
Abstract
In this study we investigated the effects of an 8-week table tennis exercise program with a task-oriented approach on visual perception and motor performance of 31 adolescents with developmental coordination disorder (DCD). The participants were identified by their teachers as having greater difficulty than their peers (450 students from three Korean middle schools) in physical education (PE) classes. On the Bruininks-Oseretsky Test of Motor Proficiency-2, these adolescents scored below the 15th percentile and showed difficulties in performing daily life activities due to motor performance problems; they did not have physical defects, intellectual or neurological impairments, or Attention Deficit Hyperactivity Disorder. Of 98 prospective adolescents with PE difficulties, we obtained personal assent and parents’ informed consent from 54, and 31 of these met screening criteria for DCD through the Developmental Coordination Disorder Questionnaire-Korean. This final group was divided in non-random fashion (based on the proximal geographic grouping of the children’s schools) between an experimental group (n = 16) and a control group (n = 15). The experimental group participated in the 8-week task-oriented table tennis training program with three 90-minute sessions per week, while the control group only participated in regular PE classes twice per week. We measured participants’ visual perception and motor performance in the same environment before and after the intervention program. Participants’ visual perception was significantly more improved in the experimental group than the control group, with specific improved skills in visual-motor search, visual-motor speed, figure-ground, and visual closure; copying and perceptual constancy skills did not improve significantly. In addition, total motor performance and motor sub-skills, including fine manual control, manual coordination, body coordination, strength, and agility were significantly more improved in the experimental group than in the control group. Thus, our task-oriented table tennis exercise program was of greater assistance than general PE classes for improving visual perception and motor performance in adolescents at risk of DCD.
Keywords
Introduction
According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V; American Psychiatric Association, 2013a, 2013b), individuals with developmental coordination disorder (DCD) have significantly lower motor coordination-related abilities than their peers; however, they have no specific medical impairment or neurological disorder. The prevalence of DCD is as high as 5–6%, and individuals with DCD show patterns of slow, inaccurate, and clumsy motor behavior from early stages of motor development (Bair et al., 2011). DCD is associated with serious problems in daily life, physical activity, and academic achievement, due to difficulties in learning new movements or planning and executing motor skills (Bart et al., 2011; Coleman et al., 2001; Rivilis et al., 2011). These characteristics lead to secondary emotional and cognitive problems (Mandich, et al., 2001). For instance, the frustration experienced while performing physical and daily life activities may negatively affect self-confidence and self-esteem (Piek, et al., 2005) and result in delays in cognitive development for more complex and diverse movements (Alloway, 2007).
Several investigators have suggested that impaired visual information processing and reduced sensitivity to visual feedback during the performance of motor tasks may contribute to the motor coordination difficulties observed in individuals with DCD (Caravale, et al., 2014; O’Brien et al., 2008; Sigmundsson et al., 2003; Vaivre-Douret, 2014). Visual perception plays an important role in goal-directed motor tasks, and the development of visual perception is crucial, particularly for generating motor behavior that corresponds to visual stimuli by tracking the location of objects (Jeannerod, 2006; Johnson, 2011). Therefore, enhancing visual perceptual abilities in individuals with DCD may enable efficient exploration strategies for receiving stimuli from the external environment through visual processing and help these individuals achieve efficient movement (Kirby, et al., 2011). Wilson and McKenzie (1998) claimed that visual perception in DCD is highly correlated with motor performance, suggesting that improving visual perception is essential for enhancing motor performance in individuals with DCD (Hulme, et al., 1982a; Hulme, et al., 1982b; Lord & Hulme, 1987a; 1987b).
Previous investigators have reported that interventions involving physical activity and motor-skill training have positive effects on the motor behavior of individuals with DCD (Davidson & Williams, 2000; Polatajko et al., 1995). Motor skill interventions have had a positive impact, not only on the motor abilities of individuals with DCD, but also on their cognitive, emotional, and psychological functioning (Jane, et al., 2018). There are two main approaches used within studies examining the effectiveness of interventions for DCD: (a) a process-oriented, bottom-up approach by which perceptual and motor training assists cognitive functioning; and (b) a task-oriented, top-down approach (Wright & Sugden, 1998). The process-oriented approach aims to improve motor abilities through the recovery of impaired physical functions, whereas the task-oriented approach focuses on the interaction between the person, task, and environment from a motor learning theory perspective, with the goal of enhancing activity performance and participation (Polatajko & Cantin, 2006).
Recently, authors of systematic literature reviews and meta-analyses have reported that a task-oriented approach is more effective than a process-oriented approach in improving motor ability in patients with DCD, suggesting a need for a shift toward task-oriented intervention methods (Armstrong, 2012; Hillier, 2007; Smits-Engelsman et al., 2013). Table tennis, is a sport that is easily accessed in schools or local communities. It requires accurate visual perception for perceiving constantly changing environmental information, and it demands continuous interactions between movement and actions (Rodrigues, et al., 2002); it requires instantaneous alternating attacking and defensive movements, as players must anticipate the direction and position of a fast moving ball. Moreover, in the case of table tennis, a racket sport, situational variations not only prompt the ability to extract information about the opponent’s posture and direction, but they also benefit the development of perceptual-motor skills essential for anticipatory processes (Piras et al., 2016). In addition, table tennis has been reported to affect not only the players’ respiratory and circulatory systems, but their neurological development (Tsai, 2009). Wright et al. (2010) reported that, in skilled versus unskilled table tennis players, there was more prominent activation of the prefrontal cortex, which integrates visual-motor information. Chen et al. (2015) demonstrated that a 16-week racket-based exercise intervention program improved the visual perception abilities of students with intellectual disability and Chang et al. (2002) found that table tennis training enhanced executive functioning and handwriting in children with Attention Deficit Hyperactivity Disorder (ADHD). Based on these findings, the use of table tennis as a visuomotor intervention approach may be an effective task-oriented method for enhancing physical and cognitive functions in DCD. Despite a progression of DCD from childhood through adulthood, most studies have investigated DCD in children (Cousins & Smyth, 2003; Rosenblum, 2013). Since adolescence is a critical period for the development of motor skills, we aimed the current investigation of an 8-week task-oriented table tennis program on the visual perception and motor performance of adolescents with suspected DCD.
Method
Ethical Considerations and Participants
This study was conducted in accordance with the ethical guidelines of Seoul University in Korea, and this research protocol was approved by the relevant Institutional Review Board (IRB No. 1603/001–028). Before the intervention began, we explained the experimental requirements and procedures related to the study to all prospective participants and their parents. All parents of participants finally accepted into this study voluntarily gave their informed consent for their children’s participation, and all child participants gave their informed assent.
The criteria for DCD used in this study were consistent with the diagnostic criteria set forth in the Diagnostic and Statistical Manual of Mental Disorders- Fifth Edition (DSM-5) published by the American Psychiatric Association (American Psychiatric Association, 2013a, 2013b), as follows: “(A) marked impairment in the ability to perform motor activities necessary for daily living based on the individual's chronological age and intellectual ability. This may manifest as delays in the first acquisition of motor skills (e.g., walking, crawling, sitting), clumsiness, dropping things, poor performance in sports or games requiring motor skills, or poor handwriting; (B) impairments in the activities in Group A significantly interfere with academic achievement and performing the daily life activities; (C) the onset of symptoms occurs during the early developmental stage; and (D) the difficulties in motor performance are not due to intellectual disability, visual impairment, or neurological problems that can affect movement (e.g., cerebral palsy, muscular dystrophy, and degenerative disorders).” (p. 74).
The Bruininks-Oseretsky Test of Motor Proficiency-2 (BOTMP-2) and Korean version of the Developmental Coordination Disorder Questionnaire (DCDQ-K) are commonly used assessment tools to evaluate criteria A, B, C, and D of the DSM-5, and they can be used to determine the presence of DCD or ADHD (Tsai et al., 2008). These tools were the methods we used to identify participants with DCD for this study. The DCDQ-K consists of a questionnaire that allows parents to identify and rate their child’s level of cooperation with activities of daily living. In addition, experts in special education and adapted physical education with prior experience in evaluating children’s motor performance administered the BOTMP-2 to each child.
We recruited participants from three middle schools located in S city, Korea after first ruling out through parents and teachers whether each student showed signs of a need for special education, physical or behavioral abnormalities, or neurological damage. We administered the DCDQ-K test to confirm the presence of difficulties in activities of daily living and low motor performance. In this study, we used the DCDQ-K adapted by Lee et al. (2016) from the original questionnaire developed by Wilson et al. (2007). The DCDQ-K is comprised of 15 items that assess three areas: (A) control during movement, (B) fine motor/handwriting, and (C) general coordination. It contains a 5-point Likert scale on which students are rated, and scores represent the sum of these ratings across all items. For this study, we recruited students with DCDQ-K scores between 15 and 75 as participants.
Third, to identify adolescents with motor coordination problems among those screened using the DCDQ-K, we also obtained scores from the BOTMP-2 test and selected those adolescents who scored below the 15th percentile. The BOTMP-2 is a test to measure the maturity level of a student’s motor performance abilities; it has been commonly adopted in clinical and research settings to diagnose DCD and has been found to be suitable for Asian students (Geuze, et al., 2001). Both the BOTMP-2 and DCDQ-K measures are described in greater detail below.
Demographic Characteristics of Study Participants.
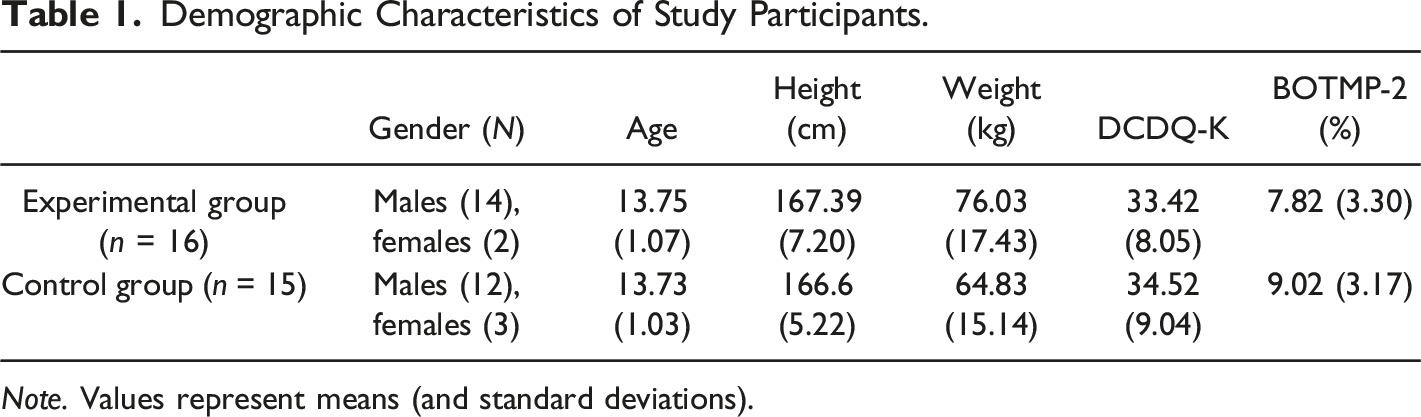
Note. Values represent means (and standard deviations).
Procedure
In this study, we obtained measurements from all participants pre- and post-intervention. The following design and procedures were used to investigate the effects of our task-oriented table tennis exercise program on adolescents with DCD (Figure 1). Study Flowchart.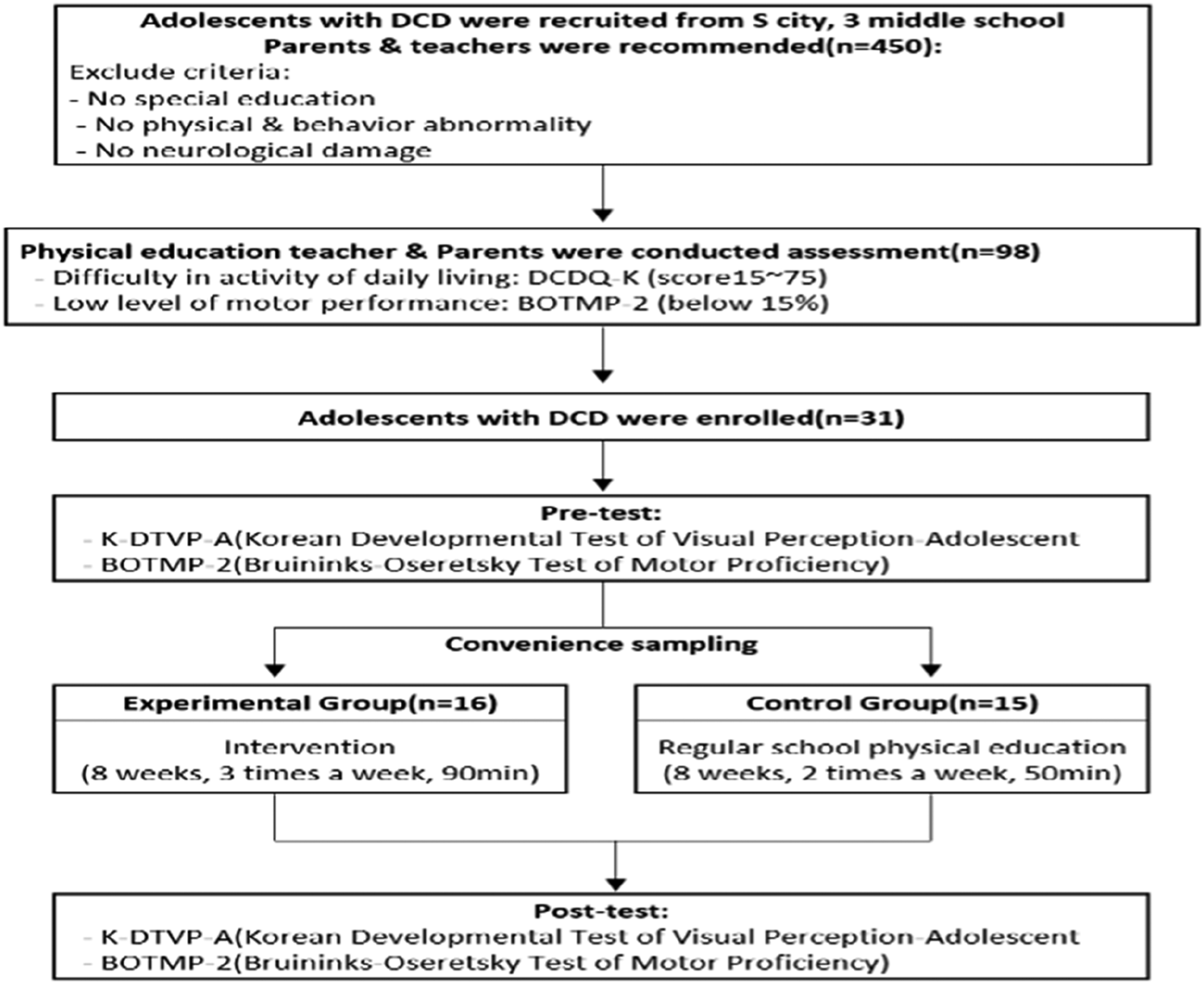
During the intervention period, the attendance rate of the experimental group was 85.4%, while the attendance rate of the control group in regular physical education classes was 100%. After the 8-week intervention program, both groups underwent a post-test with the same items and methods as before.
Intervention
Task-Oriented Table Tennis Training
The intervention program in this study was developed by modifying and improving the table tennis-based physical activity program conducted by Pan et al. (2017). For the systematic organization of the intervention program, we used the ‘teaching table tennis skills’ section from the Table Tennis Coaching Guidelines (2014) presented by Special Olympic and adapted this method to the characteristics of the participants in this study. The developed program was tested for content validity by two table tennis players and two professors majoring in special physical education, and we revised the program after this content validity test. The table tennis expert had more than 10 years of experience as a player and more than 10 years of experience teaching people with intellectual disabilities in the community.
In their meta-analysis, Pless and Carlsson (2000) revealed that exercise interventions were effective when provided at a frequency of at least 3-5 times per week for students with DCD. In this study, the duration of our intervention program (8weeks) was based on Paul et al.’s (2011) findings that table tennis players’ visual function and motor performance improved after sports vision and eye-hand coordination training offered for 45 minutes per session at a pace of three sessions per week for eight weeks. However, considering that the participants of this study were adolescents with DCD, we increased the session durations from 45 to 90 minutes.
Additionally, we designed a task-oriented approach to enhance the intervention’s effectiveness. In this task-oriented approach we listed through task analysis, the necessary movements or skills needed for a given task or movement so that the sub-skills might be learned progressively. The goal of all task-oriented approaches is to enhance performance and participation by organizing the overall task into step-by-step learning (Polatajko & Cantin, 2006). Task-oriented activities are characterized by interventions that focus on the interaction between functional individuals, environments, and tasks, emphasizing task analyses, feedback, and repetitive training (Sugden & Chambers, 2003). As noted above, exercise and physical activity intervention programs based on the task-oriented approach have been suggested as the most effective training alternative for students with DCD (Loftesnes, et al., 2017; Watemberg et al., 2007). We applied the task-oriented approach to the table tennis exercise task to enhance its visual perceptual functions. Each session consisted of a 5-minute warm-up, 20 minutes of training on each table tennis skill (serve, stroke, and receive), a 20-minute game, and a 5-minute cool-down period for a total of 90 minutes per session. The table tennis tasks were divided into three levels so that participants could gradually increase their skill levels depending on their initial performance.
In the first 1–2 weeks, participants performed each subtask related to skill level 1. Skill level 1 consisted of tasks related to upper and lower extremity coordination and saccadic eye movements with a ping-pong ball, which are essential before acquiring other table tennis skills. After recognizing the tasks through the instructor’s demonstration and practicing them repeatedly, the participants set goals for the task according to their level (time or number of success) and performed them repeatedly until they succeeded. During this period, participants competed with each other in a table tennis match to further practice this first skill level.
In the next 3–5 weeks, participants performed each subtask related to basic postures and movement for skill level 2. Initially, participants performed each task without equipment, using only upper limb and lower extremity, and trunk movements. Once the movements were familiarized, they performed the tasks using equipment (racket, ping-pong ball). For the serve task, the participants were asked to send the ball to the target location area beyond the net with their hands or racket; for the stroke skill, they were asked to strike the ball against the wall with their hands or racket (strike a bound ball); and, for the receive skill, they were asked to repeatedly receive or strike the ball quickly with their hands or racket moving on the side step. During this period, the table tennis match was organized such that participants competed against each other on groups of individual tasks for each sub-skill of table tennis based on their personal goals (number of successes against a set number of goals).
Task-Oriented Table Tennis Exercise Program.
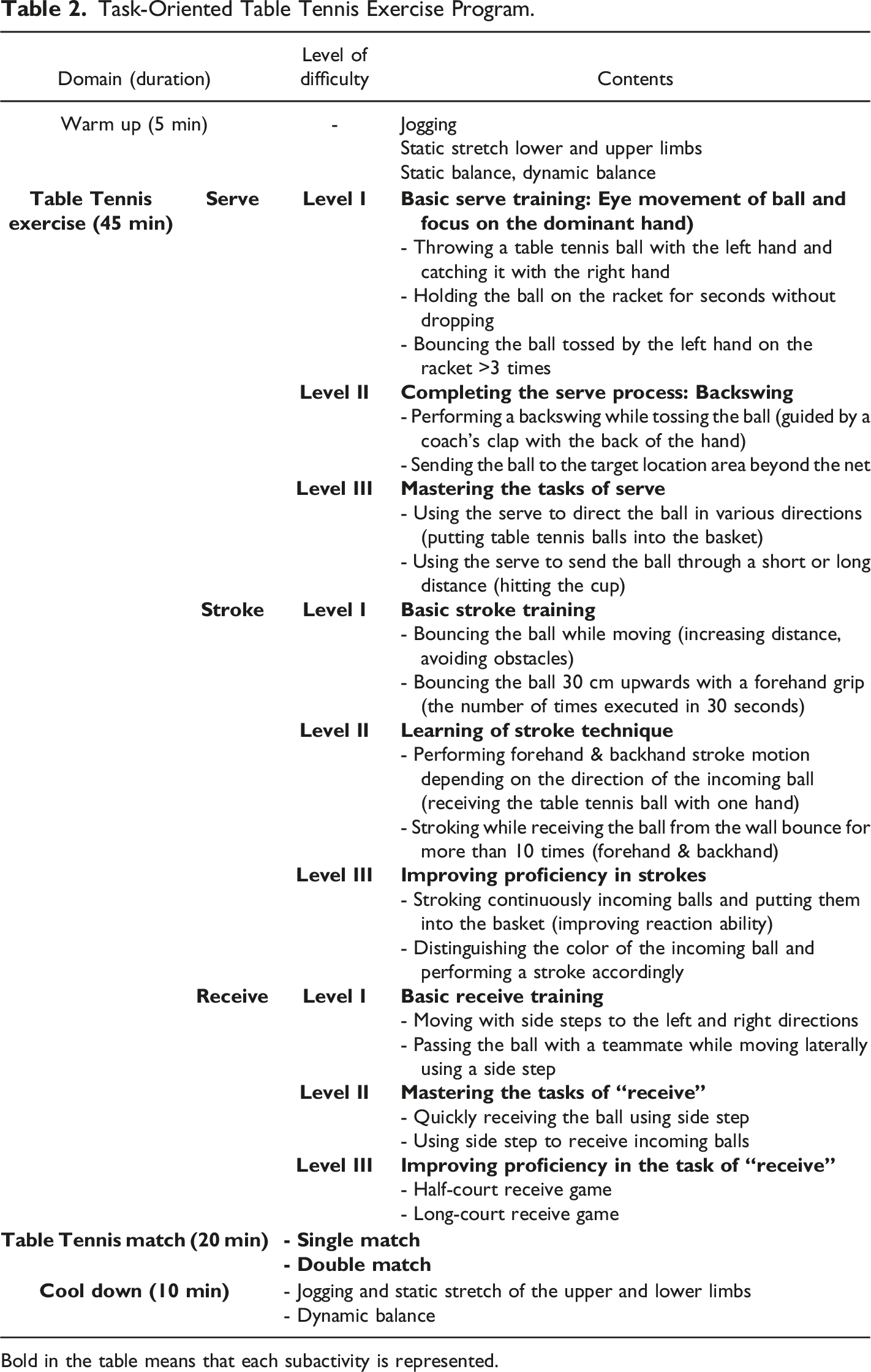
Bold in the table means that each subactivity is represented.

Flow Diagram of the Task-Oriented Table Tennis Exercise Program over 24 Sessions.
Outcome Measures
DCDQ-K Test
In addition to the motor development test (BTOMP-2) applied in DCD screening, we used the DCDQ-K to evaluate students’ day-to-day coordination abilities (Wilson et al., 2013). We used the Korean version of the DCDQ test as translated by Lee et al. (2016), based on the original questionnaire developed by Wilson et al. (2007). The DCDQ-K test evaluates three domains: control during movement, fine motor/handwriting, and general coordination. It has 15 items rated on a 5-point Likert scale. The scale has shown good internal consistency, with a Cronbach’s α of .916 for all items, an average internal validity index of .97, and a test-retest reliability of .982. We selected adolescents with scores between 15 and 75 on the DCDQ-K.
BOTMP-2 Test
The BOTMP-2 test was developed to assess an individual’s motor ability development. This test provides important information about an individual’s growth and maturation. Additionally, the BOTMP-2 test has been widely used for diagnosing DCD in clinical and research settings, and it was found to be suitable for Asian students (Geuze et al., 2001). In addition to quantitatively measuring simple movements, the BOTMP-2 measures coordination, speed, and voluntary movements. The retrieved data can be used for developing educational programs. The test can be applied to individuals ranging from kindergarten age to adulthood (4–21 years), and it has the advantage of requiring only simple training for convenient administration, scoring, and interpretation (Bruininks & Bruininks, 2005). We used the long-form version of the BOTMP-2 to select the participants and measure their motor performance. Sub-test areas included 53 items measuring fine motor control, fine motor integration, manual dexterity, bilateral coordination, balance, running speed and agility, upper-limb coordination, and strength. The administration time was approximately 35–40 minutes.
Korean Developmental Test of Visual Perception-Adolescent (K-DTVP-A)
We also used the K-DTVP-A developed by Cho and Yoo (2013) to evaluate participants’ visual perception abilities. This measure has undergone validity and reliability testing on a sample of 1100 Korean adolescents nationwide. The K-DTVP-A is an adaptation of the Developmental Test of Visual Perception-Adolescent (DTVP-A) developed by Frostig (1961) and Frostig et al. (1966). The original version of the DTVP-A divided visual perception and visual-motor abilities into six subtests (copying, figure-ground, visual-motor search, visual closure, visual-motor speed, and perceptual constancy) for individuals aged 11–74 years. The K-DTVP-A can measure the visual perception ability of adolescents aged 9–19 years. This assessment tool can be useful for objectively assessing the presence and severity of visual perceptual deficits in adolescents. It provides indices for visual perception functioning with motor-reduced requirements (Motor-Reduced Visual Perception; MRPI) and visual-motor integration function with motor skills (Visual-Motor Integration Index; VMII), allowing for comparisons between these two indices. Thus, the standardized score obtained by combining the six subtests represents the General Visual Perception (GVP) scale, which measures various types of visual perception elements and integrates them into one score. The test-retest reliability of the six subtest items of the K-DTVP-A was 0.74–0.87, and the inter-rater reliability was reported as 0.94–0.98. (Cho, et al., 2011).
Statistical Analysis
The data collected in this study were analyzed using the SPSS statistical software package (version 23.0), and we set statistical significance at p < .05. We calculated means and standard deviations for descriptive purposes, and we used an independent t test to confirm the initial similarities of the two participant groups. In addition, we used a repeated-measures two-way (Testing Time X Group) analysis of variance (ANOVA) test to examine any significant differences between Group treatments and Testing Time. When the interaction effect for Time by Group was significant, we analyzed the simple main effect using a paired t test.
Results
Pre-test Visual Perception (K-DTVP-A) Comparisons Between Experimental and Control Groups.
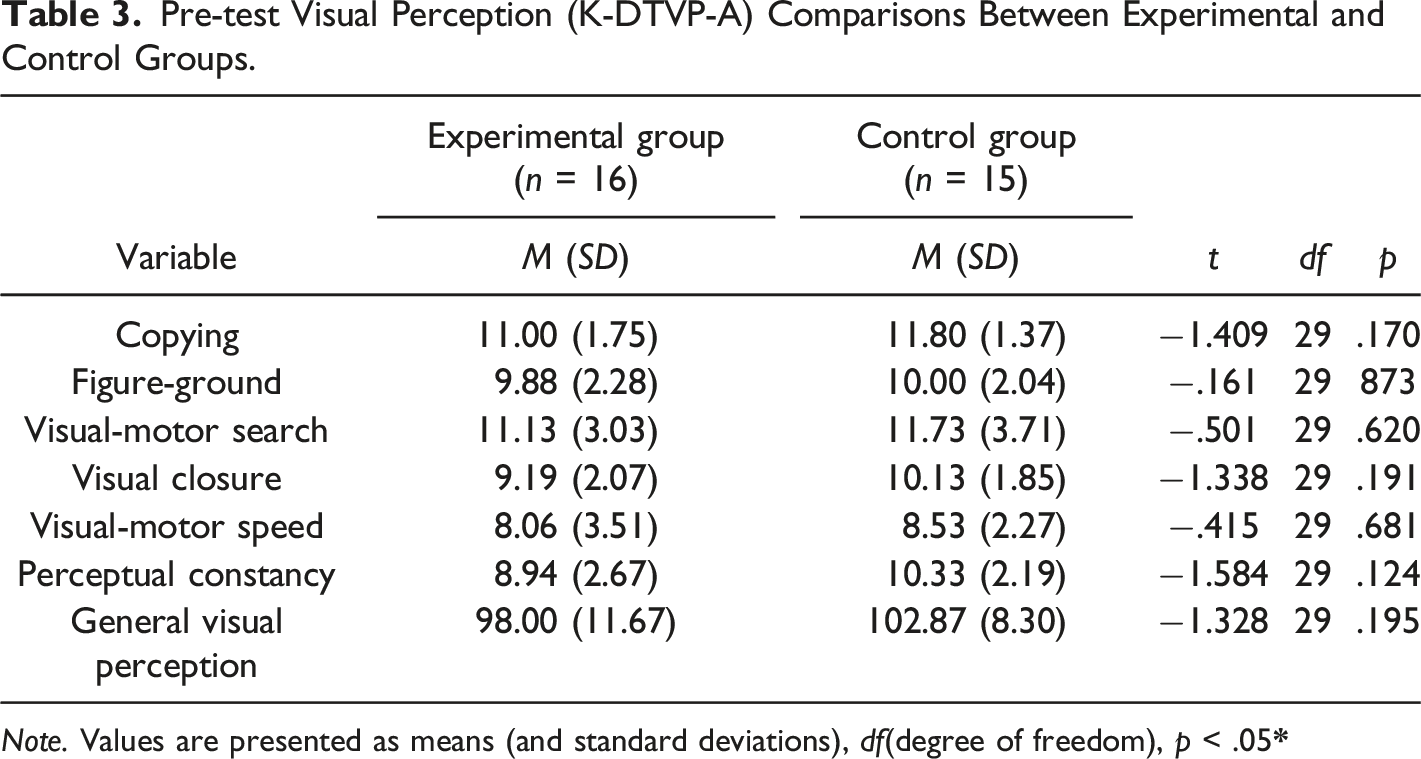
Note. Values are presented as means (and standard deviations), df(degree of freedom), p < .05
Pre-test Motor Performance (BOTMP-2) Comparisons Between Experimental and Control Groups.
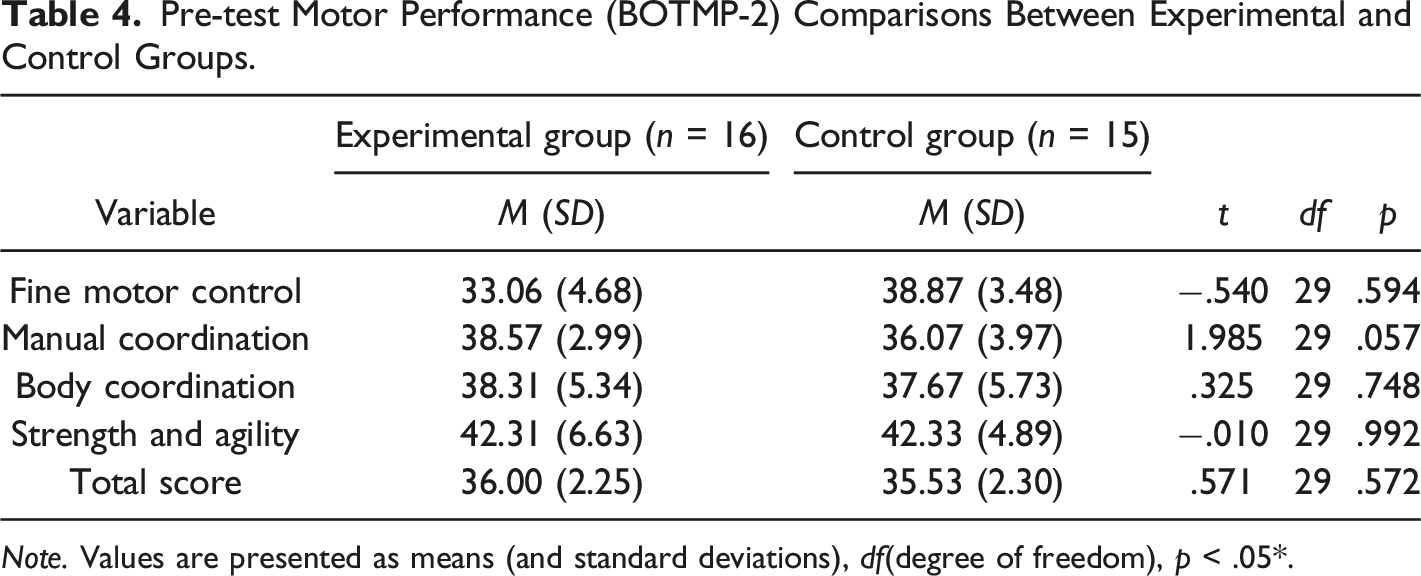
Note. Values are presented as means (and standard deviations), df(degree of freedom), p < .05*.
Visual Perception Ability Test (K-DTVP-A) Results by Group.
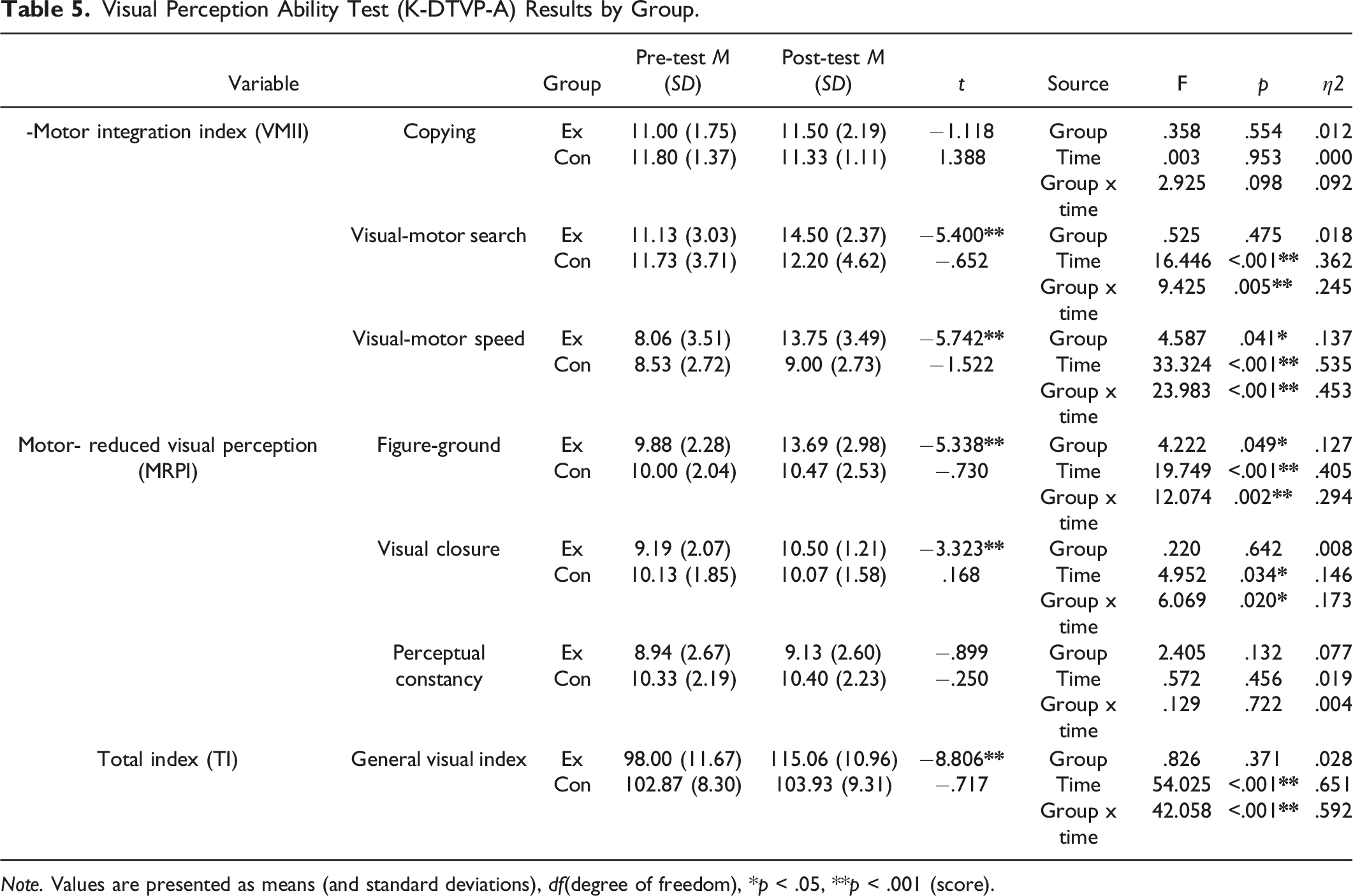
Note. Values are presented as means (and standard deviations), df(degree of freedom), *p < .05, **p < .001 (score).
Motor Performance Test (BOTMP-2) Results.
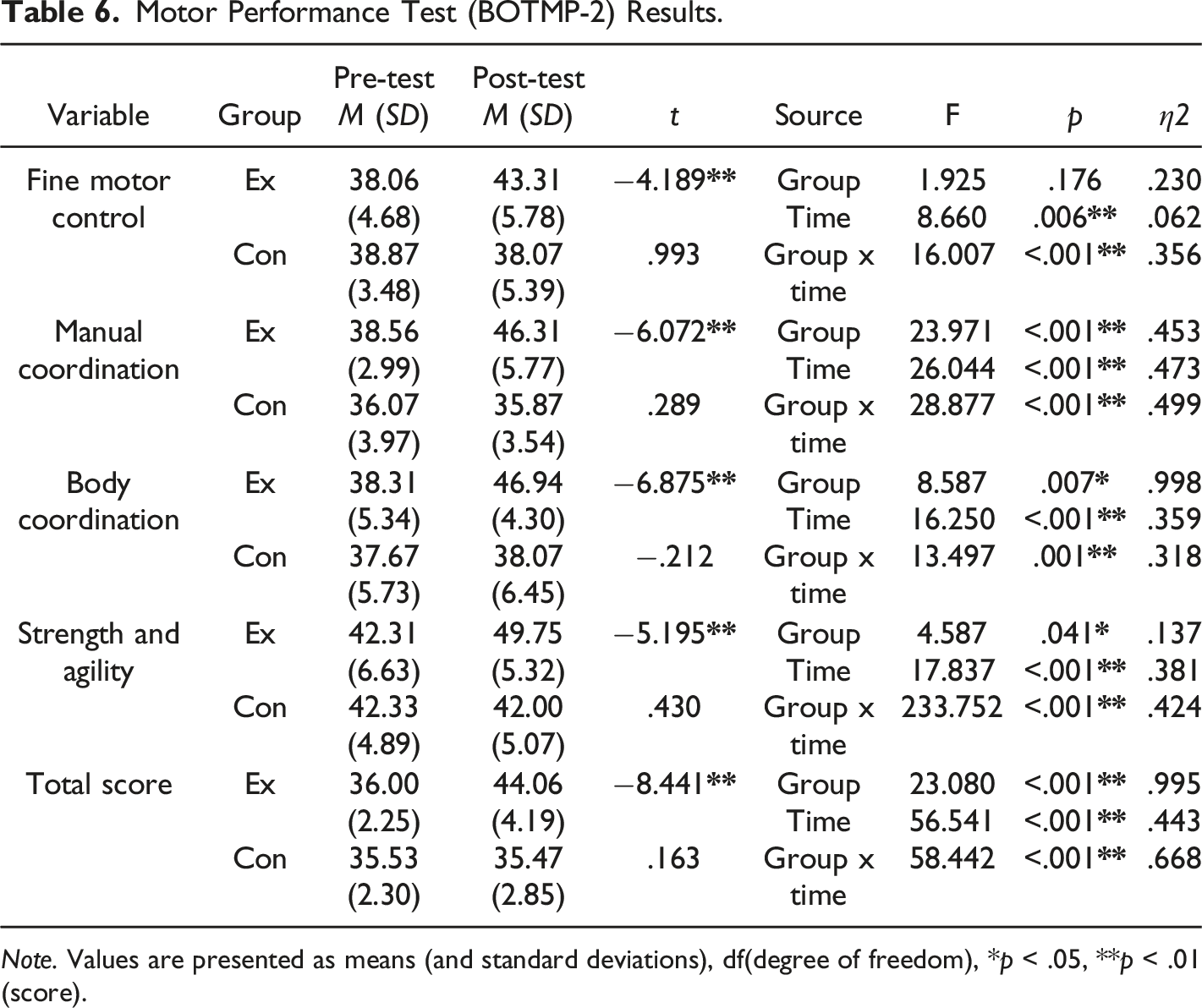
Note. Values are presented as means (and standard deviations), df(degree of freedom), *p < .05, **p < .01 (score).
Discussion
We engaged adolescent participants with DCD in a an 8-week task-oriented table tennis exercise program and compared their visual perceptual and motor performances to participants in a control group. We affirmed hypothesized improvements in the experimental versus the control group, as will be discussed and detailed in the following sections.
Visual Perceptual Findings
On the K-DTVP-A, the experimental group exhibited significant improvements not seen in the control group, including their improved skills in visual-motor search, visual-motor speed, figure-background, visual closure, and the GVP index. Visual-motor integration refers to the ability to coordinate information obtained through visual perception with the motor system through neural pathways (Dankert, et al., 2003). The VMII measure from the K-DTVP-A is a standardized clinical index that integrates results obtained from copying, visual-motor search, and visual-motor speed. Davidson and Williams (2000) reported a statistically significant improvement on the VMII among individuals with DCD after their participation in a 10-week occupational therapy program that focused on fine motor activity. Consistent with our results, Chen et al. (2015) reported, among children with intellectual disabilities, that those receiving either occupational therapy or table tennis training exhibited significantly improved visual motor integration ability relative to a control group. Kaiser et al. (2009) reported that repeated training tasks that required eye-hand coordination were important to significant improvements in visual-motor integration ability, and such training characterized the table tennis activities we used. We inferred that the repeated execution of tasks that required visual information processing, reaction planning, and appropriate reprogramming of movements to respond to cues had a positive impact on this observed improvement in our experimental group.
Of note, we observed no significant interaction effect of group and time for either the experimental or control groups on the copying item of the visual-motor integration score. This subtest, a component of the K-DTVP-A, gradually increases in difficulty from simple to complex shapes, requiring high levels of exploratory strategy. The adolescent participants with DCD in our study faced difficulties in performing the copying item of the K-DTVP-A subtest, possibly due to their inefficient, low-level visual search strategy (Dwyer & McKenzie, 1994; Wilson & McKenzie, 1998). Considering the characteristics of DCD, which manifest with difficulties in utilizing vision to explore and imitate environmental information, our 8-week intervention period may have been a relatively short period in which to effect change in this area; future studies should consider extending the intervention period to more than eight weeks.
Regarding the MRPI, referring to visual perception abilities under conditions where motor functions are minimized, we observed statistically significant differences among participants in the experimental group on the figure-ground and visual closure domains, but no significant improvements on perceptual constancy in either group over time. This is consistent with Badami et al. (2016), who showed significant improvements on the MRPI in children with dyslexia after 12 weeks of sports vision exercise participation, and with Coetzee and Pienaar (2013), who reported significant improvements in eye movement control ability through an intervention program focused on eye exercises for children with DCD. Furthermore, Sumner et al. (2018) reported that children with DCD showed more difficulties in ocular-motor control than typically developing (TD) children. Our intervention program provided various repetitive tasks to enable participants to perform saccadic eye movements, object tracking, and other related visual tasks such as striking a ball in various directions and at various speeds, transferring it to a designated area, hitting a cup, and putting the ball into a basket. During these tasks, others have shown that visual attention focusing on key task requirements facilitated improved visual control of eye movements with a positive impact on both visual attention and concentration (Wilson & Falkel, 2004). We too found that repeated practice in our task-oriented approach to eye-movement training positively impacted visual closure and figure-ground skills of our experimental group.
We observed no statistically significant interaction effect between Group and Time for the MRPI sub-test of perceptual constancy, measuring the ability to identify shapes and form in a series of images, despite differences in their size, location, shading, or complex backgrounds. In contrast, Kim et al. (2012) reported improved perceptual constancy in children with DCD who participated in a 6-week arts and crafts program, and Eo and Kim (2012) reported significant improvements in perceptual constancy through a 30-session scotoma technique in children with no disabilities. Art activities typically require sufficient time for visual information processing and exploration as well as precise and delicate movements focused on fine motor skills while rapid visual processing and involvement of more gross motor skills characterized our training activities, perhaps explaining our failure to show relatively greater gains in our experimental group on this measure.
Motor Performance
On the BOTMP-2, our experimental group showed statistically significant improvements following the 8-week table tennis intervention, in all subdomains (total score of motor performance, fine motor precision, hand coordination, body coordination, strength, and agility). These findings were consistent with those of Tsai et al. (2012) for children with DCD who underwent a task-oriented soccer intervention and Watemberg et al. (2007) who used a task-oriented sports program to assist children with combined ADHD and DCD. As reported in previous studies (Preston et al., 2017; Smits-Engelsman et al., 2013), interventions using task-oriented approaches are highly effective for students with DCD with characteristically slow and inaccurate motor performances and difficulty controlling movements.
We also observed significant improvements in fine motor control and manual coordination, following our table tennis intervention, consistent with Feguson et al. (2013) who reported statistically significant differences in the fine motor control abilities of children with DCD after neuromotor task training (NTT) that integrated movement elements based on cognitive neuroscience and motor training). Most sports that utilize rackets require a high level of eye-hand coordination and perceptual-motor abilities (Lees, 2003), since when manipulating objects, eye-hand coordination relies on obtaining and organizing visual perception information to be manifested in subsequent movement (Abrams, et al., 1990). Table tennis meets this objective by requiring players to track and explore rapidly moving objects and precisely hit the ball with a racket, using precise movement control through the coordinated movement of the head, eyes, and hands (Rodrigues, et al., 2002). Therefore, the tasks of our intervention program helped to develop eye-hand coordination.
Our experimental group showed statistically significant improvements compared to the control group in body coordination, including balance ability and bilateral coordination, both of which are essential components of motor performance. These results are consistent with Jelsma et al. (2014) who showed significant improvements in bilateral coordination and balance ability after six weeks of Wii-based Ski Saloam training for participants with DCD and balance problems. Our results are also consistent with Peens et al. (2008) whose participants with DCD improved balance and motor coordination an 8-week exercise intervention program. Tsai et al. (2012) emphasized that exercise programs should not only focus on lower-limb movements but should also incorporate simultaneous upper-limb movements that effectively improve body coordination; our intervention program did involve various fine and gross motor tasks involving simple eye-hand coordination tasks as well as simultaneous movement of the upper and lower limbs and postural control.
Finally, we observed a statistically significant difference in the improvement difference of muscle strength and agility between our experimental and control groups. These results are consistent with those Jelsma et al. (2014) in which muscle strength and agility improved in children with DCD after participating in a Wii Fit Ski program focused on body weight shifts and with Pan et al.’s (2017) observation that improved ability to control weight shift not only enhanced running performance, but also improved muscular strength and agility. In this regard, our intervention program was designed to repeatedly perform movement tasks with patterns of weight shifting associated with predicting movement of an irregularly approaching ball to enable quick reactions (Guizani, et al., 2006; Lees, 2003).
Limitations and Directions for Further Research
Of note, we did not utilize a licensed health care provider to provide diagnoses of DCD for our participants, and we did not employ random sampling and random group assignments because of difficulties in recruiting participants and conducting the intervention program in collaboration with the day-to-day operations of three middle schools in S city. In place of these methods, we utilized objective screening measures of DCD to identify participants at risk for DCD. This study should be replicated and extended with a larger sample of children who are formally diagnosed with DCD and randomly assigned to experimental and control groups.
Second, we conducted this study over only eight weeks because of the difficulty of mediating the schedules between the three middle schools. This 8-week intervention period (with three 90-minute sessions per week) was relatively short to clearly demonstrate the program’s effectiveness, and this may have limited our ability to show significant changes on some measures. Future investigators should conduct longer periods of intervention and possibly explore changes more thoroughly through pretesting, post-testing and follow-up testing to ascertain the persistence of the gains we observed.
Third, while our results confirmed the positive effect of the intervention program on the visual perception ability and motor performance of adolescents with DCD, comparisons between experimental and control groups alone may be limited in clearly demonstrating program effects. In future research, this intervention might be compared not just to a control group but to groups receiving other types of sports or intervention methods.
Conclusion
In this study, we demonstrated that, relative to a control group, an 8-week task-oriented table tennis exercise program had positive effects on both the visual perception and motor performance of adolescents with DCD. We discussed this intervention in detail, embedded our findings in a rich literature that supports the use of task-oriented visual-motor training for individuals with DCD, and we described the limitations of this study and suggested improvements for further research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.