
Abstract
Objective
While it is known that there is a close connection between motor skills and neurocognitive functions. Attention Deficit Hyperactivity Disorder (ADHD), one of the most common childhood disorders, has not been adequately evaluated. This study aimed to assess motor skills and neurocognitive functions in children with ADHD, and to examine the relationship between these functions in comparison to healthy controls.
Method
This case-control study was conducted who were diagnosed with ADHD (n = 55) and age and sex matched healthy controls (n = 57). The sociodemographic characteristics of the participants were collected using a descriptive information form. The Movement Assessment Battery for Children- Second Edition (MABC-2) was used to evaluate motor skills, while the Central Nervous System Vital Signs (CNSVS) computer-based test battery was used to assess neurocognitive functions.
Results
The scores on neurocognitive components were significantly lower in the ADHD group (p < 0.05). Children with ADHD had lower MABC-2 total scores and average balance subcomponent scores compared to healthy children (p < 0.05). Additionally, the weak positive correlations between MABC-2 scores and neurocognitive functions observed in the control group were not present in the ADHD group.
Conclusion
The results of our study suggest that children with ADHD have significantly more difficulties with motor skills and neurocognitive functions than their healthy controls. This highlights the need for a comprehensive assessment of children with ADHD.
Keywords
Introduction
Attention deficit hyperactivity disorder (ADHD) is a common neurodevelopmental childhood disorder, characterized by hyperactivity, impulsivity and behavioral distraction (Hotham et al. (2018); Kao et al. (2025)). While the prevalence of children with ADHD worldwide is around 3.0 − 7.0%, a study conducted in Turkey found it to be as high as 8.0% (Ayaz et al. (2013); Zorlu et al. (2020)). Neuroimaging studies have reported abnormalities characterized by a decrease in the volume of the prefrontal cortex, caudate nucleus, globus pallidus, anterior cingulate, and cerebellum in children with ADHD (Castellanos et al. (2001); Noordermeer et al. (2017)). Neurocognitive functions including attention, memory, processing speed, psychomotor skills, visuo-spatial skills, and language skills are common problems in ADHD. The term neurocognitive functions is used in this study instead of cognitive functions to emphasize the neural basis of cognitive processes. The literature indicates that neurocognitive functions are managed in the prefrontal parts of the frontal lobe, which has multiple neuronal connections to the cortical and subcortical regions and brainstem (Castellanos et al. (2001); Sutcubasi et al. (2020)).
Neurocognitive dysfunctions observed in children with ADHD (Brown (2008); Pennington and Ozonoff (1996); So and Hong (2025)) and its change with treatment (Ince et al. (2015); Inci et al. (2022)) are receiving increasing attention in the literature. These dysfunctions have been reported to be associated with developmental and functional differences in frontal networks, primarily the prefrontal cortex (Berenguer et al. (2018); Emond et al. (2009); Jones and Graff-Radford (2021); Miklós et al. (2020); Stuss and Benson (1984); Willcutt et al. (2005)).
It is known that 30 − 70% of children with ADHD have problems with motor skills and these problems negatively affect daily living activities of children (Fliers et al. (2009); Kooistra et al. (2005); Şahan et al. (2023); Tseng et al. (2004)). Children with ADHD have more difficulty than their peers during activities that require gross and fine motor skills. It has been reported in many studies that children with ADHD experience significantly more problems in motor skills such as posture, balance, gross and fine motor skills compared to their healthy peers (Fliers et al. (2009); Goulardins et al. (2013); Rosa Neto et al. (2015)).
In a limited number of studies evaluating motor skills and neurocognitive functions, it has been shown that motor skills are associated with neurocognitive functions such as processing speed, working memory, and academic skills (Fliers et al. (2009); Goulardins et al. (2013); Rosa Neto et al. (2015); Çak et al., 2018; Fliers et al. (2009); Goulardins et al. (2013); Rosa Neto et al. (2015)). This relationship is explained by the co-activation of the cerebellum and basal ganglia structures, which are responsible for motor activity and the prefrontal cortex, which is associated with cognitive functions during the execution and maintenance of cognitive or motor activities (Çak et al., 2018). However, it is not clear which neurocognitive sub-components are related with sub-domains of the motor skill. Moreover, it remains unclear how this relationship is affected/changed in neurodevelopmental disorders such as ADHD.
Individuals diagnosed with ADHD may experience various difficulties in their daily lives in the areas of attention regulation, executive functions, and behaviour control. These difficulties are thought to negatively affect functional performance in areas such as academic and occupational functioning, the maintenance of daily tasks, and social interactions (Ahlström and Wentz (2014); Asonitou et al. (2025); Harpin (2005); Sjöwall and Thorell (2022)). The combined assessment of motor and neurocognitive functions may contribute to a more comprehensive understanding of functional impairment in ADHD. In this context, it is important that our study examines motor and neurocognitive functions and the relationship between these functions.
Our study aims to determine the relationship between motor skills and neurocognitive functions by assessing the motor skills and neurocognitive functions of children with ADHD. In this context, the objective examination of the relationship between motor skill subcomponents and neurocognitive subcomponents in the clinical assessment processes of children with ADHD is of great importance for the planning of early intervention programmes. This clinical case-control study is expected to shed light on future intervention studies in this field. In this regard, it has been hypothesized that the relationships between motor skill subcomponents and neurocognitive function subcomponents in children diagnosed with ADHD are more pronounced compared to the healthy control group.
Method
The sample of this case-control study consisted of children aged 8–10 who were diagnosed with ADHD at a pediatric psychiatry outpatient clinic and healthy children of similar age and gender attending schools in the same regional area. The study group included 55 children, aged 8–10 years, who were diagnosed with ADHD according to DSM-5 diagnostic criteria based on psychiatric evaluation, had not received any medical treatment in the last 3 months, had no additional psychiatric disorders other than ADHD, and voluntarily participated in the study. The control group included 57 children with matching age and gender, who had not been diagnosed with any psychiatric disorder according to DSM-5 criteria, and had no chronic medical diseases or active drug use. According to the study protocol, data were collected only from children who agreed to participate in the study; no information was recorded for those who declined participation.
Ethical approval was obtained from the Inonu University Health Sciences Non-Interventional Clinical Research Ethics Committee (decision no. 2018/8-16). The parents or legal guardians of all children included in the study were informed about the aims of the study, and written informed consent was obtained.
The sociodemographic characteristics of the participants were determined by a descriptive questionnaire. Age, gender, education level, family type, family socioeconomic level, place of residence, chronic medical conditions, hearing and vision problems, as well as developmental history (delivery type, birth weight, gestational age, walking age, toilet training, etc.) were recorded.
All assessments were performed by researchers trained and experienced in the application of the measurement tools used. Neurocognitive function and clinical assessments were administered by a child psychiatrist, while motor skill assessments (MABC-2) were conducted by a physiotherapist. Both assessors were blinded to each other’s evaluations and did not have access to each other’s results. Assessments were completed for all participants on the same day in a single session lasting approximately 75–90 min. To minimize the potential effects of fatigue on neurocognitive functions, the assessment order was standardized; neurocognitive functions were assessed first, followed by a standard rest break of approximately 5–10 min, and finally motor skills were assessed. Additional rest breaks were provided as needed by the participants.
Screening Instruments
Movement Assessment Battery for Children- Second Edition (MABC-2)
In this study, Movement Assessment Battery for Children- Second Edition (MABC-2) was used to evaluate the motor skills of the participants (Henderson et al. (2007)). The MABC-2 is designed to identify impairments in motor performance in children aged 3 − 16 years and is divided into three age groups (age range 1: 3 − 6 years, age range 2: 7 − 10 years, age range 3: 11 − 16 years). In the current study, the 7 − 10 age band, which is the 2nd age band, was used. MABC-2 evaluates three different items with eight subtests in each age group and consists of two separate parts including a performance test and a checklist. The performance test consists of manual dexterity (three items), aiming and catching (two items) and balance (three items). The control list assesses the child’s motor competence on a 30-item scale and provides information about the child’s motor skill difficulties from the parents’ point of view. In the current study, children’s motor skills were evaluated with performance tests. After the test, the total test score, standard score and percentage value are obtained. According to the MABC-2 guidelines, scoring is done by correcting for age after the test. A three-color traffic light system is also used in the interpretation of the result scores. Accordingly, a percentage score of 5 or less indicates a significant movement disorder (red zone); 6 − 15% indicates those at risk (amber zone); and 16% or more is considered normal (green zone) (Brown and Lalor (2009); Hotham et al. (2018)). MABC-2 has been shown to offer high reliability and validity in identifying motor coordination difficulties, with levels of 0.88–0.99 for the subtests and 0.97 for the total score (Denysschen et al. (2026); Griffiths et al. (2018)).
The Central Nervous System Vital Signs (CNSVS)
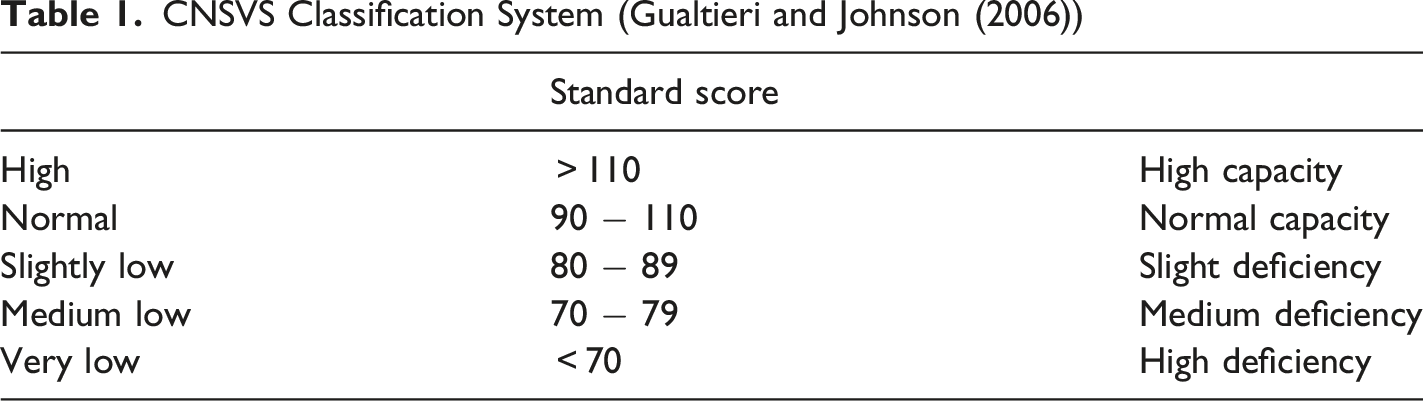
CNSVS Classification System (Gualtieri and Johnson (2006))
Turgay DSM-IV-Based Screening and Evaluation Scale for Attention Deficit and Disruptive Behavior Disorders.
The scale developed on the basis of DSM-IV includes 9 items for attention deficit, 6 items for hyperactivity, 3 items for impulsivity, 8 items for oppositional defiant disorder, and 15 items for conduct disorder (Turgay (1994)). The scale was created in line with the DSM-IV diagnostic criteria and can be filled in by the children’s parents and teachers. The items are answered on a 4 Likert scale where 0 = none, 1 = some, 2 = much, 3 = very much. The validity and reliability study of the scale was performed by Ercan et al. (2001). In this study, the scale was used to evaluate the diagnosis of ADHD and to determine the subtypes. Due to the limited number of cases in other subgroups, only combined type ADHD patients were included in the study.
Statistical Analysis
The data were evaluated by using the Statistical Package for Social Sciences (SPSS) 22.0 package program. Conformity to the normal distribution was tested by using visual (histogram and probability plots) and analytical methods (Shapiro-Wilk Test). Variables determined by measurement were expressed as mean ± standard deviation (X ± SD) and variables determined by counting were expressed by number (n) and percentages (%). Pearson Chi-Square test was used to evaluate categorical variables. The Significance of Difference Between Two Means Test was used to compare independent paired groups. The relationship between the measurement values was evaluated by using the Pearson Correlation Analysis method.
The correlation coefficients are criteria that give information about the strength (degree) and direction of the relationship between the variables and range between −1 and +1. The signs indicate the direction of the relationship. The strength of the relationship increases as it approaches −1 and +1, and decreases as it approaches 0. In the evaluation of the findings, values between 0.00 and 0.19 were interpreted as no relationship (negligible low correlation), 0.20 − 0.39 as weak relationship, 0.40 − 0.69 as moderate relationship, 0.70 − 0.89 as strong relationship, and those between 0.90 and 1.00 were interpreted as very strong relationship (Alpar (2012)).
Results
Sociodemographic Characteristics of the Participants
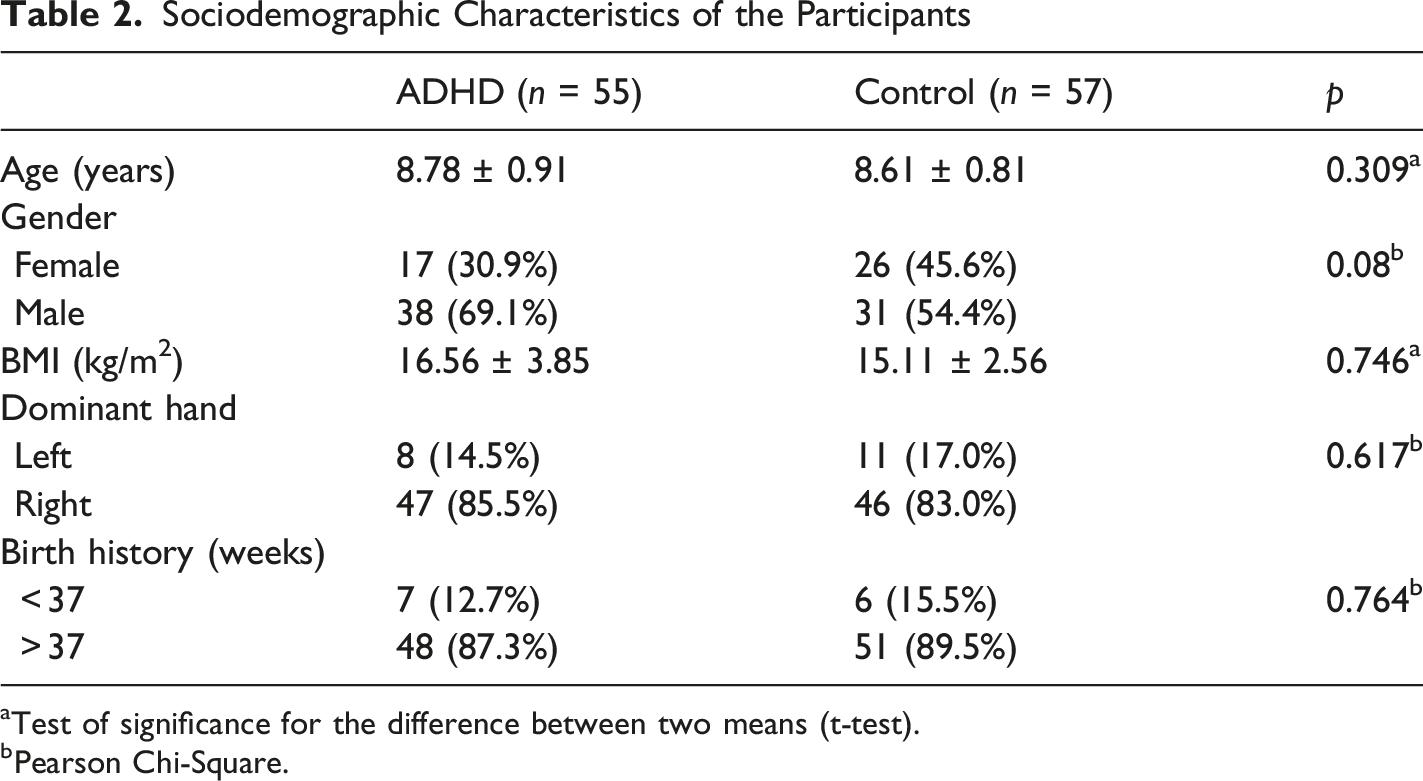
aTest of significance for the difference between two means (t-test).
bPearson Chi-Square.
Evaluation of Neurocognitive Functions
Neurocognitive Characteristics of the Participants
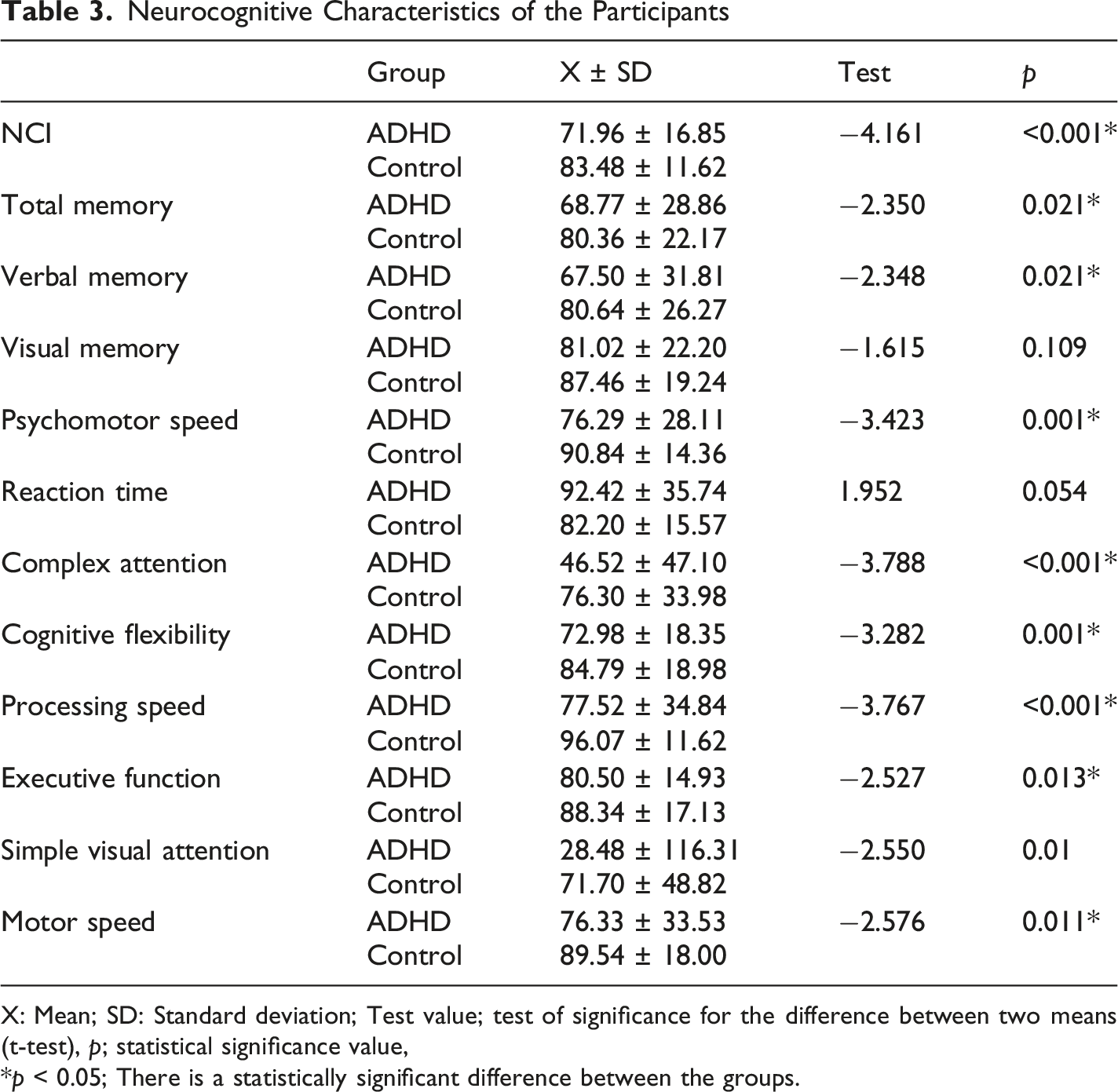
X: Mean; SD: Standard deviation; Test value; test of significance for the difference between two means (t-test), p; statistical significance value,
*p < 0.05; There is a statistically significant difference between the groups.
Assessment of Motor Skill
Comparison of MABC-2 Scale Scores
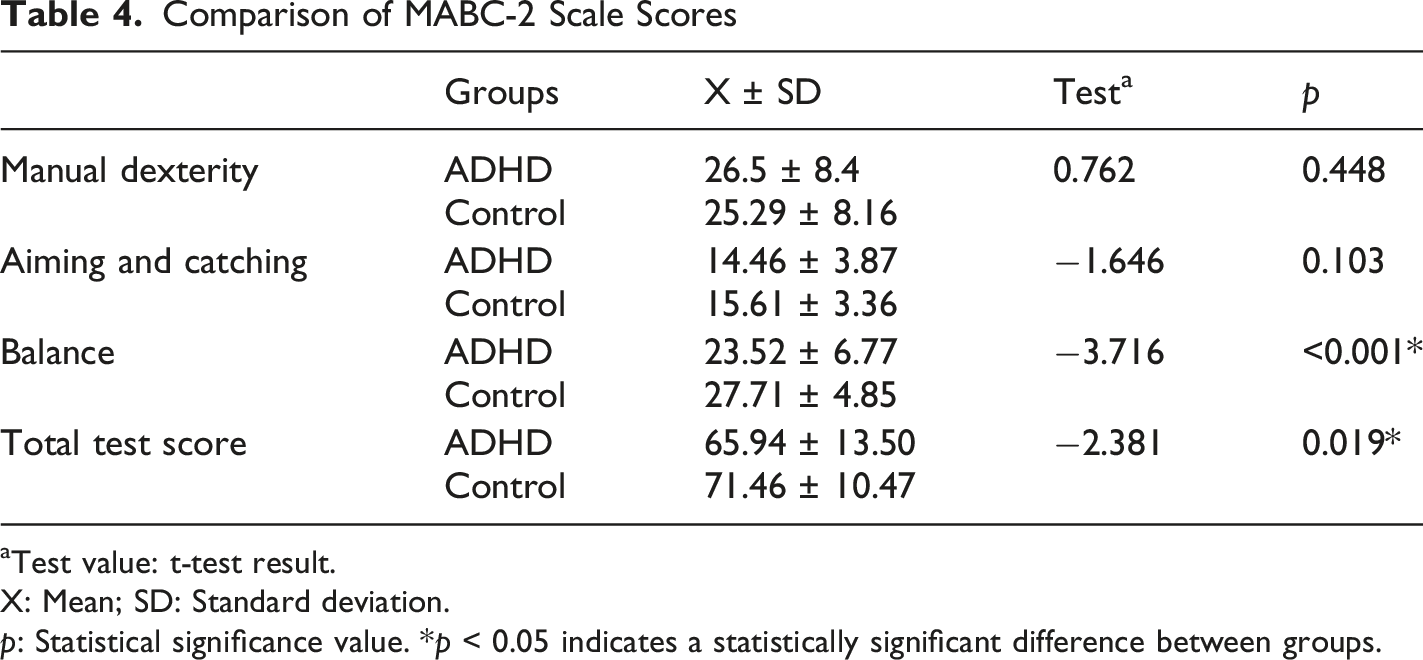
aTest value: t-test result.
X: Mean; SD: Standard deviation.
p: Statistical significance value. *p < 0.05 indicates a statistically significant difference between groups.
When the MABC-2 scores were evaluated according to the traffic light system, the number of cases in the red zone (movement disorder) was found to be 13 (23.64%) in the ADHD group and 5 (8.78%) in the control group. The cases in the yellow zone (under risk) were found to be 10 (18.18%) in the ADHD group and 9 (15.79%) in the control group.
Evaluation of the Relationship Between Motor Skills and Neurocognitive Functions
The Relationship Between Motor Skills and Neurocognitive Characteristics of ADHD and Control Groups
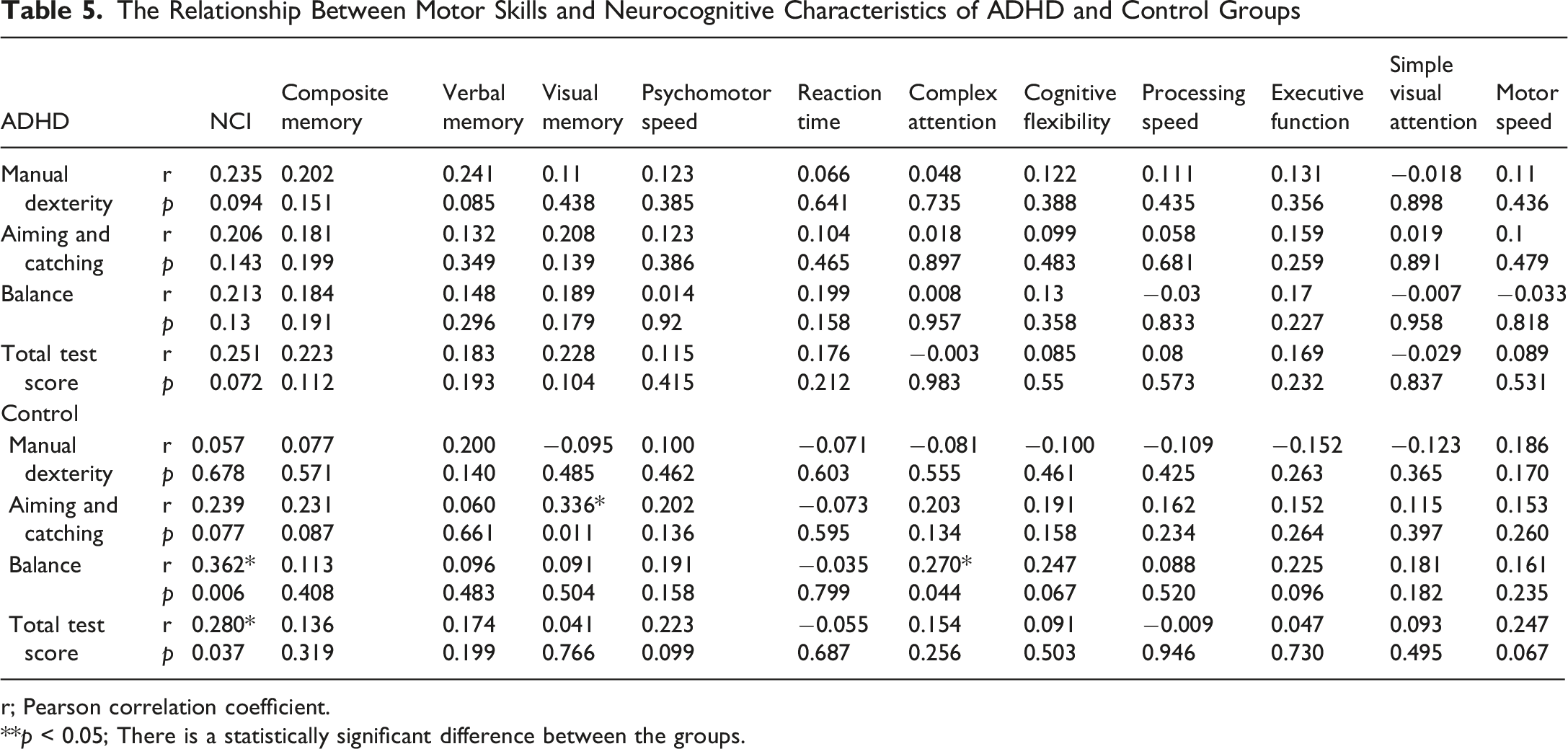
r; Pearson correlation coefficient.
**p < 0.05; There is a statistically significant difference between the groups.
Discussion
In this study, the hypothesis that the relationships between motor skill subcomponents and neurocognitive functions would differ in children diagnosed with ADHD compared to a healthy control group was partially confirmed. The significantly lower neurocognitive scores and MABC-2 total scores, as well as balance subcomponent scores, in the ADHD group compared to the healthy group indicate marked deficits in both motor and neurocognitive domains in these children. However, the absence of the weak positive relationship between motor skills and neurocognitive functions observed in the healthy control group in the ADHD group suggests that the interaction between these two areas may be impaired in ADHD. These findings reveal that motor performance and neurocognitive functions do not always progress in parallel in ADHD. Neurocognitive deficits in children with ADHD have been assessed using various neuropsychological tests, leading to the conclusion that ADHD is one of the neurodevelopmental disorders associated with deficits in neurocognitive functions. In a meta-analysis of 83 studies, Willcutt et al. highlighted that multiple neurocognitive tasks were impaired in children with ADHD, with the most pronounced deficits observed in response inhibition, vigilance, working memory, and planning (Willcutt et al. (2005)).
In our study, we found that neurocognitive functions, including NCI, total memory, verbal memory, psychomotor speed, complex attention, cognitive flexibility, processing speed, simple visual attention, and motor speed, were more impaired in children with ADHD compared to the healthy control group. However, the scores for visual memory and reaction time were similar between the ADHD and control groups.
In a study in which ADHD neurocognitive functions were evaluated by using the CNSVS test battery, the neurocognitive functions of children with ADHD including NCI, total memory, psychomotor speed, reaction time, complex attention, and cognitive flexibility functions were found to be lower in the ADHD group compared to the control group (Yazıcı (2012)). This may be due to the individual characteristics of the patients in the sample group, the relatively younger age group of the children included in the study, and the interregional differences. In addition, the period in which the study was conducted coincides with the Covid-19 pandemic period. It can be suggested that the neurocognitive functions of children in both ADHD and control groups might be affected by the situations experienced in quarantine and isolation conditions. Moreover, the children included in the study had a diagnosis of combined type ADHD. This situation may be associated with further deterioration in neurocognitive functions. It is obvious that there is need for more studies on the subject on both population-based and clinical sample groups.
In many studies, it has been reported that children with ADHD perform worse than healthy children in different areas of fine motor and gross motor skills (Kaiser et al. (2015)). In the literature, it is seen that children with ADHD often have more problems in sub-motor skill components including manual dexterity, aiming and catching, and balance (Brossard-Racine et al. (2012); Goulardins et al. (2017)). In a study using the MABC-2 test battery and evaluating the upper extremity functions of children with ADHD compared to healthy children, the standard scores of manual dexterity and aiming and catching subcomponents were found to be significantly lower in the ADHD group (Hotham et al. (2018)). In our study, the MABC-2 total score and balance subcomponent average scores were found to be lower in children with ADHD compared to healthy children with similar age and gender characteristics; while the manual dexterity and aiming and catching scores were similar. In the literature, it has been stated that the motor problems seen in children with ADHD result from changes characterized by a decrease in the volume of the globus pallidus, anterior cingulate, caudate nucleus, and cerebellum (Noordermeer et al. (2017)). Morphometric and neuroimaging studies on the cerebellum supported this view and suggested that existing motor problems in children with ADHD may be caused by cerebellar changes (Goulardins et al. (2017)). This explains the balance and coordination problems frequently observed in children with ADHD. However, in the literature, unlike our study, it has been reported that the hand functions of children with ADHD are affected (Brossard-Racine et al. (2012); Hotham et al. (2018)). This difference may be due to differences in the characteristics of the sample groups and the evaluation tools.
In the literature, the relationship between neurocognitive functions and motor skills has been investigated in a limited number of studies. In our country, Cak et al. investigated the relationship between motor skills and cognitive functions in children aged 8 − 11 years with ADHD, and found that fine motor skills are associated with attention deficits and working memory and processing speed problems (Çak et al., 2018). There are controversial opinions about the relationship between motor skills and neurocognitive functions (Molitor et al. (2015); Wilson et al. (2013)). It has been reported that the cerebellum and basal ganglia associated with motor performance and the prefrontal cortex areas related to neurocognitive functions show joint activation during the execution of neurocognitive and motor activities (Budde et al. (2008); Çak et al., 2018). However, it has not yet been clarified how this relationship is affected in diseases such as ADHD, which is thought to occur with impairments in the neurodevelopmental process. Miklos et al., in their study, referring to this relationship, emphasized that physical activity may have a positive effect on neurocognitive functions and attention performance in children with ADHD, (Miklós et al. (2020)). In our study, we observed that the relationship between motor skills and cognitive functions was significant in the control group but not in the ADHD group. Unlike previous studies, the present study contributes to the literature by employing a case–control design with a healthy comparison group and by evaluating motor and neurocognitive functions at the subcomponent level. This difference may stem from impaired activation mechanisms between common brain areas, which is part of the neurodevelopmental disorders in the ADHD group. However, further studies using objective methods are required to obtain more robust evidence-based results. In daily life, fine motor skill deficits may cause difficulties in tasks such as writing, buttoning, or holding small objects; gross motor deficits may affect walking, balance, and physical participation; these motor requirements may also indirectly challenge attention and memory performance by increasing cognitive load (Piek et al. (2008); van der Fels et al. (2015); Zhou and Tolmie (2024)). In this context, it is important for clinicians to be aware that motor performance can affect not only independent functionality but also performance in cognitive tests. It is recommended that intervention programmes be designed holistically to encompass not only neurocognitive functions but also motor skills, in order to enhance functionality and support cognitive potential in clinical practice. In this context, it is critically important for professionals to address motor and cognitive functions together in their daily assessments and therapy plans.
Conclusion
The results of our study show that children with ADHD have many more problems with motor skills and neurocognitive functions compared to healthy children. Another significant result of our study is that we found that the weak relationship between neurocognitive functions and motor skills deteriorated in children with ADHD, compared to healthy controls. This result suggests that supporting children’s motor skills may play a positive role in the development of cognitive functions in children. We think that these results will shed light on further studies on the subject.
Strengths and Limitations of the Study
Our study has many strengths. First of all, in our study, computer-based tests, which are highly valid and widely used, were used to evaluate the neurocognitive functions of children. Currently, computer-based psychiatric assessments and models are increasingly gaining importance and have been used in different areas (Ucuz et al. (2020; 2022)). Standardized results of the applied test increase the reliability of the data compared to manual tests. The MABC-2 test, which is used to evaluate motor functions, is similarly one of the tests with high validity and widespread use. Another strength of our study is that motor skills and neurocognitive functions were evaluated together. In this context, our study is one of the limited number of studies in the literature.
Our study has limitations as well as strengths. First, a limited age band was used in the study and the mean age of the subjects included in the study was relatively small. This prevents the study results from being generalized to all ADHD patients. Another limitation of our study is that the cases included in the study had a diagnosis of combined type ADHD. This patient group may go with more severe clinical deterioration compared to those with only attention deficit or only hyperactivity-impulsivity and this may result in a further decrease in both neurocognitive function and motor skill scores. Studies with a larger sample, including the subtypes of the disorder and considering the severity of the disease may yield more generalizable results. However, as separate analyses were not conducted for ADHD subtypes in the study, it is unclear to what extent the sample represents all ADHD subtypes. This may limit the generalisability of the findings, particularly with regard to the adult population with ADHD. In this context, it is important to plan future studies with larger samples that take into account ADHD subtypes and disease severity, and that include adult samples.
Footnotes
Acknowledgments
The authors would like to thank all the adolescents and their families who participated in this study.
Author Contributions
FO, IU, MKG and OOO designed and conceptualized the study. IU, FO, OOO interviewed participants and collected data. FO and IU analyzed and interpreted data together. FO and IU drafted the original manuscript. All authors reviewed, revised the manuscript and approved the final manuscript.
Funding
This study was supported by the Scientific Research Unit of Inonu University with the project code TSA-2018-1391 and ID number 1391.
Declaration of Conflicting Interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.