
Abstract
This study was designed to investigate the construct–concurrent validity and reliability of the Turkish version of the Peabody Developmental Motor Scale–2 (PDMS-2) in at-risk infants between 0–24 age in Turkey. In this study, 120 infants (70 males, 50 females) participated in the study (mean corrected age 20.18 ± 22.535 weeks). The PDMS-2 scale consists of two subdimensions, the Fine Motor Quotient (FMQ) and the Gross Motor Quotient (GMQ). Whereas the construct validity was assessed using confirmatory factor analysis, concurrent validity was investigated using the correlation between PDMS-2 and the Alberta Infant Motor Scale and the Hammersmith Infant Neurological Examination with Spearman’s correlation analysis. The PDMS-2 was applied twice for test–retest reliability. Cronbach’s alpha (α) and the intraclass correlation coefficient (ICC) were used for reliability. ICC value was with 95% CI. The overall reliability coefficient of the test was found to be Croncbach’s α = 0.865. TICC values were found (ICC FMQ: 0.998, ICC GMQ: 0.998). Construct validity (
Introduction
Infants at risk have a history of environmental or biological factors during pregnancy, birth, or the newborn period, and these factors may lead to a higher than average risk of mortality and morbidity (Allen, 1993). A “high-risk infant” is generally defined as an infant who requires more than the standard monitoring and care offered to a healthy, full-term newborn infant. Therefore, infants born prematurely or later, those with inappropriate growth for gestational age, infants with obvious signs and symptoms of systemic diseases, metabolic abnormalities, or congenital malformations that require early evaluation and treatment are considered “high-risk infants” (Raju et al., 2017). Premature infants who weigh less than 1500 g at birth; are born at ≤32 weeks of gestation; have respiratory distress syndrome, hyperbilirubinemia, retinopathy of prematurity, hypoxic ischemic encephalopathy, periventricular leukomalacia, intraventricular hemorrhage, or necrotizing enterocolitis; or have neurologic problems due to reasons such as intrauterine growth retardation and patent ductus arteriosus are included in the at-risk infant group (Atalay et al., 2013; Balci et al., 2021; Tavasoli et al., 2014).
The incidence of developmental disorders in at-risk infants is higher than in healthy infants (Doyle et al., 2014). The early detection of motor problems is important for early intervention (Akbaş Numanoğlu et al., 2020; Novak et al., 2017). It has been reported that physiotherapy and rehabilitation approaches are applied in early infancy especially to benefit from the high plasticity ability of the brain (Blauw-Hospers & Hadders-Algra, 2005). With the development of medical care facilities, there has been an increase in the survival rate of high-risk infants born preterm and with low birth weight. For these reasons, neuromotor evaluations of high-risk infants are important (Aisen et al., 2011).
Studies in the literature have evaluated the gross and/or fine motor development of infants at risk using measurement tools with different characteristics. Among these, the Alberta Infant Motor Scale (AIMS) (Piper et al., 1992), BAYLEY-III(Anderson et al., 2010), Bruininks–Oseretsky Motor Proficiency Test (Duger et al., 1999), Movement Assessment Battery for Children (Croce et al., 2001), Pediatric Evaluation of Disability Inventory (Berg et al., 2004), and Test of Gross Motor Development (Evaggelinou et al., 2002) are widely used coarse and/or fine as measurement tools for evaluting motor development. In general, the evaluation process using these scales is considered after 24 months. AIMS, one of the scales used in the motor assessment of infants younger than 24 months of age, evaluates the process until walking and does not include the postwalking period.
Folio et al. developed the PDMS-2 to assess motor development and consists of six subtests (reflex, stationary, movement, object manipulation, grasping and visual-motor integration) that measure interrelated abilities in early motor development (Folio & Fewel, 1983). It is designed to assess gross and fine motor skills in children from birth to 5 years of age. All PDMS-2 subtests contribute to the Total Motor Quotient (TMQ). This score is generally considered to be the best estimate of overall motor skills. In addition, each subtest contributes to a Gross Motor Quotient (GMQ) or Fine Motor Quotient (FMQ) score. The GMQ measures the ability to use large muscle systems to move from place to place, maintain a stable posture when not moving, respond automatically to environmental changes, and catch and throw objects. The FMQ measures a child’s ability to use hands and arms to grasp objects, stack blocks, draw shapes, and manipulate objects. Each item on the PDMS-2 is rated on a three-point scale: 0; children do not or cannot attempt the item or the attempt does not indicate that the skill is developing, 1; children’s performance shows a clear resemblance to the item mastery criteria but does not fully meet the criteria, and 2; children perform the item according to the criteria specified for mastery. Any item skipped or not attempted is given a score of zero. The Peabody Motor Development–2 (PDMS-2) includes assessments of both gross and fine motor skills and has been used to evaluate children’s developmental progress (Jensen et al., 2015), identify motor deficits and determine eligibility for interventions (Fraga-Sousa et al., 2016), and detect motor limitations in children with disabilities (Wang et al., 2017). The scale was also designed to support clinical and educational intervention plans, as well as follow-up assessments (Folio & Fewel, 1983). The psychometric properties of the PDMS-2, including various indices and adjustments, have been investigated across multiple countries and age groups. In the Netherlands, Van Hartingsveldt et al. confirmed the reliability of the PDMS-2, but only for the fine motor subscale in a small sample of 18 children aged 4–5 years (Van Hartingsveldt et al., 2005). In Portugal, Saraiva, Rodrigues, and Barreiros supported the validity of both the gross and fine motor subscales for a group of 540 preschool children aged 3–6 years (Saraiva et al., 2011). In Iran, Tavasoli et al. confirmed the validity and reliability of the PDMS-2 in a study of 88 newborn infants (Tavasoli et al., 2014). In Turkiye, Taştepe et al. assessed validity and reliability of Peabody Developmental Motor Scales-2 (PDMS-2) on Turkish 36-47 month-old children and to analyze the children’s motor development in terms of gender and age variables in Turkey (Taştepe & Akyol, 2019). Unfortunately, in Turkey, the PDMS-2 has been minimally utilized to assess children’s motor performance, according to the author’s knowledge. As a result, professionals face a shortage of tools that could be valuable in evaluating children both with and without disabilities.
In this study, the validity and reliability of the PDMS-2, which provides the opportunity to evaluate the both gross and fine motor levels of infant at risk from birth to 24 months, with detailed items, was conducted among Turkish children aged 0–24 months old, and the motor development of these children was determined. The sufficiency of psychometric properties of the PDMS-2 would enable the Turkish version of the test to be used as a standardized assessment tool for evaluating the clinical motor performance of infants both in Türkiye and Turk researcers and clinicians all aroud the world.
Materials and Methods
Research Design
We conducted a cross-sectional study with a test–retest design to determine the reliability and validity of the Turkish version of the PDMS-2 between August 2020 and May 2021.
Participants
Approval for the present study was obtained by the local ethics committee of KTO Karatay University (41901325–050.99 2020/017). The study was conducted in accordance with the principles of the Declaration of Helsinki. The data were collected after informed parental consent and written informed consent was gathered from all participants. Infants (70 males, 50 females) who had been admitted to the Pediatric Rehabilitation Unit were recruited for this methodological study. The departments consisted of tertiary specialized outpatient clinics for infants at risk of, or with, a neurodevelopmental or neurologic disorder. At-risk infants with early preterm birth (˂32 weeks), moderately preterm birth (32–34 weeks), multiple birth, hypoxic ischemic encephalopathy, bronchopulmonary dysplasia, intraventricular hemorrhage, antenatal hemorrhage, large for gestational age, periventricular locomalasia between 0-24 months old were included in the study. Infants were excluded if they had (1) a known progressive neurologic disorder (early-onset myotonic dystrophy, genetic refractory epileptic encephalopathy, refractory focal epilepsy, multiple side effects of antiepileptic drugs, structural West syndrome, cortical malformation) and (2) congenital anomalies, musculoskeletal disorders, cyanotic congenital heart disease, or mechanical dependency.
Power Analysis
A post-hoc power analysis was conducted using R version 4.2.1 (packages ‘semPower’ and ‘ICC.sample.size’, R Core Team, 2022) to determine the exact power of the study. The post-hoc power for the confirmatory factor analysis (alpha = 0.05, degrees of freedom: 5, n = 120, null hypothesized RMSEA value of 0.08, and alternative hypothesized RMSEA value of 0.021) and the ICC (obtained ICC = 0.99, null hypothesized ICC = 0.70, number of ratings: 2, alpha = 0.05, two-tailed, n = 120) were 83.01% and 99.99%, respectively. Results show that the achieved power was sufficient to draw valid and reliable conclusions based on obtained data (Faul et al., 2007).
Translation Process
The authors had translation permission from PRO-ED for PDMS-2. Based on previous studies and guidelines (Beaton et al., 2000), forward and backward translation methods were used to perform the cross-cultural adaptation. Two independent professionals translated the PDMS-2 from English to Turkish. After the translated versions were harmonized as a first version with discussion and consensus between translators and the second author, a back translation was performed by a different bilingual, native English–speaking translator who was unfamiliar with and blinded to the original version of the PDMS-2. An expert committee, including the first and second authors, who are two pediatric physiotherapists with at least 5 years of experience in the field of children with disabilities, reviewed the final Turkish version of the PDMS-2. The items didn’t needed to be considered and adapted due to cultural differences.
Procedure
To assess interrater reliability, two physiotherapists evaluated the same patient using the PDMS-2. Two therapist tested separately the same child, at different times in a day or the following day. To examine the intrarater reliability, one of the same physiotherapist scored the same patient the following day. To assess concurrent validity, the Hammersmith Infant Neurological Examination (HINE) and AIMS tests were used, as described below, on the same day. Patient characteristics (i.e., age, gender, gestational week) were also recorded. It took aproximately 40–60 minutes to administer all tests in the baseline assessment, including the time for a rest interval between the tests to allow the infant to meet physiological needs and to be at a comfortable behavioral level before each test. The physiotherapists had more than 5 years of experience in the field. The same physiotherapist conducted all tests (AIMS, HINE and PMDS-2) following standard testing guidelines for each test. In all cases, the two physiotherapists were blinded to each other’s scores. The PDMS-2 was repeated with these children after 1 week for internal consistency.
Measurements
Peabody Motor Development–2 (PDMS-2)
The PDMS-2 is used to assess children’s fine and gross performance from zero to 71 months of age. The PDMS-2 is currently used to estimate children’s motor competence and compare the results with standardizing norms, identify relative differences in fine and gross motor development among children, establish individual goals and objectives for therapy or intervention, monitor the child’s progress, and as a research tool (Fraga-Sousa et al., 2016). The standards of the PDMS-2 are based on the development of 2003 children from 46 states in the United States and a Canadian province. The representativeness of the standards and the psychometric properties of the PDMS-2 has been improved from its original version. Adequate indices of internal consistency for the subscales (α = 0.89–0.95), fine motor quotient (FMQ) and gross motor quotient (GMQ; α = 0.96–0.97), test–retest reliability (r = 0.73–0.96 in different age groups), and reliability among observers (α subscale range 0.97–0.99 and from 0.96–0.98 for motor quotients) were reported. With regard to the construct validity of the PDMS-2, two confirmatory factorial studies identified a measurement model consisting of two factors (FMQ and GMQ), defined respectively by two subscales for the FMQ, (1) visuo-motor integration with 72 tasks and (2) grasping with 26 tasks, and four subscales for the GMQ: (1) stationary with 30 tasks, (2) locomotion with 89 tasks, (3) object manipulation with 24 tasks for children 12 months and older, and (4) reflexes with eight tasks for children aged 11 months or younger. These subscales allow the estimation of three global motor performance indices: FMQ, GMQ, and Total Motor Quotient (TMQ). The scores protocol has three levels (performed the task correctly: 2 points; performed tasks partially: 1 point; did not execute the development criteria correctly: zero points). The sum of the points comprises the raw score for each subscale. The standard score, percentile, equivalent age, and z-score are also provided. The scores on each component (GMQ, FMQ and TMQ) could be as very superior (131–165), superior (121–130), above average (110–120), average (90–109), below average (80–89), poor (70–79), and very poor (35–69) (Folio & Fewell, 2000; Tavasoli et al., 2014).
Hammersmith Infant Neurological Examination (HINE)
The HINE includes three sections: the Neurological Examination, the Development of Motor Functions, and the State of Behaviour. The first section evaluates the cranial nerve, posture, movements, tone, and reflexes. These items are not age dependent. The second section evaluates head control, sitting, voluntary grasping, rolling, crawling, and walking. The third section evaluates state of consciousness, emotional state, and social orientation. The data obtained in the second and third sections are not included in the calculation of the global optimality scores. They provide additional information on the interpretation of neurological findings, but a frequency distribution for these two age-dependent sections was not calculated. The overall score ranges from a minimum of zero to a maximum of 78. At 9 or 12 months, scores ≥73 are regarded as optimal and <73 as suboptimal; whereas at 3 and 6 months, healthy term infants score ≥67 and 70 (median), respectively (Haataja et al., 1999, 2003).
Alberta Infant Motor Scale (AIMS)
The AIMS was used to assess gross motor development. This scale is a norm-referenced observational tool designed to evaluate gross motor development in infants from birth to 18 months of age or the acquisition of independent walking. It consists of 58 items and four subscales: supine (9 items), prone (21 items), sitting (12 items), and standing (16 items), which are observed in postural alignment, antigravity movements, and surface contact. The motor skills observed correspond to the infant’s motor window consisting of all items located between the less and more mature capabilities observed in the motor repertoire. Assessment was based on the free observation of the child in different positions (prone, supine, sitting, and standing) according to the child’s age. A score is obtained between zero and 58 points. The obtained score can be converted to a normative age-dependent percentile rank: 5th, 10th, 25th, 50th, 75th, or 90th percentiles. A score less than the 10th percentile was classified as possibly delayed motor development (Darrah et al., 1998).
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics Standard Concurrent User V 26 (IBM Corp, Armonk, NY, USA) and Amos V23 (IBM SPSS, Chicago, IL, USA) for confirmatory factor analysis. Descriptive statistics were used to describe patients’ demographic characteristics and assessment results. Continuous variables were expressed by mean (standard deviation), whereas categorical variables were reported as number (%). Internal consistency was assessed by calculating and categorizing the Cronbach’s alpha coefficient as follows: excellent, >0.80; adequate, 0.70–0.79; and inadequate, <0.70 (Andresen, 2000). Intrarater and interrater reliabilities were assessed using the intraclass correlation coefficient (ICC) using the two-way random effects and absolute agreement methods (Koo & Li, 2016). A principal component exploratory factor analysis was used to investigate the relationships between each of the dimensions. We applied the Kaiser criterion to retain any latent factors with eigenvalues equal to or greater than 1. Factor loadings of >0.5 were deemed to be highly relevant to the latent factor. Items with factor loadings greater than 0.40 were retained. The ratio of the chi-square test of model fit to the degrees of freedom (χ2/df; values of 5 or less). The Tucker–Lewis Index (>0.90 acceptable and >0.95 excellent), the Comparative Fit Index (>0.90 acceptable and >0.95 excellent), standardized root mean square residual (<0.08 acceptable and <0.05 excellent), and the root mean square error of approximation (<0.08 acceptable and <0.05 excellent) were used as goodness-of-fit statistics (Geldhof et al., 2014). To evaluate criterion validity, the Spearman’s correlation coefficient was calculated between the PDMS-2 and the HINE and the AIMS. The level of the relationship was classified using the Spearman’s correlation coefficient as follows: <0.30 = small/negligible, 0.30–0.50 = low, 0.50–0.69 = moderate, 0.70–0.90 = high, and >0.90 = very high (Mukaka, 2012). The descriptive level of significance was set at p < .05.
A post-hoc power analysis was conducted using R version 4.2.1 to determine the exact power of the study. The post-hoc power for the confirmatory factor analysis (alpha = 0.05, degrees of freedom: 5, n = 120, null hypothesized RMSEA value of 0.08, and alternative hypothesized RMSEA value of 0.021) and the ICC (obtained ICC = 0.99, null hypothesized ICC = 0.70, number of ratings: 2, alpha = 0.05, two-tailed, n = 120) were 83.01% and 99.99%, respectively. Results show that the achieved power was sufficient to draw valid and reliable conclusions based on obtained data (Celik et al., 2024).
Results
Sociodemographic and Clinical Features of the At-Risk Infants (N = 120).
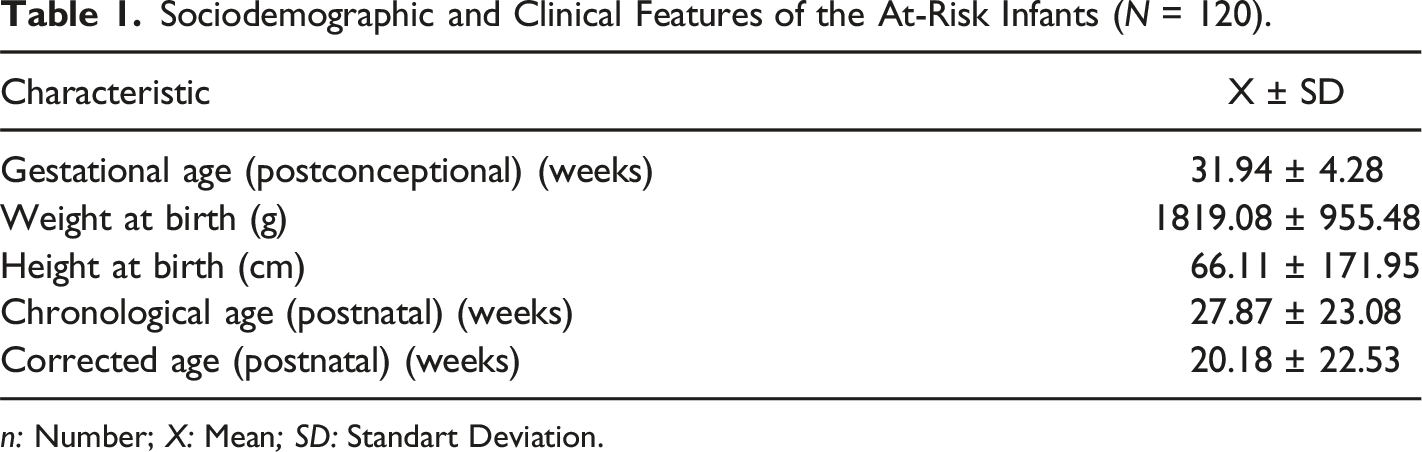
n: Number; X: Mean; SD: Standart Deviation.
Gender and Risk Features of the At-Risk Infants (N = 120).
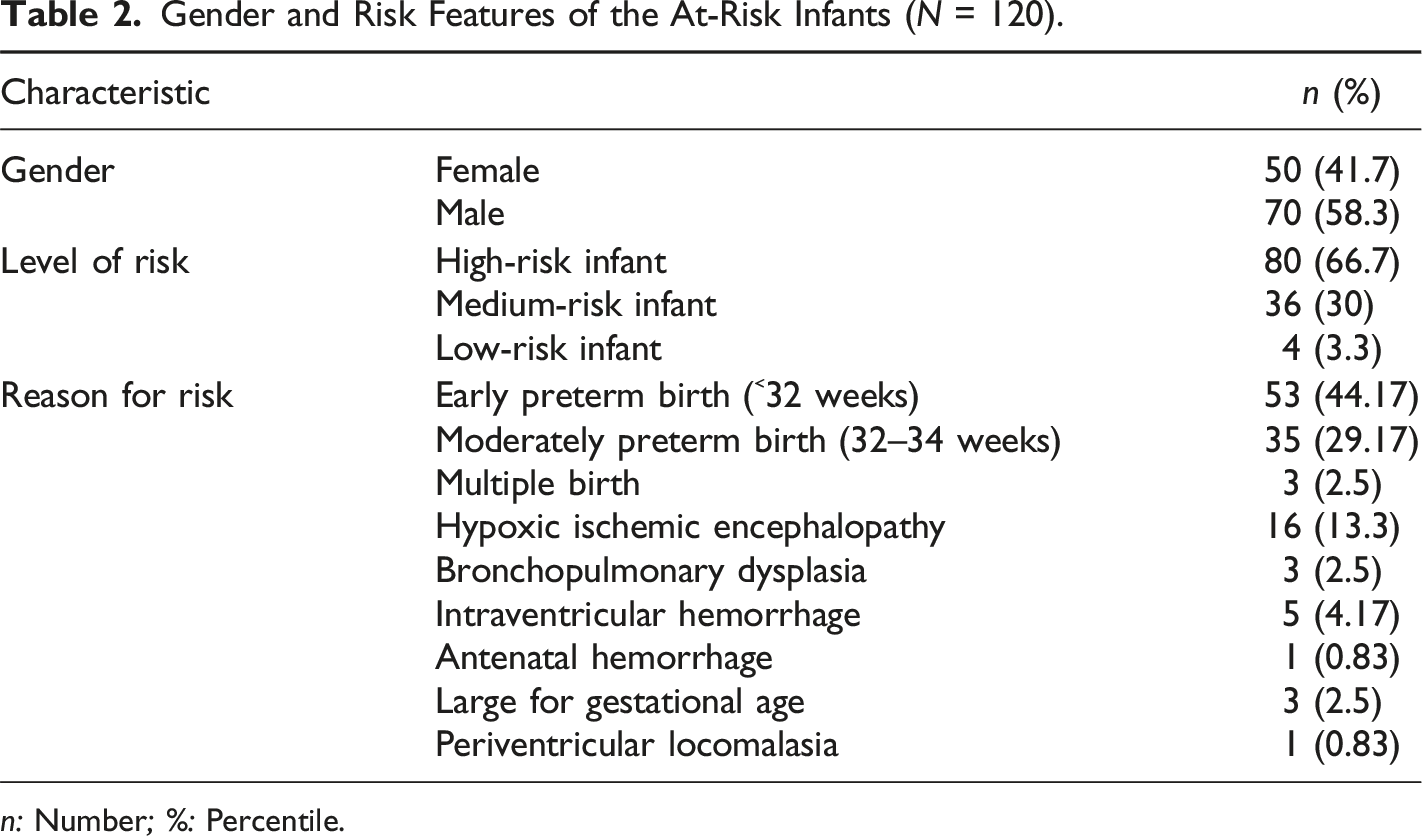
n: Number; %: Percentile.
Internal Consistency of the PDMS-2
Explanatory Factor Analysis for the PDMS-2 (n = 120).
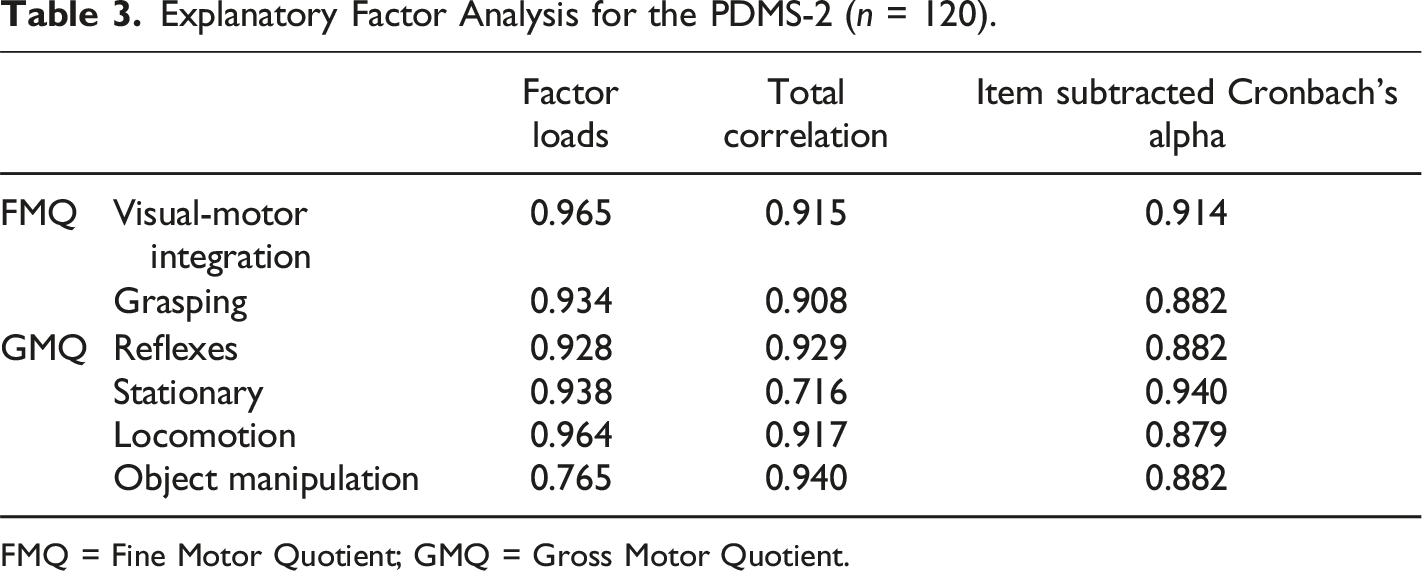
FMQ = Fine Motor Quotient; GMQ = Gross Motor Quotient.
Reliability of the PDMS-2
Intra-class Correlation Coefficients for the Reliability of the PDMS-2 (n = 120). *p < .05; **p < .01.
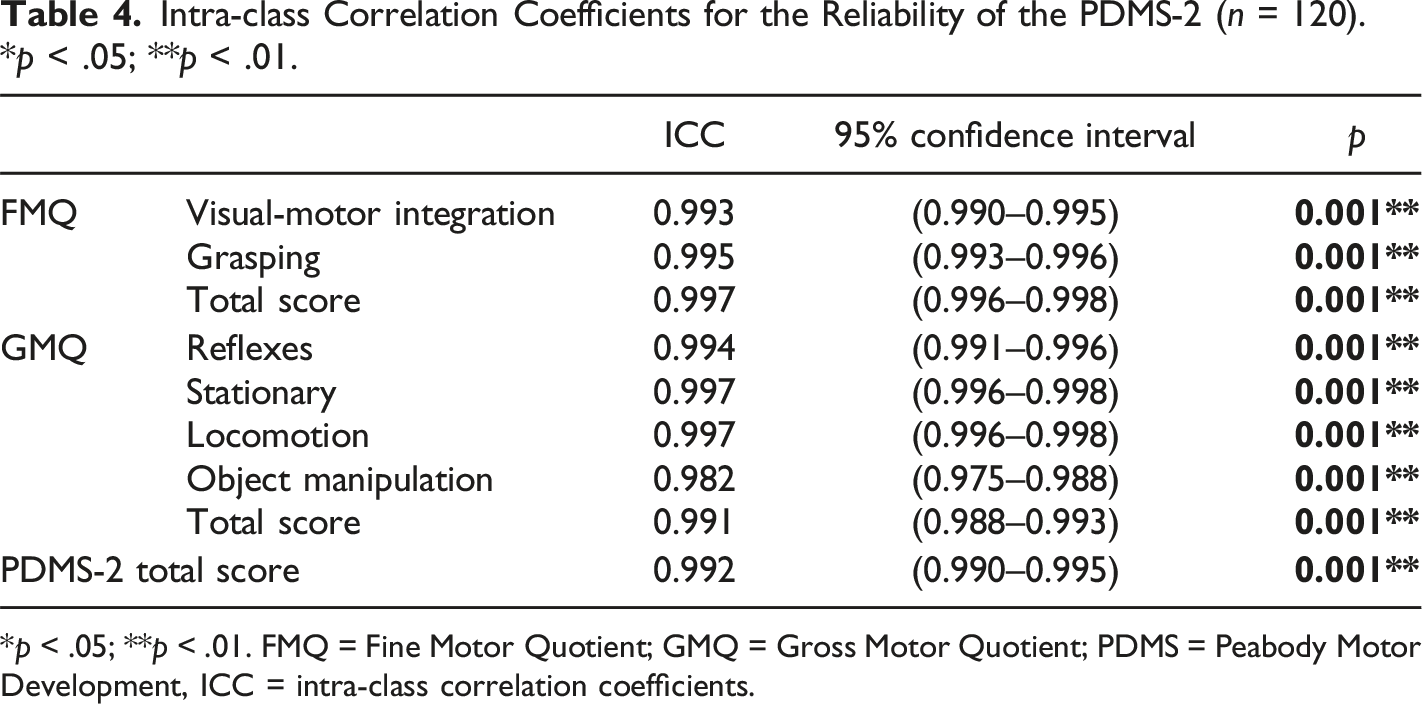
*p < .05; **p < .01. FMQ = Fine Motor Quotient; GMQ = Gross Motor Quotient; PDMS = Peabody Motor Development, ICC = intra-class correlation coefficients.
Validity of the PDMS-2
Cross-Cultural and Content Validity
The translation process was completed without any difficulties. All translations were examined by the expert committee (eight academicians; pediatric neurologist, pediatrician, physiotherapist, and English lecturer) and it was confirmed that semantic, idiomatic, experiential, and conceptual equivalence between the Turkish and English versions was appropriate.
Content validity was assessed by considering both the perspectives of clinical educators. Each item was scored and the content validity index (CVI) was found to have the maximum value (1.00). Therefore, no changes were made to the items and it was decided that PDMS-2 could be applied (Polit et al., 2007).
Construct Validity
Results of Confirmatory Factor Analysis.
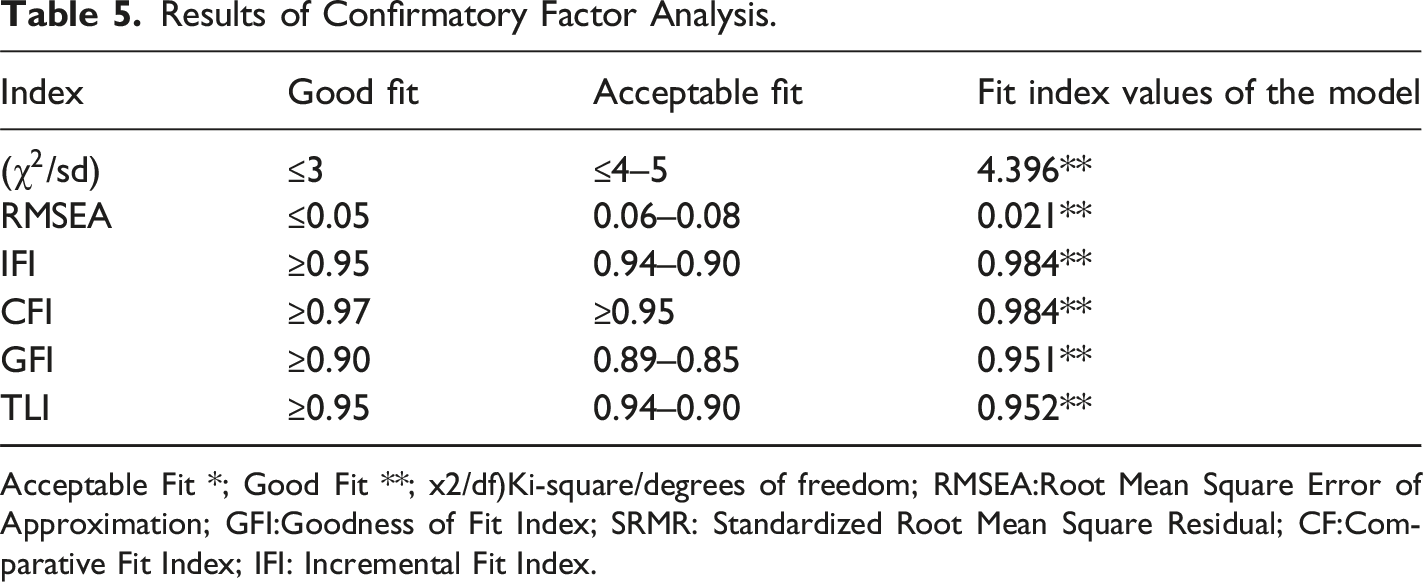
Acceptable Fit *; Good Fit **; x2/df)Ki-square/degrees of freedom; RMSEA:Root Mean Square Error of Approximation; GFI:Goodness of Fit Index; SRMR: Standardized Root Mean Square Residual; CF:Comparative Fit Index; IFI: Incremental Fit Index.
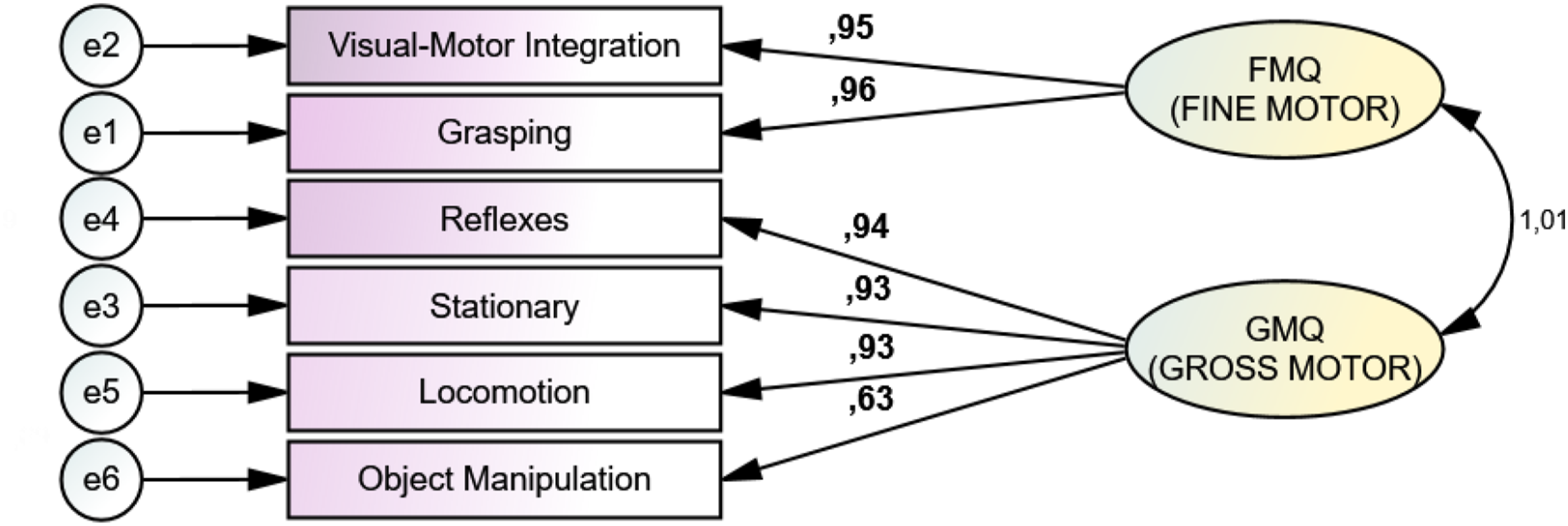
PDMS-2 model.
Interdimensional Relationships for the PDMS-2 (n = 120).
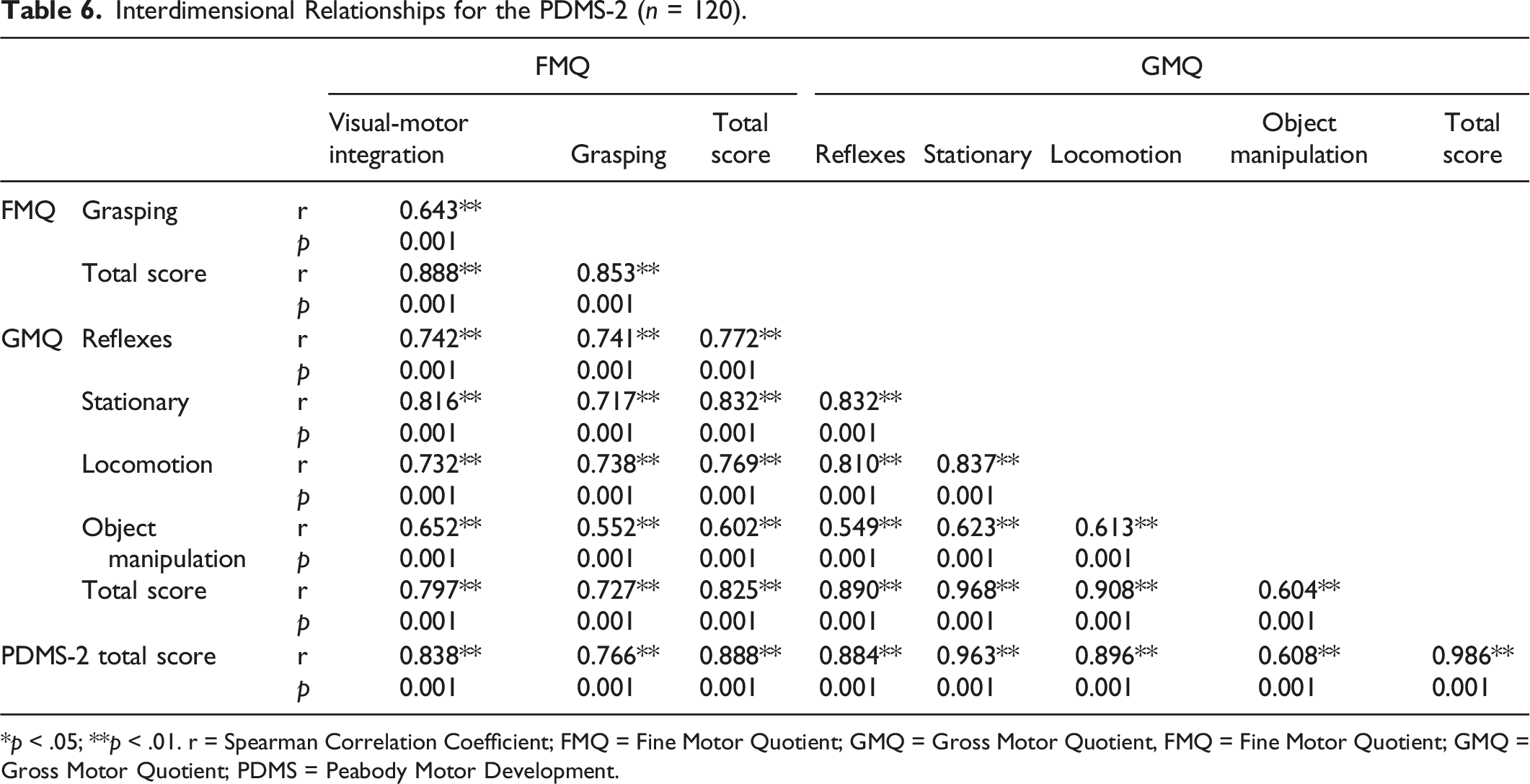
*p < .05; **p < .01. r = Spearman Correlation Coefficient; FMQ = Fine Motor Quotient; GMQ = Gross Motor Quotient, FMQ = Fine Motor Quotient; GMQ = Gross Motor Quotient; PDMS = Peabody Motor Development.
Effects of Subdimensions on the PDMS-2.
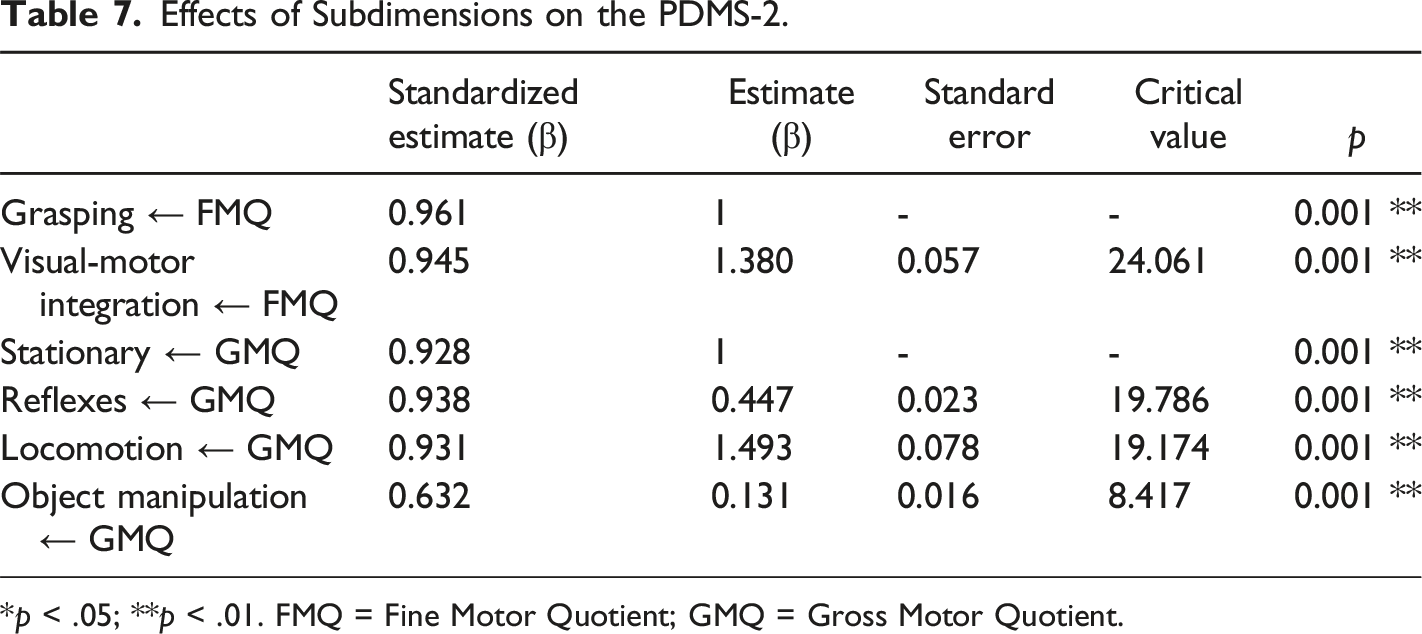
*p < .05; **p < .01. FMQ = Fine Motor Quotient; GMQ = Gross Motor Quotient.
Concurrent Validity
Correlations Between PDMS-2 and HINE and AIMS Scales.
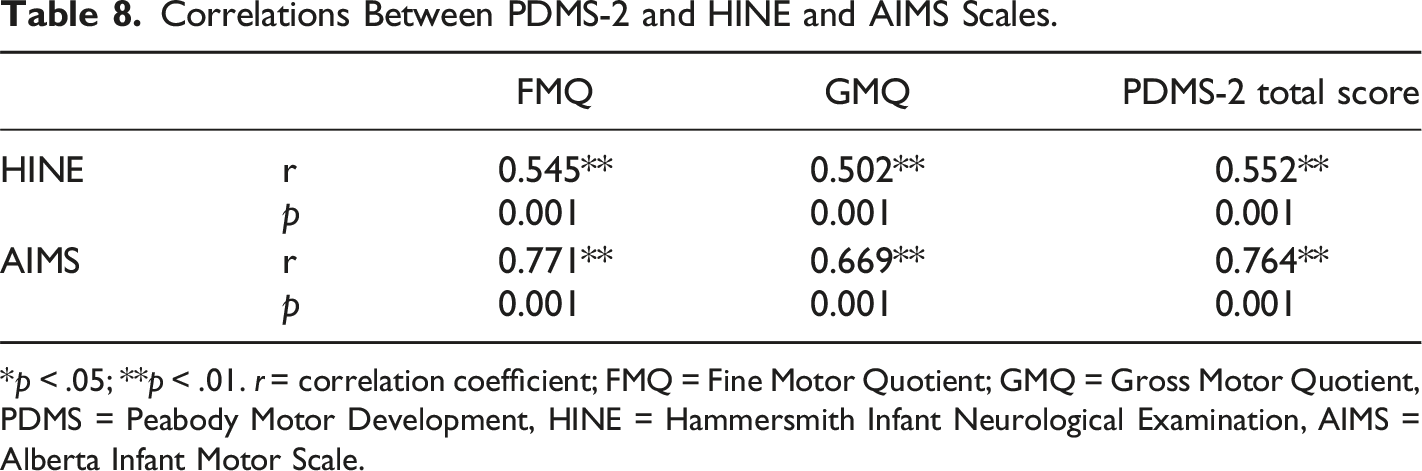
*p < .05; **p < .01. r = correlation coefficient; FMQ = Fine Motor Quotient; GMQ = Gross Motor Quotient, PDMS = Peabody Motor Development, HINE = Hammersmith Infant Neurological Examination, AIMS = Alberta Infant Motor Scale.
Discussion
Early evaluation of high-risk infants in follow-up clinics is very important for their development, and valid and reliable scales should be used for evaluation. This study was conducted to determine whether PDMS-2 is a valid and reliable measurement method for Turkish children aged 0–24 months. The findings of our study show that the PDMS-2 is a valid and discriminating measure for determining the motor competence of zero to 24-month-old Turkish at-risk infants.
The acceptability of the PDMS-2 is due in part to its compound structure, which allows a multidimensional interpretation of motor development. The test consists of six motor subtests: reflexes, stationary, locomotion, object manipulation, grasping, and visual-motor integration. These subtests allow the estimation of three general motor performance indices, referred to as composites: the FMQ, GMQ, and TMQ. The empirical evidence of its validity and reliability is detailed in the PDMS-2 testing manual (Fraga-Sousa et al., 2016). Tavasoli et al. made a study that assess motor development of low birth weight preterm infants with PDMS-2 and found that it can be used in clinical settings for assessing motor development in low birth weight infants (Tavasoli et al., 2014). Similarly in our study we found PDMS-2 also a useful tool for assesing motor development in at-risk infants like preterm infants, hypoxic ıschemic encephalopathy etc. Also we can conclude that the translated Turkish version of PDMS-2 is understandable or applicable for clinical practice.
In our study, factor loadings of the subdimensions of the PDMS-2 were found to be sufficient, as the Cronbach’s α was greater than 0.70 (α = 0.865). Thus, the two subdimensions of the PDMS-2 measure separate features. The questionnaire we created according to these results is a reliable measurement tool. In our scale, the total correlation values of the dimensions range from 0.716 to 0.940, and there is no need to make any reduction in dimensions in the PDMS-2.
The Kaiser–Meyer–Olkin (KMO) test evaluates whether the distribution is sufficient for factor analysis, and the range of 0.80–0.90 is considered to be very good (Ibrahim et al., 2011). Thus, it can be said that the KMO value in this study is at a very good level. The result of the Barlett test was found to be 1051.70 (p < .05). This measurement shows that the variable we created is multivariate in the universe parameter. In this study, no limitation was placed on the number of factors, and factors with an eigenvalue of 1 or >1 were accepted as important factors (Büyüköztürk, 2002). Considering that variance rates that range from 40% to 60% are considered ideal in factor analysis (Scherer, 1988), it can be said that the amount of variance obtained in this study is sufficient.
Internal consistency coefficients were evaluated for two subdimensions and three measurements for the total score obtained in our study. As a result of these evaluations, measurements made at different times show a high similarity in size. Internal consistency results showed sufficient reliability for the GMQ and FMQ subscales and TMQ for the zero to 24-month-old infant group formed according to the PDMS-2 task structures. The PDMS-2, which consists of two subsections, was found to have good internal consistency as a result of our study. All interitem correlations were positive and significant. The coefficients also showed that excluding any item would not change the internal consistency. Tavasoli et al. reported that the internal consistency of the PDMS-2 was high in their study for evaluating the motor development of low-birth-weight preterm infants. In conclusion, the Turkish version of the PDMS-2 is reliable both within and between raters (Tavasoli et al., 2014).
The construct validity of the PDMS-2 was acceptable (p < .05). The model fit of the scale is given in the findings of our study. There are four dimensions of the PDMS-2 in the model (χ2 = 21.982, df = 5, p < .001). As a result of confirmatory factor analysis, factor loadings were found to be at an acceptable level, which demonstrates that the PDMS-2 is suitable for Turkish culture. Results of the confirmatory factor analysis regarding construct validity support the two-factor structure of the original scale. In general, when it is shown to be important in large samples, the chi-square ratio to degrees of freedom and fit indices is a method used to determine fit (Revelle & Zinbarg, 2009).
After examining the findings of our study, we found the factor loadings to be acceptable. The fit index values obtained as a result of confirmatory factor analysis showed that the model was in good agreement (Topuz et al., 2011). In other words, each factor accurately represents the questions that compose it. Our results are in line with the studies conducted in American, Brazilian, and Portuguese children (Folio & Fewell, 2000; Saraiva et al., 2011; Zanella et al., 2021).
In our study, the HINE and AIMS questionnaires, which are known to be valid and reliable, were used to evaluate concurrent validity. We used these items because they are widely used and most known test batteries in the literature. We found a positive, weak to highly significant correlation between all PDMS-2 scale subtests and the HINE and AIMS. Upon examing the levels of these relations, it is seen that they vary between 0.502 and 0.771. Büyüköztürk et al. defined the correlation coefficient as an absolute value between 0.70 and 1.00 as a high-level correlation, between 0.70 and 0.30 as a medium-level correlation, and between 0.30 and 0.00 as a low-level correlation (Büyüköztürk, 2002). Based on this definition, it can be said that the values obtained as a result of the analysis are at medium and high levels. These results show that the Turkish version of the PDMS-2 scale is valid.
The limitation of this study was may be the intrarater reliability the time interval of one day between the two measurements to prevent recall might be too short and should be discussed and might contribute to the high ICCs found in this study.
Infant neurodevelopmental assessments serve dual purposes. Initially, they focus on evaluating the current developmental state of the infant. Understanding the infant’s present condition enables professionals to educate caregivers about their child’s attributes and offer guidance on fostering their development, whether through professional early intervention or other means. Additionally, these assessments are utilized to anticipate and identify potential developmental disorders in at-risk population (Bosanquet et al., 2013; Novak et al., 2017). In this study, of the PDMS-2 evaluated neuromotor development very well parallel with other test batteries HINE and AIMS. These results shows that of the PDMS-2 can be used in clinics for early evaluation of at-risk infants and enable earlier interventions and improved outcomes of the infants in Turkish population.
The limitation of this study was we lack of evaluating effects of clinical sociodemographic factors of the infants on neuromotor development. Interaction effects of gender, level of risk of the infants and sociodemographic factors were not investigated, which might have affected the results. Further studies could determine if clinical properties and the sociodemographic factors of the infants may affected the neuromotor development that assessed with the of the PDMS-2.
Conclusion
Overall, this study demonstrated the reliability and discriminative validity of the Turkish version of the of the PDMS-2. The Turkish version of the of the PDMS-2 was a valid and reliable tool and we think that the Turkish version of the of the PDMS-2 will be a valuable tool in clinics as it is a fast and effective method for evaluating the neurodevelopment of infants at-risk in Turkish population. The PDMS-2 is a usable scale because it evaluates both fine and gross motor in detail and covers the first 24 months. The translation and adaptation process based on international guidelines and inclusion of a large sample size with a wide age range are the strength of this study. Furthermore, the participants were recruited from several centres from different cities in Turkey, and this might positively influence the generalisability of the scale. In clinical settings, the Turkish version of the of the PDMS-2 can be employed to assess the neurodevelopment of at-risk infants. This assessment provides insights into neuromotor outcomes, guiding professionals in determining suitable intervention methods and facilitating early intervention efforts.
Footnotes
Acknowledgments
The authors thank to the familiy of the infants contributed to this study.
Author Contributions
BY data collection, design literature review writing, NCB design, supervision writing, data collection; HG data collection, design literatüre review writing; SU data collection design literatüre review writing; SNK data collection design literatüre review writing, MD analysis interpretion
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author’s Note
All authors have agreed upon the content of the article and the order of authorship. The manuscript has not submitted or published somewhere else.