for giving witness evidence in a court of law (Cooke et al., 2002), coping during natural disasters such as earthquakes (Tarnanas & Manos, 2001), shopping (Tam et al., 2005), improving physical fitness (Lotan et al., 2009; 2011), augmenting sensorimotor functioning (Wuang et al., 2011), and increasing cognitive skills, such as assessing sequential time passage (Passig, 2009) and spatial perception (Akhutina et al., 2003). Other researchers have studied the practicality of VEs for social skills training (Parsons & Mitchell, 2002; Standen et al., 1998) and as a medium for leisure activities (Walker & Sylwester, 1998; Yalon-Chamovitz & Weiss, 2008). In their review of various virtual reality rehabilitation applications for people with IDD, Standen and Brown (2005) supportively concluded that those few empirical studies that have examined VE use for people with IDD have shown it to be potentially effective and meaningful. Or as so eloquently expressed by the title of their article, “Virtual Reality in the Rehabilitation of People with Intellectual Disabilities,” virtual reality has a role in removing the barriers that impede rehabilitation for people with intellectual disability.
Despite the severely limiting balance problems that are common among individuals with IDD (Chiba et al., 2009; Willgoss et al., 2010) and the efficacy of virtual gaming for improving balance in other populations (Mao et al., 2014), no prior study has reported virtual game use for balance improvement among individuals with IDD. While virtual gaming appears to provide a readily available, low-cost, easy-to-operate, adaptable and motivating approach, no research has yet explored the use of VE-based games to affect balance problems in individuals with IDD. Thus, this study was intended to fill this research gap. We compared an experimental group of participants with IDD who received exposure to virtual game balance-improvement training with a control group of participants with IDD who received no virtual game training. We hypothesized that our experimental group would show significant balance improvements relative to the control group.
Method
Ethics
This protocol received ethical approval from the Institutional Review Board of the University of Haifa (229/13), from the head scientist at the Ministry of Welfare and Social Affairs, and from the management of the Bnei-Zion and Neve Menashe residential centers. A parent or legal guardian of each participant signed a written statement of informed consent before the research commenced for that participant.
Participants
All participants’ mild-moderate levels of IDD were determined by the national placement committee, under the auspice of the ministry of welfare. We randomly assigned 16 adult participants to an experimental virtual game-treatment group (8 males, 8 females; age range: 30–77 years, Mage = 51.8, SD = 11.2 years) and 15 adult participants to a no-treatment control group (8 males, 7 females; age range: 24–63 years, Mage = 45.6, SD = 13.8 years). A research assistant who was blind to the treatment program, participant assessments and data analyses made these random assignments by selecting the participant’s names from a hat, while blindfolded. We based the sample size on the number of participants used in previous intervention programs of this kind and have managed to present statistically significant results (n = 12; 4; and 20 respectively) (Brien & Sveistrup, 2011; Bryanton et al., 2006; Delasta Lazzari et al., 2015).
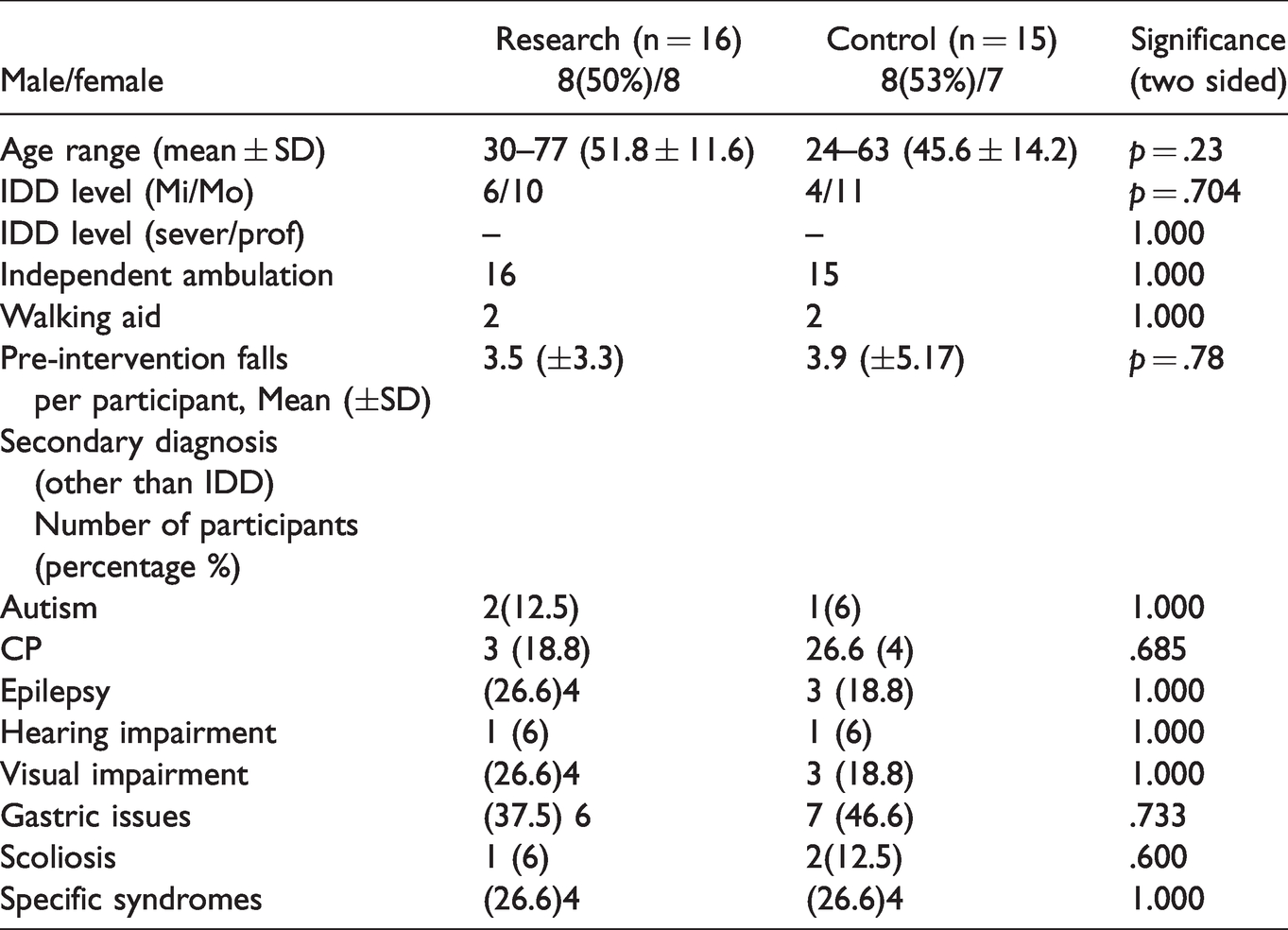
Participant inclusion criteria included a requirement that the participant have experienced more than two falls in the year preceding the intervention, with no sustained injury that prevented them from engaging in the light-moderate physical activity demands of the intervention program. This criterion was set to avoid accidental falls during the participants’ research engagement. Other inclusion criteria were cognitive abilities sufficient for understanding the virtual game requirements, demonstrated sufficient visual and auditory acuity (with correction, if necessary) to see the monitor display and hear the auditory feedback, and demonstrated shoulder range of motion greater than 130° flexion and abduction. These criteria were based on our previous research findings that individuals at a level lower than mild IDD were unable to fully enjoy and actively use virtual gaming (Lotan et al., 2011). All participants were approved to enter the research procedure by the residence physician. Participants were excluded if they presented neuromuscular or cardiovascular pathology that prevented them from participating in a moderate level of physical activity via video gaming. After assigning participants to the experimental and control groups, we experienced no participant drop-outs. In addition to participation in this study protocol, both groups continued their regular daily activities such as going to sheltered work activities each morning and participating in afternoon leisure activities (which were similar for all participants). See Table 1 for participant characteristics.
Demographic and Medical Characteristics of Participants.
Instrumentation
SeeMe Virtual Games
SeeMe is a camera tracking, video-capture, gesture-operated virtual gaming system, run with a Microsoft Kinect three-dimensional (3 D) camera, laptop computer and a connection to any large monitor/TV (further details can be found at the website: http://www.virtual-reality-rehabilitation.com/products/seeme/tasks-overview/gym).
This system presents a suite of video games that have been customized for a range of rehabilitation populations, including those with neurological and orthopedic conditions. The SeeMe games may be adapted to accommodate different levels of cognitive and motor difficulty, enable the recording of game results, and allow for user follow-up training from session-to-session. The games are operated by movements of the upper and/or lower extremity and trunk, as designated by the operator, usually a therapist. All SeeMe games used in this study were able to challenge balance abilities of the participants and included Warm Up (introducing the virtual games to the user), Window Cleaner (requiring the user to move upper body and limbs in wide lateral movements), React (a ball randomly appears at the side of the screen for a limited time – requiring the user to move upper body and limbs in wide quick lateral movements), Raft (drifting on a river trying to catch randomly appearing fish and avoiding randomly floating barrels - requiring the user to move laterally to both sides quickly and in sync with object movements on the screen), Gym (hitting or kicking a square randomly appearing at different heights and angels from the participant's avatar - requiring the user to quickly move upper and lower limbs to all directions, including standing on one leg) and Sorter (ball with different colors dropping from above needs to be sorted into the appropriate color container - requiring the user to move upper body and limbs in wide coordinated lateral movements). The selection of virtual games was based on two preliminary interactions/familiarization session with the participants in which the participants selected the games that were of greatest interest to them. These sessions were not part of the research protocol, described below.
Outcome Measure
Timed Up and Go Test (TUG)
The TUG test assesses balance by measuring the time it takes for an individual to get up from a sitting position on a chair, walk in a straight line for three meters towards a mark on the floor, turn around, go back towards the chair, and sit down again. The TUG has high psychometric support when used for individuals with IDD (Salb et al., 2015) or without IDD (Boer & Moss, 2016), and it has been used frequently among individuals with IDD in numerous intervention programs (Enkelaar et al., 2012; Taylor et al., 2011). The test is especially adapted to people with IDD, as it contains simple daily living activities that are easy for individuals with IDD to understand. We provided participants with explanations regarding test performance before the initiation of this test. The test can be performed with an assistive device (e.g., cane, walker), but not with the help of another person. The TUG has specific norms, according to which a person who takes ≥10 seconds to complete the TUG is at moderate risk for falling and a person who takes ≥12 seconds to complete it is at high risk for falling (Enkelaar et al., 2012; Taylor et al., 2011).
Procedures
The participants who were allocated to the virtual gaming group received two 30-minute sessions per week for 12 weeks. They played each game for a duration of three minutes. The order of games was selected in accordance with each participant’s preference for each session, although all games had to be played. During the session the investigator stood behind each participant using a transfer belt around the participant’s chest in a way that ensured safety yet did not impede performance (as demonstrated during initial pilot trials); the balance task was therefore both challenging and safe. An evaluator who was blinded to the experimental procedure and the participants’ group allocations assessed participants in both groups for balance (TUG) prior to and following the intervention. The TUG evaluation included four tests (including two familiarization trials) for each participant at each evaluation cycle, with the mean of the last two tests used as the outcome measure.
Data Analysis
We analyzed data using the Statistical Program for the Social Sciences (SPSS, Version 23.0, IBM Inc., Chicago, IL USA). Statistical analyses included the computation of descriptive statistics (means and standard deviations) for the demographic and physical performance variables. We checked the normality of the data distributions with the Kolmogorov-Smirnov test and found them to meet criteria for assumptions of normality and homogeneity, allowing the use of parametric tests. We conducted independent t-tests (continuous variables) to determine group differences. Bivariate analyses included one-way analysis of variance tests for balance test comparisons between control and experimental groups, with group demographic differences treated as covariates (analysis of covariance). Effect sizes were also calculated (Lakens, 2013), and we considered an effect size at a power of less than 0.5 to be a small effect, an effect size at power between 0.5–0.8 as a moderate effect size, and an effect size at power larger than 0.80 as a large effect (Cohen, 1988). We set statistical significance at p < .05 level for all calculations.
Results
Prior to intervention, we found no statistically significant differences between the control and experimental groups on comparisons of the participants’ age, gender, cognitive ability level, number of falls before the intervention, and use of walking aids versus independent walking. Using Student's two-way t-tests, differences for the pre-intervention TUG tests between the experimental group (M = 14.6, SD =5.2) and the control group (M = 14.5, SD = 5.1) were not statistically significant. Effect size was calculated according to Cohen's d: (14.5–14.6)/5.150243 = 0.019417 (Lakens, 2013).
As shown in Table 2, comparing pre-intervention (M = 14.5, SD = 5.1) and post-intervention (M = 14.3, SD = 5.9) TUG scores for the control group revealed no statistically significant difference (p = .933). Effect size was calculated according to Cohen's d: = (14.5–14.3)/5.514526 = 0.036268 (Lakens, 2013).
TUG Means (and Standard Deviations) for Experimental and Control Group Participants.
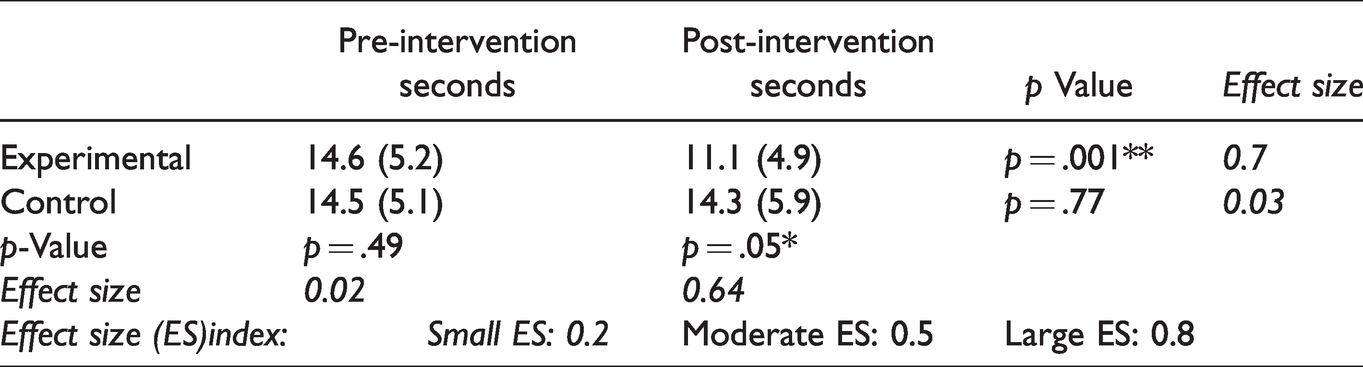
There was, however, a statistically significant difference between the pre-intervention (M = 14.6, SD = 5.2) and post-intervention (M = 11.1, SD = 4.9) TUG scores for the experimental group, reflecting a significant improvement for this group, (t = (15) = 5.255; p < .001. Cohen's Effect size is: Cohen's d = (14.6–11.1)/5.052227 = 0.7 (Lakens, 2013).
There was also a statistically significant (p = .0049) change score (after-before) at the post-intervention TUG test between the experimental group (M = 11.1, SD = 4.9) and the control group (M = 14.3, SD = 5.9), t (−3.772) = 28.97. Cohen's effect size was: Cohen's d = (14.3–11.1)/5.423099 = 0.6 (Lakens, 2013).
Discussion
In this study, a group of participants with IDD, residing in residential care centers, who had a history of multiple falls, received 12 bi-weekly, 30-minute sessions, aimed at improving balance via virtual gaming. We compared this group to a no-treatment control group of similar participants with IDD. The groups were compared and found to be comparable on pre-intervention variables such as: balance, number of falls and use of walking aids. When comparing pre-intervention and post-intervention testing with the TUG test, only the experimental (i.e., virtual game training) group showed a significant improvement in balance following the intervention.
These results suggest that repeated bi-weekly virtual gaming sessions can be effective for enhancing balance skills of individuals with mild to moderate IDD. This result has important implications for this population, and it emphasizes the strength of virtual gaming as an effective way to intensify and facilitate exercise adherence to enable positive and significant exercise results for individuals with IDD. The power of virtual gaming as a useful and effective way to implement physical activity programs corresponds with previous research (Yalon-Chamovitz & Weiss, 2008) demonstrating that virtual gaming of this kind (Lotan et al., 2009, 2011) improved physical fitness on the Twelve Minute Walk Test (McGavin et al., 1976), Total Heart Beat Index (Hood et al., 2002), and Energy Expenditure Index (Piccinini et al., 2006).
Other findings also support the present results. For instance, 12 children with cerebral palsy (CP) participated in a VR gaming-based exercise program. The participants reported feelings of fun and enjoyment during the VR exercises. Moreover, the project found that the participating children completed many repetitions of the exercises. Our results are similar to those suggesting that VR gaming improved exercise compliance, and enhanced exercise effectiveness (Bryanton et al., 2006). In a different study all four adolescents with physical disability showed significant improvements in various functional, mobility and balance abilities after involvement in a short-term intensive VR-gaming program (Brien & Sveistrup, 2011).
Physical fitness and balance skills of individuals with IDD have been well documented (Bonavolonta et al., 2019; Chiba et al., 2009; Fernhall et al., 1996; Graham & Reid, 2000; Willgoss et al., 2010), and such prior findings reinforced a need to discover and implement regular, effective and intensive exercise programs for this population (CDC, 1997; Lotan, 2006; Rimmer, 2004). Given secondary health risks associated with chronically poor physical fitness, a sedentary lifestyle (Draheim et al., 2002) and associated falls (Chiba et al., 2009; Willgoss et al., 2010), this need has been seen as urgent. Among individuals with IDD, there are limitations to physical activity programs imposed by the physical environment (Ruuskanen & Parkatti, 1994), especially for those who live in residential settings (Temple, 2007). Poor health may be both a result of and a further contribution to a sedentary lifestyle that further interferes with preventative participation in exercise programs (Ruuskanen & Parkatti, 1994). Similarly, individuals with IDD often receive insufficient support and encouragement for engagement in exercise from family members or caregivers (Heller et al., 2002). A key factor in this engagement is the need to find attractive and reinforcing physical activities (Temple, 2007) that have personal value for participants (Gignac, 2003). Findings from this study and others (Booth et al., 2014; Lotan et al., 2009, 2011) suggest that virtual gaming addresses these concerns. The ability of virtual gaming to motivate individuals with IDD and to promote their cooperation with and enjoyment of physical activity is likely to play an important role in helping these individuals become more physically active (da Cunha et al., 2018; Lotan et al., 2009, 2011; McMahon & McMahon, 2016).
Limitations and Directions for Future Research
Among our most important limitations was a reliance on a relatively small sample size of 31 participants with IDD (divided into experimental and no-treatment control groups). We modeled this sample size after other studies with small numbers of participants, but we did not conduct a statistical power analysis. Moreover, this small sample limits generalization of our findings to other populations, meaning that our results should be interpreted cautiously, pending replication by other researchers, as was also suggested by Bonavolonta et al. (2019). Of course, this caution extends especially to generalizations to individuals with IDD who have lower intellectual functioning (e.g., those with severe and profound IDD). While it is difficult to recruit large numbers of participants from this population, future studies should strive to increase sample size. A more diverse sample might also help address the mediating role of other demographic characteristics (e.g., gender, uncontrolled co-morbidities, etc.) in this population. We note that there were some non-statistically significant differences in the pre-intervention scores between participants in our control and research groups, mostly regarding their age and severity of balance problems. While these tendencies suggested that some participants in the control group may have been more physically fit, despite our random assignment of participants to groups, our findings suggest that this apparent limitation proved to be less important for participants in the present intervention than it might be for any future investigators. Additionally, our exclusive reliance on the TUG test to measure balance changes is a weakness that future researchers should address. Also, had we measured participants’ affect and/or motivation, we might have been more certain that they found virtual gaming pleasurable and motivating. Nevertheless, prior findings found this type of intervention enjoyable for individuals with IDD (Yalon-Chamovitz & Weiss, 2008) Finally, we included no follow-up data with which to better understand whether virtual gaming gains would persist over time. Despite previous findings suggesting that results of similar interventions persisted, at least for a month post-intervention (Bryanton et al., 2006), future investigators might better address the long-term effects of interventions of this kind and compare them to other interventions rather than to a passive control group in order to better gauge the relative value of virtual gaming.
Conclusion
In conclusion, we found a virtual gaming intervention system (SeeMe) to be both feasible and beneficial for improving balance skills among adults with mild-moderate IDD who were living within residential settings. We recommend replicating and extending this study with larger numbers of more diverse participants with IDD and with a wider array of clinically applicable field tests. Meanwhile, there is considerable promise for virtual gaming methods of improving the clinical management of individuals with IDD and there are opportunities for additional research in this realm.
Footnotes
Acknowledgments
The authors would like to thank all participants taking part in the present intervention, and their parents/legal guardians authorizing their participance.
Authors’ Note
The present work has been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments involving humans. Informed consent was obtained for experimentation with human subjects (in the present project by legal guardians of all participants). The privacy rights of human subjects have been observed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.