
Abstract
Gradual and sustained increases in resting blood pressure are accompanied by gradual and sustained reductions in the capacity to consciously experience several affective and somatosensory processes. Burgeoning theory suggests that this phenomenon, termed cardiovascular emotional dampening, contributes to heart disease risk by interfering with our ability to effectively respond to environmental demands. Interpersonal relationships are contexts in which this risk cascade likely occurs, but prior researchers have paid little attention to how emotional dampening might influence these relationships. As empathy is a construct used to describe facets of emotion-linked responding that facilitate interpersonal relationships, if emotional dampening influences interpersonal relationships, then we might expect resting blood pressure to covary with measures of empathy as it does with other previously studied aspects of affective responding. We recruited 175 healthy undergraduate college student participants (120 Women; M age = 19.17, SD age = 2.08) to complete a counterbalanced procedure in which we measured resting blood pressure and related it to participants’ responses on the Toronto Alexithymia Scale, the Questionnaire of Cognitive and Affective Empathy, and a demographic survey. Bivariate comparisons revealed a significant inverse relationship between average resting systolic blood pressure (SBP) and cognitive empathy, as well as a significant inverse relationship between SBP and affective empathy. Multiple regression analyses revealed that SBP remained a significant predictor of cognitive empathy, but not affective empathy, after controlling for related covariates (i.e., sex, age, and alexithymia). SBP predicted cognitive empathy such that higher SBP was associated with lower cognitive empathy. Thus, people with higher resting blood pressures might experience increased interpersonal distress because of a reduced capacity for empathetic accuracy and perspective-taking. We discuss the implications and future directions of these findings.
Introduction
Multiple past investigations have provided evidence that gradual and sustained increases in resting blood pressure accompany reductions in the capacity to consciously experience affective and somatosensory processes (Delgado et al., 2014, Inagaki et al., 2018, Loveless et al., 2018, McCubbin et al., 2011, 2014, 2018, Pury et al., 2004, Saccò et al., 2013, Shukla et al., 2018, 2019, 2020, Yoris et al., 2020). Researchers have termed this phenomenon, “cardiovascular emotional dampening,” and they have proposed that it contributes to heart disease risk by hindering effective responses to environmental demands (Delgado et al., 2014, McCubbin et al., 2014, 2018). While interpersonal relationships are contexts in which such demands occur, there has been minimal research attention paid to how emotional dampening might influence these relationships. Other lines of research have established robust connections between blood-pressure and relationship quality, and the theory developed around this work has assumed that increases in resting blood pressure are caused by overexposure to problematic relationships (Birmingham et al., 2019, Holt-Lunstad & Uchino, 2019). While that may be true, increases in resting blood pressure may also contribute to the development of problematic relationships via the emotional dampening phenomenon (McCubbin et al., 2014, 2018, Pury et al., 2004). In the present study we explored this idea by determining if resting blood pressure would covary with self-reported aspects of emotional responding that are unique to facilitating interpersonal relationships, like affective and cognitive empathy.
The Risk Cascade Associated with Cardiovascular Emotional Dampening
Cardiovascular emotional dampening is a psychophysiological phenomenon wherein sustained increases in resting blood pressure have seemed to co-occur with (a) a restricted capacity to experience emotion, whether evoked explicitly or implicitly (Delgado et al., 2014, Loveless et al., 2018, McCubbin et al., 2011, 2014, Pury et al., 2004, Shukla et al., 2019, 2020), (b) reduced sensitivity to acute physical pain and interoceptive cuing (Saccò et al., 2013, Yoris et al., 2020), (c) reduced sensitivity to emotional pain (Inagaki et al., 2018), and (d) an increased propensity to engage in appetitive as well as risky behavior (Loveless et al., 2018, McCubbin et al., 2018, 2020). While researchers have studied this phenomenon across a variety of adult-aged samples, they and have not consistently observed any apparent moderating influences of health status, sex, age, socioeconomic status, or cultural background. Emotional dampening has been appreciated within normotensive, pre-hypertensive, and hypertensive blood pressure samples, and it has been shown to be distinct from similar constructs like alexithymia and those which underlie an emotionally repressive coping style (McCubbin et al., 2011, Pury et al., 2004, Shukla et al., 2018). While the physiological mechanisms that support this phenomenon are not completely understood, neurovisceral dysregulation involving afferent inhibitory baroreceptor signaling as well as altered central nervous system control of autonomic functioning are likely involved (Critchley & Harrison, 2013, Delgado et al., 2014, Hagemann et al., 2003, McCubbin et al., 2011, 2018, 2020, Taggart et al., 2016, Thayer & Lane, 2000).
The hypothesized link between emotional dampening and heart disease risk is believed to occur through the development of hypertension, the sustained abnormal elevation of resting blood pressure. Broadly, the regulation of blood pressure occurs via the interplay between the cardiovascular, endocrine, and nervous systems. Feedback and feedforward loops within and across these systems allow the body to effectively martial resources to respond to stressors, with sustained elevations in resting blood pressure typically denoting some failure in the proper regulation of these mechanisms (Hagemann et al., 2003, Johnson et al., 2015, Thayer et al., 2000). Several researchers have hypothesized that emotional dampening contributes to the development of hypertension via a failure in the ability to consciously detect and effectively respond to stressors (Delgado et al., 2014, McCubbin et al., 2014, 2018). If emotions are adaptive psychophysiological responses to stressors (Buck, 1985) and sustained elevations in resting blood pressure dampen emotional responsivity (Delgado et al., 2014, Loveless et al., 2018, Pury et al., 2004, Shulka et al., 2019, 2020), then there may be perpetuation of a positive feedback loop wherein stress exposure heightens blood pressure that, in turn, reduces emotional responsivity, interferes with adaptive responding, and thwarted adaptive responding completes the circle by perpetuating further stress (Delgado et al., 2014, McCubbin et al., 2014, 2018). This process has been termed the cardiovascular emotional dampening cascade, whose logical consequences would be the eventual onset of hypertension and increased risk of other cardiovascular disease.
Interpersonal relationships are contexts in which the cardiovascular emotional dampening cascade may reasonably be expected to occur. Although the emotional dampening literature only hypothesizes about the caustic influence of this process on interpersonal relationships via the creation of psychosocial distress (McCubbin et al., 2014, 2018, Pury et al., 2004), intimate connections between relationship quality and indicators of cardiovascular health have been revealed by other lines of research. In their review of the literature, Holt-Lunstad and Uchino (2019) explained that interpersonal relationships considered to be ambivalent have been associated with particularly deleterious cardiovascular system behavior. Ambivalent relationships are defined as containing both a high degree of positive and negative aspects; thus, they have tended to be experienced as neither fully supportive nor regularly aversive (Holt-Lunstad & Uchino, 2019; Uchino et al., 2001). The literature on ambivalent social relationships may support the hypothesis that psychosocial distress is a consequence of the cardiovascular emotional dampening cascade.
The state of current evidence regarding the connection between relationship ambivalence and deleterious cardiovascular system behavior is quite robust. Several cross-sectional laboratory studies have demonstrated that both explicit and implicit exposure to ambivalent social connections may evoke increased cardiovascular reactivity (as measured by changes in blood pressure, heart rate, and heart rate variability) and slower recovery during and following acute stress exposure relative to exposure to more wholly supportive social network ties (Holt-Lunstad & Uchino, 2019). Other evidence from both cross-sectional and longitudinal laboratory studies also suggests that those with a greater baseline quantity of ambivalent social ties have reflected greater cardiovascular reactivity during stress and that changes in cardiovascular reactivity over time have seemed to covary with changes in exposure to those ambivalent relationship ties such that increased exposure has been associated with increased cardiovascular reactivity (Holt-Lunstad & Uchino, 2019). Longitudinal observations have demonstrated that individuals who experience more interactions with ambivalent social connections have tended to have higher ambulatory blood pressures throughout the day, relative to those with less interactions with ambivalent social connections (Birmingham et al., 2019, Holt-Lunstad & Uchino, 2019). These findings collectively lend support to the notion that relationship quality and cardiovascular outcomes are linked; however, prior investigators have presumed that changes in cardiovascular system behavior (and consequently cardiovascular health) are merely consequences of ambivalent relationship exposure. Within the cardiovascular emotional dampening cascade, sustained changes to cardiovascular system functioning may both contribute to and represent a consequence of increased ambivalent interpersonal relationships.
If the cardiovascular emotional dampening cascade promotes ambivalence in interpersonal relationships, then we would expect to observe associations between resting blood pressure and aspects of emotional responding that are unique to the facilitation of interpersonal relationships. Empathy is a multidimensional construct used to describe our ability to appreciate the lived experience of others (Davis, 1983, Kerem et al., 2001). It is comprised of two subordinate facets, both of which have been demonstrated to be essential in the establishment and maintenance of variety of interpersonal relationships (Fincham et al., 2002, Gungordu et al., 2022, Holt-Lunstad & Uchino, 2019, Paleari et al., 2005, Verhofstadt et al., 2016). The first is affective empathy, which refers to our ability to experience similar emotions to those expressed by others; the second is cognitive empathy, which refers to our ability to take the perspective of others (Davis, 1983, Kerem et al., 2001). Largely considered to occur as a function of simulation, the neurophysiological pathways responsible for both types of empathetic responding share close structural and functional similarities with those implicated in the direct experience of emotionally evocative events, with quick bottom-up mechanisms associated with affective empathy and slow top-down mechanisms associated with cognitive empathy (Bonini et al., 2022, Lamm & Majdandžić, 2015, Uribe et al., 2019, Yu & Chou, 2018). Given this and the evidence which links sustained elevations of resting blood pressure to reduced implicit as well as explicit emotion recognition and responding, we should expect to observe inverse relationships between resting blood pressure and measures of both domains of empathy (Delgado et al., 2014, Loveless et al., 2018, McCubbin et al., 2011, 2014, Pury et al., 2004, Shulka et al., 2019, 2020).
The Present Study
The present study probes the associations between resting blood pressure and empathy with a correlational design. Specifically, we explored the relationships between resting blood pressure, trait affective empathy, trait cognitive empathy, and other covariates among a sample of healthy undergraduate college students recruited from a large public university in the Southeastern United States. We hypothesized that resting blood pressure would be inversely related to measures of trait empathy, and that resting blood pressure would maintain its associations with the measures of trait empathy after controlling for covariates known to covary with trait empathy, like age, sex, and alexithymia (Beadle & de la Vega, 2019, Grynberg et al., 2010).
Method
Ethical Considerations
The Middle Tennessee State University Institutional Review Board reviewed and approved all methods, materials, and procedures used in this study. All participants provided their informed consent for participation, and all were compensated for their participation via course credit.
Participants
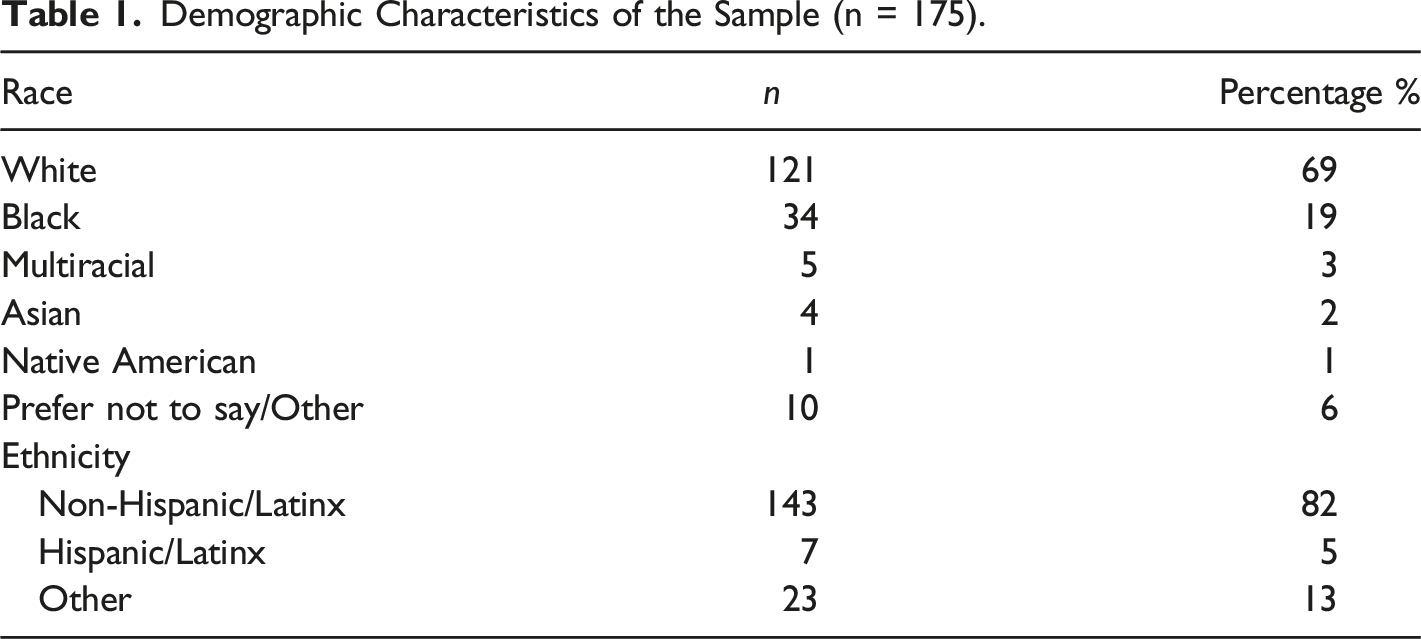
We recruited a sample of 175 healthy undergraduate student participants (120 Women; M age = 19.17, SD age = 2.08, Min age = 18, Max age = 38) from the Middle Tennessee State University, Department of Psychology’s volunteer participant pool. A priori power analyses conducted using G*Power (Faul et al., 2009) indicated that a minimum sample size of 84 participants would be necessary to observe medium effects among bivariate correlation analyses (given that β = .20 and α = .05), and that a minimum sample size of 92 participants would be needed to observe medium effects among multiple regression models with five predictors (again, given that β = .20 and α = .05). Given the medium sized effects observed in other cardiovascular emotional dampening studies (Loveless et al., 2018, McCubbin et al., 2011, 2014, 2018, 2020, Pury et al., 2004, Shukla et al., 2018, 2019), the present study should be sufficiently powered with the aforementioned sample size.
Demographic Characteristics of the Sample (n = 175).
Materials
Questionnaire of Cognitive and Affective Empathy
We used the Questionnaire of Cognitive and Affective Empathy (QCAE; Reniers et al., 2011) to measure dispositional empathy. The QCAE is a 31-item self-report measure of cognitive and affective empathy that was empirically derived from several well-established measures of empathy to create a more comprehensive measure of both facets (Reniers et al., 2011). Items in the QCAE are presented as statements, and respondents are asked to indicate their level agreement for each using a 4-point Likert scale wherein, 1 indicates, “Strongly Disagee,” and 4 indicates “Strongly Agree.” Respondent selections are then summed to calculate five separate subscale scores, two of which are summed to derive a cognitive empathy scale score and three of which are summed to derive an affective empathy scale score. Higher scale scores indicate greater empathetic ability within each dimension (Reniers et al., 2011). For the purposes of this study, we only used scores on the two main scales in the data analysis.
Available psychometric data associated with the QCAE support the notion that it is a reliable and valid measure of cognitive and affective empathy among non-clinical samples (Reniers et al., 2011). With respect to internal consistency, recent studies have reported alpha coefficients ranging between .87 and .89 for the cognitive empathy scale, as well as .78 and .88 for those related to the affective empathy scale (Lockwood et al., 2014, Powell, 2018). Work by Powell and Roberts (2017) has provided evidence that the instrument possesses decent test-retest reliability, and there is there is ample support for the validity of the measure to include evidence of convergent validity, discriminant validity, and predictive validity (Horan et al., 2015, Michaels et al., 2014, Reiners et al., 2011). In the present sample, Cronbach’s alphas for the cognitive empathy and affective empathy scales were consistent with those that have been reported in the published literature (α = .84 and α = .77 for the cognitive empathy and affective empathy scales, respectively).
Twenty Item Toronto Alexithymia Scale
We used the Twenty Item Toronto Alexithymia Scale (TAS-20; Bagby et al., 1994) to measure alexithymia. The TAS-20 is the successor of the original Toronto Alexithymia Scale developed by Taylor et al. (1985). Revised in 1994, it has become one of the most popular self-report measures of alexithymia (Bagby, et al., 1994, Bagby, et al., 2020). Items in the TAS-20 are presented as statements, and respondents are asked to indicate their level agreement for each using a 5-point Likert scale wherein, 1 indicates, “Strongly Disagree,” and 5 indicates, “Strongly Agree.” Respondent selections are then summed to calculate three separate subscale scores, all of which are summed to produce a total alexithymia score. Higher total scores indicate a greater degree of alexithymia (Bagby, et al., 1994). For the purposes of this study, we used the total scores in the data analysis.
Available psychometric data support the reliability and validity of the TAS-20. The original validation study reports that the internal consistency estimate for the entire instrument was good (α = .80), and internal consistency estimates from subsequent published research which utilized this instrument have been consistent with such (Bagby et al., 1994, 2020). Additionally, previous work has demonstrated that the instrument possesses good test-retest reliability, and there is an abundance of evidence to suggest that the measure possesses good construct validity (Bagby et al., 2020). In the present sample, Cronbach’s alpha for the whole instrument was consistent with those reported in the published literature (α = .83).
Demographics Questionnaire
We created a 5-item questionnaire to collect demographic information. It featured a free-response question which asked about age, and four multiple choice questions which asked about participants’ assigned sex at birth, current gender identity, racial identity, and ethnic identity.
GE Carescape V100 Vital Signs Monitor
We collected blood pressure data in accordance with the American Heart Association’s recommendations for reliable and valid blood pressure measurement in clinical and laboratory settings (Pickering et al., 2005). Our laboratory features a calibrated GE Carescape V100 Vital Signs Monitor (General Electric Company; Fairfield, CT), which we employed within an isolated, sound attenuated, and well-lit participant chamber to take blood pressure measurements within a distraction free environment. Participants sat upright in a supportive chair with their feet resting flat on the floor and their non-dominant arm resting on a table. Constrictive jewelry was removed, and cellphones were not allowed in the participant chamber. An appropriately sized blood pressure cuff was placed around the upper part of the non-dominant arm, just above the elbow. Participants were instructed to relax and make as little movement as possible. We recorded resting blood pressure discontinuously at 2-min intervals for a 12-min period, while observing participants via a webcam within the chamber to verify compliance with instructions. We used averages of the final three readings to capture participants’ resting systolic and diastolic blood pressures, respectively.
Procedures
Individuals interested in participating in the study scheduled a laboratory appointment wherein we informed them regarding the research details, screened them and provided the opportunity for them to give their informed consent. Consenting participants then completed a counterbalanced procedure whereby resting blood pressure was measured and surveys were administered. We recorded blood pressure measurements within an isolated, sound attenuated, and well-lit participant booth, and administered surveys via Qualtrics (Qualtrics, Provo, UT) at a quiet participant computer workstation within the lab. We set Qualtrics to randomize the survey order; however, the demographics questionnaire was administered last. After the completion of the study, a member of the research team debriefed the participants, assigned their participation credits, and then dismissed them.
Statistical Analysis
We primarily analyzed our data using IBM SPSS (Version 26); however, we also used SAS (Version 9.4) and R Squared (Version 1.1) to compute confidence intervals for correlation and regression coefficients, respectively. We began our analysis by inspecting the data for quality, missing values, and normality of data distributions. Additionally, we also probed for order effects. Next, we used univariate procedures (means and standard deviations) to describe the data, and bivariate procedures (Pearson correlation procedures) to explore the relationships between our variables of interest. We then used a series of multiple regression analyses to predict affective and cognitive empathy scores from sex, age, alexithymia, and blood pressure. Because researchers have observed significant interactions between sex and blood pressure on various criterion variables in other emotional dampening studies (Loveless et al., 2018, McCubbin et al., 2014, 2020), we conducted hierarchical multiple regressions to probe for such. In these models, we included our predictors in step 1 and a Sex X Blood Pressure interaction term in step 2. Finally, we used follow-up simultaneous multiple regression analyses with the interaction term dropped for those models where the interaction term was non-significant. For all analyses, we considered a p-value of <.05 statistically significant.
Results
We included all collected data in our analyses, as there were no missing values, and the data were sufficiently normally distributed. Additionally, we observed no order effects, so order was not included as covariate in the subsequent analyses.
Univariate and Bivariate Analyses
Descriptive Statistics and Bivariate Comparisons (n = 175).
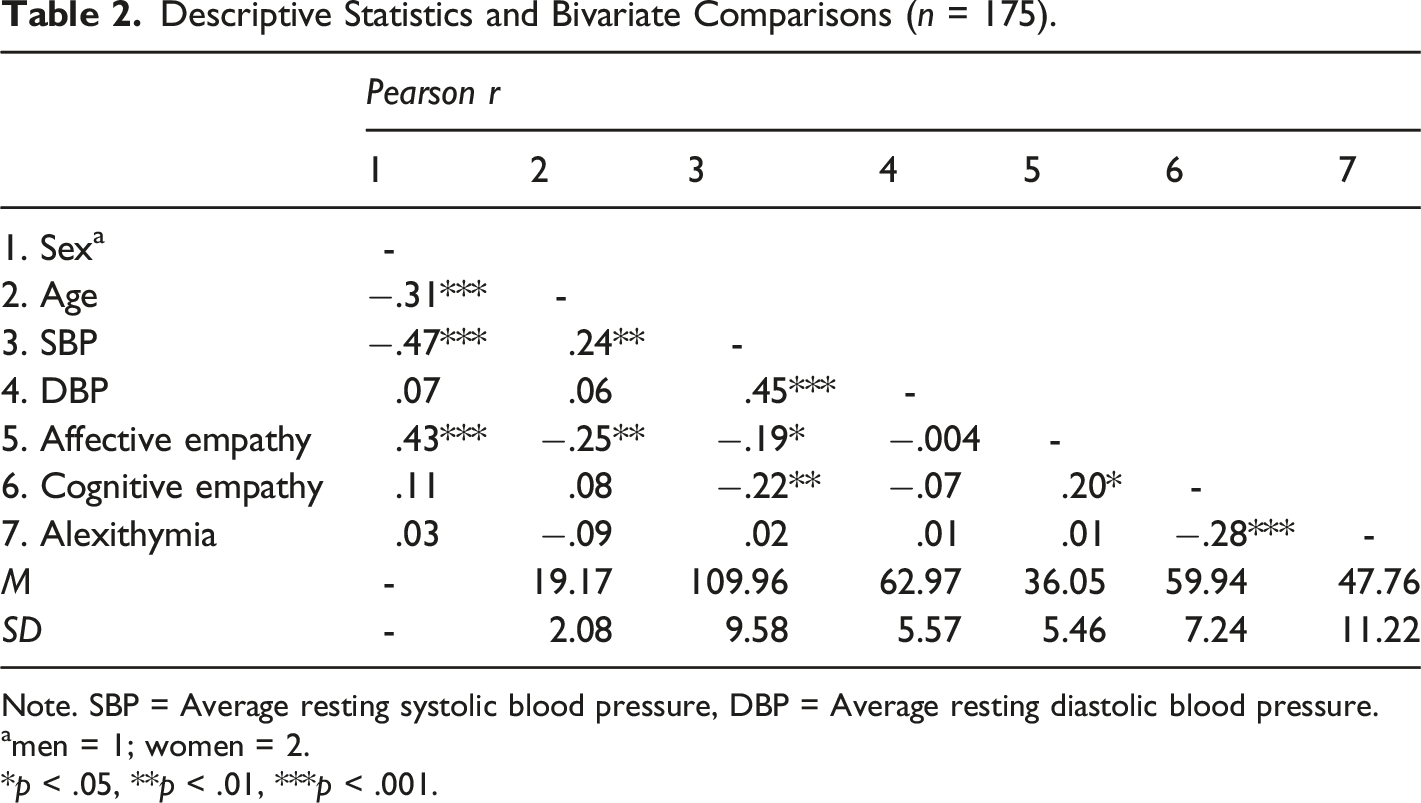
Note. SBP = Average resting systolic blood pressure, DBP = Average resting diastolic blood pressure.
amen = 1; women = 2.
*p < .05, **p < .01, ***p < .001.
We also observed additional significant findings relative to both age and average resting systolic blood pressure, respectively. Regarding age, average resting systolic blood pressure was significantly related to age such that increases in age corresponded with increases in average resting systolic blood pressure; r = .24, n = 175, p = .002, 95% CI [.09, .38]. Age was also negatively associated with affective empathy, indicating that younger individuals endorsed a greater tendency to experience emotion states similar to that of those around them when in a situation where emotions are evoked; r = −.25, n = 175, p = .001, 95% CI [-.39, −.10]. Regarding average resting systolic blood pressure, it was significantly related to average resting diastolic blood pressure such that as one increased so too did the other; r = .45, n = 175, p < .001, 95% CI [.32, .56]. Significant inverse relationships were also observed between average resting systolic blood pressure and affective empathy (r = −.19, n = 175, p = .01, 95% CI [-.33, −.04]) as well as average resting systolic blood pressure and cognitive empathy (r = −.22, n = 175, p = .003, 95% CI [-.36, −.07]), respectively. Individuals with higher average resting systolic blood pressures endorsed a reduced tendency to experience emotion states similar to those around them when in a situation where emotions are evoked as well as a reduced propensity towards taking others’ perspectives when reflecting on their behavior.
Finally, we observed significant relationships between affective empathy, cognitive empathy, and alexithymia. Affective empathy was significantly related to cognitive empathy such that individuals who endorsed greater levels of one also endorsed greater levels of the other; r = .20, n = 175, p = .01, 95% CI [.05, .34]. Cognitive empathy was also inversely related to alexithymia, indicating that individuals who endorsed a greater propensity towards taking others’ perspectives when reflecting on their behavior tended to endorse lower levels of difficulty with recognizing and describing emotion; r = .20, n = 175, p = .01, 95% CI [.05, .34].
Multivariate Analyses
Hierarchical Multiple Regression Results for Sex × SBP interaction (Model 1 With Interaction Term Added).
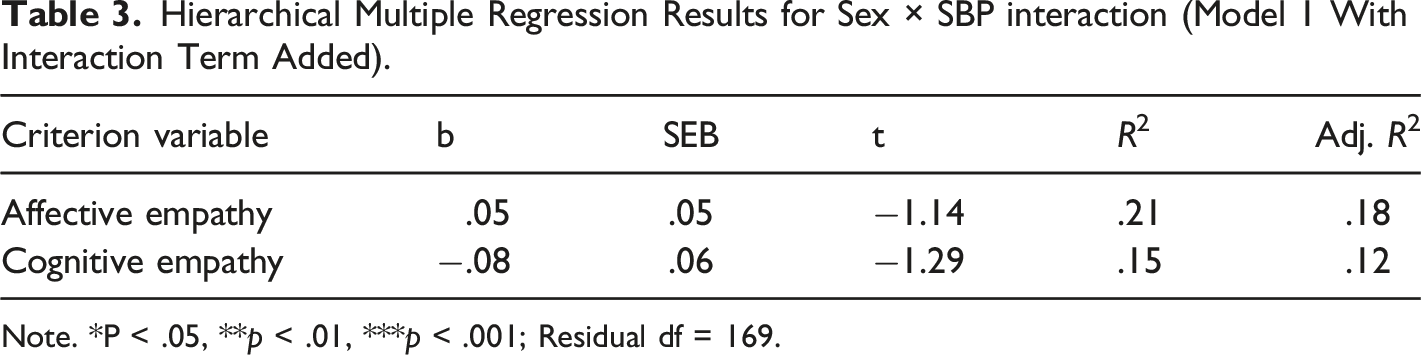
Note. *P < .05, **p < .01, ***p < .001; Residual df = 169.
Simultaneous Multiple Regression Predicting Affective Empathy.
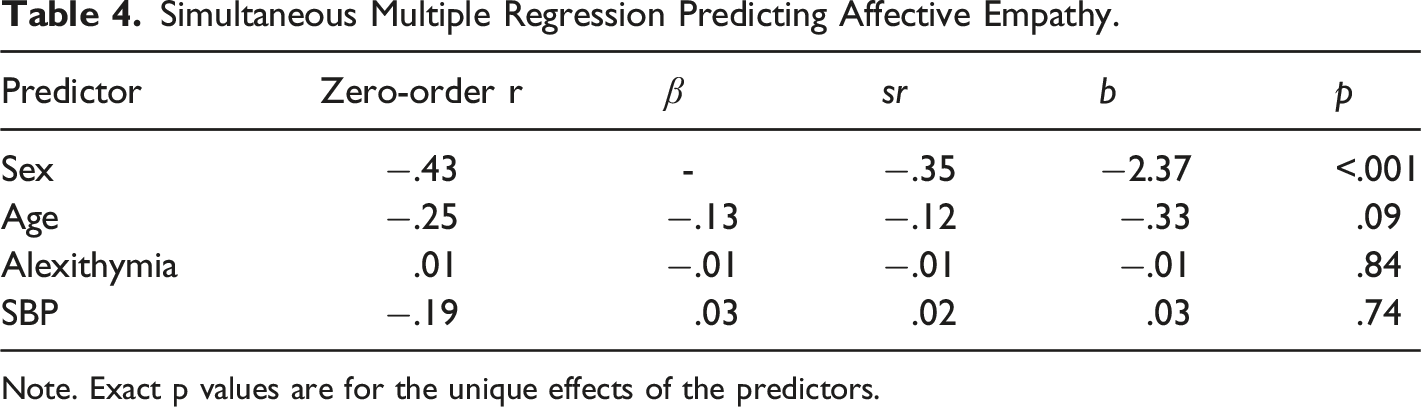
Note. Exact p values are for the unique effects of the predictors.
Simultaneous Multiple Regression Predicting Cognitive Empathy.
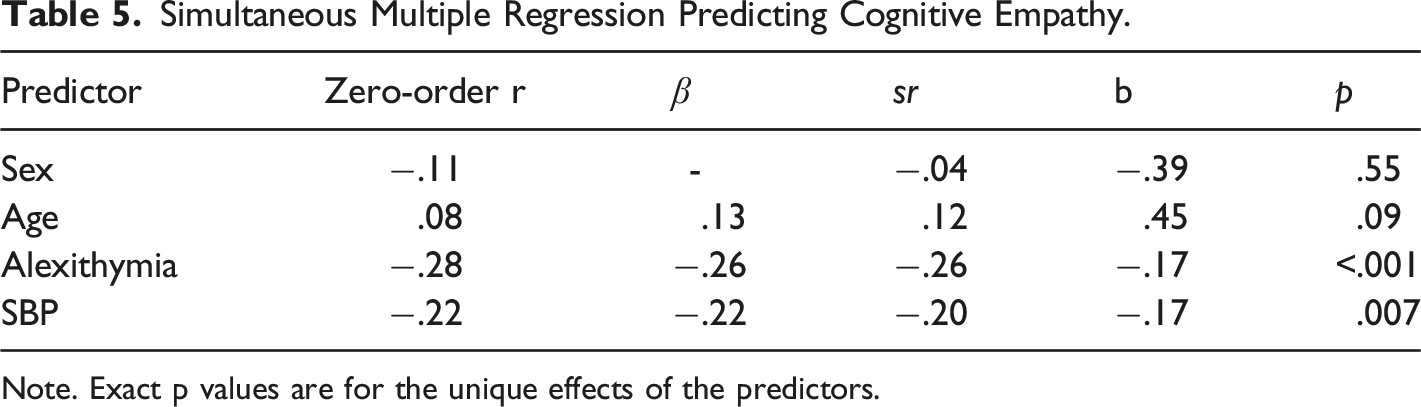
Note. Exact p values are for the unique effects of the predictors.
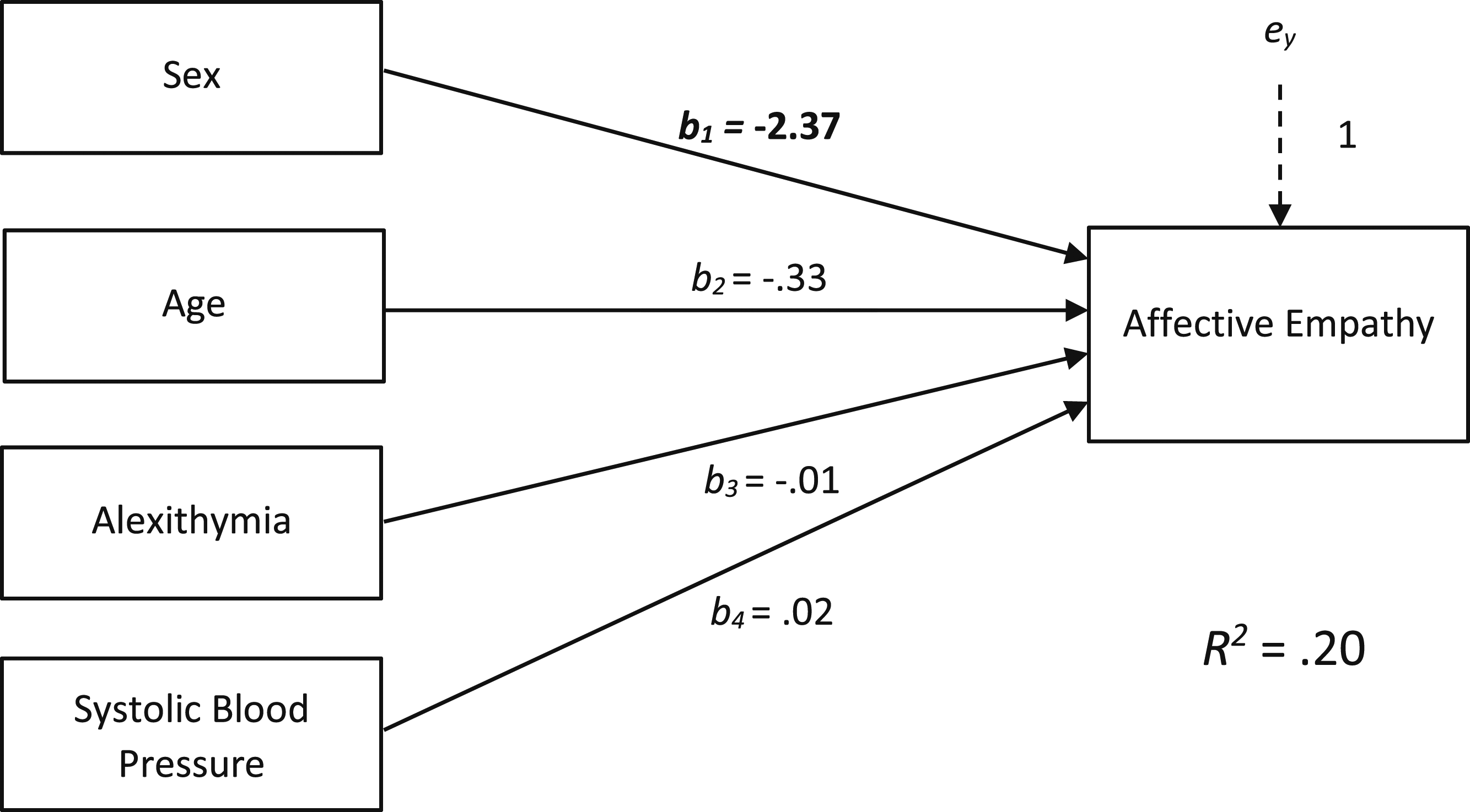
Multiple Regression Predicting Affective Empathy. Note. Bolded Values Denote Significant Independent Relationships.
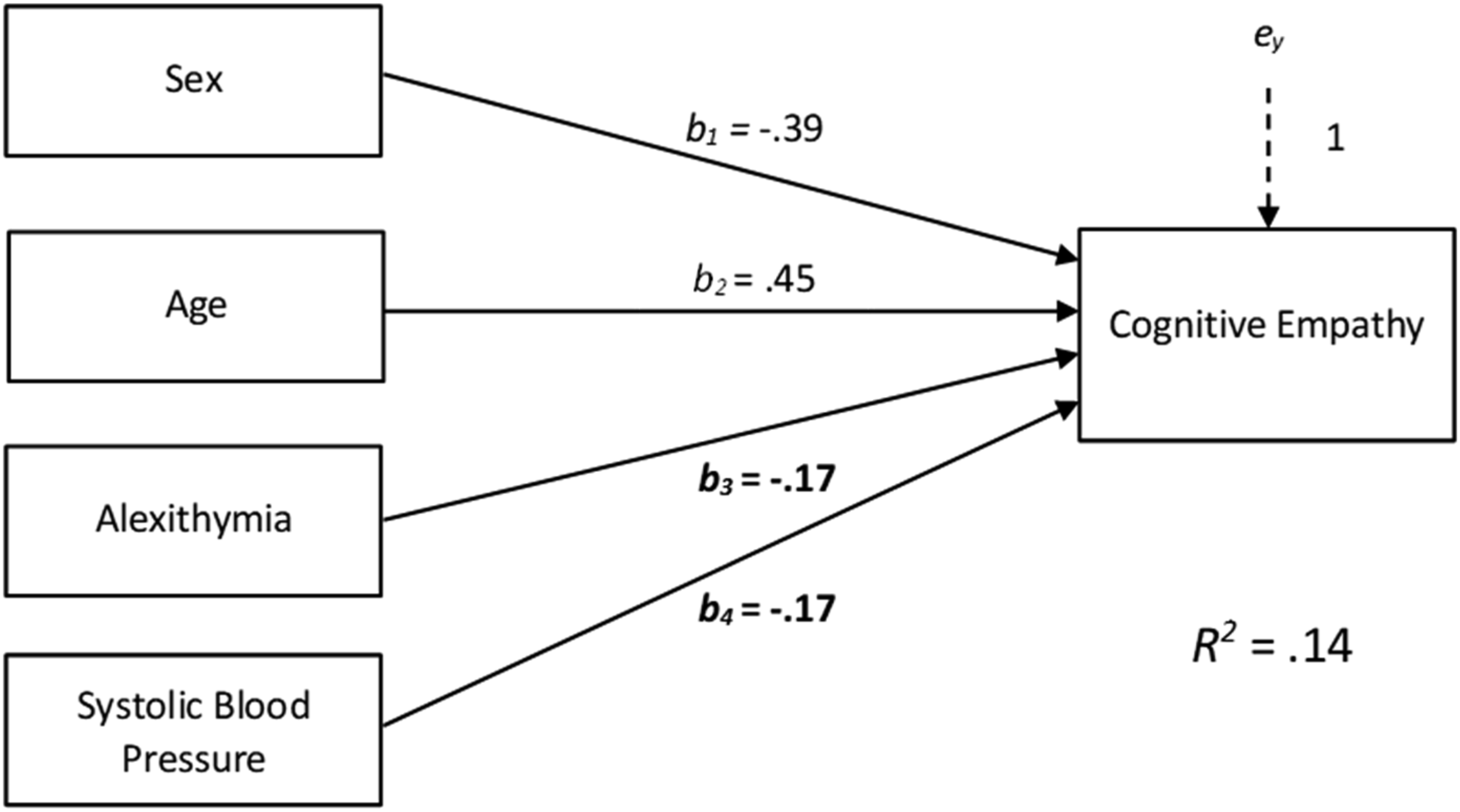
Multiple Regression Predicting Congitive Empathy. Note. Bolded Values Denote Significant Independent Relationships.
Discussion
Given the previously hypothesized link between cardiovascular emotional dampening and relationship quality (McCubbin et al., 2014, 2018, Pury et al., 2004), in the present study we aimed to explore the associations between resting blood pressure and the different dimensions of empathy among a sample of healthy college students. Specifically, we hypothesized that resting blood pressure would be inversely related to measures of trait cognitive empathy and trait affective empathy, and that resting blood pressure would maintain its associations with both measures of trait empathy after controlling for age, sex, and alexithymia. The data did not completely support these hypotheses, as results revealed that while resting systolic blood pressure was inversely related to trait affective empathy and trait cognitive empathy, resting systolic blood pressure ceased to have a significant relationship with trait affective empathy when other covariates were considered. Taken together, the findings provide evidence that the cardiovascular emotional dampening phenomenon may include cognitive but not affective empathy within its constellation of direct associations.
Present Findings as They Relate to the Extant Literature
To the extent that empathy involves the capacity to access simulated forms of emotion processing during interpersonal interactions (Uribe et al., 2019, Yu & Chou, 2018), our findings largely dovetail with those previously reported in the cardiovascular emotional dampening literature. Specifically, in the connection between resting systolic blood pressure and cognitive empathy, there was further evidence that even modest elevations in resting blood pressure seemed to co-occur with appreciable reductions in the ability to engage in explicit top-down processing of emotion-linked information. Investigators in many of the cardiovascular emotional dampening studies which have examined the link between blood pressure and emotion awareness used top-down behavioral tasks featuring long duration presentations of stimuli and/or lengthy allowable response latencies (Loveless et al., 2018, McCubbin et al., 2011, 2014, 2018, Pury et al., 2004, Shukla et al., 2018, 2019). These studies demonstrated that even when given long or sometimes unlimited amounts of time to view or respond to stimuli, participants with elevated resting blood pressures were less accurate at identifying emotions represented within task stimuli (e.g., facial expressions and other-focused written narratives; McCubbin et al., 2014, 2011, 2018, Shukla et al., 2018, 2019) or reported attenuated affective responding to emotionally evocative imagery (Loveless et al., 2018, Pury et al., 2004). Given that many of the aforementioned findings represent some deficit in the top-down recognition and labeling of emotion-related information presented by or involving other people, the cognitive empathy findings associated with the present study are not surprising as a failure to properly identify expressed emotions during an interpersonal encounter would likely interfere with a few of the constituent cognitive processes inherent in cognitive empathy such as perspective taking and empathic accuracy on the part of the observer (Lui et al., 2016).
Our findings related to affective empathy, however, were not consistent with expectations drawn from the extant emotional dampening literature. The few previous studies which have directly explored the relationship between implicit emotion evocation and resting blood pressure demonstrated that increases in resting blood pressure tend to be associated with a decreased susceptibility to affective priming via backward masked visual stimuli as well as a reduced pupillary startle response (Loveless et al., 2018, Shukla et al., 2020). These findings would suggest that increases in resting blood pressure are associated with reduced sensitivity to more bottom-up environmentally mediated emotion evocation. As such, we would expect to observe similar trends related to affective empathy given that it largely encompasses bottom-up emotion evocation that is interpersonally cued (Uribe et al., 2019, Yu & Chou, 2018).
Contrary to our prediction, and despite a significant bivariate relationship between the two variables, we did not observe a significant partial relationship between resting systolic blood pressure and affective empathy when controlling for other covariates. This may be due to the inclusion of participant sex in the model as there were large differences between men and women regarding affective empathy. Thus, the present findings lend support to the notion that women tend to possess higher levels of trait affective empathy relative to men, independent of any variation in such due to resting blood pressure. Although this sex-related finding is similar to findings reported in previous studies (for a review, see Christov-Moore et al., 2014), sex differences found when affective empathy was measured via self-report survey seemed to reflect differences in sex-role response bias rather than actual differences in empathetic responding (Groen et al., 2013). As such, it would be advantageous for future explorations of the potential connection between affective empathy and cardiovascular emotional dampening to feature behavioral measures of affective empathy (e.g., backward masked facial expression paradigms and/or ERP protocols) to accurately examine such.
Implications of a Connection Between Cognitive Empathy and Resting Blood Pressure
The connection between resting blood pressure and cognitive empathy has potential implications for our understanding of how cardiovascular emotional dampening might impact relationship quality. Multiple papers have hypothesized that gradual changes in resting blood pressure likely contribute to interpersonal distress via the associated restrictions in emotion processing (McCubbin et al., 2014, 2018, Pury et al., 2004). Our findings provide support for this broader hypothesis by demonstrating that resting systolic blood pressure covaries with cognitive empathy, a construct that has previously been found useful in the development and maintenance of healthy interpersonal relationships (Fincham et al., 2002, Gungordu et al., 2022, Holt-Lunstad & Uchino, 2019, Paleari et al., 2005, Verhofstadt et al., 2016).
Cognitive empathy reflects an iterative process of understanding that involves multiple subprocesses to include perspective taking (i.e., the ability to take another’s perspective), theory of mind (i.e., the ability to consider that another might have a different perspective to one’s own), and empathetic accuracy (i.e., the ability to accurately detect and identify real-time changes in other’s expressed cognition and affect; Beadle & de la Vega, 2019, Uribe et al., 2019, Yu & Chou, 2018). From the context of the present study, it is unclear if some or all of these processes are implicated in the emotional dampening cascade; however, it is conceivable that perspective taking and empathetic accuracy might be involved given their connection to central nervous system pathways involved in top-down emotion processing (Beadle & de la Vega, 2019; Uribe et al., 2019; Yu & Chou, 2018). Future work should clarify the relationships between resting blood pressure and the constituent components of cognitive empathy to yield a more nuanced appreciation of how cardiovascular emotional dampening is connected to cognitive empathy.
Blood pressure related reductions in cognitive empathy might be a contributing factor to the trends observed in previous relationship quality literature. As previously discussed, the proliferation of ambivalent social relationships (e.g., those which are experienced as highly supportive and aversive) has been linked to heart disease risk, in part, via tonic increases in resting as well as ambulatory blood pressure (Uchino et al., 2001; Holt-Lunstad & Uchino, 2019). Within this literature, changes in blood pressure have been discussed as consequences of ambivalent relationship exposure; however, the emotional dampening cascade would predict that it is both a consequence of ambivalent relationship development and a contributor to yet further ambivalent relationship development. Specifically, blood pressure-related changes in cognitive empathy could contribute to the experience of further ambivalence within relationships via a worsening ability to accurately appreciate the lived experience of one’s dyadic partner(s), especially during stressful moments when such might be critical (i.e., emergencies, fights, etc.). Predictably, this could lead to an increase in inappropriate or ineffective responding for more emotionally dampened individuals, and thus contribute to further turmoil and stress (sic sources of ambivalence) within the dyad. Moreover, these psychophysiological and interpersonal changes could co-occur across time such that what was once considered a largely supportive relationship becomes more ambivalent with time as gradual increases in resting blood pressure among its members reduces the ability for each to understand one another. From the context of the present study, this discussion is somewhat speculative and begs further study; however, the connection between resting blood pressure and cognitive empathy observed herein invites further inquiry to explore and reconcile these related areas of the literature.
Limitations and Future Directions
There are several methodological limitations to the present study that merit consideration. First, this study featured a cross-sectional and non-experimental design. While this was consistent with our aims in this project, this type of design does not permit determining causality between variables of interest (Rutter, 2007). For example, no causal inference can be made related to the associations observed herein between cognitive empathy and resting systolic blood pressure. Association is necessary for causality to exist, and cross-sectional non-experimental research is helpful in establishing that associations between variables seem to naturally occur. To probe questions related to the causality, however, future studies with experimental or quasi-experimental designs will be required (Bleske-Reschek et al., 2015, Rutter, 2007). Within the context of studying phenomena linked to blood pressure and heart disease risk among humans, research ethics governing participant safety would necessarily prohibit any line of experimental research which would cause undue harm. As such, experimental paradigms using animal models, or quasi-experimental paradigms featuring human samples would be appropriate to probe causal effects. Likewise, longitudinal work would also be useful given the hypothesized developmental nature of the cardiovascular emotional dampening cascade (McCubbin et al., 2011, 2014, 2018).
Second, this study was performed with a sample of healthy normotensive college students. The use of healthy normotensive samples in cardiovascular emotional dampening studies has been previously justified with the acknowledgement that the inclusion of participants with chronic cardiovascular, endocrine, or psychiatric illnesses makes it difficult to disentangle whether observed effects are related to more normative psychophysiological processes implicated in the regulation of blood pressure or other pathophysiological changes associated with those conditions (McCubbin et al., 2018). While such a sampling approach is useful in identifying the unique associations that resting blood pressure share with the various psychological or behavioral phenomena which could be theoretically linked to hypertension and heart disease risk among otherwise healthy people, the findings of these studies need to be replicated among more diverse samples to determine the extent to which they generalize to older or sicker populations. From the context of the present study, observing a similar link between cognitive empathy and resting blood pressure among individuals with essential hypertension (or other illnesses) would provide further evidence of the intimacies between the mechanisms which govern blood pressure regulation and higher-order emotion processing, and could potentially offer useful targets for behavioral intervention.
Finally, this study measured aspects of trait empathy via self-report. While widely used in the research literature, self-report measures of empathy are considered to possess a degree of response bias which might interfere with the interpretation of associated findings (Beadle & de la Vega, 2019, Christov-Moore et al., 2014, Groen et al., 2013). Moreover, the extent to which measures of trait empathy capture empathetic responding of respondents during all interpersonal interactions is questionable. There is a rich literature which supports the notion while empathy is a stable trait, the utilization of such can vary as a function of interpersonal and environmental contexts (Cuff et al., 2016, Powell & Roberts, 2017). Beyond these considerations, Loveless et al. (2018) questioned the use of self-report measures of affective phenomena in cardiovascular emotional dampening studies as the accuracy of such could be confounded by participants resting blood pressure. Taken together, future work would likely benefit from the inclusion of behavioral measures of empathetic responding in addition to a self-report measure of such to substantiate and extend the findings observed within this study.
Conclusions
The present study is the first to provide evidence that cognitive empathy is implicated in the cardiovascular emotional dampening phenomenon. Modest elevations in resting systolic blood pressure among healthy and young individuals seem to be associated with a reduced self-reported ability to access top-down processes tied to perspective taking and empathetic accuracy, independent of related covariates. These findings add yet further evidence of cardiovascular emotional dampening as a construct, extend the burgeoning emotional dampening literature by showing that it likely exerts an influence on an aspect of daily living that have not yet been explored in the literature (i.e., interpersonal relationships), and provides a plausible mechanism (i.e., empathy) to reconcile this literature and its findings with the more established relationship quality literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.