
Abstract
Performing physical exercise during hemodialysis has been debated regarding safety and efficacy for improving life quality for patients with chronic kidney disease (CKD). Thus, we explored the influence of physical exercise during hemodialysis on both autonomic modulation of heart rate and quality of life for patients with CKF in a randomized clinical trial. We randomly allocated participants requiring hemodialysis to an experimental exercise group (EG) and a control no-exercise group (CG) and assessed their quality of life with the Kidney Disease Quality of Life Short Form—KDQOL-SF™ 1.3 and with Polar RS800CX to monitor their heart rate variability (HRV) before and three months after the end of the exercise intervention. EG participants reported a significant increase in their quality of life (p = .05, physical function, physical aspects, pain, emotional well-being, emotional function; p = .03, energy and fatigue) and showed HRV improvement (p = .05, RMSSD, SDNN, and SD2; p = .004, SD1) after three months of exercise. Thus, we recommend supervised physical exercise during hemodialysis for carefully selected patients.
Introduction
Chronic kidney disease (CKD) affects 5–7% of the world population, with an estimated annual increase in hemodialysis treatment over the last two decades of 6–12% in developed countries and even more in developing countries (Amdur et al., 2016; Woo et al., 2012). CKD can be characterized as the most advanced stage of kidney disease in which there is a progressive and irreversible loss of kidney function, with a series of associated clinical, bio-chemical, and metabolic disorders (Kraus et al., 2016; National Kidney Foundation, 2015).
CKD symptoms and symptoms associated with undergoing hemodialysis are very similar, since both present a catabolic state that causes loss of energy and protein, presenting clinically as weakness, fatigue, a low level of physical activity, low physical function, extremity edema, weight loss, nausea, vomiting, sleep disturbance, cognitive impairment, pulmonary edema, and dyspnea. This condition leads to a higher incidence of falls, hospitalizations, loss of independence, low quality of life, and an increased mortality rate (Brown et al., 2017; Martin-Alemañy et al., 2016; Rivara et al., 2017). Quality of life (QOL) is a subjective manifestation of a set of beliefs and personal experiences and expectations. QOL is strongly related to chronic diseases, due to both a series of life changes and limitations, and the presence of invasive and painful treatments that affect physical, psychological, social, and economic well-being (Ahlawat et al., 2018).
Cardiovascular dysfunction is common in patients with CKD, due to the increase in myocardial calcium that results from parathyroid hyperactivity, especially after starting hemodialysis (Rostand et al., 1988). It is also important to emphasize that cardiac dysfunction stems from altered neuro-humoral activity that also influences long-term survival (Marenzi et al., 2001). A common condition in this population is decreased autonomic modulation of heart rate, predisposing people to a greater risk of cardiac events such as arrhythmias, coronary artery disease, cardiomyopathies, and heart valve diseases that directly affect QOL (Senanayake et al., 2017). A deteriorating physical condition in patients with CKD is evident; and while it can be improved by starting hemodialysis, there is still a worsening physical capacity (McCullough et al., 2016).
In this context, physical exercise has emerged as a potential tool to prevent further decline and help rehabilitate these individuals through better blood pressure control, oxygen consumption (Mohseni et al., 2013), and kidney function. Exercise generally increases aerobic capacity and QOL (McCullough et al., 2016), but its use with patients with CKD has been questioned (Hu et al., 2021). In the present study, we hypothesized that aerobic exercise with a cycle ergometer performed during hemodialysis would be well tolerated and beneficial. Thus, our objective was to determine whether performing aerobic exercise during hemodialysis influenced the autonomic modulation of heart rate and quality of life of older patients with CKD.
Method
Study Design
This was a randomized, double-blind trial, conducted according to the CONSORT guidelines for randomized clinical trials (Costa et al., 2011). This study was approved by our research ethics committee under number 2.260.224 and it was registered in clinical trials under number NCT03556540. All participants freely signed the informed consent form. We conducted the study between February 2018 and February 2020.
Participants and Randomization
This study included individuals between 50–70 years old who had undergone hemodialysis for at least six months. Participants had an upper limb fistula for hemodialysis that they underwent three times a week at a hemodialysis center. We excluded individuals who had been previously hospitalized for CKD or who were hospitalized during the application of the protocol. We also excluded (a) patients with musculoskeletal diseases that prevented the performance of the proposed exercise; (b) individuals who used drugs that influenced their heart rate; (c) individuals who had values below 24 points on the Mini Mental State Examination (MMSE; Bossola et al., 2011; Folstein et al., 2001); (e) individuals with pacemakers installed, or who had undergone previous cardiac surgery within less than six months; and (f) those with a body mass index greater than 30 kg/m2.
Volunteers who met these selection criteria were randomly assigned into two groups by a researcher who did not know the study’s details: an experimental group (EG), who received the physical training protocol with a cycle ergometer; and a control group (CG), who continued to receive the usual care from the multidisciplinary treatment team but who did not exercise during hemodialysis. Randomization was by computer generation and was overseen by a second researcher who was not involved in selecting study participants. The allocation of patients into these groups was carried out on the website https://randomization.com.
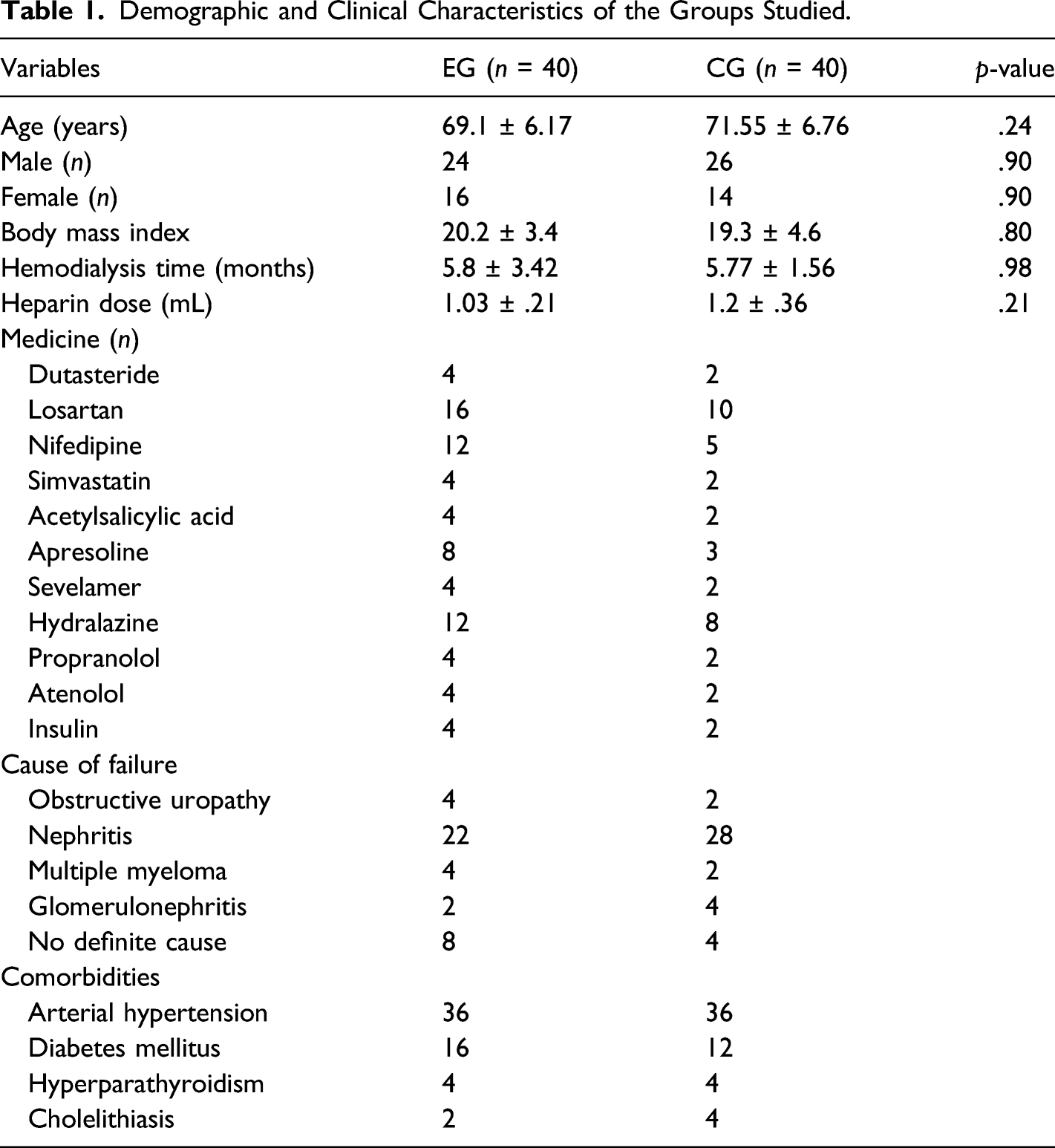
A power analysis to estimate a required sample size was performed using the GraphPad StatMate application, version 1.01, with statistical significance set at 5% and statistical power set at 99%, using, as a reference, the number of cases found in published reports in the literature. This analysis led to a determination that we needed to include 20 volunteers with CKD who underwent hemodialysis treatment in each of our groups. From an initial participant sample of 195 individuals, 97 failed to meet inclusion criteria or did not consent to participate, another 18 were excluded throughout the study for various reasons after randomization (see Figure 1); and, by the end of the study, 40 volunteers in each group completed the study. Table 1 shows the main socio-demographic and clinical characteristics of the participants in this study. Flowchart of Volunteer Participation in the Study. Demographic and Clinical Characteristics of the Groups Studied.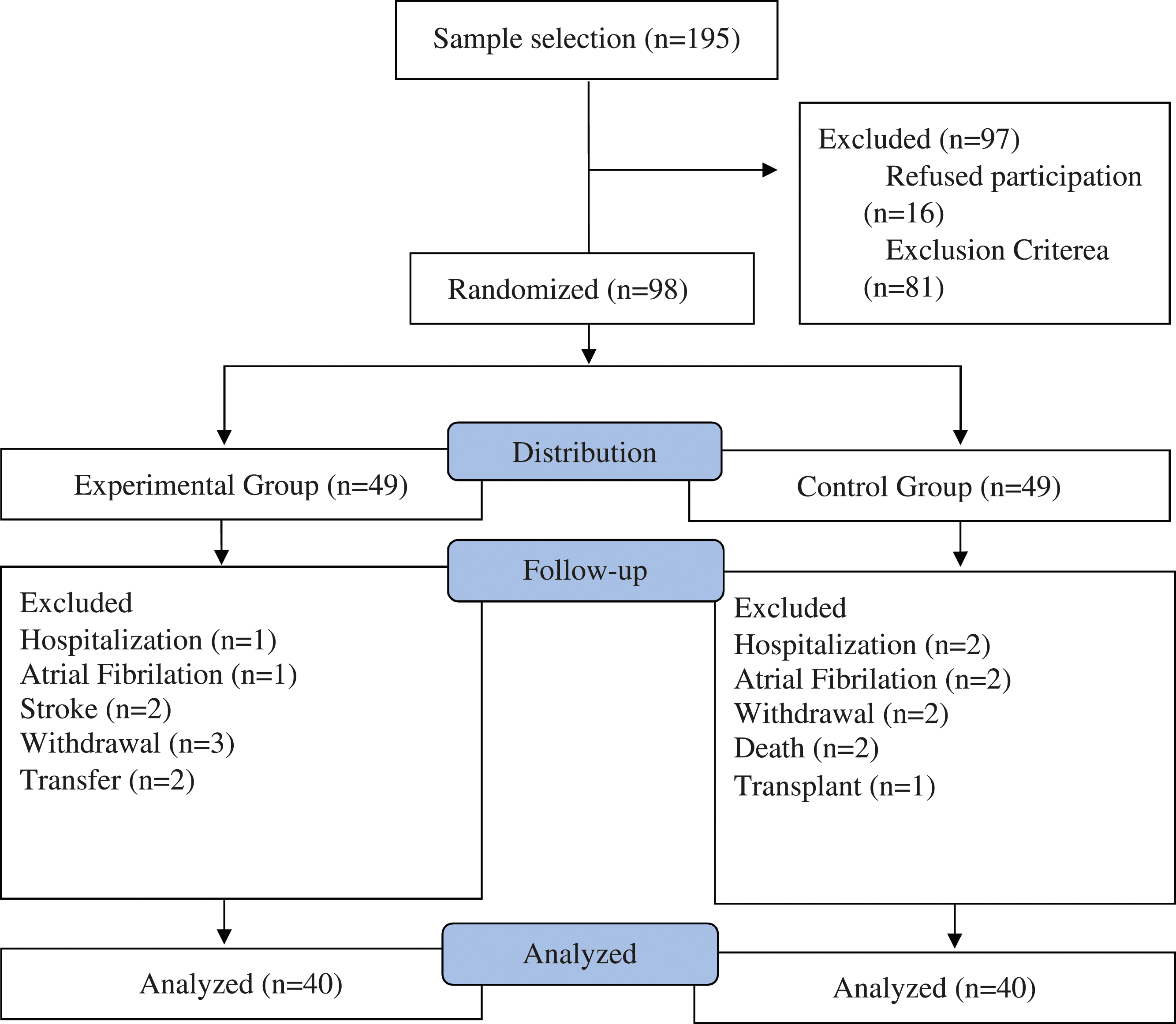
Data Collection Procedure
The research protocol was divided into three phases: (a) an initial assessment of QOL and heart rate variability (HRV), (b) the physical exercise training protocol, and (c) reassessment. QOL assessment was with the Kidney Disease Quality of Life Short Form (KDQOL-SFTM 1.3; McCullough et al., 2016; Senanayake et al., 2017). This questionnaire, related to physical, social, emotional, cognitive, and satisfaction aspects of QOL, was read to participants; and participants were then given time to use answer options for their responses.
To evaluate HR variability, we used the POLAR® cardiofrequencimeter RS800CX model (Polar Electro TM. Kempele. Finland). We evaluated participants’ autonomic modulation of heart rate before and after the end of the intervention. Patients were awake and in a supine position for 10 minutes for this evaluation. We collected the 256 data points with the highest signal stability and analyzed the linear variables in the time domain (RMSSD and SDNN) and the non-linear variables (SD1 and SD2). To analyze heart rate variability, we transferred the cardiofrequencimeter data to a researcher who did not know the experimental group to which the participants belonged. The data recorded were then transferred to the Polar ProTrainer Software (Polar Electro OY, Kempele, Finland) through an infrared signal emission interface where it was stored and from which it was later exported into TXT format so that it could be analyzed in the Kubios HRV 2.2 program (MATLAB, Kuopio, Finland) and saved on the computer with the collection time.
Intervention
The exercise training protocol consisted of 30 minutes of aerobic physical activity using a cycle ergometer (Physycal, Londrina, Brazil). The exercise was applied in the first two hours of hemodialysis, three times a week for three months. The participants’ vital signs were monitored every 10 minutes with polar. The sessions were divided into warm-up, conditioning, and cool-down periods. In the warm-up phase, participants performed five minutes of exercise at between 60–70% of their maximum heart rate, with their self-reported perceived rate of exertion (PRE) between 1 and 2 on the modified Borg scale (Silva et al., 2013). During the conditioning phase, participants engaged in 20 minutes of moderate exercise, with HRV between 70–80% of maximum heart rate and self-reported PRE between 3 and 4. The cool-down phase lasted five minutes and was characterized by HRV between 60–70% of maximum and self-reported PRE between 1 and 2. The maintenance of the parameters was regulated by the speed of the exercise and increased by 5% speed every month. Training intensity adjustments were based on each patient’s Borg scale and HRV to keep within the target training zone. A percentage of the maximum heart rate was calculated from data during the 6-minute walk test. Exercise was interrupted if the participant had systolic blood pressure above 180 mmHg, diastolic blood pressure above 95 mmHg, 20% change in heart rate, saturation below 88%, physical exhaustion, chest pain, dyspnea, dizziness, and/or fatigue of the exercised limbs. Participants in the control group performed no supervised physical exercise intervention and only received information regarding the importance of performing physical exercise when diagnosed with chronic renal failure and undergoing hemodialysis.
Data Analysis
We performed statistical analysis using the Bioestat 5.3® program, in which we used the Shapiro-Wilk test and multivariate analysis of variance (MANOVA) with multiple post-hoc comparisons conducted with the Tukey test. We set statistical significance at p <.05. The analysis of data referring to QOL were computed by the KDQOL-SF Working Group® program. The results were expressed as means and standard deviations, minimum and maximum values, with a 95% confidence interval.
In addition to these statistical tests, we made intergroup comparisons to measure effect sizes of group differences with the Effect Size Generator application, version 2.3 (Swinburne University of Technology, Center for Neuropsychology, Melbourne, Australia) and interpreted these effect sizes using the Cohen’s d pooled method and Cohen’s (1988) guidelines such that values less than .3 were considered a small effect, values between .4 and .7 as medium, and those above .7 as a large effect.
Results
Among the evaluated groups, the experimental participants’ mean age was 69.1 (SD = 6.17) and the control group participants’ mean age was 71.55 (SD = 6.76). There was a prevalence of males (70% for the EG; 80% for the CG), and there were predominantly people of color (80% for EG; 100% for CG) in this sample; participants had less than high school education (60% elementary school; 40% middle school). As for clinical data, EG participants averaged 5.8 (SD = 3.42) months of hemodialysis, while CG participants averaged 5.77 months (SD = 1.56). Nephritis was the underlying CKD, and arterial hypertension was the main associated comorbidity. Participants in the EG received an average dose of Heparin of 1.03 mg (SD =.21) while those in the CG group received an average heparin dose of 1.2 mg (SD =.36). In addition, many participants received multiple medicines.
Quality of Life
Analysis of Specific Aspects of Kidney Disease.
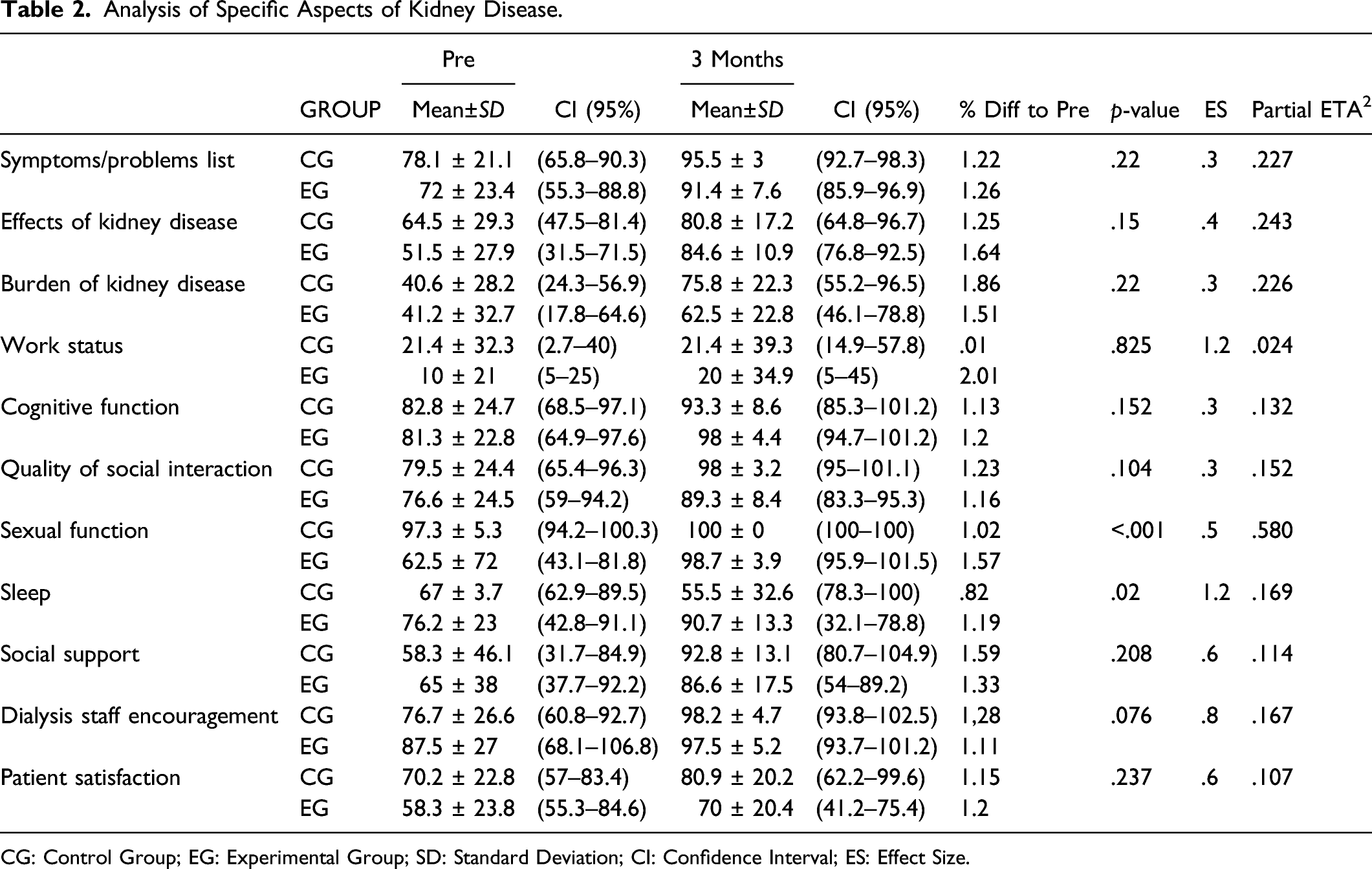
CG: Control Group; EG: Experimental Group; SD: Standard Deviation; CI: Confidence Interval; ES: Effect Size.
Analysis of General Aspects of Quality of Life.
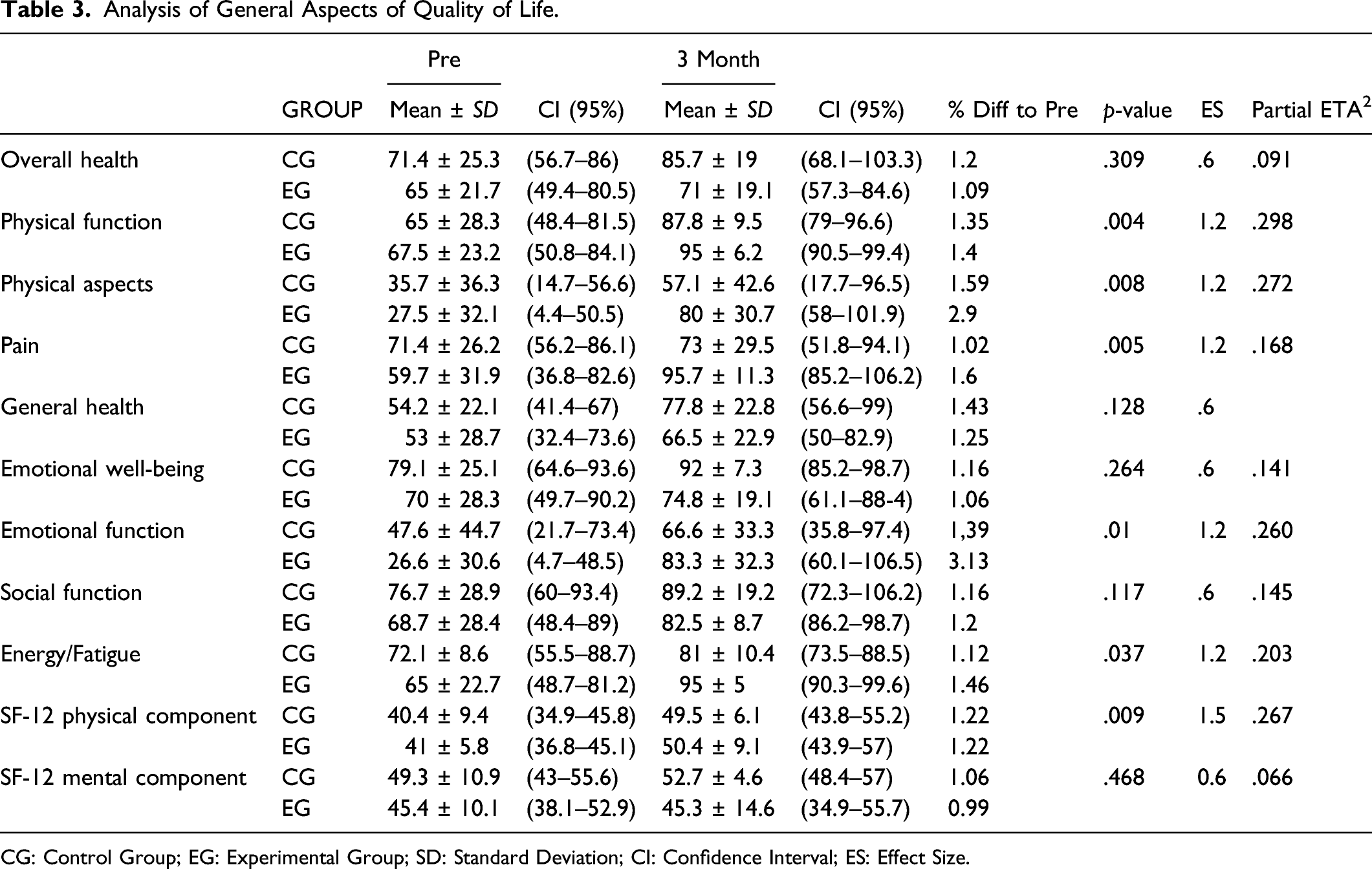
CG: Control Group; EG: Experimental Group; SD: Standard Deviation; CI: Confidence Interval; ES: Effect Size.
Table 3 shows data referring to general aspects of self-reported QOL as assessed by the KDQOL-SFTM 1.3 scale. There was an increase in aspects of QOL related to physical function (p = .05), physical aspects (p = .05), pain (p = .05), emotional function (p = .05), and energy/fatigue (p = .03), among participants in EG, relative to CG; and these changes demonstrated a large effect size benefit to the 3-month exercise protocol performed by the experimental group during hemodialysis.
Autonomic Heart Rate Modulation
Analysis of Heart Rate Variability (HRV).
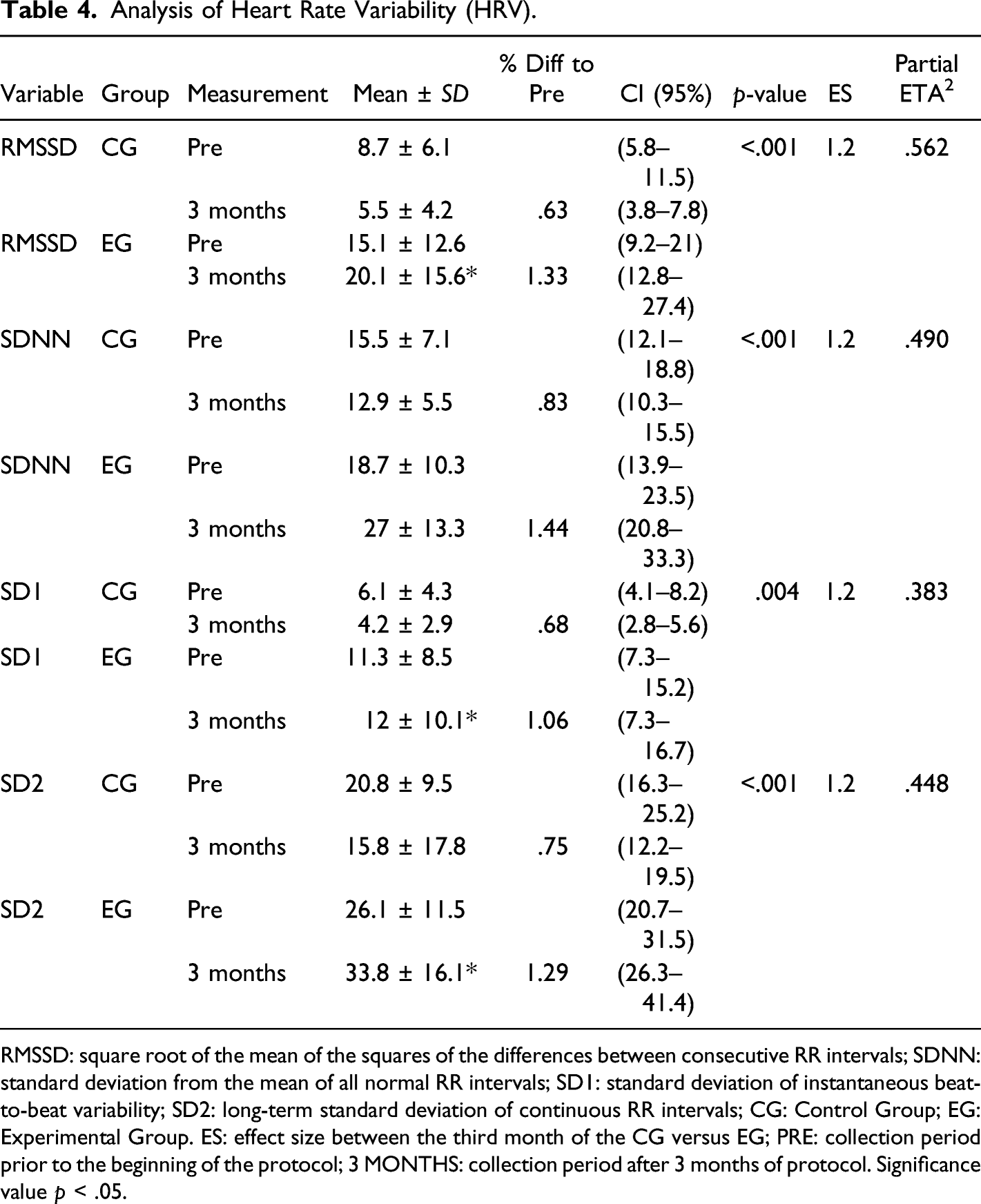
RMSSD: square root of the mean of the squares of the differences between consecutive RR intervals; SDNN: standard deviation from the mean of all normal RR intervals; SD1: standard deviation of instantaneous beat-to-beat variability; SD2: long-term standard deviation of continuous RR intervals; CG: Control Group; EG: Experimental Group. ES: effect size between the third month of the CG versus EG; PRE: collection period prior to the beginning of the protocol; 3 MONTHS: collection period after 3 months of protocol. Significance value p < .05.
Discussion
In this study, we showed that participants with CKD who engaged in physical exercise during hemodialysis improved both their autonomic modulation of heart rate and their QOL, relative to control group participants with CKD who did not engage in exercise. Kidney disease and hemodialysis negatively influence the autonomic modulation of heart rate (Yalım et al., 2020), and this modulation difficulty is related to sudden death and cardiac events in these patients (Ranpuria et al., 2008). Thus, our results signal an important medical benefit to physical exercise during hemodialysis in the form of increased autonomic heart rate modulation with increased vagal tone and sympathovagal modulation. In addition, aerobic exercise promoted gains in self-reported QOL among our volunteers with CKD, leading us to recommend closely monitored physical exercise during hemodialysis for well selected older adults with CKD.
The prevalence of chronic renal failure increases with age, especially for those with associated comorbidities or underlying diseases, including diabetes mellitus, systemic arterial hypertension, or both (Mallappallil et al., 2014). This can be explained by the decrease in the glomerular filtration rate and structural changes in the blood vessel walls with increases in age (Tonelli & Riella, 2014). It is important to emphasize that the real impact of this process on health depends on how the individual deals with their condition. In addition, CKD is one of the most evident examples of disparities in health conditions, as it is most prevalent among individuals from racial minorities and those with a lower level of education (Harawa & Norris, 2015). As both these associated health and socioeconomic conditions were predominant in our participant sample, our findings of protective benefits of exercise during hemodialysis are still more important.
Anticoagulant therapy is of paramount importance in hemodialysis treatment, with heparin administration one of the most common means of controlling it in developed countries, such as the United States. Yet, studies have shown that its use is still indiscriminate and that dosages vary, based on patient weight and bleeding risk. These heparin use patterns were corroborated in the present study, with adjustments made according to clinical signs suggesting that patients experienced varied propensities to develop episodes of osteopenia and thrombocytopenia (Harmon et al., 2013; Shen & Winkelmayer, 2012). In addition, the use of anticoagulants may relate to the incidence of atrial fibrillation and stroke among older adults (Winkelmayer et al., 2012), leading to a worsening QOL and autonomic modulation of heart rate. We also saw, among our participants, a predisposition to polypharmacy with the increasing side effects and drug interaction toxicity risks that are common among patients with CDK (Marquito et al., 2014).
Data within our study demonstrated a low self-reported QOL before the exercise training protocol that has been previously attributed to the hemodialysis routine, with frequent time in hospital environments, water and food limitations, physical inactivity, absence from work, concerns arising from the disease, lack of social support, and other factors (Ahlawat et al., 2018; Brown et al., 2017; Jhamb et al., 2016; Jhee, et al., 2017). Physical activity, from aerobic or resistance exercise, has been shown to improve health-related QOL due to morphological changes in muscle capillary density, improved oxidative metabolism, and reduced systemic inflammation from exercise that culminates in an improvement in physical performance, physical function, and consequently, the patient’s QOL (Afsar et al., 2018; Heiwe & Jacobson, 2014; Lewis et al., 2015). While we did not investigate changes in capillary density, we found both positive results in almost all aspects of self-reported QOL and better autonomic heart rate modulation. These data are in accordance with Wu et al. (2014) whose participants also performed intradialytic aerobic activity and obtained significant improvement in all domains measured in their intergroup analysis: physical function, physical aspects, general health, energy/fatigue, sleep, quality of social interaction, sexual function, list of symptoms/problems, encouragement of the hemodialysis team, and patient satisfaction. Their control group showed improvement only in the encouragement of the hemodialysis team and patient satisfaction. Another study involving QOL and intradialytic aerobic exercise (Paluchamy & Vaidyanathan, 2018) used a protocol of approximately 15 minutes of exercise on an exercise bike in the first two hours of hemodialysis three times a week for 12 weeks and also found improvement in all domains evaluated by the KDQOL-SFTM.
We found a large effect size benefit of physical exercise during hemodialysis on the autonomic modulation of heart rate in our patients with kidney failure. Several prior studies (Agarwal, 2008; Bauer et al., 2008) evaluated interactions of exercise and non-cardiac diseases and showed that physical exercise can influence these variables. Furthermore, as cardiac modulation is highly influenced by emotional factors, a low QOL further predisposes individuals with CKD to greater associated comorbidities and increased mortality. Among our participants, there were many reported benefits on the emotional sub-scale, apparently due to exercise.
According to prior literature (Agarwal, 2008; Bauer et al., 2008), practicing physical exercise reduces the risks of adverse cardiac events by modifying the autonomic balance and improving the sympathovagal balance. The improvement in cardiovascular capacity has significant effects, in turn, on patients’ cardiac autonomic modulation during hemodialysis, since physical practice causes an increase in the time and frequency domains of heart rate variability (Alvarez-Ramirez et al., 2017; Drawz, et al., 2013; Okano, et al., 2010). One prior protocol demonstrated a reduction in cardiovascular episodes associated with structural impairment of vessels or damage to the autonomic nervous system due to the action of uremic toxins with an associated increase in the SDNN, RMSD parameters (Chung et al., 2017). Another study found reduced sympathetic tone and increased vagal tone leading to a lower risk of cardiac outcomes following 10 months of physical activity (Kouidi et al., 2009). There was also an increase in SD1 and SD2 values in the experimental group, due to the aerobic exercise performed in this group. The values of SD1 and SD2, are non-linear variables of heart rate variability and the higher values indicated greater autonomic modulation of heart rate as can occur in hemodialysis ((Da Silva et al., 2016); in both groups, there was an improvement in these values due to the practice of physical exercise (Del Angel et al., 2019).
Limitations and Directions for Further Research
Among this study’s limitations was the small number of participants who met criteria for and were able to complete the study, compared to our larger group of initial volunteers. Significant participant attrition was due to death, hospitalization, changes in access to hemodialysis, and CKD complications during the data collection period, unrelated to exercise during hemodialysis. Many of these factors, such as the location of the double-lumen or permcath catheter, used to perform hemodialysis, could not be controlled by the researchers. While these problems illustrate health problems associated with late stage CKD that can interfere with an exercise intervention, our sample carried sufficient statistical power to lend confidence to our findings, and these results may be best generalized to those patients who are at particular socioeconomic risk. Generalization to other patient groups who may have higher physical activity levels premorbidly and perhaps even during CKD is less certain.
Delays in starting dialysis in patients with CKD can significantly influence changes in motor and cognitive functions and related QOL variables, due to the accumulation of toxic substances produced both by the pathophysiology of the disease and hemodialysis therapy, with its central nervous system repercussions (Abra & Kurella Tamura, 2012; Radić et al., 2011). In this study, it was not possible to determine the minimum time for the initiation of hemodialysis after the diagnosis of CKD, because this information was not available in the participants’ medical records.
Conclusion
Aerobic physical exercise performed during hemodialysis increased self-reported QOL and improved autonomic heart rate modulation for older patients with kidney failure. These data have important implications for expanding physical exercise opportunities during hemodialysis for similar patients. We showed that a practical and effective means of increasing aerobic exercise and obtaining the benefits we demonstrated is to monitor heart rate variability with the use of a cycle ergometer during hemodialysis. A caveat to these benefits is the need and difficulty associated with selecting appropriate patients for this intervention. Further replicative research that examines the time interval between diagnosis of kidney failure and hemodialysis and that uses larger and more diverse participant samples is still needed. The intradialytic exercises should be specifically designed to attend to the specific needs of patients and be practical to utilize during hemodialysis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.