
Abstract
The three-dimensional movement of the horse in physical therapy is a valuable kinesio-therapeutic phenomenon that simultaneously affects several body systems, including particularly the neuromuscular system. However, the effects of equine-assisted services (EAS) on neuromuscular activation patterns in older adults have not been thoroughly investigated. In this study, we evaluated the impact of a 10-weeks EAS program on trunk muscles in older adults who used a saddle and placed their feet in stirrups for the first 15 minutes and out of stirrups for the remaining 15 minutes of 30-minute EAS sessions. We gathered electromyographic (EMG) data of the trunk muscles five times each on the first, fifth, and 10th sessions: pre-EAS and post-EAS on a stationary horse and at 1-minute, 15-minutes, and 30-minutes on a horse in motion. Participants were 20 adults, aged 60–79 years. We analyzed normalized EMG data with 5 (session time) by 3 (session number) analyses of variance (ANOVAs) with repeated measures and with Bonferroni’s testing (p ≤ .05). There was a significant difference over the number of interventions for the right thoracic paravertebral muscle (p = .025) and session time effect for the left trapezius (p = .042), right thoracic paravertebral (p < .001), right and left multifidus (p < .001), and right and left rectus abdominis muscles (p < .001). Thus, trunk muscles in older adults showed complex neuromuscular activation synchronized with the horse’s movement, which was influenced by session time and number of interventions. The practical implication of these findings is that EAS can reduce fall risk among elderly adults of both sexes.
Keywords
Introduction
Maintaining trunk muscle strength is of great importance for locomotive ability and is associated with a lower risk of falls (Sasaki et al., 2018) that are common causes of morbidity and mortality among older adults (Berková & Berka, 2018). Physical exercise has been shown to reduce fall risk (Sherrington et al., 2020), and is a recommended non-pharmacological intervention for older adults (Kouloutbani et al., 2019; Ricci & Cunha, 2020). A sedentary lifestyle should be avoided in all age groups, including the geriatric population (McPhee et al., 2016; Mora & Valencia, 2018), making equine-assisted services (EAS) (Wood & Fields, 2021) an increasingly widespread health rehabilitation offering, even for the elderly (Borges de Araujo et al., 2019; Hilliere et al., 2018; Sylvia et al., 2020).
The three-dimensional movement of a horse is a valuable kinesio-therapeutic experience that influences several body systems simultaneously, including the sensory, limbic, and neuromuscular systems (Koca & Ataseven, 2015). These stimuli are directed to corresponding cortical regions of the central nervous system through integrated and complementary information processing that provides support for producing a desired response (Moraes et al., 2016; Rigby et al., 2020). This constant stimulation may improve the symmetry of trunk muscle activity, muscle balance, mobility, gait ability, and muscle strength (Hilliere et al., 2018; Lakomy-Gawryszewska et al., 2019; Rigby & Grandjean, 2016), all of which are associated in turn with reduced falls or fall risks (Diniz et al., 2020; Sherrington et al., 2020).
A recent systematic review of EAS indicated that, to advance scientific evidence of this intervention, researchers must address existing gaps in fundamental work to date (Wood & Fields, 2021). Another systematic review about the benefits of hippotherapy and horse-riding simulation exercise on the health of older adults showed that different treatment protocols make it difficult to compare results, as the inclusion of postural exercises on the horse can modify the intensity of the intervention; across these studies the duration of the EAS ranged from 8-12 weeks and sessions were conducted 2–3 times per week for 15 and 60 minutes per session involving the use or not of the saddle.
Variables such as intensity, time and equipment can be essential factors in intervention effects. Therefore, the best protocol characteristics cannot be defined with current evidence (Hilliere et al., 2018). To fill these gaps, we designed a basic EAS program that is easy to apply and replicate. Our EAS program consisted of 10 30-minute sessions, scheduled once a week, with the horse walking at a human’s pace as led by a handler. We did not include any exercises during the sessions to evaluate only the effect of the horse’s three-dimensional movement on the rider. A previous study with a cerebral palsy group showed greater neuromuscular activity of the trunk with the feet supported on the stirrups, while participants with Down syndrome and intellectual disability showed greater neuromuscular activity without the stirrups (Lage et al., 2020). However, as we did not find studies with older adults, we used a saddle with feet in the stirrups for the first 15 minutes and out of the stirrups for the remaining 15 minutes of a 30-minute session. Our objective was to evaluate the impact of an EAS program on older adults’ trunk muscles. We assessed electromyographic (EMG) trunk activity five times (pre- and post-EAS on a stationary horse; and at 1-minute, 15-minute, and 30-minute timepoints on a horse in motion) at the first, fifth, and 10th sessions. Our null hypothesis was that the EAS program would not promote neuromuscular stimulation of the trunk of older adults as a function of time within a session or the session number.
Method
Our research design was longitudinal, observational, quantitative, and self-controlled. We used the simple random sampling method (probability sampling). A post hoc sample size calculation was conducted considering α = .05 and power of 95% for the primary outcome EMG activity during the first minute of the first session [mean paravertebral right thoracic muscle = 89 (0, 10) and during the 30th minute of the first session = 96 (.12)], and an effect size of .628. The estimated minimum sample size required was 19 participants. We performed this sample size calculation with G*Power v 3.0.10 software (Franz Faul, Kiel University, Kiel, Germany). Participants were informed verbally and in writing about the purposes and stages of the research protocol, as approved by the Ethics Committee of the University of Triângulo Mineiro, Uberaba, MG, in accordance with Resolution 466/12 of the Brazilian National Health Council (approval number 690.039) and the Brazilian Registry of Clinical Trials (ReBEC), accessed through the link (http://www.ensaiosclinicos.gov.br/rg/RBR6phs67/). All participants provided signed written informed consent prior to their involvement in the study.
Participants
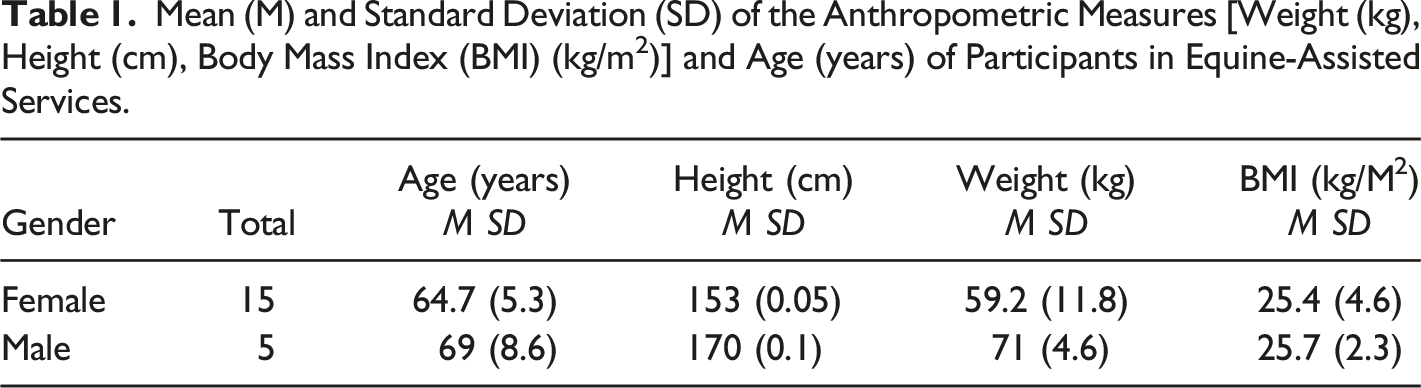
We selected 90 older adults of both sexes for this study, based on inclusion and exclusion criteria determined through clinical examination and anamnesis in which we obtained information regarding personal data, lifestyle, clinical history, diseases, and use of medications. Specifically, inclusion criteria were individuals of both sexes aged between 60–79 years, without gait impairment, severe spinal disorders, shoulder or hip dislocation, and/or equino-phobia. Exclusion criteria were joint pain, musculoskeletal dysfunction, or other diseases at the time of the session. A criterion for discontinuing participation was consistent absences and/or failure to complete the 10 sessions of EAS. All participants began the practice of EAS during the project. A participant flow chart from the start of the study to its end is shown in Figure 1. Ultimately, we evaluated 20 participants (15 women, 5 men; M age = 66.85, SD = 6.95). More detailed participant characteristics are presented in Table 1. Flow Chart. Mean (M) and Standard Deviation (SD) of the Anthropometric Measures [Weight (kg), Height (cm), Body Mass Index (BMI) (kg/m2)] and Age (years) of Participants in Equine-Assisted Services.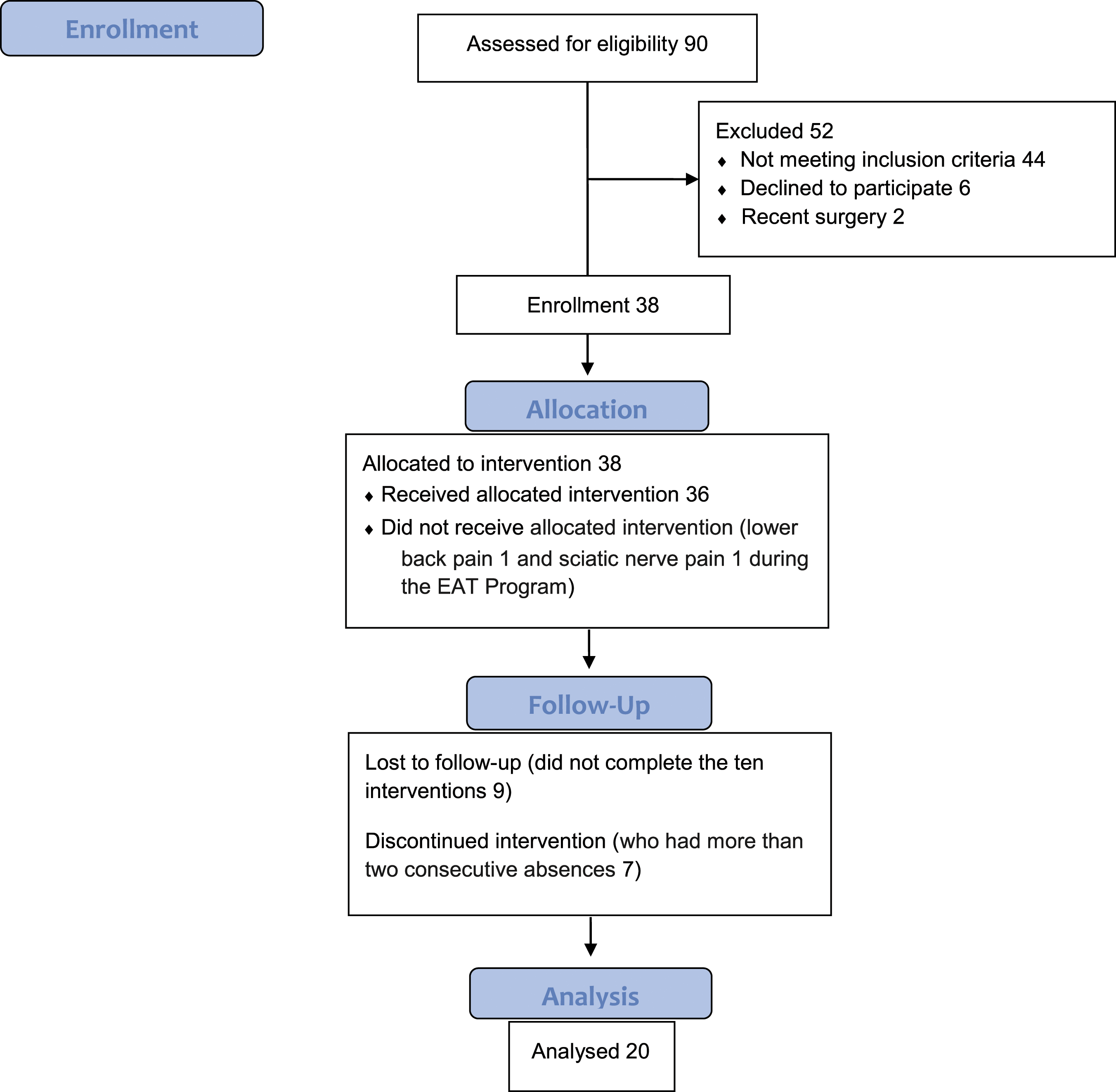
Intervention
Equine-assisted service interventions were performed at the Association of Parents and Friends of the Exceptional in the city of Uberaba, Minas Gerais, Brazil,which contains an appropriate covered area and access platform for getting onto the horses. We randomly used three trained horses. In each session, participants were encouraged to sit upright and relaxed with shoulders back, and to look up and past the horse’s ears. The interventions followed a basic protocol of physical therapy using equine movement. The selected riding material was a saddle, and participants’ rode the first 15 minutes with feet in the stirrups and the last 15 minutes with feet out of the stirrups (Diniz el al., 2020). Physiotherapists qualified by the National Association of EAS performed all interventions.
Data Collection
Electromyographic activity was evaluated using a portable 8-channel wireless, 14-bit signal acquisition resolution, 5000-V electrical insulation surface EMG (EMG800RF, EMG System, São José dos Campos, SP, Brazil) equipped with a data acquisition, control, storage, processing, and analysis system. The signal picked up by the electrodes was amplified 2000 times and filtered with bandpass filters from 5 to 500 Hz and common module rejection >120 dB (dB). One-centimeter (cm) disk-shaped self-adhesive solid foam/Ag/AgCl surface bipolar electrodes were connected to preamplifiers with a center-to-center distance of two cm in diameter. The electrodes were positioned bilaterally in the upper fibers of the trapezius (midline between the acromion and seventh cervical vertebra), thoracic paravertebral muscles (3 cm from the spinous process of the ninth thoracic vertebra), multifidus (3 cm lateral to the level of the spinous process of the fifth lumbar vertebra), and rectus abdominis (3 cm lateral to the umbilicus), following the recommendations of the International Society of Electrophysiology and Kinesiology (ISEK, 2021) and surface electromyography for non-invasive assessment of muscles (SENIAM, 2021). A health professional qualified to use electromyography collected the EMG signal. Before the participant mounted the horse, the professional responsible for the EMG performed the trichotomy (if necessary), cleaned the skin with alcohol and placed the surface electrodes. Electromyographic data collection was performed during the first, fifth, and 10th intervention sessions. The duration of each testing session was collected in each of these sessions five times (10 seconds each time) pre-EAS, during session (at the first, 15th, and 30th minute), and at post-EAS. These time intervals were selected because they were at the beginning, in the middle and at the end of each session and treatment. During the pre-session, the participant was seated in the saddle with the weight balanced on the seat bones and the feet supported (not pushing) on the stirrups. During the post-session, the feet were out of the stirrup. In these two moments the EMG signal was recorded with the horse stationary. The other times of the session were recorded with the horse in motion. A time-domain variable, root mean square (RMS), was used to process the EMG signal (McManus et al., 2020). Root mean square values were obtained in microvolts/second (μV) and normalized by maximal voluntary isometric contraction (MVIC) for 10 s. Normalized RMS values were used for statistical analysis.
Data Analysis
We used the Statistical Package for Social Sciences (SPSS ® Statistics, v. 234.0), IBM Corp., Amonk, NY) to analyze the data. Normalized EMG data were analyzed using descriptive statistics and a two-factor analysis of variance (ANOVA) with repeated measures and Bonferroni post-hoc tests. Factor one was time within session (at pre-EAS, at first, 15th, and 30th minute during EAS, and at post-EAS) and factor two was the intervention number (first, fifth, and 10th sessions). We performed the Mauchly sphericity test for sphericity, and, if sphericity assumptions were violated, we performed the Greenhouse–Geisser correction in degrees of freedom. We used a statistical significance level of p < .05 for all analyses.
Results
Quantitative Analysis of the Electromyographic Activity of the Trunk Muscles for Effects of Session Time, Intervention Number and the Interaction Effect of Both Factors.
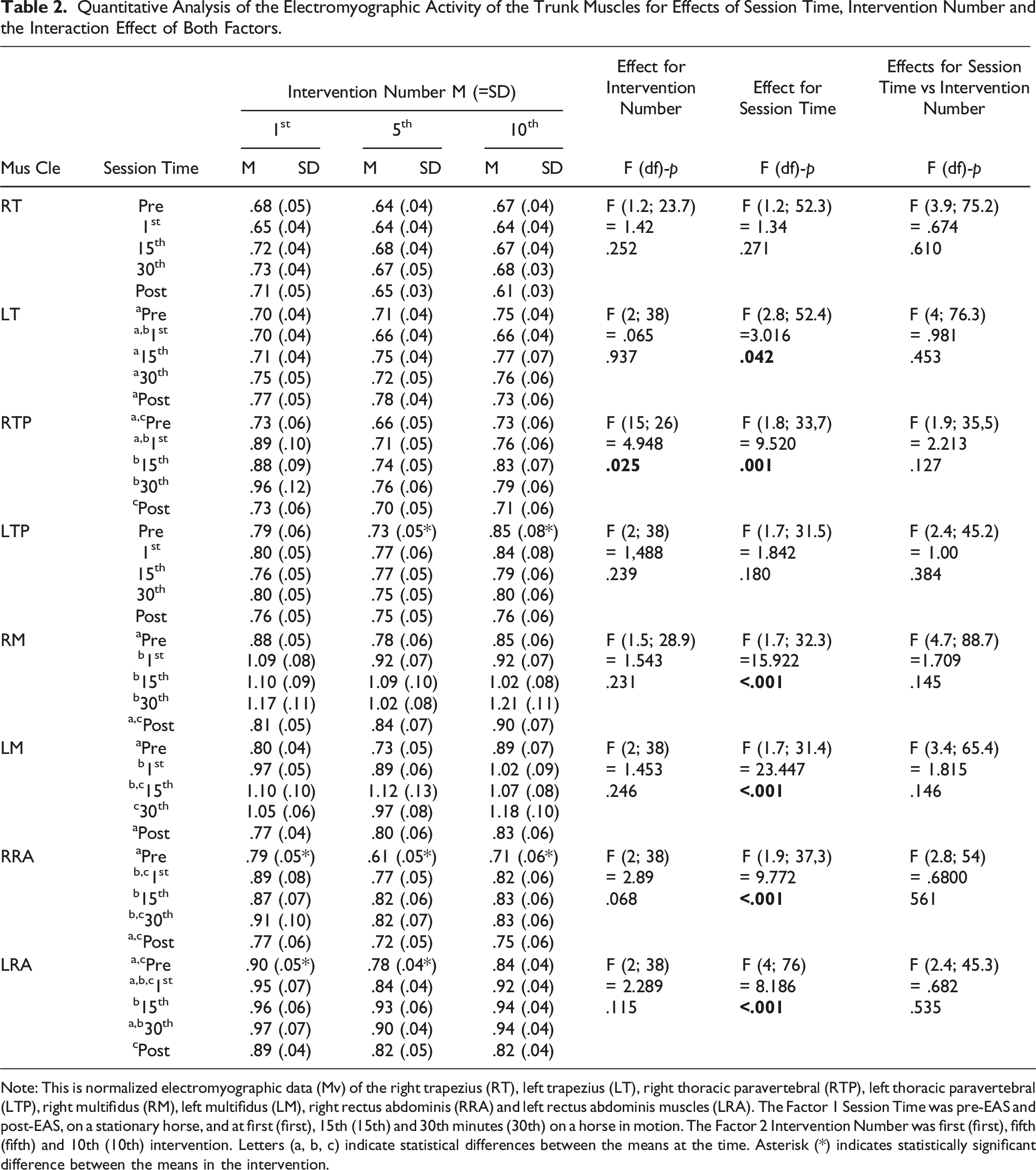
Note: This is normalized electromyographic data (Mv) of the right trapezius (RT), left trapezius (LT), right thoracic paravertebral (RTP), left thoracic paravertebral (LTP), right multifidus (RM), left multifidus (LM), right rectus abdominis (RRA) and left rectus abdominis muscles (LRA). The Factor 1 Session Time was pre-EAS and post-EAS, on a stationary horse, and at first (first), 15th (15th) and 30th minutes (30th) on a horse in motion. The Factor 2 Intervention Number was first (first), fifth (fifth) and 10th (10th) intervention. Letters (a, b, c) indicate statistical differences between the means at the time. Asterisk (*) indicates statistically significant difference between the means in the intervention.
Discussion
The surface EMG we used to record trunk muscle activation in this EAS study is a reliable technique for evaluating neuromuscular activation and improving knowledge of muscle biomechanics. This method provides an objective and accurate assessment of neuromuscular activation patterns even during complex movements (Stastny et al., 2017). These neuromuscular activation patterns should be considered when selecting and prescribing physical exercises, since the force of muscle contraction is regulated by the total number of motor units recruited. The recruitment of low- or high-threshold motor units depends on exercise intensity (McManus et al., 2020; Oliva-Lozano & Muyor, 2020). The analysis of neuromuscular activation of the trunk of older adults during our 10-week EAS program for older adults showed positive results over time and intervention number effects when using a saddle with feet supported or not in the stirrups. Thus, we rejected the null hypothesis of no effect of this intervention. These data are consistent with EAS literature for individuals with motor control deficiency of the trunk (A. Espindula et al., 2015; A. P. Espindula et al., 2012) and healthy children (Bravo Gonçalves Junior et al., 2020). These results allow for a more reliable analysis of the effects of practice and help devise more promising treatments in terms of mount type, intervention number, and adequate duration of the EAS session (Stergiou et al., 2017; Wood & Fields, 2021).
The upper trapezius muscle was the only muscle that showed an initial decrease in neuromuscular activation in the first minute, followed by an increase after 15 minutes of the session when compared to levels at the initial rest. These data may be explained by the modulation of postural response amplitudes. The cranial extremity is most spatially displaced during three-dimensional movements of the equine (Bravo Gonçalves Junior et al., 2020). However, at the beginning of the session, the individual may be tenser and show a lower postural amplitude. Thus, the trapezius muscle can enter a feedforward state, defined as a preventive action that occurs prior to the sensory detection of a homeostatic rupture (Kobesova & Kolar, 2014). With repeated exposure to movement, a more confident and relaxed rider can increase body balance and demonstrate greater amplitude postural responses by refining response characteristics to optimize task effectiveness. The rider needs to keep the head up, shoulders aligned and level, and arms relaxed. To maintain this balanced position, reflex contractions of the agonist and antagonist muscles are necessary throughout the body, including the muscles of the head, neck, and trunk (Goodworth et al., 2019). The trapezius is a superficial muscle that is easily recruited during many movements of the head and shoulders (Cheng et al., 2016). The increasing myoelectric activation of the trapezius muscle during EAS has been confirmed in other studies of chronic non-progressive encephalopathy (A. P. Espindula et al., 2012), Down syndrome (A. Espindula et al., 2015), and healthy children (Bravo Gonçalves Junior et al., 2020).
The thoracic paravertebral, multifidus, and rectus abdominis muscles showed an increase in neuromuscular activation 1 min after the session in relation to the initial riding and at the end of the session. These results were expected, because the gain in neuromuscular activation increased when the horse was in motion. The somatosensory, vestibular, and musculoskeletal systems stimulated by equine movement can influence postural tone distribution in the trunk (Park et al., 2021; Silva et al., 2021). In contrast, the lowest EMG values were recorded in the pre- and post-intervention moments when the horse was stationary. These results are confirmed by other studies, because even when stopped, the horse is not immobile, as it changes its support, flexes its neck, moves its head, and shakes its tail, generating stimuli and triggering tonic adjustments by the rider (A. P. Espindula et al., 2014; Ribeiro et al., 2019). In addition, myoelectric activity above resting levels is present during an upright posture, suggesting that some degree of muscle activation is necessary to support the spine and generate postural stability (Kienbacher et al., 2015).
The right thoracic paravertebral muscle also showed a reduction in neuromuscular activation throughout the intervention compared to that in the first session. The thoracic paravertebral, erector muscle of the spine, is one of those responsible for the maintenance of posture. A lower amplitude of the EMG signal indicates a smaller number of motor units recruited to perform the same movement, indicating greater efficiency of the muscular fibers, that is, better muscular conditioning (McManus et al., 2020). Repetitive exposure to equine movements promotes effective motor learning, making the spine resilient in the required function. A study of the trunk musculature of individuals with Down syndrome showed a reduction in the signal amplitude after the 25th session (A. P. Espindula et al., 2015). Other studies are needed to assess whether an EAS program with a longer duration or a greater number of weekly sessions can improve the conditioning of the other muscles evaluated. The highest mean normalized EMG values were recorded for the core muscles assessed (multifidus and rectus abdominis). The multifidus is one of the posterior muscles responsible for trunk extension, while the abdominal muscles perform the opposite movement of trunk flexion. The “core,” also referred to as the lumbopelvic-hip complex, is a 3-dimensional space with muscular boundaries: diaphragm, abdominal, oblique muscles, paraspinal, gluteal muscles, pelvic floor and hip girdle (Akuthota & Nadler, 2004). The core muscles are the center of the body, where most kinetic chains transfer force to the extremities. Proper core functioning promotes spinal stabilization in both static and dynamic postures (Oliva-Lozano & Muyor, 2020). Effective stabilization of the lumbopelvic-hip complex is not possible if the core muscles are exercised in isolation. Synergistic work increases the stability and motor control of this complex (Huxel Bliven & Anderson, 2013). The lumbopelvic-hip region is highly stimulated in the horseback riding movement because it is the region of the trunk that absorbs the impact created between the horse and rider (Garner & Rigby, 2015). Given that the greater the EMG activity, the greater the challenge to the neuromuscular system, equine movement may be useful for strengthening the core. These results corroborate a study that demonstrated that simulated and real horseback riding activates the core muscles in younger and older adults (Kim et al., 2018). In addition, the result was enhanced when core exercise was performed slowly, controlled, and with good breathing. The horse’s gait during walking is consistent, cyclical, rhythmic, bilateral, and symmetrical (Garner & Rigby, 2015; Lightsey et al., 2021). Pelvic mobilization during riding favors diaphragmatic breathing due to the accommodation of the organs located in the abdomen, lowering of the diaphragm, and increase in inspiratory volume (Valle et al., 2014). Repetitive neuromuscular activation of core muscles promotes body alignment, prevention and reduction of low back pain, maintenance of trunk joint mobility, and improved balance and gait performance. Stable and strong core muscles contribute to more efficient use of the upper and lower limbs and are important for the successful performance of day-to-day activities during old age, such as walking, chair stand tasks and are associated with a lower risk of falls (Ishak et al., 2016; Kato et al., 2019). A study using the same EAS Program showed that EAS improved functional mobility, dynamic balance and flexibility in older adults (Diniz et al., 2020). A systematic review showed this effective therapy improves physical function (balance, core and lower limb muscle strength, mobility and gait speed), in addition, it improves hormone levels (reduces cortisol and increases serotonin) and brain activity (Hilliere et al., 2018). The gains in functional capacity reflect the ability to perform routine tasks, simple or complex, necessary for an independent and autonomous life in society. Functional capacity is related to physical, cognitive and emotional aspects of the individual (Liu et al., 2014).
To improve horseback riding, experienced riders have recommended removing the feet from the stirrups, thus increasing the balance and harmony between the horse and rider. However, few studies have evaluated this method of riding in EAS (Guptill, 2018; Madden, 2020). Studies with healthy individuals concluded that placing the feet in stirrups promoted greater muscle activation (Bravo Gonçalves Junior et al., 2020; Ribeiro et al., 2018). In another study, Down syndrome and intellectual disability groups presented greater neuromuscular activity of the trunk and lower limbs without the feet supported in the stirrups, whereas a cerebral palsy group presented greater neuromuscular activity with the feet supported in the stirrups (Lage et al., 2020). In our study, there was no significant difference in the body trunk musculature when the feet were inside or outside the stirrups.
In short, the trunk muscles showed complex neuromuscular activation synchronized with equine movement. However, studies involving EMG and EAS are scarce, and different muscles have been evaluated, making a comparison of results between studies even more challenging. Our findings may contribute to the enrichment of EAS scientific knowledge and suggest that older adults may also benefit from EAS practice in view of increased neuromuscular activations (especially in the core muscles) during for them during these interventions. For the mount type, we found no differences in using a saddle with feet supported in the stirrups or not. For the effects of session time, neuromuscular activation increased during the 30-minute sessions for all muscles evaluated. For intervention number, the EAS program with 10 weekly sessions promoted better conditioning of the thoracic paravertebral muscle.
Limitations and Directions for Further Research
While our results reveal that EAS offers an alternative to traditional exercise programs for older adults, our study was limited by the number of interventions for the thoracic paravertebral muscle; and the other muscles seem to require a longer program. Future research will need to elucidate whether (a) a longer-duration EAS program or a greater number of weekly sessions can improve the conditioning of other muscles; (b) EAS offers psychological and social benefits, and (c) similar benefits may accrue to various clinical populations.
Conclusion
This study demonstrated that trunk muscles in older adults showed complex neuromuscular activation that synchronized with movement of the horse in physical therapy. This change was influenced by both the time within sessions and the session number. We did not find different effects from placing feet in or outside of stirrups. These data provide support for EAS as a means of reducing fall risk among elderly adults of both sexes. The muscle activation pattern assessed should be considered when choosing and prescribing the mount type, intervention number, and appropriate length of the session to increase the effectiveness of the EAS intervention. Further research is necessary to further address these variables.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors are grateful for financial support received for this research, provided by the following institutions: Coordination of Improvement of Higher Level Personnel (CAPES), National Council for Scientific and Technological Development (CNPq), Foundation for Research Support of the State of Minas Gerais (FAPEMIG), Uberaba Teaching and Research Foundation (FUNEPU) and Association of Parents and Friends of the Exceptional of Uberaba (APAE).
Ethic Approval Information
Disclosure
The interventions were performed at the Association of Parents and Friends of the Exceptional in the city of Uberaba, Minas Gerais, Brazil.