
Abstract
In this study, we compared the orthographic and semantic preferences of healthy adults and age and gender matched adults with aphasia, an acquired language disorder. Previous research in word retrieval and word associations has addressed semantic and phonological connections, but it has not as often included analyses of orthographic skills. We matched (on age and gender) 10 neurotypical adults and 11 older adults with aphasia and administered to both groups a lexical discrimination task requiring them to select, from 18 choices, those words that were most different from three words (daughter, laughter, son). Among the choices were foil words (e.g., daughter), orthographic similarities (laughter) and semantic similarities (son). Results revealed that individuals with aphasia focused on orthographic differences, while healthy adults chose semantic differences. Further studies should further explore this orthographic focus to develop treatment strategies, using behavioral and objective measures, for word-finding deficits in aphasia.
Introduction
Naming deficits are very common in aphasia. Naming requires processing at the level of word meaning (semantics) that is connected to word form (phonology; Dell et al., 1997; Levelt et al., 1999). Impairment in one or both of these processing stages, or the connections between them, can lead to naming difficulty (Levelt et al., 1999; Schwartz et al., 2006). Therapy for impaired naming can target either semantic or phonological processing or a combination of both. Word-finding therapies have used semantic, phonological, and orthographic cues (e.g., Nickels, 2002; Wisenburn & Mahoney, 2009).
Although single-word production models vary in their details and concepts of processing, all models assume that naming a pictured object involves activation of at least semantic and phonological processing (Caramazza, 1997; Dell & O’Seaghdha, 1992; Levelt et al., 1999; see also Rapp & Goldrick, 2000). These models depict naming activation patterns and possible breakdowns—at the semantic processing level, the phonological processing level, and/or links between these levels—that can lead to naming errors. These models provide a useful template for creating paradigms to treat aphasic naming deficits (i.e., anomia) (e.g., Abel et al., 2007; Schwartz et al., 2006). Harnish et al. (2014) reviewed semantic-based approaches to treating single-word naming deficits. Tasks typically used in these approaches included contextual priming, semantic features, cueing hierarchies, semantic decisions/semantic verification tasks, or some combination of these tasks. Studies of these approaches have reported improvements in naming accuracy, presumably by strengthening semantic representations through the priming of weakened representations in order to facilitate lexical access and retrieval processes (Nickels, 2002; Wisenburn & Mahoney, 2009).
Anomia in Aphasia
Anomia has been studied extensively in aphasia (see, for example, Goldfarb & Halpern, 1989; Halpern & Goldfarb, 2013), largely because word-finding deficits are among the most common characteristics of aphasia. Anomia is a predominant feature of aphasia and is a frequent target of intervention. However, little is known about why some individuals with aphasia with similar language profiles respond differently to anomia therapy (Nickels, 2002). A systematic review of intensity of aphasia therapy (Cherney et al., 2008) found moderate evidence for improved behavioral outcomes with more intensive therapy schedules. Massed practice for language therapy has received attention due to Constraint Induced Aphasia Therapy (CIAT), a treatment approach that uses the principles of massed practice, constraint of language output to speech, and behavioral relevance (Pulvermuller et al., 2001). Some investigators have studied intensive schedules across paradigms, including the semantic (Kurland et al., 2012; Marcotte et al., 2013) and the phonological (Vitali et al., 2007) as well as more comprehensive treatment paradigms incorporating a variety of treatment tasks.
Semantic Approaches to Treating Anomia
Semantic approaches aim to improve naming by restoring or strengthening semantic representations, which requires priming weak semantic representations (Maher & Raymer, 2004). Semantic tasks for improving naming in individuals with aphasia include: (a) generating semantic features of the object to be named, a method referred to as semantic feature analysis (SFA; Boyle & Coelho, 1995; Coelho et al., 2000; Lowell et al., 1995); (b) semantic feature verification (Kiran & Thompson, 2003); and (c) judgments about features, semantic features, or relatedness of objects (Nickels & Best, 1996a; 1996b). The idea of substantive strategies is to engage other intact subsystems (e.g., right hemisphere systems) to compensate for the deficits in language processing in the left hemisphere. For instance, compensatory treatments for alternate means of communication (e.g., nonverbal) are used to assist impaired naming. A substantive treatment is the use of gestures to replace impaired verbal communication abilities (Kiran & Bassetto, 2008). A review by Rose (2006) examined 18 treatment studies that used gestures as a compensatory mechanism. The evidence supported the claim that patients with moderate to severe aphasia could benefit from learning new gestures to improve their communication abilities. As with many substantive treatment options, generalization to more natural settings is inconclusive.
In general, restitutive treatments for improving semantic processing have included tasks such as auditory-word to picture matching, written-word to picture matching, answering yes/no questions, picture and spoken word categorization, and judging relatedness to a target word given a set picture (Howard et al., 1985a, 1985b; Marshall et al., 1990; Nickels & Best, 1996a). The goal of these tasks is to strengthen the semantic activation of specific targets to facilitate word retrieval of the specific targets. These tasks are conceptualized as semantic in nature; however, phonological representation of the target words is also provided in many of these tasks. These gains could be due to a combination of semantic and phonological cues presented in treatment. This is consistent with the theoretical models of lexical access that imply that a semantic/phonologic treatment will strengthen semantic and phonologic representations at the semantic and phonological levels (Kiran & Bassetto, 2008).
Phonological Approaches to Treating Anomia
Phonological approaches aim to strengthen either representations at the lexical level of the word form (Maher & Raymer, 2004) or the connections between the semantic system and the word form. Naming impairment due to deficits in post-semantic and phonological processing may be the result of impaired access to the phonological output lexicon or in the lexical representations
Therapy tasks that improve naming in people with aphasia include cueing hierarchies and repetition (Raymer et al., 1993); reading aloud (Eales & Pring, 1998; Howard, 1994; Nickels & Best, 1996b), syllable judgments; initial phoneme discrimination; and rhyme judgment (Franklin et al., 2002). Repetition is the most common phonological task used in the majority of treatments (Nickels, 2002; Nickels & Best, 1996a). A subset of phonological approaches has used orthographic cues, such as providing the first letter of the target word (Greenwood et al., 2010: Hicken et al., 2002; Leonard et al., 2008; Lorenz & Nickels, 2007). Traditionally, semantic and phonological tasks had different effects on word retrieval (Nickels & Best, 1996a; 1996b). Early research reported that phonological tasks improved naming for a very short time, (10‐15 minutes) whereas semantic tasks improved naming for about 24 hours (Howard et al., 1985a). Other studies have shown that phonological cues can produce durable effects. Best and Nickels (2000) argued that there are many unanswered questions about the efficacy of many different therapies, including why it is still difficult to predict which therapeutic task will be successful at remediating particular disorders. They discussed reasons for these differences, arguing that weak specificity of theoretical models, complexity of therapeutic tasks, and a lack of comprehensive assessments of linguistic deficits all contribute to the problem.
Reviews of Studies on Anomia Treatments
Howard (2000) suggested that the difference between semantic and phonological tasks might be overstated. As Howard (1994) and Nickels (2002) indicated, most treatments comprise tasks with semantic, phonological, and sometimes orthographic elements, despite the fact that most clinicians characterize treatments as either semantic or phonological. For example, most studies using semantic tasks require the word form, either spoken or written, meaning that they also seem to require phonological processing. In phonological tasks, a picture of the object is usually present, suggesting that these methods also involve semantic processing. This is a common case for semantic feature analysis (SFA; Boyle & Coelho, 1995; Coelho et al., 2000). Boyle’s (2010) report was the first to examine the efficacy of SFA, and this review addressed seven studies in which SFA was used for confrontation naming of nouns. Across this review, of 17 participants with aphasia, 16 improved their ability to name pictured nouns. These participants had a variety of aphasia syndromes, including classic fluent and nonfluent subtypes. The review concluded that SFA treatments improved naming of treated items for most participants, regardless of whether they required participants to generate the feature themselves or to analyze features that were generated by others (Boyle, 2010). Maddy et al. (2014) also conducted a systematic review of SFA but excluded studies that involved verification, rather than generation, of features (Edmunds & Kiran, 2006; Kiran & Roberts, 2010). This review addressed 11 studies, and, of 24 participants with aphasia, 17 had nonfluent aphasia while seven had fluent aphasia. Generalization to untrained words and contexts was typically limited to words that were semantically related to those in the intervention. This review concluded that SFA is an effective intervention for improving confrontational naming of items trained in therapy; however, in most studies, there was limited generalization from this intervention to untrained items to facilitate connected speech (Edmunds & Babb, 2011; Kiran & Thompson, 2003; Wisenburn & Mahoney, 2009).
A review of anomia therapy by Nickels and Best (1996a, 1996b) covered 19 group and single-case designs throughout the 1980s and 1990s. These authors analyzed the treatment approach (semantic or phonological) in comparison with participant characteristics and found that both semantic and phonological therapies were efficacious. While semantic therapy appeared to show more generalization to untreated items, the relationship of participant characteristics to optimal therapy types and the patterns of generalization remained unclear.
Certain tasks provide a greater focus on either semantics or phonology for different participants (Nickels, 2002). Two well-known cued naming treatments for persons with aphasia are SFA (Boyle & Coelho, 1995) and Phonological Components Analysis (PCA; Leonard et al., 2008; Rochon et al., 2005). Neumann (2018), in a single-participant series design, replicated multiple repeated baselines for naming across four participants. The participants were provided with a counterbalanced order of SFA and Neumann (2018) found differential effects across participants, due to severity of anomia, order of treatment presentation, and participant capacity limits. These findings highlight the importance of expanding our analysis of a participant’s word-retrieval behaviors to consider what other important factors might inform intervention decisions.
In a systematic review of 21SFA studies of 55 persons with aphasia, Efstratiadou, et al. (2018) compared six types of SFA studies (confrontation naming of nouns, confrontation naming of verbs, connected speech/discourse, group studies, multilingual studies, and studies in which SFA was compared to other approaches). They concluded that SFA leads to positive outcomes, despite widespread variability in the treatment procedures, dosage, duration, and variations to the traditional SFA protocol. There is still a need for efficacy studies of SFA and generalization effects in larger controlled studies.
Phonomotor Treatment for Aphasia
An alternative to commonly delivered aphasia therapies is phonomotor treatment (PMT), which focuses on improving knowledge of individual phonemes and phoneme sequences (i.e., phonological sequence knowledge). Researchers have shown that intensively delivered PMT improves confrontation naming on trained words and generalization and maintenance to naming of untrained words relating to discourse production and indicators of quality of life (Kendall et al., 2008, 2015). More specifically, in 2015, Kendall and her colleagues examined whether intensive, neutrally distributed phonologic therapy can generalize to untrained phonologic sequences. Regularities in phonologic sequence knowledge should generalize from the production of words trained to words untrained. The results of this trial demonstrate a generalization of training effects in laboratory measures to sustained improvements at three months, and these findings also provided support for theories motivating phonomotor treatment (Kendall et al., 2015).
PMT has been shown to alter the linguistic network, as evidenced by a decrease in omission errors, both immediately posttreatment and three months later (Minkina et al., 2015); and PMT has improved oral reading of real words and nonwords following treatment (Brookshire et al., 2014). Kendall et al. (2019) tested the efficacy of PMT against SFA for generalization across word classes (i.e., from nouns to verbs) and found, consistent with other PMT research, that there was no between-group difference in generalization to untrained words that did not share semantic or phonological sequence features. However, the within-treatment group results in the maintenance phase add to evidence from prior studies that PMT is more apt than SFA to facilitate generalization after training. Although generalization to untrained stimuli was minimally maintained after SFA treatment, there was further improvement to untrained exemplars over time following PMT (Kendall et al., 2019). Another study examined changes in picture naming errors after 28 individuals with aphasia received 60 hours of phonomotor treatment (Minkina et al., 2019). Confrontation naming was assessed at pretreatment, immediately posttreatment, and three months posttreatment for trained and untrained nouns. The treatment group improved whole-word accuracy on trained items and maintained their improvement. In addition to improved whole-word naming accuracy, results of the error analysis suggested that a global (i.e., both lexical-semantic and phonological) change in lexical knowledge underlined changes in confrontation naming accuracy following phonomotor treatment.
In summary, semantic therapy for anomia is well established both in research and in clinical practice (see also Efstratiadou et al., 2018; Howard et al., 1985a; Marshall et al., 1990). Research on phonological therapy is more limited, and the results are more equivocal (Kendall et al., 2019; see also Howard et al., 1985a; Raymer et al., 1993). However, a therapy study using a choice of phonological or orthographic cues reported significant improvements in word finding for seven out of eight participants with aphasia (Hicken et al., 2002).
Orthographic Cues in Word Finding
There is relatively little research on the use of written cues for word finding. An exception is the work of Bruce and Howard (1988), who found that none of a group of 20 people showed improved naming with a letter board (of nine letters) present. This result led to the conclusion that orthographic cues may not be useful in facilitating word finding. More recent work suggests that this conclusion may not apply to all individuals with aphasia. Howard and Harding (1998) worked with an individual whose naming improved dramatically in the presence of the written alphabet.
In the present study, we included orthographic cues on the premise that the study’s results might have both clinical and theoretical implications. According to Lorenz and Nickels (2007), both orthographic and phonological information from a target word can provide information cues in treating anomia. As noted earlier, both are often used in clinical practice even though the effectiveness of orthographic cues are often debated (e.g., Basso et al., 2001; Best et al., 2002; Howard & Harding, 1998). Originally, form-specific word cues, such as the initial sound or rhyme, produced effects on spoken naming, and others observed that the cue effects were short-lived (Howard et al., 1985b; Patterson et al., 1983). In general, there continued to be controversy regarding the most appropriate treatment task (Nickels, 2002). Accordingly, in this study we addressed the sublexical transcoding ability and effectiveness of an orthographic cue. Others have assumed that the effectiveness of orthographic cues related to sublexical processing abilities for written materials (e.g., Best et al., 2002; Nickels, 1992). The idea is that orthographic cues are effective because the written cue activates the sublexical reading route that, in turn, loops back to the phonological representation of a word. Other authors have found significant benefit from orthographic cues in patients with aphasia without sublexical transcoding abilities for written materials (e.g., Howard & Harding, 1998; Lorenz & Nickels, 2007) which suggests that there are additional mechanisms explaining the efficacy of orthographic cueing. Bruce & Howard (1988) argued that in order for letter cues to be effective cues, phonological cues must also be intact. Letter cues continue to receive little attention in clinical research and practice, while phonemic cues are predominant. Yet, according to three case studies analyzed by Lorenz and Nickels (2007), clinicians should look to letter cues as tools for facilitating word production, even in patients with varied sublexical transcoding abilities who do not benefit from phonemic cues.
Purpose of the Present Study
Across 18 different single word choice trials from with three-word options (e.g., daughter, laughter, son) in which two words were semantically related (e.g., daughter, son) and two were orthographically related (daughter, laughter), we asked 10 neurotypical adults and 11 adults with aphasia (5 fluent; 6 nonfluent) to select the most different word. Our study hypotheses were that neurotypical adults would choose the word that was not semantically related (e.g., laughter) as the most different; and that adults with aphasia would choose the word that was not orthographically related (e.g., son).
Method
Participants
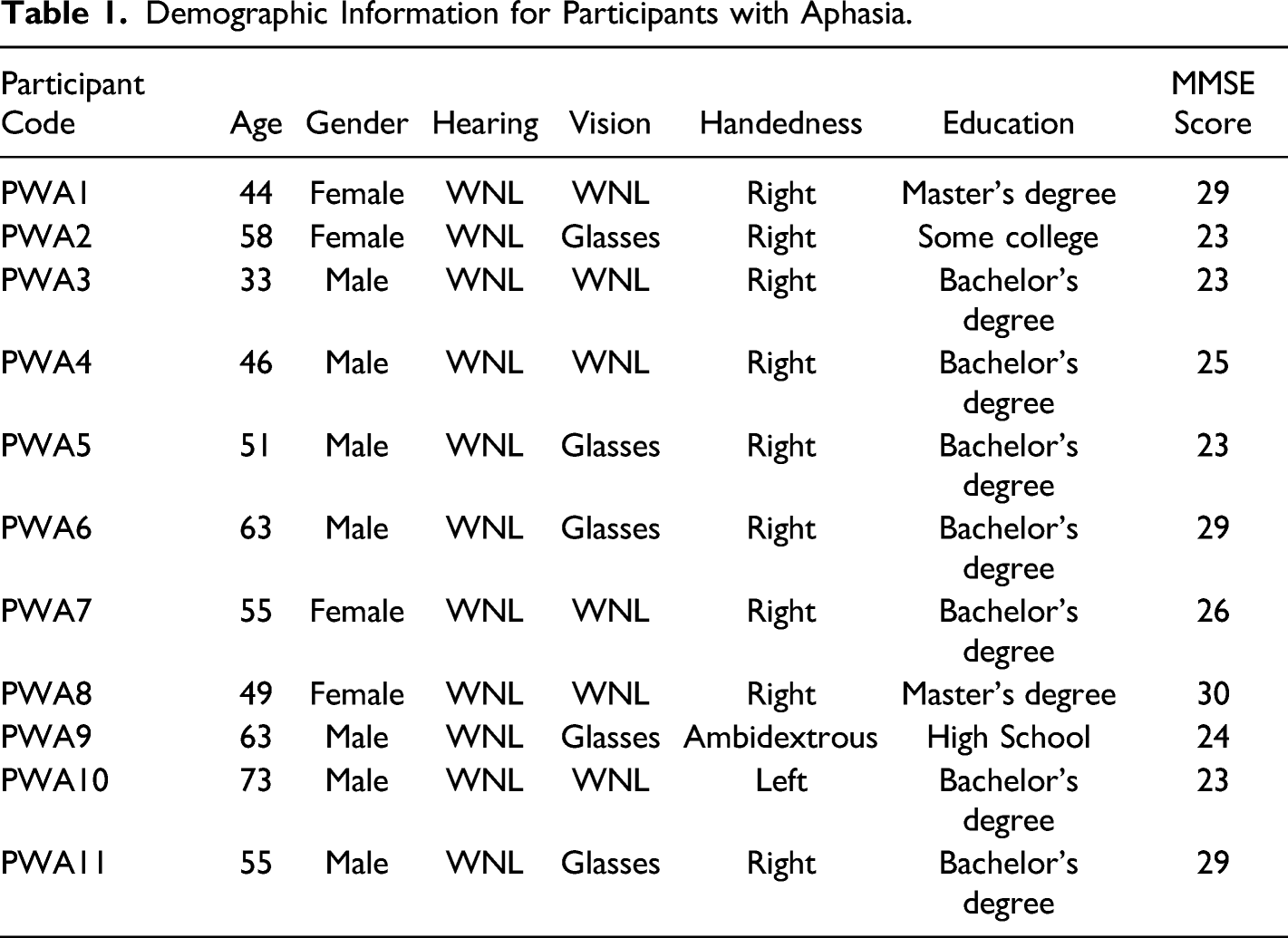
Demographic Information for Participants with Aphasia.
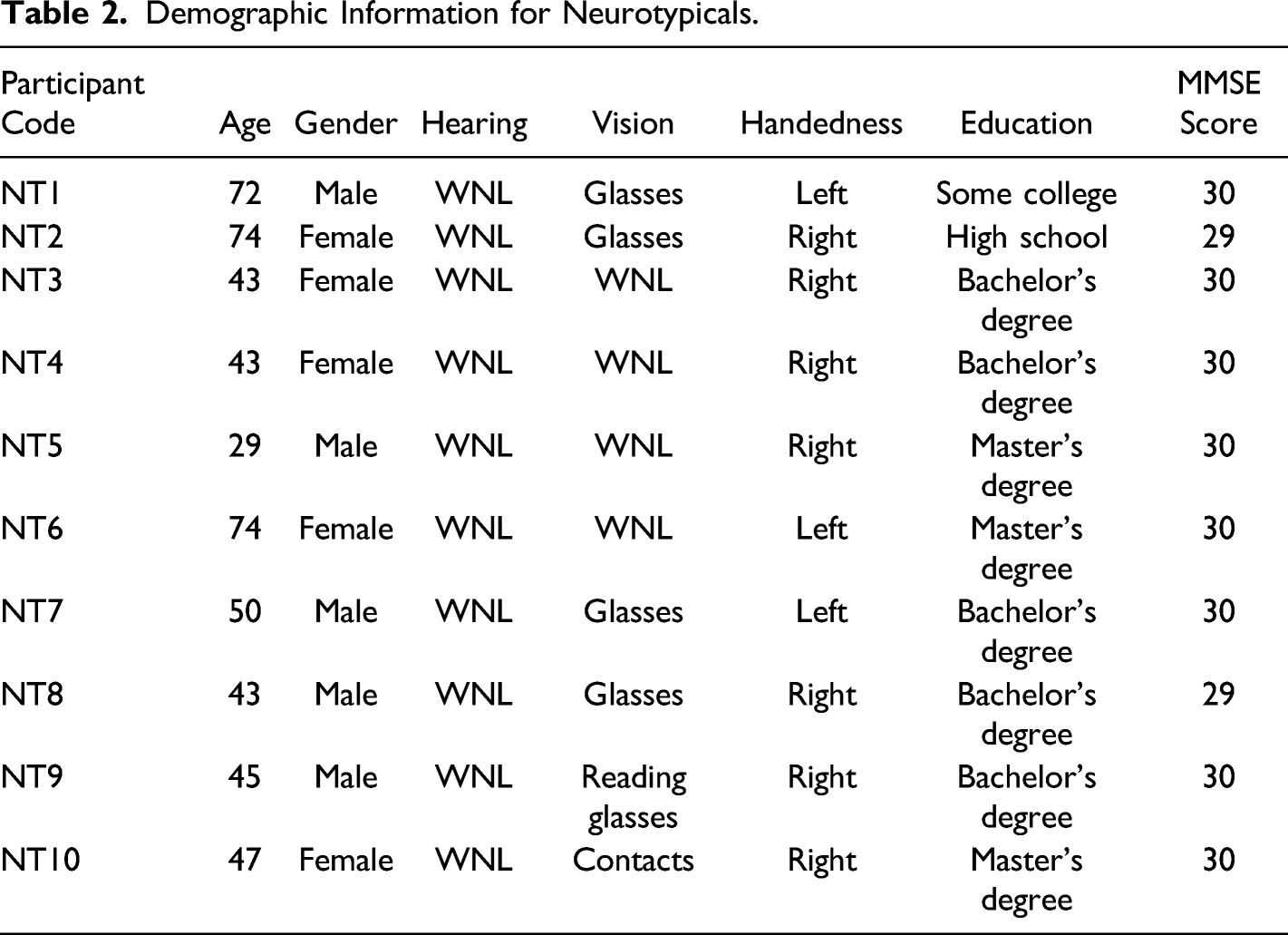
Demographic Information for Neurotypicals.
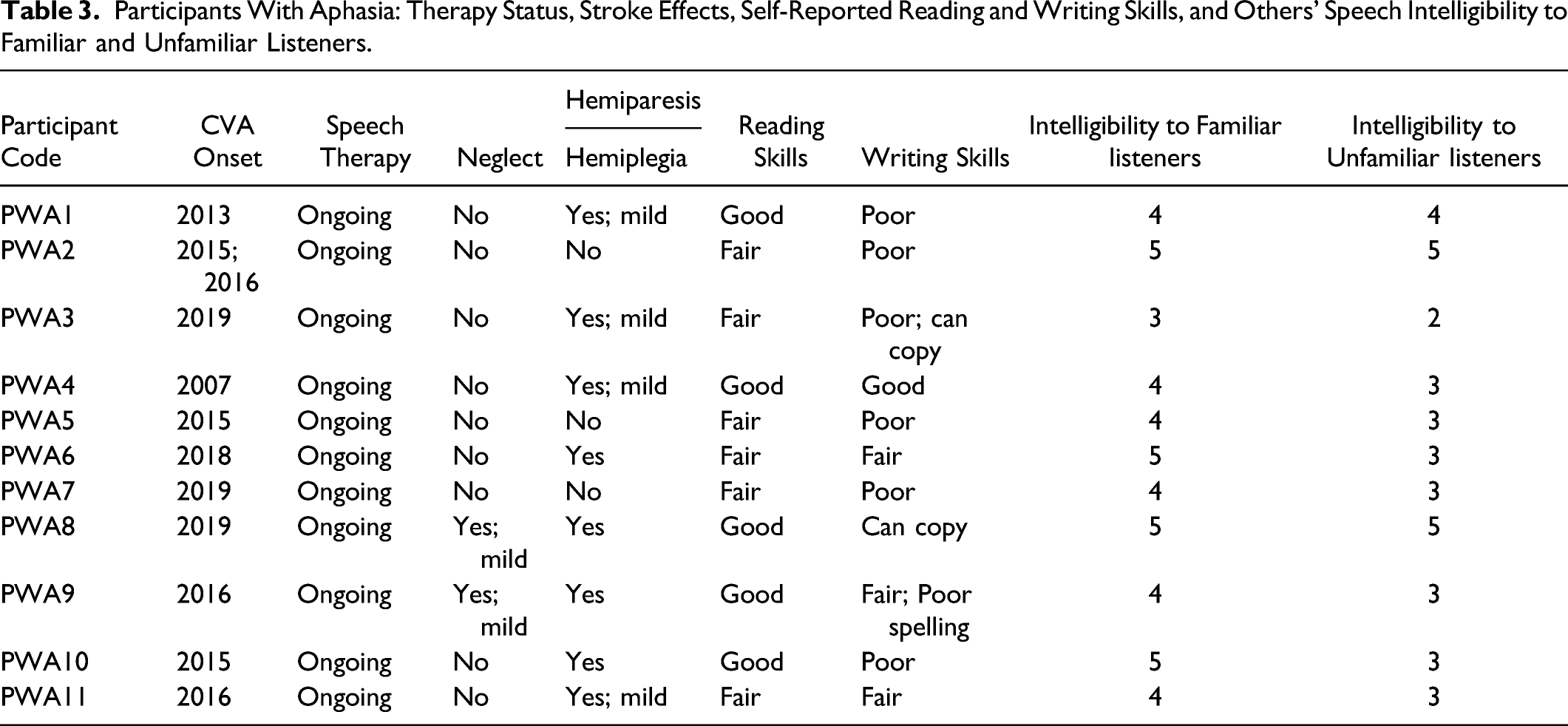
Participants With Aphasia: Therapy Status, Stroke Effects, Self-Reported Reading and Writing Skills, and Others’ Speech Intelligibility to Familiar and Unfamiliar Listeners.
Protocol and Stimuli
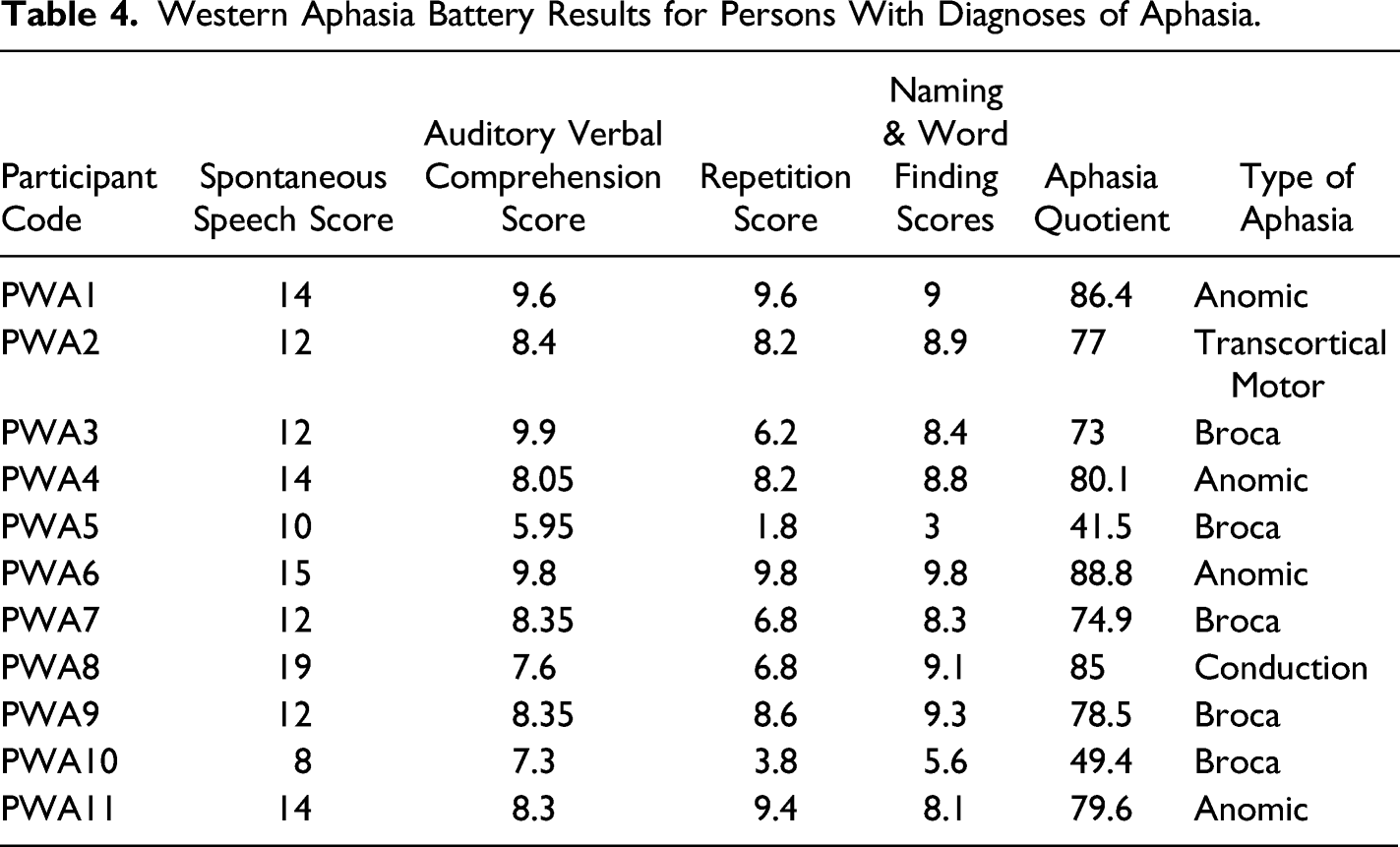
The participants reviewed and signed an informed consent from Adelphi University’s Intuitional Review Board that approved the study. To determine that individuals with aphasia understood the concept of “different,” we repeated the first part of a protocol (Goldfarb & Balant-Campbell, 1984) used for cognitive discrimination in adults with acquired brain damage. Our participants were asked to choose which was different among, for example, two blue squares and one red square (color difference) and two blue squares and one blue circle (form difference). They were then asked, “Which one is the most different?” when presented, for example, with one red square, one blue square, and one red circle (color vs. form preference). Neurotypical participants were given the same three tasks before beginning the present lexical discrimination task. The neurological and audiological records of the participants revealed no significant history of hearing loss. All pure tone thresholds were 30 dB or better for octave frequencies 250 to 8 k Hz indicating that participants did not have significant hearing loss. A visual screening was performed, since the testing was performed on the Zoom HIPAA platform. Each participant was given the Mini-Mental State Examination (Folstein et al., 1975) to ensure that our neurotypical group had adequate cognitive skills. The participants with aphasia (PWA) were administered the Western Aphasia Battery (WAB) (Kertesz, 2007) to determine type of aphasia and severity.
Research Design
The lexical discrimination task required the participant to choose the word that was most different among a foil, an orthographically related word, and a semantically related word (e.g., leopard, leotard, lion). There were 18 sets that included the three options. Assuming that “leopard” was understood to be the foil, the hypothesis was that neurotypical adults would select the orthographically related word (“leotard”) as most different, because of the saliency of the semantic pair. Individuals with aphasia would choose the semantically related word (“lion”) as most different, because of their word-finding deficit and the letter similarities in the orthographic pairs. The list of word stimuli was pseudorandomly ordered to avoid presentation of three consecutive variables (e.g., the foil in the first position). Response times were not calculated. The participants had unlimited time to complete the task. See Appendix 1 for a list of stimuli.
Results
Western Aphasia Battery Results for Persons With Diagnoses of Aphasia.
Means (and Standard Deviations) of Aphasia and Neurotypical Groups.

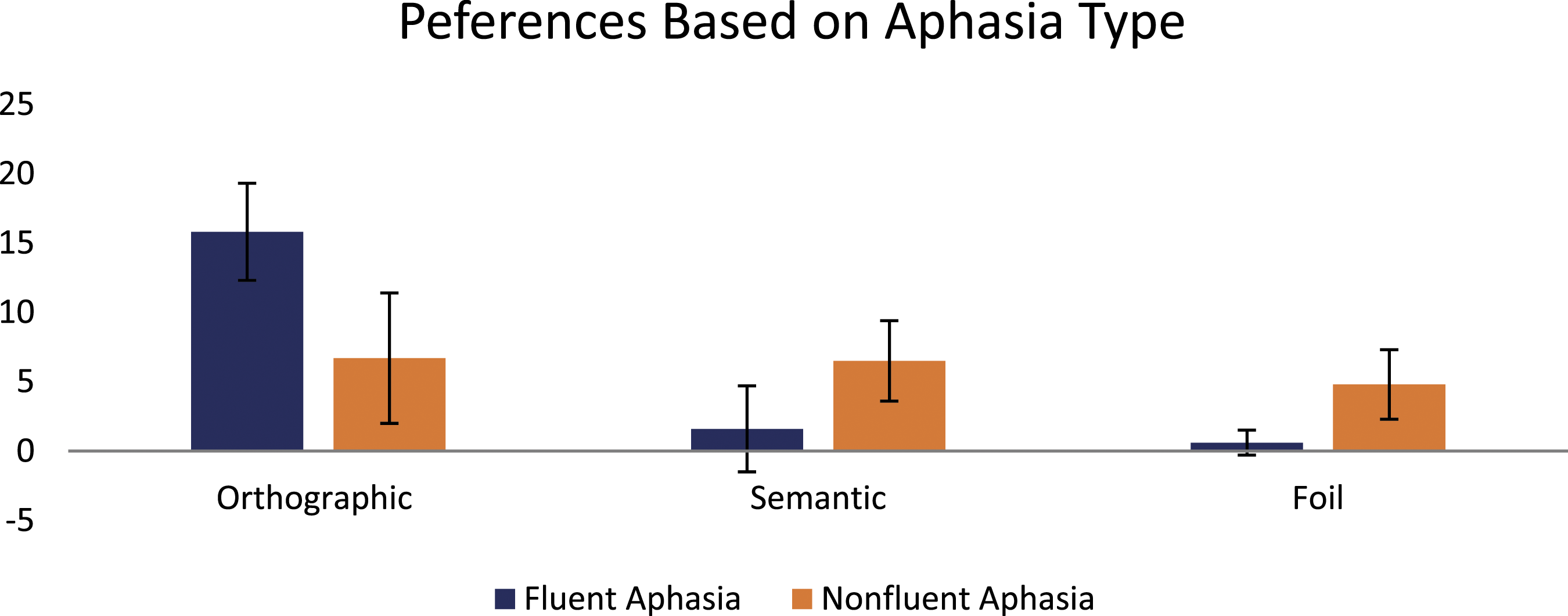
Means (and Standard Deviations) of Fluent and Nonfluent Aphasia Participants.

The choice of three words consisted of a foil (e.g., “scent”), a word that was orthographically similar but semantically different (e.g., “scene”) and a word that was semantically similar but orthographically different (e.g., “odor”). For the “Most Different” choices, a “semantic” response meant that the participant rejected the semantic similarity choice (e.g., scent—“odor”) as being the most different among the three words, as was the overwhelming case for neurotypical adults (NT) who chose the orthographically similar but semantically different word (“scene”) as most different. An “orthographic” response meant that the participant rejected the orthographic similarity (e.g., scent— “scene”) as being the most different among the three words, as was the case for the majority of adults with aphasia (PWA) who tended to choose the word that was semantically similar but orthographically different (“odor”) as the most different. Also, a few individuals with aphasia rarely chose the foil (“scent”) word as most different (Figure 1 and Figure 2). Significant Results Between Aphasia and Neurotypical Groups for each Condition. Non-significant differences between fluent and nonfluent aphasia participants.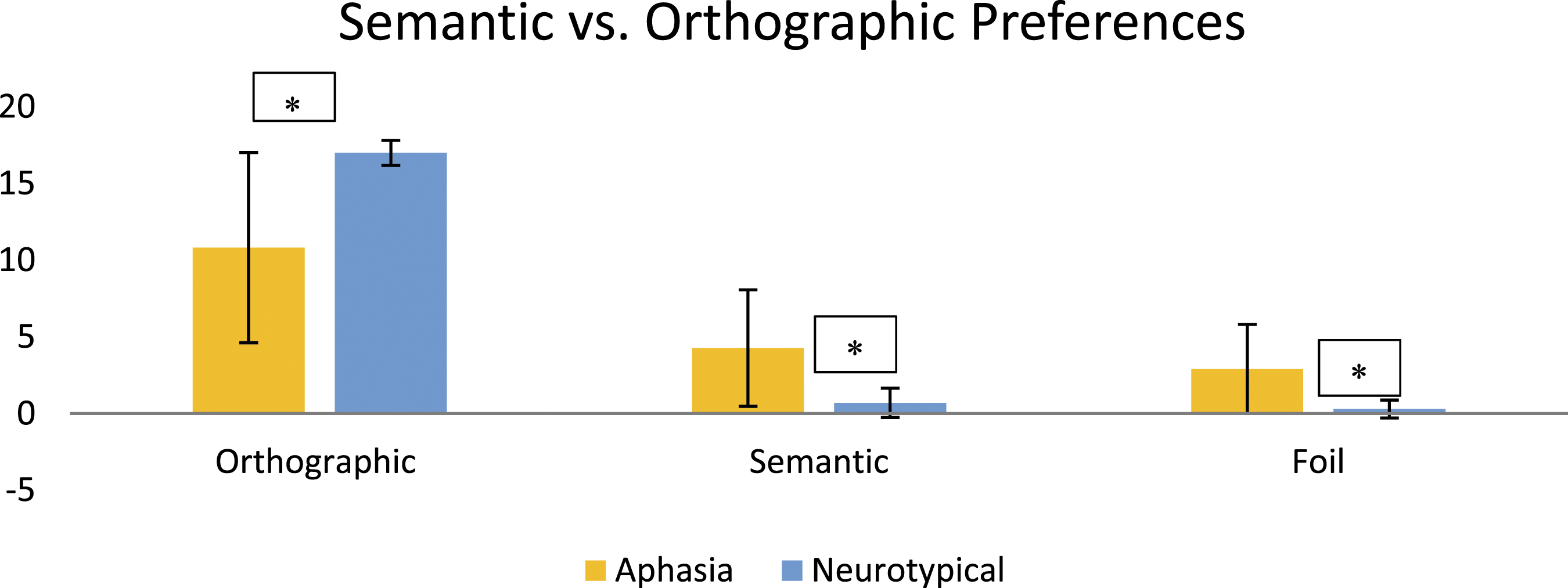
Discussion
Both our experimental hypotheses were supported in the present investigation. Individuals with aphasia selected the word that was not orthographically related (e.g., son in the daughter-laughter-son trial) as the most different, while neurotypical adults selected the word that was not semantically related (e.g., laughter in the daughter-laughter-son trial) as the most different. These findings strengthened the hypotheses that adults with aphasia focused on orthographic word differences, while adults without language disorders were drawn to semantic word differences. In addition, we further analyzed the separate results of participants with aphasia who showed fluent aphasia (i.e., 4 anomic, 1 conduction) and nonfluent aphasia (i.e., 5 Broca, 1 TMA). While we did not find significant group differences (likely due to insufficient sample size and associated statistical power), we noticed that the participants with fluent aphasia seemed to prefer the semantic connection (e.g., they selected the orthographically similar word “laughter” as most different from “daughter” and “son”), while participants with nonfluent aphasia seemed to prefer the orthographic connection (e.g., they selected the semantically similar word “son” as most different from “daughter” and “laughter”). This more speculative trend should be further explored in future research. The likelihood of word-finding (semantic) deficits in aphasia may account in part for these results. As found in Nickels (2002), due to the nature of aphasia and anomia therapy, we are uncertain what types of cues work for specific types of aphasia. While this study did not specify the type of aphasia, we did explore orthographic cues as a facilitation technique for word-finding strategies. As clinicians, we know it is a challenge to tease out semantic, phonological, and orthographic representations when using a multi-modal therapy approach of sounds, pictures, and words. As stated in our introduction, the majority of studies using semantic tasks require the word form which would seem to require phonological processing. In phonological tasks, the picture is usually present, suggesting the involvement of semantic processing. Individuals with aphasia may also have been drawn to the obvious visual differences of words with very different orthographic representations.
Few studies have examined orthographic approaches to aphasia therapy, with the exception of self-cueing strategies that use letter-to-sound correspondences (Nickels, 2002). An underlying assumption of a self-cueing strategy is that the client’s knowledge of the written form is relatively intact (Herbert et al., 2001). Despite limited prior support for orthographic training in aphasia therapy, the results of the present study support including some aspects of reading comprehension such as identifying semantically associated words (e.g., synonyms and antonyms) that have different orthographic representations in the early stages of therapy.
Limitations and Future Clinical Implications
This study employed a small sample and did not formally test these participant’s reading skills. While a self-report is informative, a more objective screening or standardized measure would be more helpful. For example, a lesion in Wernicke’s area of the brain may extend into the angular gyrus of the parietal lobe, resulting in varying forms of dyslexia and dysgraphia. In a previous study, we did not find differences in resolving grammatical category ambiguity based on age of the neurotypical participant (Goldfarb & Bekker, 2009), but the same conclusion may not apply in semantic and orthographic tasks.
Also, we did not examine response time in this study, nor did we further probe the participants’ word choice decisions. Future studies might categorize participants by type of aphasia and assess which categories of cues (semantic, orthographic, and phonological) are most beneficial for each person with aphasia in a priming task for word-finding. This could lead to treatment protocols that can improve lexical access in people with aphasia. Future studies can also use semantic and orthographic representations visually, perhaps using other advanced instrumentation such as eye-tracking with specific diagnosis of types of aphasia based on sensitive testing measurements.
Conclusion
Comparing patients with aphasia to neurotypical adults, we showed that participants in these groups responded differently to information about the orthographic form versus semantic characteristics of words. This finding has important implications for the benefits of using orthographic word form to cue word recall in individuals with aphasia, and we outlined some further research that is needed in this area.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.