
Abstract
The study aimed to compare limits of stability (LoS) scores and Timed Up and Go test (TUG) times between adults aged between 18-65 years with and without chronic neck pain (CNP) and to determine the associations of pain characteristics with these measures. Forty-five adults with CNP and forty-five asymptomatic controls were included. LoS scores were obtained for eight directions, with each target positioned at 45° intervals, using a stabilometric platform. TUG was performed at a self-selected comfortable speed under two conditions: without a concurrent task and while counting backwards by threes. Groups were compared using the analysis of covariance. Correlations between variables were determined and multiple linear regression was performed to determine whether pain characteristics predict the composite LoS score and TUG time. In the results, adults with CNP exhibited lower LoS scores in all directions except forward and backward and longer TUG times under both conditions (p < 0.05). In both groups, higher LoS scores were correlated with shorter TUG times while counting (p < 0.05), but not with TUG times without a concurrent task (p > 0.05). After adjusting for demographics, pain intensity during neck movements and neck disability explained an additional 29.2% of the variance in the composite LoS score and an additional 15.7% of the variance in TUG time while counting backwards (p < 0.05). Neck disability uniquely predicted both the composite LoS score (β = −0.413) and TUG time while counting (β = 0.391), after adjusting for demographics and pain intensity (p < 0.05). LoS and TUG may be relevant parameters to consider in individuals with CNP, particularly given their association with neck disability.
Introduction
Neck pain is a highly prevalent condition that leads to considerable pain, disability, and economic cost (GBD 2021 Neck Pain Collaborators, 2024). Disturbed sensorimotor control is reported as among the main problems in people with chronic neck pain (CNP), which is caused by the impairment of cervical proprioception (Särkilahti et al., 2024). The cervical spine has a highly sensitive proprioceptive system that contributes significantly to the control of posture and balance (Peng et al., 2021). CNP causes the cervical mechanoreceptors to produce a large number of erroneous sensory signals and subsequently leads to a disturbance of sensorimotor control, such as poorer joint position sense and wider postural sway (Peng et al., 2021; Särkilahti et al., 2024;).
In existing studies investigating balance performance in people with CNP, static standing balance under different sensory conditions was predominantly assessed (Särkilahti et al., 2024). Although relatively few studies investigated dynamic balance in people with CNP using clinical tests such as the Y-Balance Test, Berg Balance Scale, and functional and lateral reach tests, there remains a need for studies using computerized dynamic balance assessment (Alshehri et al., 2025; Gomes et al., 2018; Raizah et al., 2023; Özel Aslıyüce et al., 2022;). Prakash et al. reported that adults aged 18 to 65 years with CNP exhibited higher sway and stability indices while standing on both a fixed and a movable platform, indicating greater postural instability compared to controls (Prakash et al., 2024). On the other hand, the limits of stability (LoS) assessment, one of the most commonly used tests for dynamic balance, provides objective data on an individual’s maximum reach distance, reflecting how far they can shift their center of gravity in different directions without losing balance (Nolff et al., 2024). Alshehri et al. assessed LoS using a stabilometric platform and reported that older adults with CNP exhibited a lower composite LoS score compared to controls (Alshehri et al., 2025). Given that static balance impairments are well-documented in adults aged 18 to 65 years with CNP, it is essential to investigate whether these impairments also extend to their stability limits, as this could further contribute to postural stability deficits.
In addition to numerous studies reporting reduced gait speed in people with CNP (Burton et al., 2023), there are also studies indicating reduced functional mobility performance, assessed with the Timed Up and Go test (TUG), in older adults with CNP (Alshehri et al., 2025; Aslan Telci et al., 2019; Madsalae et al., 2022; Quek et al., 2014; Raizah et al., 2023;). Despite consistent results regarding increased TUG time in older adults with CNP, Gomes et al. reported that TUG time did not significantly differ between young adults with and without CNP (Gomes et al., 2018). Madsalae et al. reported that the TUG with the counting backward by threes task was the most challenging component of the Balance Evaluation Systems Test, which includes clinical stability limits, standing balance, and gait speed tests performed under various conditions, for all groups consisting of young adults without CNP and older adults with and without CNP, followed by the standard TUG (Madsalae et al., 2022). Although no significant impairment was reported in young adults with CNP, we thought that TUG time may be longer in adults aged 18–65 years with CNP. Additionally, adding the counting backward by threes task to the TUG test may further challenge compensation for the performance decline caused by neck pain in this population.
It is obvious that the negative impact of neck pain on dynamic balance and functional mobility becomes more of a concern when combined with the effects of aging. However, beyond aging, additional health issues that may occur in the 18–65 age population could also impair these abilities, making the impact of neck pain an even more critical issue. The primary aim of this study was to compare LoS scores and TUG under single- and dual-task conditions between adults with CNP and asymptomatic controls. The secondary aim was to examine the associations of neck pain characteristics with these measures. It was hypothesized that adults with CNP would exhibit lower LoS scores and longer TUG times under single and dual-task conditions compared to asymptomatic controls, and that greater pain intensity and neck disability would be associated with poorer performance.
Methods
Design
This case-control study was conducted at Izmir Katip Celebi University Ataturk Training and Research Hospital. Ethical approval for this study was obtained from Izmir Katip Celebi University Institutional Non-invasive Research Ethics Board (Number: 0210 - Date: 14.11.2024). All procedures were conducted according to the Declaration of Helsinki. All participants provided written informed consent.
Participants
Forty-five adults with CNP and forty-five asymptomatic adults were included in the study. The required sample size was calculated with G*Power (version 3.1.9.7, Düsseldorf University, Germany) as 90 (45 for each group) for the tail(s) = two, effect size d = 0.699, alpha error probability = 0.05, power = 0.90%, allocation ratio = 1. The effect size (d) was calculated for the composite LoS score from the pilot study which included ten adults with CNP and ten asymptomatic adults. In the pilot study, the composite LoS score was 80.94 ± 13.11 in the neck pain group and 88.4 ± 7.49 in the asymptomatic group.
Individuals presenting with neck pain were screened at the time of their presentation to the Physical Therapy and Rehabilitation outpatient clinic, prior to the initiation of any physiotherapy intervention. Those who met the eligibility criteria were informed about the study, and those who agreed to participate were included and underwent an assessment after providing informed consent.
The inclusion criteria for the neck pain group were as follows: (1) being between 18 and 65 years of age, (2) experiencing neck pain lasting longer than three months, (3) having a score higher than 10/100 on the Neck Disability Index (NDI), and (4) having no neurological deficits resulting from neck disorders. Patients’ companions and hospital staff were included as controls by matching them with participants with CNP in terms of gender, age and body mass index (BMI). The matched control was within both 5 years of the case’s age (age±5years) and 2 kg/m2 of the case’s BMI (BMI±2 kg/m2). The inclusion criteria for the asymptomatic group were as follows: (1) being between 18 and 65 years of age, (2) having no current neck pain, (3) having no history of neck pain lasting longer than three months. The exclusion criteria for both groups were as follows: (1) having a history of spinal pain lasting longer than three months in the thoracic or lumbar region, (2) having current thoracic or lumbar pain, (3) having a history of trauma or surgery in the spine or head regions, (4) having other musculoskeletal problems which may affect balance and gait performance, (5) having been diagnosed with any neurological, vestibular, metabolic, or endocrine disorders.
Assessment of Pain Intensity and Neck Disability
The intensity of neck pain experienced over the past week at rest (while physically immobile and untouched) and during daily tasks requiring neck movements (pain experienced in response to neck movements) was assessed (He et al., 2017). The visual analogue scale (VAS) was used to assess neck pain intensity. Participants were asked to mark the intensity of their pain on the 100 mm line. The VAS pain ranges from 0 to 100. A score of 0 represents no pain while a score of 100 represents the worst imaginable pain. The intensity of neck pain was interpreted as follows: 0-4 mm = no pain, 5-44 mm = mild pain, 45-74 mm = moderate pain, 75-100 mm = severe pain (Jensen, 2003). The NDI was used to assess the disability caused by neck pain through the patient’s self-report. Higher scores indicate greater disability. The NDI was reported to be a valid and reliable method for assessing disability in patients with neck pain (Telci et al., 2009). The NDI scores were interpreted as follows: 0-8% = none, 10-28% = mild disability, 30-48% = moderate disability, 50-68% = severe disability, over 68% = complete disability (Vernon, 2008).
Assessment of Limits of Stability
LoS scores were obtained using a stabilometric platform (Stability-E, Tecnobody, Dalmine, Italy) with a sampling rate of 20 Hz. (Hou et al., 2024; Toprak Celenay et al., 2019;). Participants performed a barefoot double-leg stance on the circular platform, with their feet positioned according to the specific format required by the device, placed parallel to each other and shoulder-width apart, and their arms resting at their sides (Figure 1). For the assessment, participants were asked to look at the computer screen positioned at their eye level and 1 meter away from the center of the platform. On the screen, eight targets positioned at 45° intervals around the center were indicated by eight boxes, and the center of pressure of the person on the platform was represented by a dot. Participants were then instructed to reach toward each of the eight on-screen targets by shifting their body weight in the direction of the target as quickly as possible without lifting or moving their feet. If participants were unable to reach a target, they were instructed to lean as far as possible in the direction of the target. The sequence of the targets was randomized by the device, and participants moved the dot toward the flashing target and then returned to the center before proceeding to the next target. The test ended when participants completed all eight targets. The time taken to complete the test and the percentage of how much participants reached each of the eight targets were calculated by the device’s software (Figure 1). Before the assessment, the procedure was explained to all participants, and they all practiced the entire test procedure once. From left to right: feet placement on the stabilometric platform and the limits of stability test result screen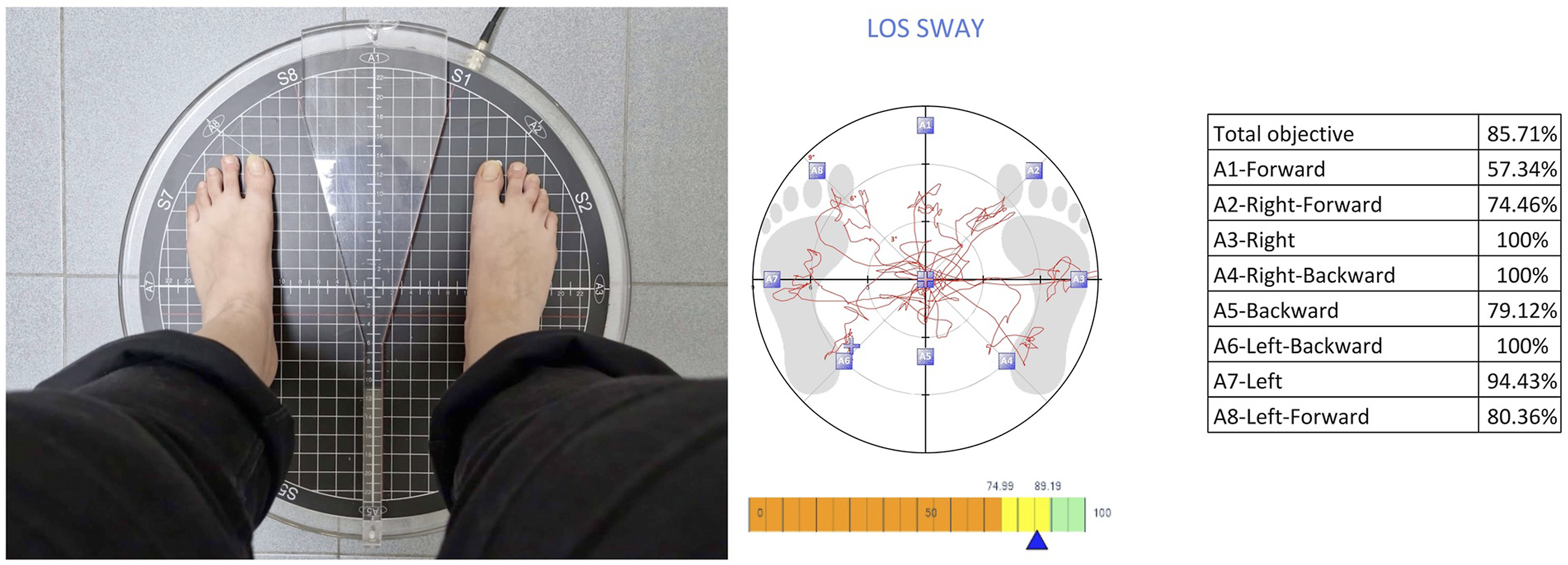
Assessment of Functional Mobility
TUG was used to assess functional mobility performance with and without a concurrent task (Christopher et al., 2021). The test was performed barefoot by all participants. A 3-m walkway was marked on the floor, with a chair at the starting point. Participants were instructed to (1) stand up from the standard chair, (2) walk 3 meters at a comfortable speed to the marked point on the floor, (3) turn, and (4) return to the chair to sit down. No specific instructions were provided regarding how to turn. The total time taken to complete the TUG test was measured using a stopwatch with a precision of 1/100 seconds. The TUG test was performed at a self-selected comfortable speed under two conditions: first, without a concurrent task, and second, while counting backwards by threes from a random number between 100 and 200. In the concurrent cognitive task condition, no instructions were given on which task to prioritise. The total number of counts as well as the number of correct counts were recorded. Each condition was repeated three times, and the scores were averaged. Lower TUG times represent better functional mobility.
Statistical Analyses
The statistical analysis was performed using SPSS 25. Shapiro-Wilk test, along with descriptive statistics, showed that all data had a normal distribution except for pain duration. A log10 transformation was applied to normalize the pain duration data. Analysis of covariance (ANCOVA) was performed to compare the groups, with the LoS scores and TUG times as the dependent variables, group as the independent variable, and age and BMI as covariates. Although groups were matched based on age and BMI within defined tolerances, perfect matching is rarely achievable. Therefore, age and BMI were included as covariates in ANCOVA to statistically control for residual confounding and enhance the precision of group comparisons (Pearce, 2016). Effect sizes for ANCOVA were reported using partial eta squared (η2p), with values interpreted as follows: 0.01 indicates a small effect, 0.06 a medium effect, and 0.14 a large effect (Fritz et al., 2012). Furthermore, Pearson correlation coefficients were calculated to determine the relationships between LoS scores and TUG times in both groups and the relationships between LoS scores, TUG times, and pain characteristics including pain duration, pain intensity at rest, pain intensity during neck movements, and neck disability in the neck pain group. Statistically significant correlation coefficients were interpreted as follows: correlation coefficients (r-values) less than 0.10 indicate negligible correlation, coefficients between 0.10 and 0.39 indicate weak correlation, coefficients between 0.40 and 0.69 indicate moderate correlation, coefficients between 0.70 and 0.89 indicate strong correlation, and coefficients between 0.90 and 1.00 indicate very strong correlation (Schober & Schwarte, 2018). Subsequently, multiple regression analysis was conducted to determine whether pain characteristics that were significantly correlated with the composite LoS score and the TUG score also predicted these scores. To control for their interaction with other factors, demographic characteristics, including age, body mass index (BMI), and gender were entered in Step 1. In Step 2, pain intensity and neck disability were included. The level of significance was set at p < 0.05.
Results
Demographic and Pain Characteristics of Participants
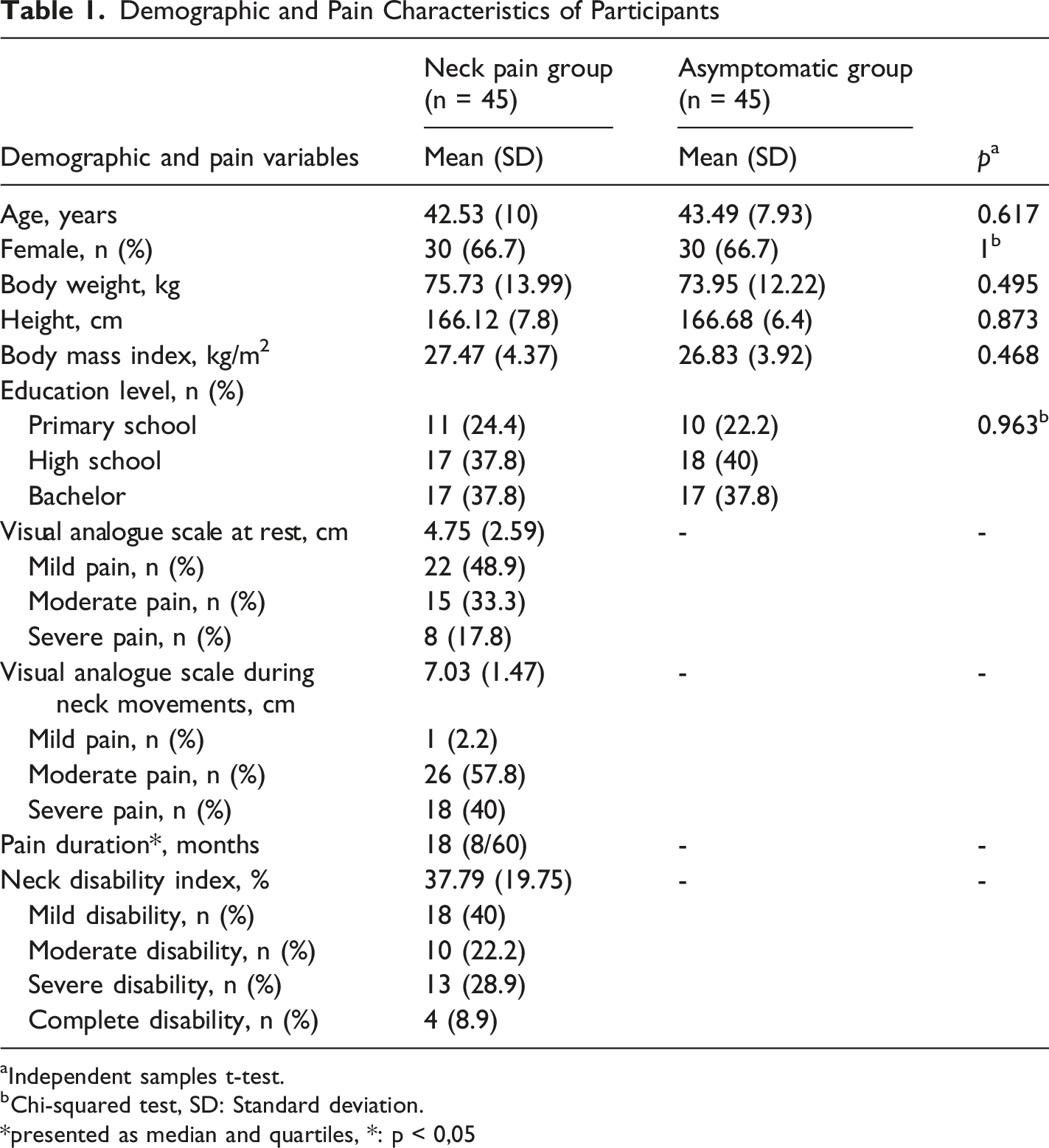
aIndependent samples t-test.
bChi-squared test, SD: Standard deviation.
*presented as median and quartiles, *: p < 0,05
Comparison of Age- and BMI-Adjusted Limits of Stability and Functional Mobility Between Groups
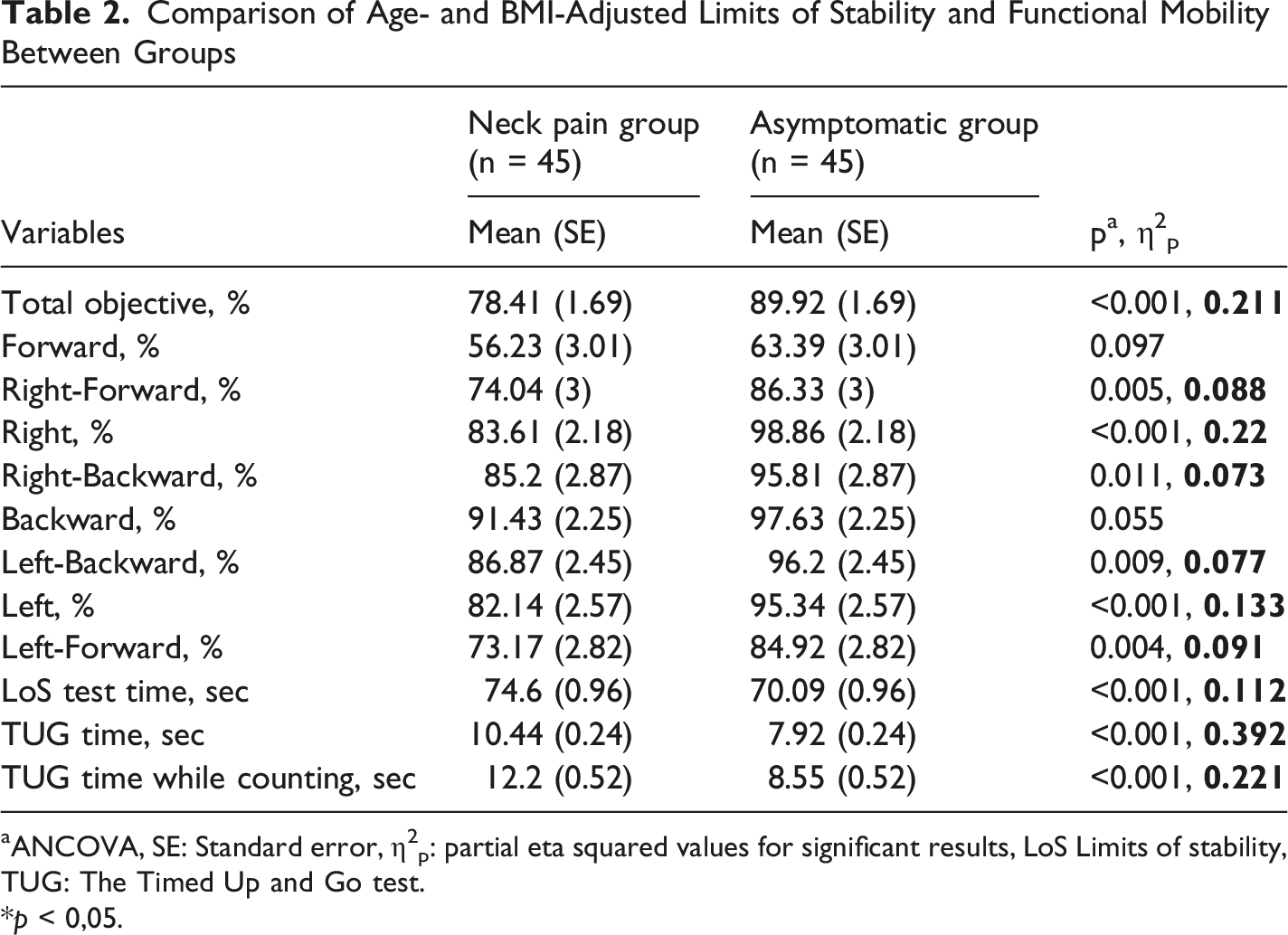
aANCOVA, SE: Standard error, η2p: partial eta squared values for significant results, LoS Limits of stability, TUG: The Timed Up and Go test.
*p < 0,05.
No significant difference was found between the groups in the number and percentage of correct responses (p > 0.05). The mean number of correct responses was 12.9 ± 5.4 in the neck pain group and 13.3 ± 5.2 in controls. The percentage of correct responses was 88.7% ± 16.3 in the neck pain group and 90.6% ± 9.8 in controls. Adults with CNP required more time to complete the TUG both with and without the counting task, with large effect sizes η2p = 0.39 and 0.22, p < 0.05) (Table 2).
Correlations Between Limits of Stability and Functional Mobility
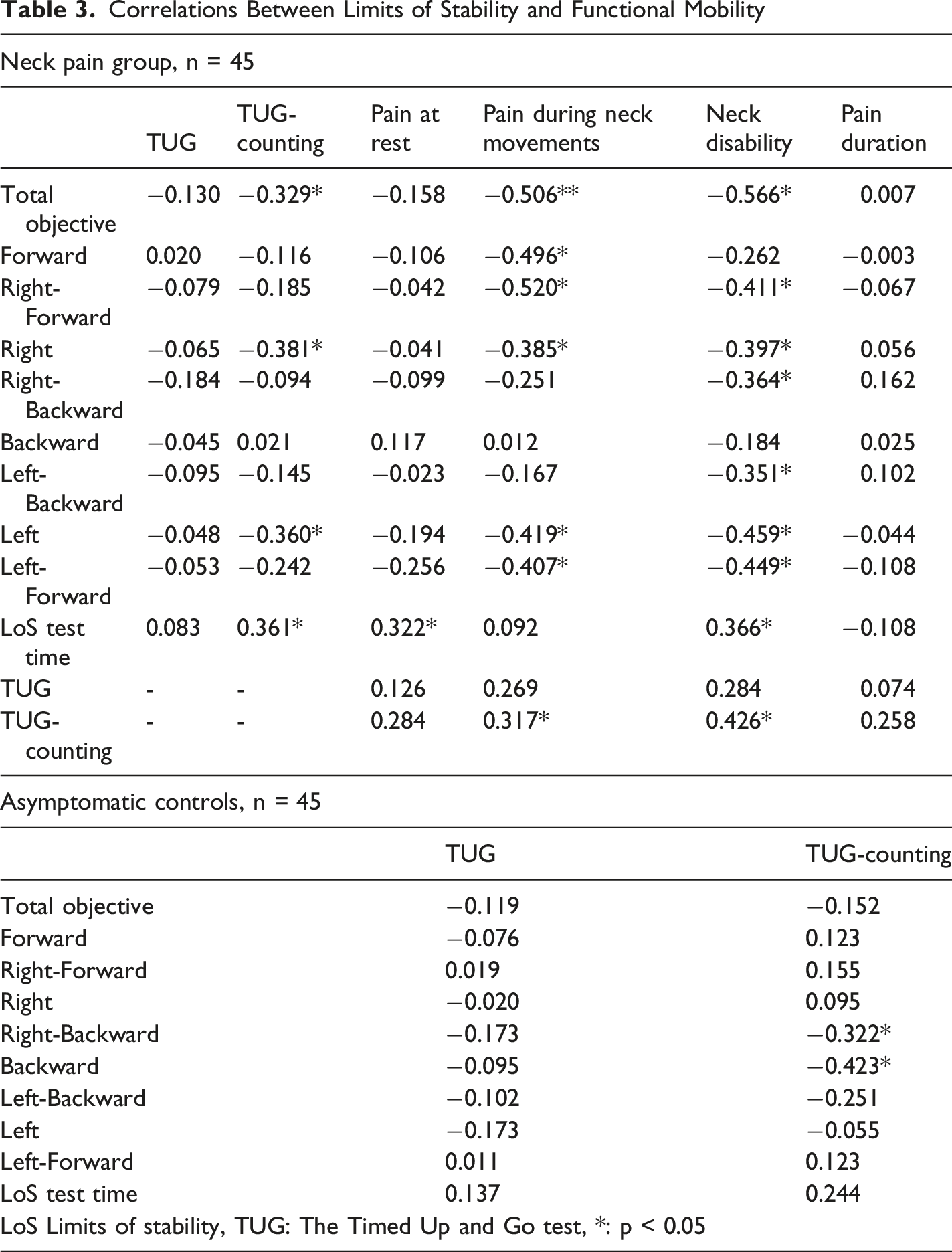
Pain intensity during neck movements was negatively and weakly to moderately correlated with the composite LoS score and the LoS scores in the forward, right-forward, right, left, and left-forward directions (r = −0.385 to −0.520, p < 0.05). Neck disability was negatively and weakly to moderately correlated with the composite LoS score and the LoS scores in the right-forward, right, right-backward, left-backward, left, and left-forward directions (r = −0.351 to −0.566, p < 0.05). The time taken to complete the LoS test was positively and weakly correlated with TUG time while performing the counting task, pain intensity at rest, and neck disability (r = 0.322 to 0.366, p < 0.05) (Table 3).
TUG time while performing the counting task was positively and weakly to moderately correlated with pain intensity during neck movements and neck disability (r = 0.317 and 0.426, p < 0.05). However, TUG time without a concurrent task was not significantly correlated with pain characteristics (p > 0.05) (Table 3).
Hierarchical Regression Analyses With the Composite Limits of Stability Score as the Dependent Variable in the Neck Pain Group, n = 45
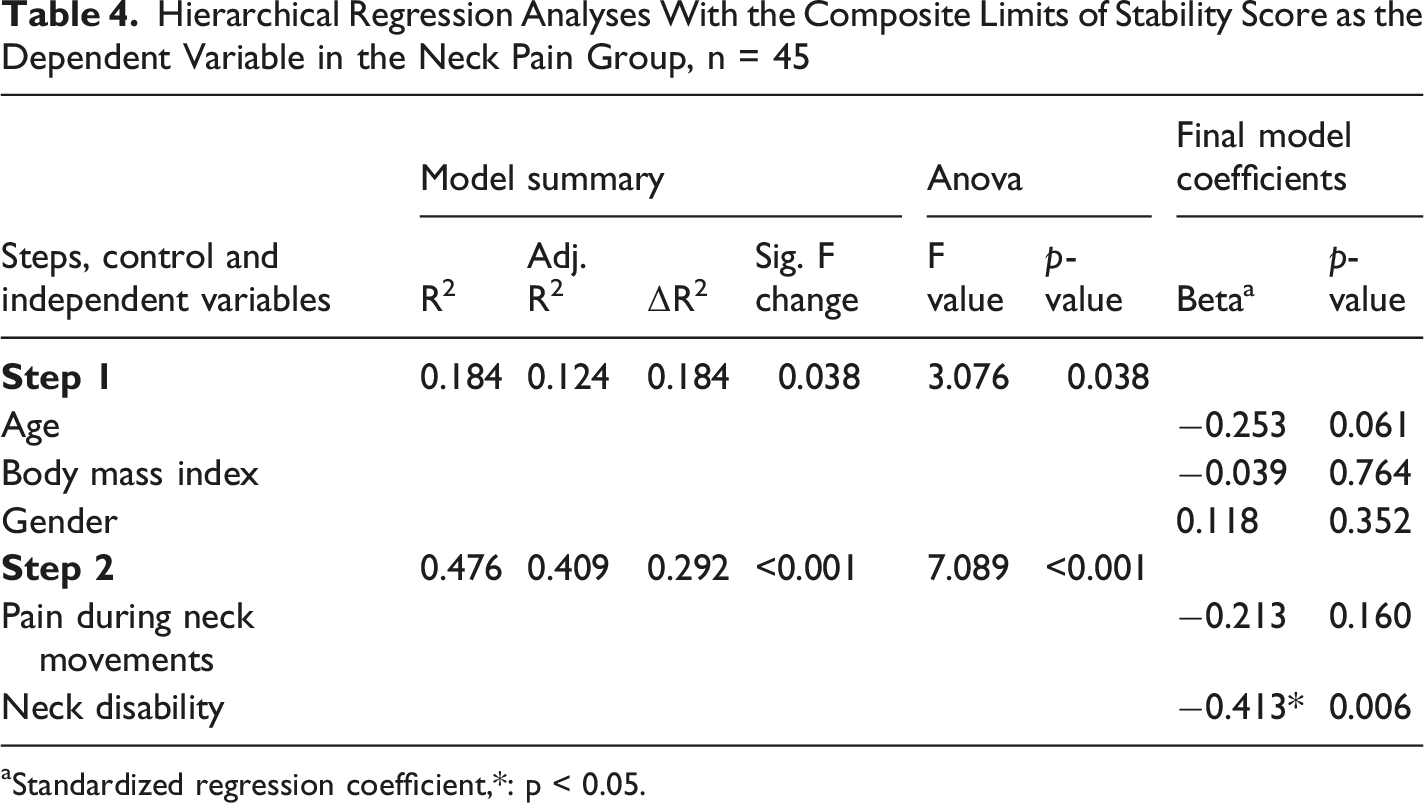
aStandardized regression coefficient,*: p < 0.05.
Hierarchical Regression Analyses With TUG Time While Counting as the Dependent Variable in the Neck Pain Group, n = 45
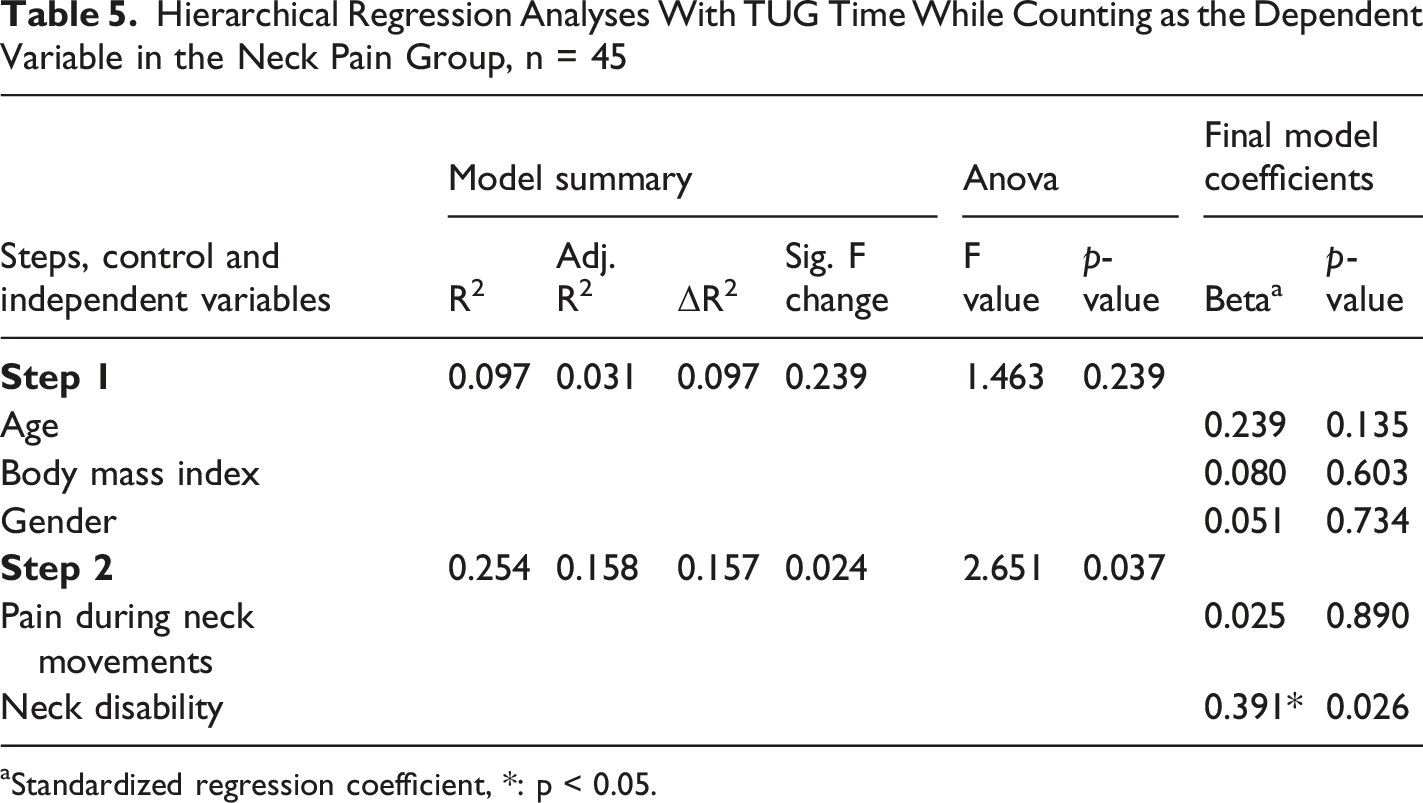
aStandardized regression coefficient, *: p < 0.05.
Discussion
The results indicated that adults with CNP exhibited lower LoS scores in all directions except forward and backward and longer TUG times. In both groups, higher LoS scores were correlated with shorter TUG times while counting, but not with TUG times without a concurrent task. Additionally, neck disability uniquely predicted both the composite LoS score (β = −0.413) and TUG time while counting (β = 0.391), after adjusting for demographics and pain intensity.
Gomes et al. compared anteroposterior and mediolateral stability limits assessed with functional and lateral reach tests between young adults with and without CNP, reporting that no statistically and clinically significant differences were found between groups (Gomes et al., 2018). Aslıyüce et al. compared dynamic balance assessed with Y Balance Test between adults with and without CNP and reported that the neck pain group had worse dynamic balance only in the anterior direction reach of the left leg (Özel Aslıyüce et al., 2022). In our study, the differences in stability limits were significantly greater compared to the two mentioned studies. This may be explained by two reasons: (1) the considerably higher mean age of our participants compared to the study by Gomes et al. and the substantially higher pain intensity and/or neck disability compared to both studies, and (2) the use of computerized posturography, which provides a more precise method for assessing balance performance. Alshehri et al. assessed LoS using a stabilometric platform and reported that older adults with CNP exhibited a lower composite LoS score compared to controls (Alshehri et al., 2025). Our study further suggests that LoS scores may also be lower in certain directions in adults aged 18–65 years with CNP.
Gomes et al. also reported that TUG time did not significantly differ between young adults with and without CNP (Gomes et al., 2018). We attribute the differences in TUG time comparison results to the considerably higher mean age of our participants and the substantially higher pain intensity and neck disability in the neck pain group compared to those in Gomes et al.'s study. There is also consistent evidence regarding reduced TUG times in older adults with CNP (Alshehri et al., 2025; Aslan Telci et al., 2019; Madsalae et al., 2022; Quek et al., 2014; Raizah et al., 2023;). Our study further suggests that TUG time, both with and without the counting backward by threes task, may also be longer in adults aged 18–65 years, most of whom experience moderate to severe neck pain with neck movements and mild to severe neck disability.
Gomes et al. reported that greater pain intensity during neck movements was weakly correlated with a lower anteroposterior stability limit assessed with the functional reach test in young adults with CNP (Gomes et al., 2018). Chaurangi et al. found that greater current pain intensity was moderately correlated with a lower modified star excursion balance test composite score in young adults experiencing neck pain for at least three weeks (Chaurangi & Varghese, 2020). In addition to demonstrating that greater pain intensity during neck movements and higher neck disability were weakly to moderately correlated with the composite LoS score and TUG score with the counting backward task, we identified neck disability as a unique predictor of these scores after adjusting for demographics and neck pain intensity. On the other hand, Alshehri et al. indicated that lower cervical flexor and extensor strength were moderately correlated with lower composite LoS score and longer TUG time in older adults with CNP (Alshehri et al., 2025). Raizah et al. reported that greater cervical joint position error was moderately correlated with longer TUG time in older adults with CNP (Raizah et al., 2023). In our study, higher LoS scores were correlated with shorter TUG time during the counting backward by threes task but not with TUG time without a concurrent task. Since TUG with a cognitive task is more challenging compared to standard TUG, it may have potentially revealed its relationship with stability limits.
There are several limitations in this study. First, pain-related fear of movement, which could potentially affect stability limits, was not assessed and should be addressed in future studies. Second, information regarding the use of medications such as analgesics or muscle relaxants prior to testing was not recorded; therefore, the potential effects of recent medication use on pain perception and balance performance cannot be ruled out. Additionally, the inclusion of a general adult population without consideration of specific occupational groups, such as sedentary workers or individuals engaged in physically demanding jobs, may limit the generalizability of the findings. Furthermore, comparing balance and functional mobility variables by grouping people with neck pain based on disability scores in larger sample sizes may provide further evidence on the effects of disability on these variables.
Conclusion
Adults with CNP exhibited lower LoS scores in all directions except forward and backward and longer TUG times. Higher LoS scores were correlated with shorter TUG times while counting backwards, but not with TUG times without a concurrent task. After adjusting for demographics, pain intensity during neck movements and neck disability explained an additional 29.2% of the variance in the composite LoS score and an additional 15.7% of the variance in TUG time while counting backwards. Additionally, neck disability uniquely predicted both the composite LoS score and TUG time while counting backwards, after adjusting for demographics and pain intensity. These findings suggest that future studies may examine whether improvements in neck disability are accompanied by changes in LoS and TUG, and whether interventions targeting neck disability alone are sufficient or if additional balance and functional mobility training is required. In addition, these parameters may be useful to consider during assessment, given that balance and functional mobility performance may decline with increasing levels of neck disability.
Footnotes
Acknowledgments
The authors acknowledge the support provided by TÜBİTAK (The Scientific and Technological Research Council of Türkiye) under the 2224-A Grant Program for ParThe ticipation in Scientific Meetings Abroad (2025/3 Term, Application No: 1919B022507577) for participation in ESMAC 2025, where this study was presented.
Ethical Considerations
Ethical approval for this study was obtained from Izmir Katip Celebi University Institutional Non-invasive Research Ethics Board (Number: 0210) on November 14, 2024. All procedures were conducted according to the Declaration of Helsinki. Participants read and signed the informed consent before their participation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.