
Abstract
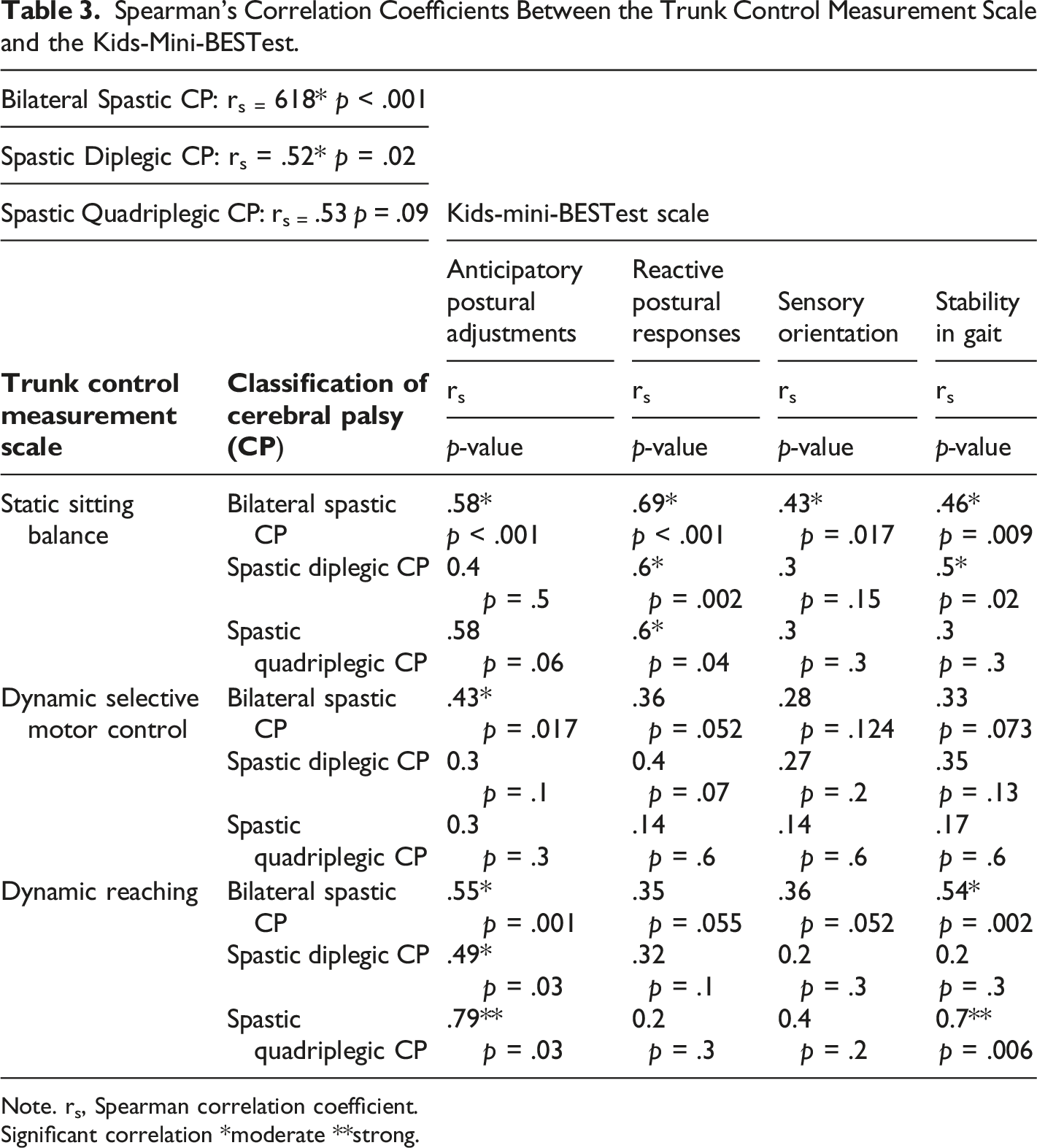
Impairments of postural responses are a salient feature of children with cerebral palsy (CP). While the systems approach describes balance in seven components, the relationship between trunk control and balance in children with CP has not been previously examined with all seven of these components. In this study, we aimed to identify correlations between trunk control and all seven systems approach balance components in children with bilateral spastic CP. Our participants were 30 children (M age = 11.83, SD = 2.32 years) with CP having a Gross Motor Function Classification System level ranging from I to III. We assessed trunk control with the Trunk Control Measurement Scale, including static and dynamic balance (selective voluntary control and reaching). Balance in standing was assessed using Kids-Mini-BESTest involving four domains: anticipatory, reactive, sensory orientation and stability in gait. We used Spearman’s rank correlations to correlate trunk control and balance, and we obtained a moderate correlation between the trunk control measurement scale and the Kids-Mini-BESTest in children with both bilateral spastic CP (rs = .618, p < .001) and spastic diplegic CP (rs = .52, p = .02). Analysis of the correlations between separate domains of the Kids-Mini-BESTest and the trunk control measurement scale subscales revealed moderate correlations between the static sitting balance subscale and all four domains of the Kids-Mini-BESTest. The dynamic selective motor control subscale of the trunk control measurement scale moderately correlated with the anticipatory domain of the Kids-Mini-BESTest. The dynamic reaching subscale also correlated moderately with anticipatory and stability in gait domains. This correlation was statistically significant in the 13 to 17-year-old age group and was strong among females, whereas the correlation was moderate in males. Trunk control was moderately associated with balance considering all the systems theory components of balance in children with bilateral spastic cerebral palsy.
Keywords
Introduction
Cerebral Palsy (CP) is the most common cause of childhood physical disability (Ikeudenta & Rutkofsky, 2020), affecting almost two out of 1000 live births worldwide (Oskoui et al., 2013). Children with CP have sensorimotor deficits such as muscle tone abnormalities, weakness, balance impairments, and sensory disorders (Sadowska et al., 2020; Shim et al., 2022). Children with CP also exhibit impairments in movement and postural control mechanisms because of disturbances in the developing fetal and infant brain (Bax et al., 2005; Rose et al., 2002).
Children with CP have difficulties controlling posture from an early age in static and dynamic situations (Rose et al., 2002). As postural control helps maintain the body’s position in space, it is essential for stabilization and orientation (Shumway-Cook & Woollacott, 2012). Maintaining a stable posture demands complex interactions between the nervous and musculoskeletal systems, which are defined in detail by the systems approach to understanding balance (Shumway-Cook & Woollacott, 2012). The systems approach provides a theoretical basis for designing and evaluating interventions. It comprises seven components: the musculoskeletal system, sensory system, sensory strategies, anticipatory mechanisms, adaptive mechanisms, neuromuscular synergies, and internal representations (Shumway-Cook & Woollacott, 2012).
Balance is affected in children with CP because of impaired muscle strength, limited joint range of motion, muscle spasticity, poor ankle, hip and stepping strategies and poor postural feedback reactions (Dewar et al., 2017a; Kiefer et al., 2021; Rose et al., 2002). In children with CP, a descending (rather than ascending) recruitment pattern of lower limb muscles is seen in standing (Levitt & Addison, 2019). These atypical muscle recruitment patterns are associated with agonist and antagonistic co-contractions, variability in muscle responses, prolonged activation latencies, and poor adaptation to the intensity of external perturbation, all of which contribute to impaired postural control mechanisms (Van Balen et al., 2012).
Children with spastic CP have difficulty with trunk control, particularly in the frontal and transverse planes (Heyrman et al., 2013). Trunk control plays a part in organizing postural control and balance responses as it maintains the center of gravity (Liao et al., 2003). Optimal trunk control is necessary for tasks such as sitting and reaching, wherein the trunk acts as a stabilizing unit (Kallem Seyyar et al., 2019). Trunk control is also responsible for the proper functioning of the upper and lower limbs (Yildiz et al., 2018), which helps perform activities of daily living (Curtis et al., 2015; Kallem Seyyar et al., 2019). Trunk control can be influenced by impaired trunk position sense (Monica et al., 2021), axial segments, and gait (Balzer et al., 2018; Pierret et al., 2021).
Trunk control is assessed by the Trunk Control Measurement Scale (TCMS) in children with CP, which examines trunk control in static and dynamic conditions (Heyrman et al., 2011). While balance is generally assessed by the Pediatric Balance Scale (PBS), the PBS only assesses three systems approach components: anticipatory mechanisms, sensory systems, and internal representations. As all seven components of the systems approach are essential, a comprehensive system-based assessment known as the Kids-Mini-BESTest scale was developed from the Mini-BESTest, commonly used to assess balance in adults (Dewar et al., 2017b). The Kids-Mini-BESTest assesses static and dynamic standing balance and timed-up and go skills with dual tasking (Dewar et al., 2017b, 2019).
Motor deficits in children with CP, mainly associated with balance and trunk control, significantly affect functioning and, consequently, quality of life. Establishing the relationship between trunk control and balance can help with a thorough understanding of the impairments associated with CP and help develop effective treatment plans. Current knowledge of the relationship between trunk control and balance in children with CP is limited. A previous study correlated only three components of the systems approach to balance: anticipatory mechanisms, sensory systems, and internal representations of trunk control and found a strong correlation (Panibatla et al., 2017). However, an examination of performance across all seven components is required for optimal balance assessment. Thus, we used all systems approach components as contained within the Kids-Mini-BESTest. We hoped that this method would yield a comprehensive understanding of how trunk control impacts various components of balance and provide direction for developing more effective and targeted interventions for improving balance and trunk control in children with CP.
Method
Participants
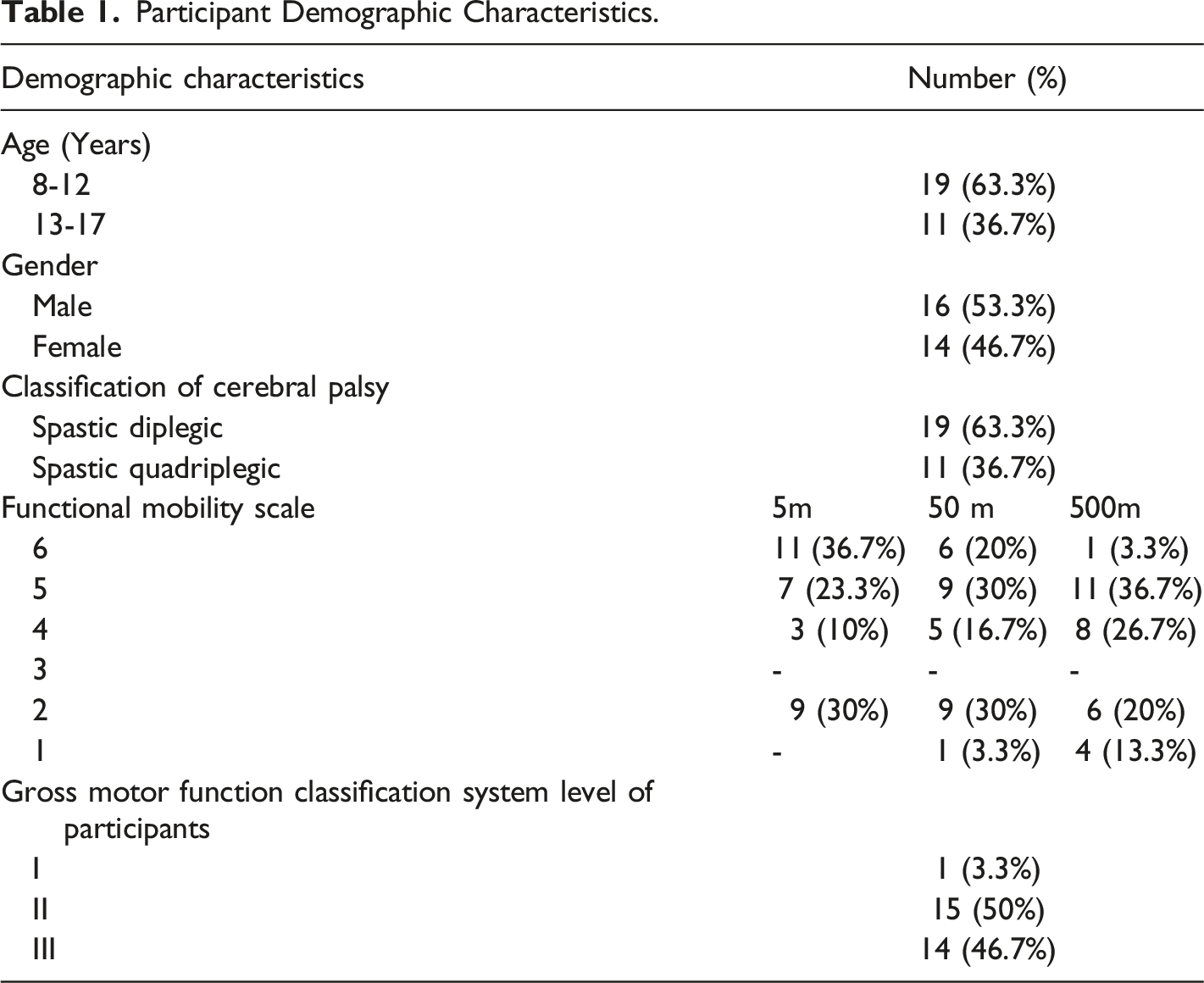
This cross-sectional study was conducted between August 2022 and April 2023 at special schools in Bengaluru, India. To be included in the study, children with CP met the following inclusion criteria: (a) be between the ages of 8 and 17 years, (b) be diagnosed as level I, II or III according to the Gross Motor Function Classification System (GMFCS) and have bilateral spastic CP, and (c) be able to understand and follow commands. Children with a history of spasticity management (such as BOTOX) or orthopedic surgery (lower limb surgeries such as lateral lengthening) in the last three months or any behavioral difficulties limiting their full participation in the assessment were excluded from the study.
The study complied with the tenets of the Declaration of Helsinki and was approved by the Institutional Research Committee of Manipal College of Health Professionals (MCHP), and permission from the concerned authorities of the special schools was obtained. Written consent and assent were obtained from parents and children, respectively, before participation in the study.
Measures
The Trunk Control Measurement Scale (TCMS) was used to assess the trunk control of children with CP (Heyrman et al., 2013). The TCMS consists of fifteen items divided into two subscales of static sitting balance and dynamic sitting balance - further divided into selective movement control and dynamic reaching. All items on this scale are scored on a two-, three-, or four-point ordinal scale. The total score of the TCMS ranges from zero to 58, with a higher score indicating better performance. The scale has acceptable inter-rater and intra-rater reliability (interclass correlation coefficients = 0:91 – 0:99; kappa = 0:45 – 1; Cronbach’s alpha coefficients = 0:82 – 0:94) and good validity in children with CP (Heyrman et al., 2013).
To assess balance, we used the Kids-mini-BESTest, which contains 14 items divided into four domains: anticipatory postural adjustments, reactive postural responses, sensory orientation, and stability in gait. The scores range from two (best performance) to zero (worst performance), with a total score of 28 points. The scale has excellent reliability (interclass correlation coefficients ranging from .79–.98) in assessing balance in children with CP (Dewar et al., 2019).
Procedure
A qualified physiotherapist was guided and trained to administer both outcome measures in a single session. Demographic data such as name, age, gender, and any use of assistive devices along with GMFCS level were collected from all participants. The Functional Mobility Scale (FMS) was used, which consisted of six levels that assessed the use of mobility aids by the child to travel 5, 50 and 500-m distances. For assessing trunk control, children were seated on a bench or chair without support for the back, arms, or feet and without orthoses, shoes, or trunk brace. A maximum of three repetitions were performed, and the best score was used for further analyses. While assessing balance, if the child used any assistive devices (walker, crutches, or rollator), the scores for that task were reduced by one. The total assessment was completed in 35 minutes, wherein the TCMS took 15 minutes, and the Kids-Mini-BESTest took 10 minutes, with a 10-min break between the two tests to avoid participant fatigue.
Statistical Analysis
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS, version 29.0). We used median and interquartile ranges to represent the ordinal data descriptively. We used the non-parametric Spearman’s rank correlation test to estimate the correlation between trunk control and balance. Correlation analyses were also conducted within each subgroup, categorizing the participants by age, gender, GMFCS level and classification of CP. A p-value <.05 was considered statistically significant, with the correlation coefficients interpreted as .00–.10: negligible correlation; .10–.39: low correlation; .40–.69: moderate correlation; .70–.89: strong correlation and .90–1.00: very strong correlation (Schober & Schwarte, 2018).
Result
Participant Demographic Characteristics.
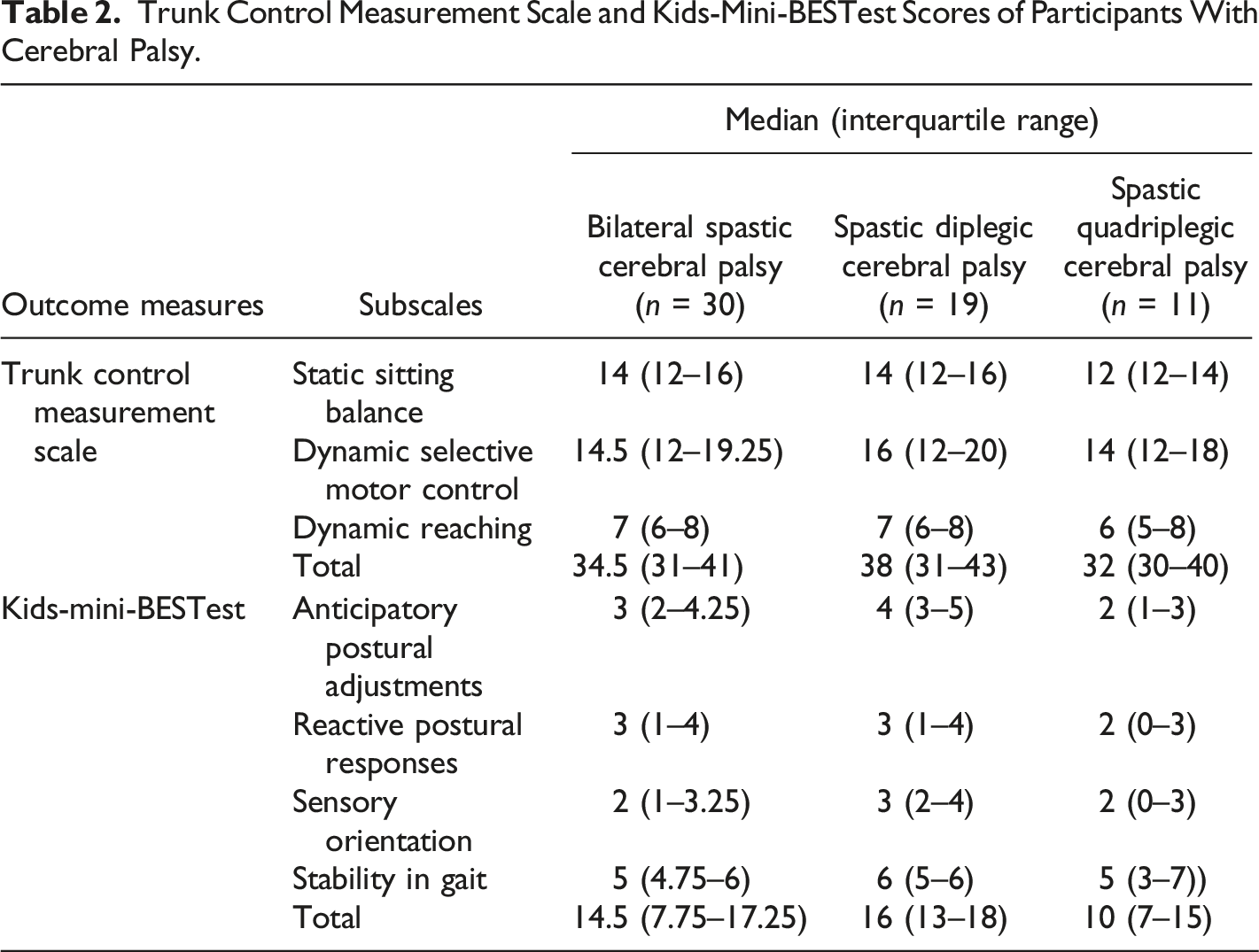
Trunk Control Measurement Scale and Kids-Mini-BESTest Scores of Participants With Cerebral Palsy.
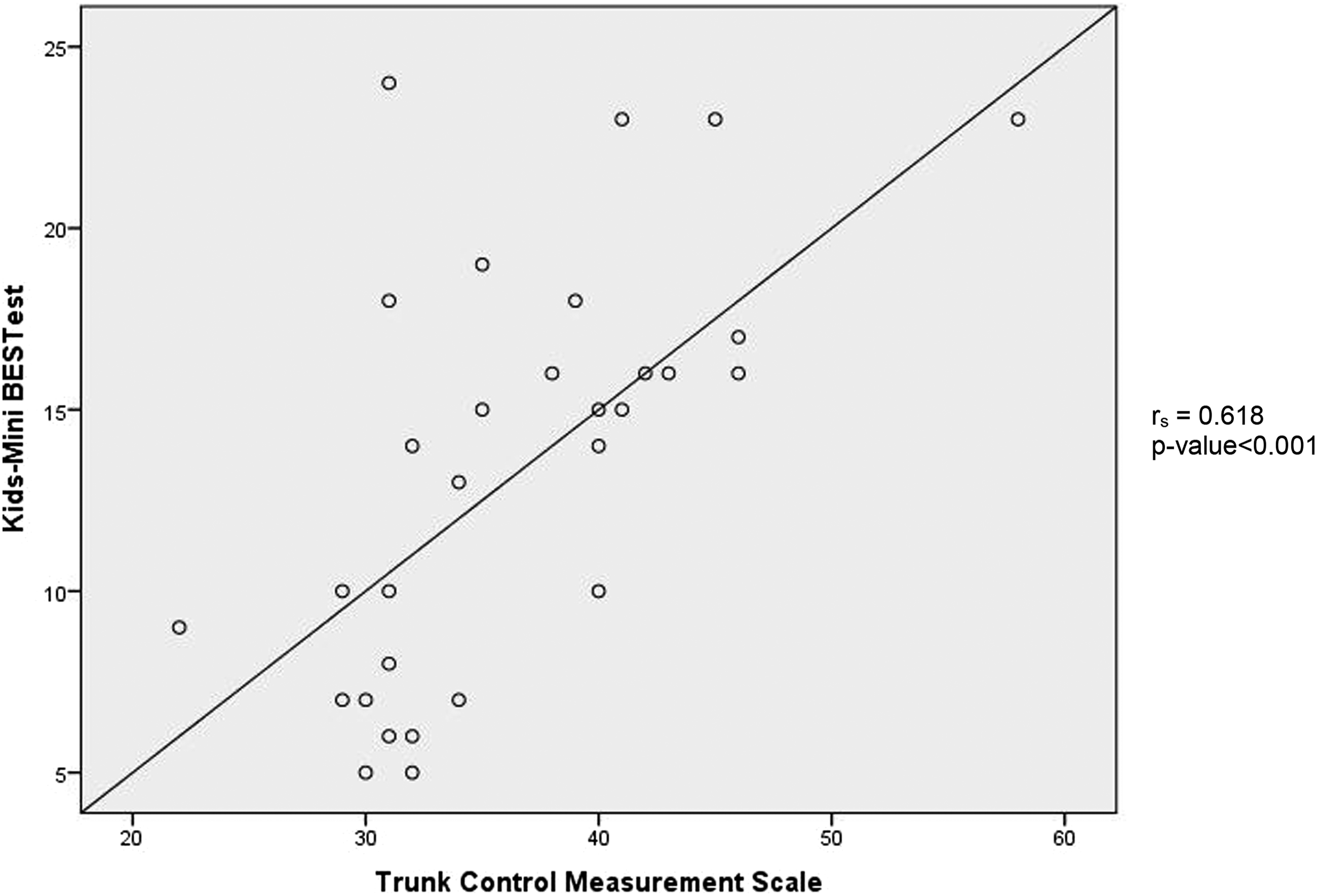
Scatter Plot Showing the Correlations between the Trunk Control Measurement Scale and Kids-Mini-BESTest scores.
Spearman’s Correlation Coefficients Between the Trunk Control Measurement Scale and the Kids-Mini-BESTest.
Note. rs, Spearman correlation coefficient.
Significant correlation *moderate **strong.
Correlation Analyses Between the Trunk Control Measurement Scale and the Kids-Mini-BESTest Scores Based on Participant Characteristics.
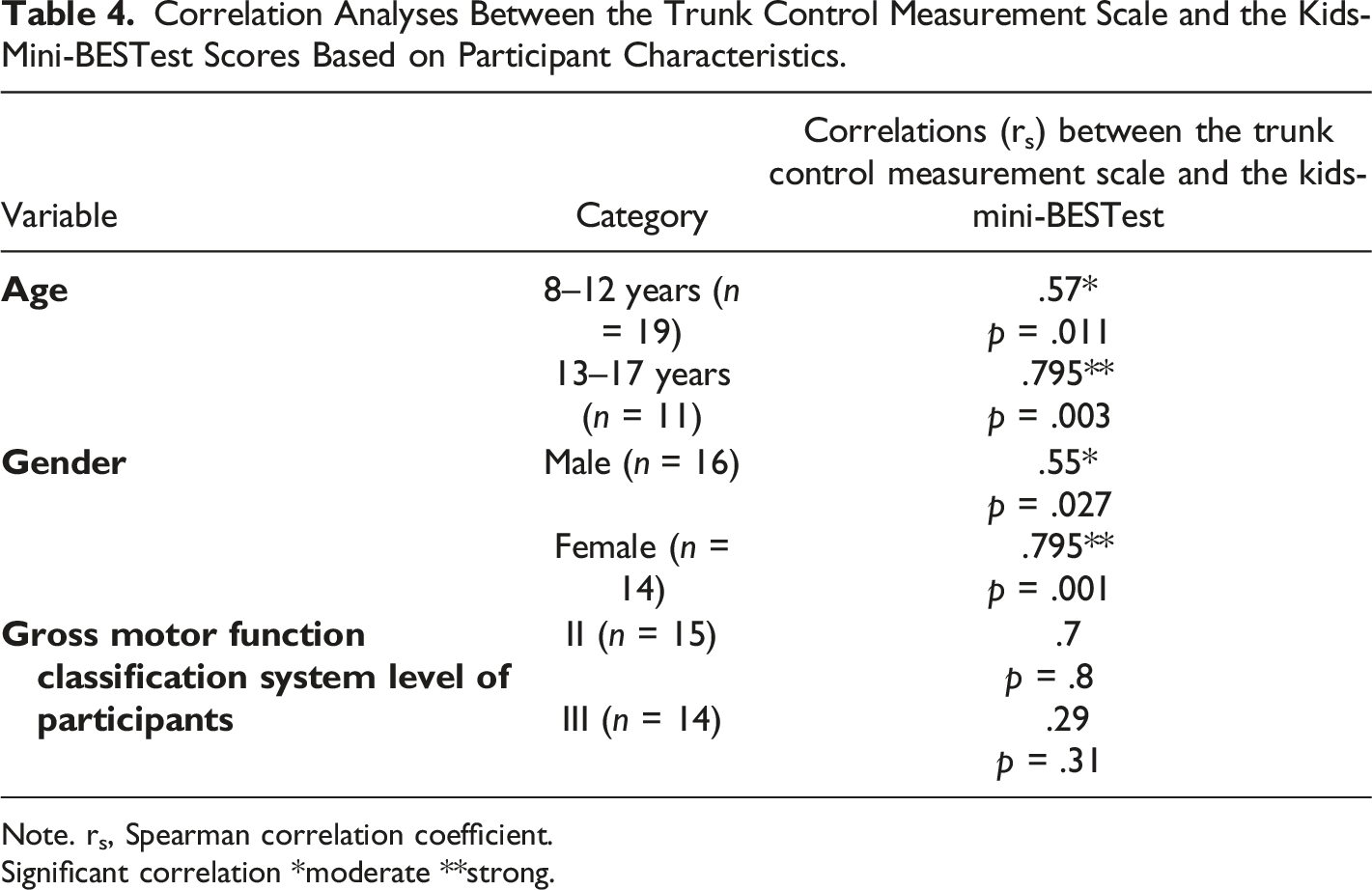
Note. rs, Spearman correlation coefficient.
Significant correlation *moderate **strong.
Discussion
In this study, we examined the relationship between trunk control and balance using the Trunk Control Measurement Scale (TCMS) and the Kids-Mini-BESTest in children with bilateral spastic CP. Our data demonstrated that trunk control and balance are significantly and moderately correlated. The static sitting component of the TCMS significantly and strongly correlated with the reactive domain of the Kids-Mini-BESTest. We also reported significantly strong correlations between trunk control and balance in females and across the 13 to 17-year-old age group.
We found that trunk control was moderately associated with balance in children with bilateral spastic CP. These findings are consistent with a previous study using a pediatric balance scale and TCMS (Panibatla et al., 2017). Our findings suggest that the trunk should be targeted when rehabilitation therapists aim to improve such aspects of balance as the ability to move from sitting to standing, standing on toes, standing on one leg, walking over obstacles and dual-tasking while walking. Our correlational analyses with children with spastic diplegics showed moderate correlations between trunk control and balance. Trunk control in spastic diplegics was associated with active lower limb movements, perhaps suggesting that truck control may be the basis for impaired balance in standing (Heyrman et al., 2013).
The low scores we obtained for participants’ trunk control and balance (Table 2) were consistent with reports from previous studies of children with spastic CP (Balzer et al., 2018; Gunes et al., 2022; Heyrman et al., 2013). Children with spastic diplegic CP had better trunk control and balance than did children with quadriplegic CP. Children with spastic quadriplegic have been show to have weak sitting abilities owing to trunk and distal segment (upper and lower limb) weakness), impaired axial segments, and limited range of motion (Heyrman et al., 2013; Pierret et al., 2021). Because of deficits in trunk position sense and segmental trunk control, static and dynamic trunk control can be low in children with CP (Monica et al., 2021; Pierret et al., 2021). There is a consensus in the literature that trunk control impairments in static and dynamic aspects of balance are commonly seen in children with CP, and these problems may influence standing and gait anomalies (Balzer et al., 2018).
The domains of the Kids-Mini-BESTest are anticipatory postural adjustments, reactive postural responses, sensory orientation, and stability in gait, which were also correlated with trunk control in our analyses (Dewar et al., 2017b). The anticipatory postural adjustments domain assesses the activation of postural responses before voluntary muscle contraction is needed to maintain balance (Shumway-Cook & Woollacott, 2012). The anticipatory domain includes sit-to-stand and static standing balance tasks, which were moderately correlated with trunk control in our participants. This observation can be attributed to disorganized muscle recruitment in postural responses, which could impair the anticipatory balance in children with CP (Van Balen et al., 2012). These findings were consistent with previous studies, which found a significant relation between trunk control with sit-to-stand tasks and the anticipatory domain of the pediatric balance scale (Gunes et al., 2022). Furthermore, the increased displacement of the center of pressure in static sitting and standing in children with CP (impaired balance) may have further decreased scores on the TCMS (Gunes et al., 2022; Shim et al., 2022).
The reactive postural responses domain includes muscle contraction in reaction to an external perturbation. Children with CP take longer to stabilize and recover from any external force exerted, such as a gentle push (Pavão et al., 2013). The reactive postural responses domain was moderately correlated to static sitting balance among our participants, which implies that a child with a better static sitting balance will have a better reactive response. The center of gravity sway velocity in static sitting is an indicator of dynamic balance in standing, which may have influenced the relationship between trunk control and reactive balance (Gunes et al., 2022; Shim et al., 2022). However, the present findings were in contrast with a posturography assessment study that concluded that reaction to perturbation in standing was related to displacement in dynamic but not static sitting (Shim et al., 2022).
The third domain of the Kids-Mini-BESTest is sensory orientation, which assesses somatosensory, visual and proprioception feedback necessary to maintain balance, which is also impaired in children with CP. In our study, we found the static sitting domain of TCMS to be moderately correlated with sensory orientation, consistent with Pierret et al. (2021), who observed that diminished sensory feedback increased the demand to maintain balance, attributable to increased demand on axial segments, which are already compromised in children with CP. This may explain the association between static sitting balance and sensory orientation, which is essential to maintain balance.
Assessing gait stability comprehensively assesses all components of the systems approach as gait requires both dynamic standing balance and timed up and go skills (Dewar et al., 2017b). This domain was moderately correlated with static sitting and dynamic reaching in sitting, which means that when the trunk is stable, it can facilitate optimal efficiency in distal (lower limb) functioning. These outcomes also agreed with other findings on the association between trunk control and gait (Balzer et al., 2018).
The correlations we obtained can be due to the anatomical and physiological causes and impairments present in children with CP. Brain damage in the fetal and infant brain in children with CP results in the disconnection of descending inhibitory and excitatory signals, causing deficits in the development of neurological mechanisms of postural control, balance, and movement, which are disorganized and delayed. Loss of descending excitatory input may also cause diminished muscle growth and weakness, affecting selective motor control and balance, as we observed (Yun et al., 2023; Zhou et al., 2017).
We also observed a correlation between the total scores on the TCMS and Kids-Mini-BESTest for participant subgroups of age, gender, and GMFCS levels. Among the 13–17-year-old age groups, there was a stronger correlation between trunk control and balance, which could be because adolescents have better developed balance responses when compared to younger children (Micarelli et al., 2020). Within gender, females had a strong correlation, consistent with Panibatla et al. (2017) and attributable to females’ biomechanical and hormonal factors. There was no significant correlation between these variables among children at GMFCS levels II and III, possibly due to uneven sample sizes among the subgroups.
Limitations and Directions for Further Research
Our study had limitations that should be noted. First, as this was a correlational study, we cannot make definitive inferences regarding the causal directions of effects between these variables. Second, we did not include equal numbers of participants from GMFCS levels I, II and III. Third, we used the shorter version of Kids BESTest instead of the full version. Despite these limitations, the study’s strengths included that it is the first to consider all system theory components of balance with reliable outcome measures, and it demonstrated correlations between these components and trunk control in children with bilateral spastic CP. Improved future studies might include larger sample sizes using the Kids BESTest scale and different types of CP. Longitudinal research that follows children over time would help determine a suspected causal relationship between trunk control and balance.
Conclusion
Trunk control and balance were moderately correlated in children with bilateral spastic cerebral palsy. In the 13–17-year-old age group and among females, we found this correlation to be statistically significant. Our assessments showed that trunk control and balance were affected in all domains of the Kids-Mini-BESTest in children with bilateral spastic CP. These findings imply that trunk control is clearly related to and may influence balance in terms of all the components of the systems approach. The practical implications of these findings for various professionals involved in caring for children with bilateral spastic CP include that tailored interventions addressing both trunk control and balance are needed and should specifically address all the components of the systems approach to improve gait and, eventually, the quality of life. Future researchers may delve into a deeper understanding of the contribution of each component of the systems approach on overall balance and develop targeted interventions accordingly. In essence, our study provides valuable insights that contribute to balance and trunk control research in children with CP.
Footnotes
Author’s Note
The study complied with the tenets of the Declaration of Helsinki and was approved by the Institutional Research Committee of Manipal College of Health Professionals (MCHP), and permission from the concerned authorities of the special schools was obtained. Written consent and assent were obtained from parents and children, respectively.
Acknowledgments
The authors thank all the children and their parents from special schools who participated in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.