
Abstract
Our purpose in this study was to determine the effects of a virtual reality intervention delivering specific motivational motor learning manipulations of either autonomy support (AS) or enhanced expectancies (EE) on frontal plane single-leg squatting kinematics. We allocated 45 participants (21 male, 24 female) demonstrating knee, hip, and trunk frontal plane mechanics associated with elevated anterior cruciate ligament injury risk to one of three groups (control, AS, or EE). Participants mimicked an avatar performing five sets of eight repetitions of exemplary single-leg squats. AS participants were given the added option of choosing the color of their avatar. EE participants received real-time biofeedback in the form of green highlights on the avatar that remained on as long as the participant maintained pre-determined ‘safe’ frontal plane mechanics. We measured peak frontal plane knee, hip, and trunk angles before (baseline) and immediately following (post) the intervention. The control group demonstrated greater increases in knee abduction angle (Δ = +2.3°) than did the AS (Δ = +0.1°) and EE groups (Δ = −0.4°) (p = .003; η2p = .28). All groups demonstrated increased peak hip adduction (p = .01, ηp2 = .18) (control Δ = +1.5°; AS Δ = +3.2°; EE Δ = +0.7°). Hip adduction worsened in all groups. AS and EE motivation strategies appeared to mitigate maladaptive frontal plane knee mechanics.
Introduction
Despite efforts over the previous two decades to decrease the incidence and impact of anterior cruciate ligament (ACL) injuries in athletes, challenges remain. Recurrent injuries to the contralateral or ipsilateral limb are reported to be as high as 33% among adolescent athletes (Webster et al., 2021; Wiggins et al., 2016). Even when a second ACL injury is avoided, 35% of athletes with a primary ACL injury do not return to play at the same level (Walden et al., 2016). More alarming, poor function one year after primary ACL reconstruction increases the risk of early onset osteoarthritis by over 200% (Odds Ratio = 3.66) (Patterson et al., 2020). Because of the heavy economic, psychological, and physical burdens associated with primary and secondary ACL injury, a need remains for advanced injury mitigation strategies that can be broadly implemented.
Multiple reasons have been postulated for the poor long term outcomes associated with ACL reconstruction, and among them are traditional injury prevention programs that focus on enhancing peripheral neuromuscular control but fail to replicate the sensorimotor demands of real-time sport participation (DiCesare et al., 2019c). Specifically, there is a need to consider those sensorimotor-related processes that are critical for both maintaining safe knee position and ensuring the retention and transfer of learned injury-resistant biomechanics from the lab and clinic to a sport setting (Diekfuss et al., 2020a; Diekfuss et al., 2021; Diekfuss et al., 2020b; Diekfuss et al., 2019a; Grooms, 2022). The emergence of real-time biofeedback technologies provides an opportunity to capitalize on sensorimotor capacity for adaptation and, thus, fully integrate perceptual and motor factors that can support injury-resistant movement behaviors. Real-time biofeedback is capable of modifying peripheral movement patterns via visual, vestibular, and proprioceptive inputs, which may simultaneously enhance functioning for the successful transfer of acquired movement strategies to the sporting environment (e.g., ‘neural efficiency’ to support injury resistant knee motor control) (Diekfuss et al., 2020b; Grooms, 2022).
Motor learning techniques show promise for cognitively engaging learners during movement-focused interventions. Specifically, the Optimizing Performance through Intrinsic Motivation and Attention for Learning, or OPTIMAL, theory (Wulf & Lewthwaite, 2016) is a key theoretical motor learning framework that has been extended and modified to optimize current injury
The potential beneficial effects of AS on motor performance and learning have been inconsistent, particularly for paradigms that aim to promote self-control via a task-irrelevant choice or manipulation (McKay et al., 2022). However, an overwhelming majority of studies that failed to replicate AS effects were focused on discrete tasks with obvious goal-oriented outcomes (e.g., whether a dart hit a bullseye), potentially masking an AS influence on more granular mechanistic processes of motor behavior (e.g., the movement mechanics of a dart throw).
Therefore, our purpose in this study was to determine the relative efficacy of two motivational-based, single-leg squatting interventions to improve frontal plane mechanics in individuals exhibiting poor frontal plane knee, hip, and trunk mechanics compared with an attentional-based intervention. Because an external focus of attention (with and without additive visual biofeedback) has established efficacy, we focused on the unique effects of autonomy support (AS) and enhanced expectancies (EE) for developing injury resistant movement. Compared to participants who trained with a standard virtual stimulus, we hypothesized that those who trained with a stimulus incorporating either an EE or an AS feature would display improved frontal plane single-leg squatting kinematics following a brief intervention. Our secondary, exploratory, purpose in this study was to determine potential sex-specific responses to these motor learning manipulations.
Method
Ethical Considerations
We obtained advanced approval for this research protocol from our university’s Institutional Review Board (IRB) before involving any participants in this research. All participants provided written informed consent, approved by the university’s IRB before participating.
Participants
Participant Demographic Characteristics With Mean Values (and 95% Confidence Intervals).
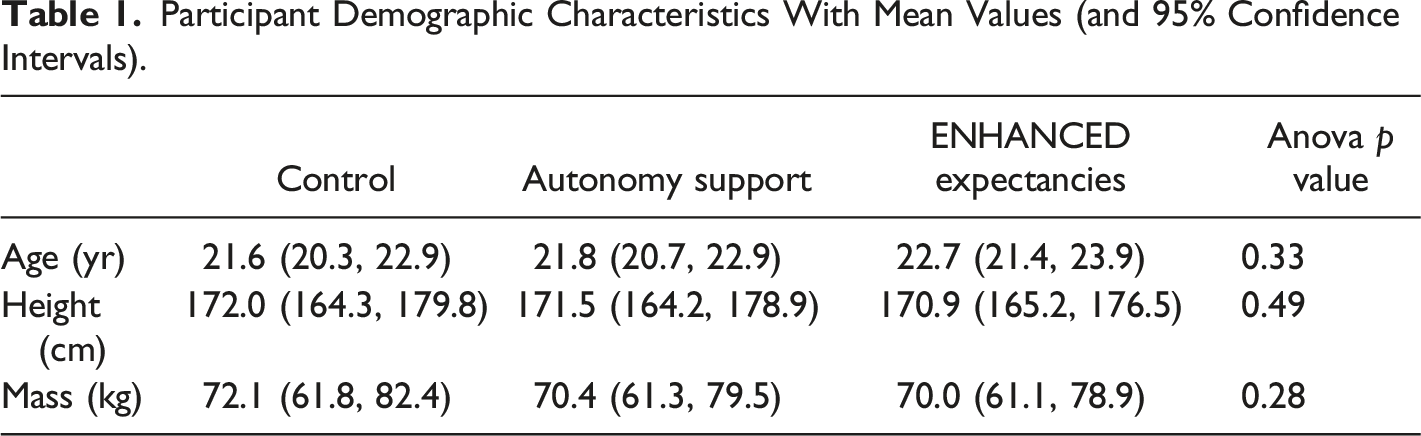
To determine eligibility and confirm the presence of high-risk frontal plane biomechanics, we assessed participants’ frontal plane angles of medial knee displacement, contralateral pelvic drop, and lateral trunk lean at the point of maximum knee flexion prior to the intervention and assessed with ImageJ software (Rasband, 2018). Risky frontal plane mechanics were operationally defined as exhibiting at least two of the following: medial knee displacement >10° for males or >13° for females (Cronström, Creaby, Nae, Ageberg, et al., 2016aCronström, Creaby, Nae, & Ageberg, 2016), contralateral pelvic tilt > 5°, and ipsilateral trunk lean > 5°. We assigned participants to one of three groups (control, autonomy support [AS], or enhanced expectancies [EE]) in a quasi-random fashion (to ensure that there were 8 females and 7 males in each group).
Instrumentation
We affixed retro-reflective adhesive markers to the following anatomical landmarks bilaterally: C7 vertebrae, T10 vertebrae, manubrium, sternum, iliac crest, acromion process, greater trochanter, medial and lateral femoral condyles, medial and lateral malleoli, posterior and medial and lateral heel, 5th metatarsal head, 1st metatarsal head, and great toe. In addition, we affixed five tracking plates, each containing four retroreflective markers, on the participants’ left and right lateral thighs, left and right shanks, and the sacrum. Participants’ movements were digitized using Vicon Nexus software (Vicon, Oxford Metrics, UK, https://www.vicon.com/software/nexus/). Ankle and knee joint centers were defined as the midway point between the medial and lateral malleoli and medial and lateral femoral condyles, respectively. Hip joint centers were determined using the Bell method (Bell et al., 1989). Data were obtained with an 8-camera Vicon motion capture system sampling at 100 Hz.
The instrumentation we used for kinematic biofeedback delivery has been reported in detail elsewhere (Hogg et al., 2022; Williams et al., 2022). Briefly, kinematic data for biofeedback delivery were collected using the Microsoft Azure Kinect DK (https://azure.microsoft.com/en-us/services/kinect-dk/). Through Kinect DK, we obtained joints’ transient position and corresponding Quaternion rotation (denoted as
Motor Learning Assessment Procedures
Motor learning is broadly defined by relatively permanent gains in the capability for skilled performance via processes associated with practice or experience (Schmidt & Lee, 2013)
Intervention Procedures
We employed a one-day intervention consisting of single leg squats while participants viewed a digital avatar displayed in real-time through a virtual reality headset (Hogg et al., 2022; Williams et al., 2022). The same investigator delivered all interventions in a standardized manner but could not be made unaware of the participant’s allocation to an experimental group and so was not tasked with data reduction or analysis. For the intervention, each participant completed five sets of eight single-leg squats on the left leg with self-selected rest periods between each set. Single-leg squatting is an appropriate task during which to deliver real-time biofeedback. We chose the single leg squat task as this slow, continuous movement allows for real-time biofeedback to be successfully delivered and provides participants time to immediately correct their movement prior to their next repetition (Bonnette et al., 2019). During the single-leg squats participants wore a VR headset (HTC Vive Pro, New Taipei City, Taiwan) that displayed a posterior view of a squatting avatar demonstrating exemplar frontal plane knee, hip, and trunk mechanics. All participants were told that the avatar exemplified proper squatting mechanics and were simply instructed to mimic the avatar as closely as possible. Using minimal instructions, we aimed to isolate the effects of the motor learning manipulations.
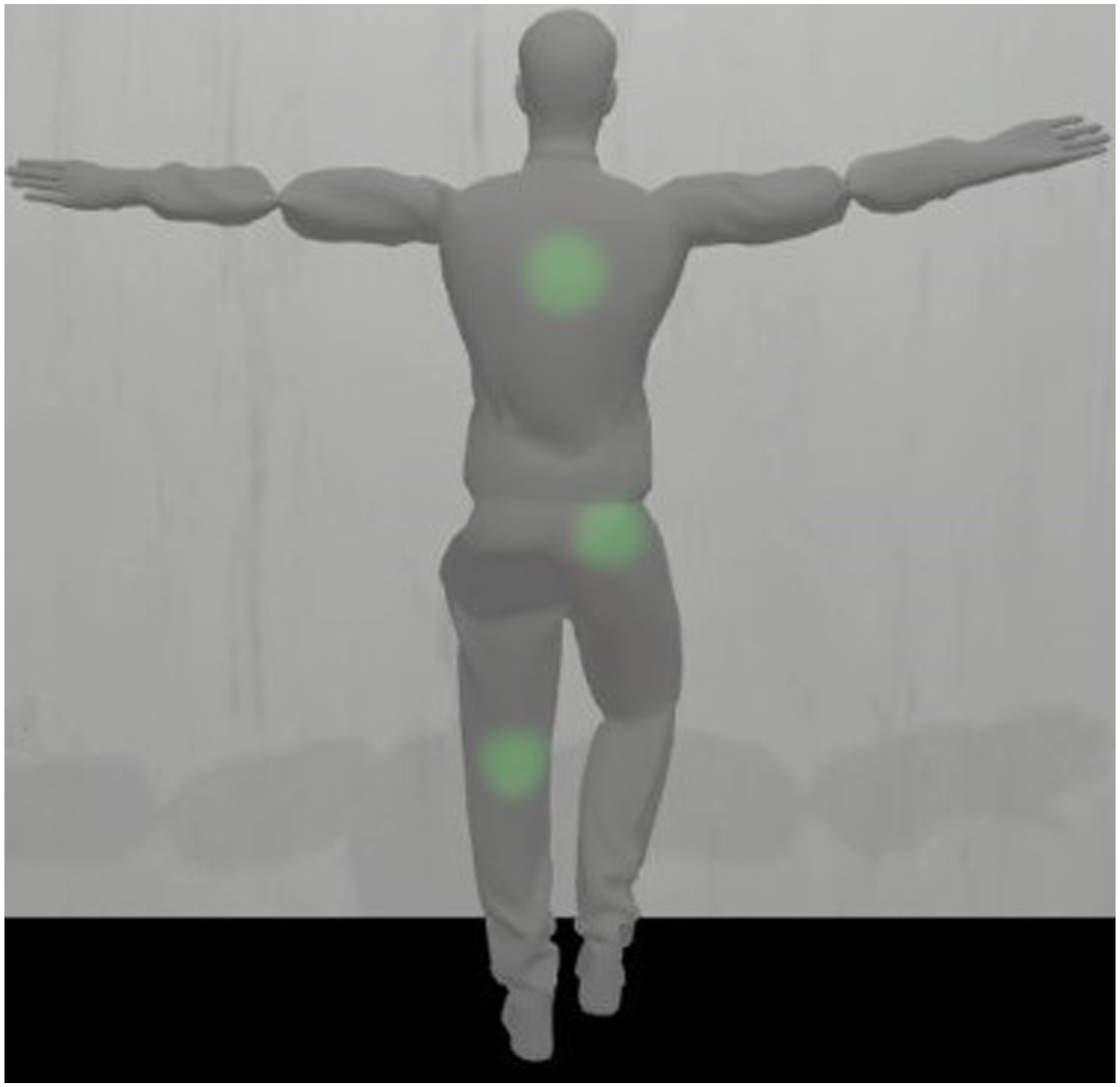
The control group received no other feedback or autonomy. The AS group was allowed to choose the color of their avatar for each set but did not receive feedback (Figure 1). The EE group received real-time biofeedback in the form of green highlights placed on the avatar’s left knee, right buttock, and middle of the back. The highlights remained on as long as the participant did not exceed predetermined knee valgus, pelvic drop, or trunk lean thresholds. Participants in the EE group were instructed to move in such a way as to retain the green lights on the avatar but were given no explicit feedback on how to accomplish this (Figure 2) (Williams et al., 2022). Representation of the Avatar with Examples of Color Choice Options Seen by Participants in the Autonomy Support Group. Representation of the Avatar with Positive Feedback (Green Highlights) as seen by Participants in the Enhanced Expectancies Group.
Data Processing
We collected data from single-leg squatting trials serially in a single data capture period. Trials were separated at the point of maximum knee extension. Following interpolation of gaps up to 30 milliseconds, kinematic data were filtered with a 10 Hz, low-pass, 4th order, zero-lag Butterworth filter. We calculated joint rotations with the following rotation sequence: (a) flexion-extension about the x-axis, (b) adduction-abduction about the y-axis, and (c) internal-external rotation about the z-axis. Peak joint angles occurring between the point of maximum knee extension and maximum knee flexion were extracted. All flexions, adductions, and internal rotations were defined as positive angles. All extensions, abductions, and external rotations were defined as negative angles. Trials were averaged within participants for analysis. Data processing was conducted in Visual3D (C-Motion, Rockville, MD, USA).
Statistical Analysis
We assessed data normality with histograms and used Levene’s test to determine homogeneity of the repeated measures factor. We used a one-way analysis of variance (ANOVA) for each dependent variable to determine the need to covary for baseline differences. We conducted a 3x2 (Group by Session) MANOVA to determine omnibus differences. Our primary analysis consisted of three 3x2 repeated measures ANOVAs (between factor: Group [control, AS, EE]; within factor: Time [baseline, post-test]), for measures of peak knee abduction, peak hip adduction, and peak trunk ipsilateral lean. Given the preliminary pilot and proof of concept nature of this study and consistent with similar prior work (Hogg et al., 2022; Williams et al., 2022), we used effect sizes (ηp2 and Cohen’s d) to interpret the magnitude of main effects and interactions. We interpreted ηp2 effect sizes as small (.01), moderate (.06), and large (.14) and Cohen’s d effect sizes as small (0.2), moderate (0.5) and large (0.8) as according to Cohen (Cohen, 1988). We further investigated main effects of ηp2 > .06 with Tukey post-hoc testing and computed delta scores (Δ) to aid in interpretation. To determine potential sex-specific effects for future studies, we also conducted sex-stratified analyses and inspected between-sex change score differences. This analysis was conducted in JASP (0.14.1) (JASP, 2024).
Results
We were unable to use data from six participants due to technology-related problems (4 in the control group, 1 in AS, and 1 in EE), resulting in our use of a total of 39 participants for all final reported analyses. Data distributions were normal and Levene’s test indicated homogeneity of variances between pre- and post-testing for all variables.
Participants’ Joint Angles at Baseline and at Post-testing Stratified by Group and Sex as Represented With Mean Values (and 95% Confidence Intervals).

Note. *Positive direction denotes worsening kinematics.
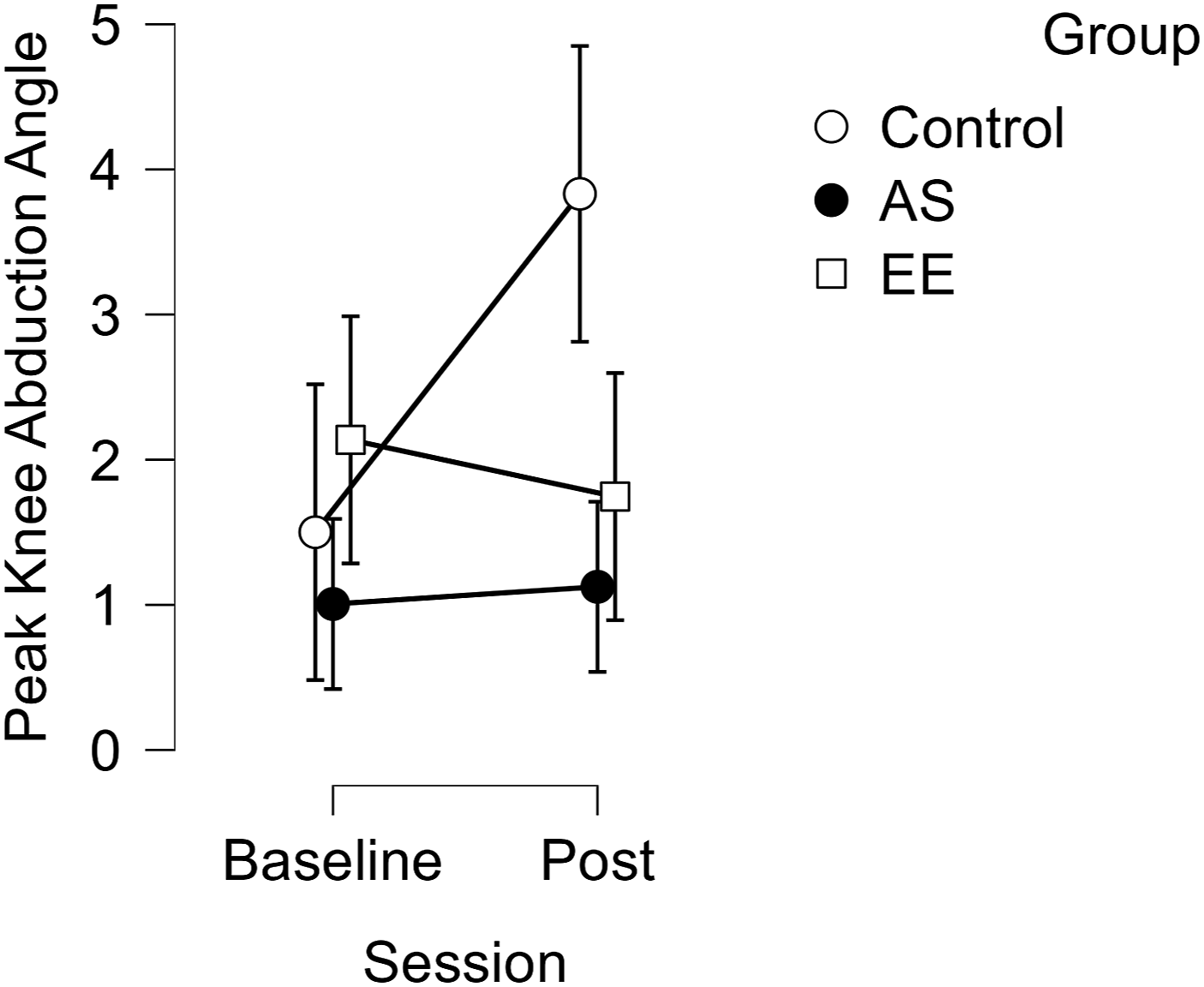
Pre-Post Changes in Knee Abduction Angles for Each Group.
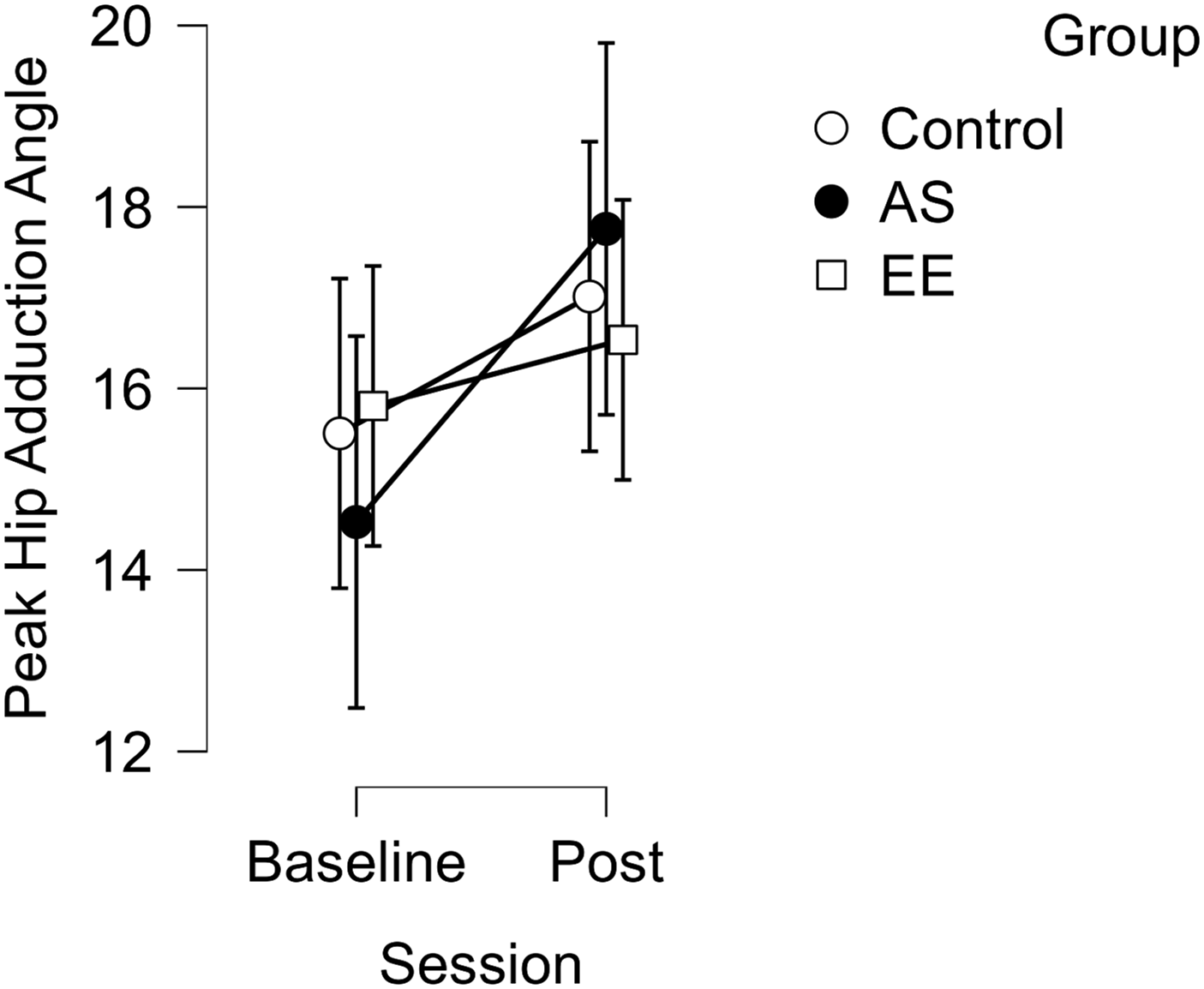
Pre-Post Changes in Hip Adduction Angles for each Group.
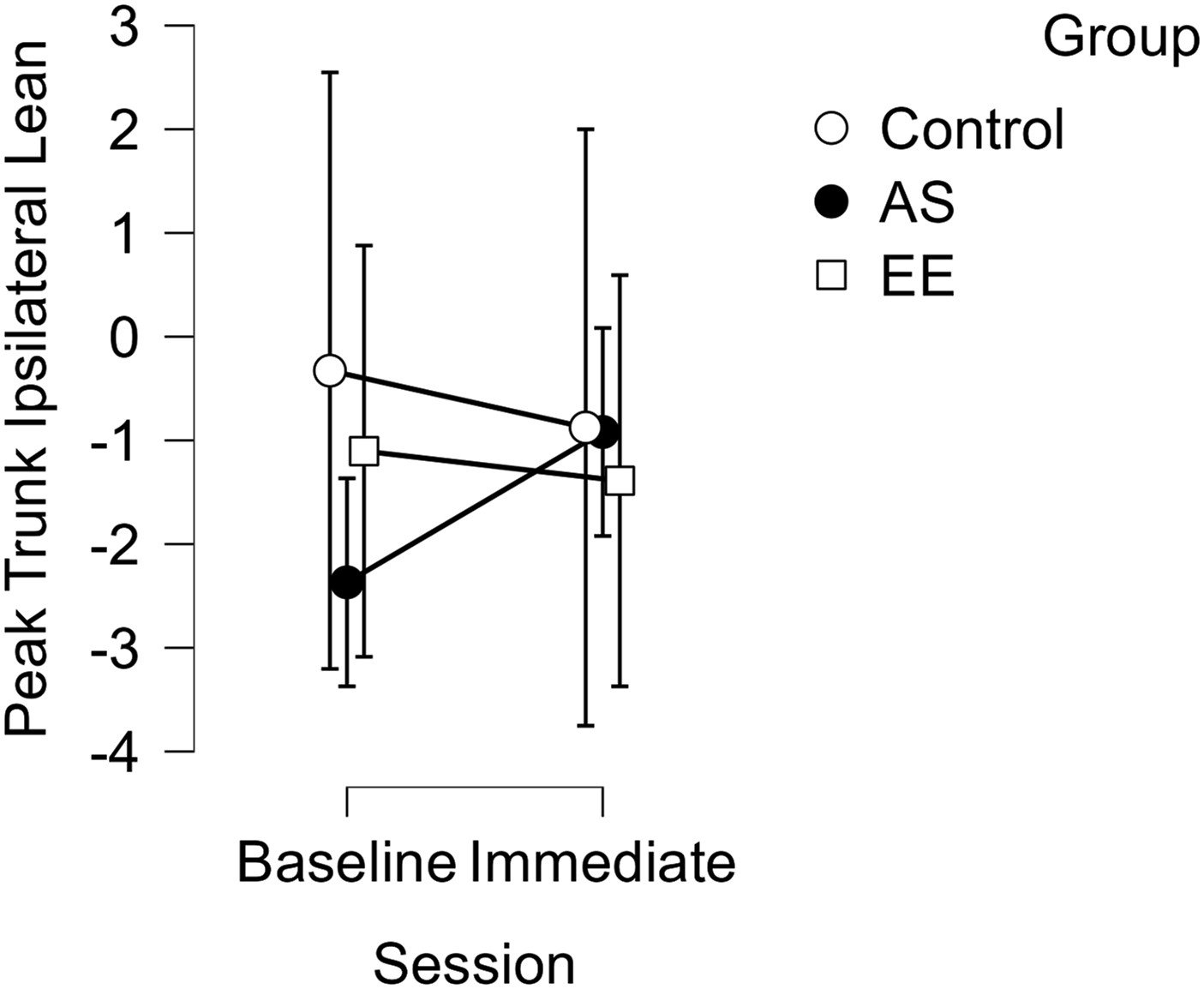
Pre-Post Changes in Ipsilateral Trunk Lean Angle for Each Group.
Discussion
Our hypothesis that participants in the OPTIMAL PREP intervention groups would display improved frontal plane kinematics compared to a control group was partially supported. At post-testing, we observed a marked difference in knee abduction angle between the intervention groups and the control group, but this difference resulted from a worsening of knee angle movement patterns for the control group that was not evident in the intervention groups. At the hip, all groups displayed high-risk adduction at post-testing, while trunk lean kinematics did not change following the intervention.
Following our brief single-leg squatting intervention, the control group displayed 2.3° greater peak knee abduction angle, while the AS and EE groups displayed changes of 0.1° and −0.4°, respectively. The control group, without the motivational aids of AS or EE, may have succumbed to poorer knee movement patterns at post-testing. Conversely, participants in the two intervention groups were able to maintain neutral knee positions at post-testing, even though participants in all groups increased their hip adductions at post-testing. Although not our intent, our intervention of five sets of eight single-leg squat repetitions may have introduced muscle fatigue that was either attenuated for knee angle in AS and EE groups or not in the control group and attenuated in no groups for hip movementsat post-testing. We are speculating that fatigue was the causative factor for these results, because we did not capture muscle strength or activation data. Squatting and jumping fatigue protocols typically require >100 squat and jumps to attain fatigue (Collins et al., 2016), while our protocol consisted of only 40 squats on each leg with self-selected rest. The hip and knee are often thought to be coupled joints, with hip adduction explaining up to 30% of knee abduction (Hogg et al., 2019; Imwalle et al., 2009), which has been documented as a primary predictor of ACL injury (Hewett et al., 2005), In the present study, all groups demonstrated worsening hip adduction from baseline to post-testing. Nevertheless, the interventions implemented here appeared to override the influences of greater hip adduction, since participants in the control group showed these influences while those in treatment groups did not. Our observed effects align with contemporary views of the three pillars of OPTIMAL PREP. Our control group was directed with an external focus of attention, which is theorized to drive primary motor cortex (M1) efficiency (reduced neural activity) via increased sensorimotor integration activity concomitant with intracortical inhibition and corticospinal excitability of M1 (Diekfuss et al., 2021; Kuhn et al., 2017). Conversely, the ‘reward-boosting’ motivational-oriented pillars of autonomy support and enhanced expectancies in our treatment groups are hypothesized to modulate cortical excitability and also trigger a dopamine response throughout various neural pathways (e.g., fronto-striatal circuity) that positively facilitates synaptic transmission between neurons and cells important for sensorimotor control (Diekfuss et al., 2021; Lo & Wang, 2006; Wulf & Lewthwaite, 2016). Thus, giving learners control over their learning environment (AS) or enhancing their expectations for success (EE) theoretically leads to greater motivation (Wulf & Lewthwaite, 2016) and improved dopaminergic transmission that supports stronger within- and between-network brain functional connectivity (Schultz, 2013).
Beyond an external focus of attention, autonomy support and enhanced expectancies are the two motivational tenets of the OPTIMAL theory (Wulf & Lewthwaite, 2016). Using these motor learning techniques to improve performance outcomes has been robustly supported in the literature (Bahmani et al., 2018), but support for their use in improving specific biomechanical, injury-related risk factors has been limited. Specifically, employing real-time visual biofeedback mitigated high-risk biomechanics (Bonnette et al., 2019), and delivering simple EE and AS instructions improved postural balance measures (Chua et al., 2020). To our knowledge, there have been no data addressing the role of these motivational strategies on biomechanics following a potentially fatiguing manipulation. As the third, and most heavily researched, tenet of the OPTIMAL theory, an external focus of attention has repeatedly resulted in both better performance and more efficient muscle contractions (Lohse et al., 2010; Marchant et al., 2009). Thus, it is reasonable to theorize that autonomy support and enhanced expectancies may also result in greater cognitive engagement and muscle efficiency, explaining our observation that our two experimental groups maintained frontal plane knee position despite increased hip adduction.
Because lower extremity biomechanics are known to differ between sexes (Cronström et al., 2016b), we also inspected sex-stratified results. Interestingly, worsening of the control group’s knee abduction appears to have been more pronounced among our female than in our male participants (Table 2). The addition of either an AS or EE feature to the intervention may have eliminated normally identified between-sex differences, suggesting that motor learning motivational strategies may benefit females more than males. An alternative explanation is that because females rely more on frontal plane restraints than males (Cronström et al., 2016b), the improvement in participants’ knee abduction angles could be partially attributed to the targeted movement plane. Future investigators should seek to determine the role that sex-specific biomechanical tendencies and planes of movement may play in the efficacy of motor learning intervention strategies.
Clinical Implications
The present findings have important implications for clinical practice. The advantage of motor learning principles is their ease of use, often requiring only simple adjustments in instructional wording or allowing patient autonomy within the confines of an already existing rehabilitation or prevention protocol (Diekfuss et al., 2020a). Delivering autonomy support could mean allowing a patient to choose the order of exercises or when to receive performance feedback. However, we emphasize that our autonomy support manipulation—asking individuals to choose the color of one’s avatar—would be considered ‘task-irrelevant’ and warrants additional research before clinical implementation. The beneficial effects of task-irrelevant choices on motor performance and learning are not universally supported, as they have had notably less or null effects when delivered to learners possessing high intrinsic motivation (Ikudome et al., 2019; McKay et al., 2022). Nevertheless, our study is unique in that our assessments were not goal-oriented outcomes, but, instead, evaluated more mechanistic biomechanical process for which the ‘goal’ was more nebulous to individuals. A replication of the present findings and a consideration of other means to promote autonomy for improving complex movement patterns is warranted (e.g., task-relevant choices).
As for EE, this intervention is broadly inclusive of any method that results in the learner expecting their own success. This often takes the form of supplying feedback only after successful repetitions, or comparing the learner’s current performance to their own prior performances or to normative performances of lesser quality to immediately bolster self-confidence. Using these strategies in a clinic or sports setting has the added benefit of creating a learner-centered environment, and as such, learning strategies can be personalized to individual preferences.
Limitations and Directions for Further Research
As a preliminary investigation, there are several limitations to our study. First, we did not quantify participants’ cognitive engagement (e.g., motivation) or physical fatigue (e.g., electromyography; rating of perceived exertion), limiting our ability to interpret these findings. Future investigators should add measures to better determine mechanistic drivers underlying the positive motor learning strategies employed herein. For instance, recent investigators have implemented manipulation checks to evaluate the influence of OPTIMAL-based interventions to elicit participant self-efficacy, confidence, motivation, etc. (Simmonds et al., 2023; Simpson et al., 2020; Wulf et al., 2014). We expect our present intervention to produce similar positive cognitive outcomes, but future researchers should employ appropriate manipulation checks to confirm this hypothesis (e.g., via self-report questionnaires or semi-structured interviews). Also, we did not measure physical fatigue and cannot speak directly speak to the possibility that our motor learning manipulations delayed fatigue. Future work should assess learner motivation and include more task-relevant AS options. Similarly, we did not assess transfer learning of the single-leg squatting task to a task more representative of injury-risk scenarios (e.g., simulated sport in virtual reality), and this too might be achieved in subsequent research. Lastly, we assessed AS and EE in separate motor learning interventions, each combined with an external attention focus, to determine which conferred the greatest biomechanical benefit. Prior evidence indicates benefits to employing additive OPTIMAL PREP pillars (Wulf et al., 2014), and future research might include multiple motor learning principles in a single manipulation, perhaps including a “true” control group in which participants are exposed to no motor learning pillars, not even an external attention focus.
Conclusions
The preliminary data from this study indicate that the motor learning strategies of autonomy support and enhanced expectancies can support the immediate retention of injury-resistant frontal plane knee kinematics. Specifically, AS and EE motivational strategies applied during exercise performance may be useful to mitigate maladaptive frontal plane knee mechanics. While not determined in this project, practitioners should consider the potential dose-response effects that can better optimize adaptive responses from autonomy support and the enhanced expectancies enhancement that can be best retained and transferred to other, more sport-specific, tasks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tennessee Higher Education Commission’s Center of Excellence in Applied Computational Science and Engineering, R041302265. Jennifer A. Hogg and Jed A. Diekfuss receive textbook royalties from Kendall Hunt Publishing. Gregory D. Myer consults with commercial entities to support commercialization strategies and applications to the US Food and Drug Administration but has no direct financial interest in commercialization of the products. Dr. Myer’s institution receives current and ongoing grant funding from National Institutes of Health/NIAMS (U01AR067997, R01AR070474, R01AR055563, R01AR076153, R01AR077248, R61AT012421), Department of Defense (W81XWH22C0062), and Arthritis Foundation (OACTN). Dr. Myer has received industry-sponsored research funding to his institutions related to injury prevention and sport performance and has current ongoing funding from Arthrex Inc. to evaluate ACL surgical treatment optimization strategies. Dr. Myer receives author royalties from Human Kinetics and Wolters Kluwer. Dr. Myer is an inventor of biofeedback technologies (patent #US11350854B2, Augmented and Virtual Reality for Sport Performance and Injury Prevention Application, approval date: 06/07/2022, software copyrighted), designed to enhance rehabilitation and prevent injuries. Dr. Myer receives inventor-related royalties from biofeedback technologies (Include Health: LIC1907082014-0706).