
Abstract
Objective
To investigate ankle proprioceptive sensitivity under different position exposure times (PETs) and performance score relationship with the severity of perceived ankle instability in individuals with CAI.
Design
Test-retest reliability, cross-sectional comparative study.
Settings
University laboratory.
Participants
Forty-eight individuals (24 CAI, 24 non-CAI).
Outcome measure
Smartphone Proprioception for Ankle Navigation (SPAN) was used to assess active ankle movement proprioceptive performance under two PET conditions (0.25 s and 1 s). The symptomatic (CAI-SS) and asymptomatic side (CAS-AS) were tested and retested for reliability for CAI group, whilst randomly selected side of non-CAI group was tested once for between-group comparisons. Cumberland Ankle Instability Tool (CAIT) was self-administered to quantify perceived severity of ankle instability.
Results
Longer PET (1.0 s) improved proprioceptive sensitivity in non-CAI and CAI-AS groups but not in CAI-SS. Ankle proprioceptive performance at 1.0 s PET was significantly correlated with CAIT scores. SPAN test-retest reliability was influenced by PET, with similar ICCs for CAI-SS at both PETs but notable differences for CAI-AS.
Conclusion
This study highlights the temporal aspect of proprioceptive impairments associated with CAI as measured with SPAN. Individuals with CAI struggled to utilize prolonged exposure time to enhance proprioceptive sensitivity, and this limitation was significantly associated with the severity of perceived ankle instability.
Keywords
Introduction
Ankle sprains are among the most common lower limb injuries, and by one estimate, approximately 40–70% of previous acute ankle sprains could progress to chronic ankle instability (CAI) (Herzog et al., 2019; Zhang et al., 2022). As a leading musculoskeletal disorder, CAI is characterized by recurrent ankle sprains, a sense of ankle instability, and a series of neuromuscular control impairments, impacting on physical participation in daily life and sports (Hertel & Corbett, 2019; Shi et al., 2025). Ankle proprioception plays an important role in lower limb neuromuscular control (Cho & Kim, 2021; Shi, Cao, et al., 2023). Several systematic reviews have suggested that the ankle proprioception deficit associated with CAI may contribute to the development of CAI (Thompson et al., 2018; Xue et al., 2021). Accordingly, restoring proprioceptive performance has been a focus in CAI rehabilitation (Jain et al., 2014; Kabbaligere et al., 2017; Shi et al., 2019). Nevertheless, existing knowledge regarding the characteristics of the ankle proprioception deficit remains limited, and this poses challenges to tailoring proprioceptive assessment and rehabilitation programs for this condition.
Current evidence indicates that the proprioceptive deficit in CAI may be joint-specific (Han et al., 2013; Waddington & Adams, 1999), direction-specific (Xue et al., 2021), and task-specific (Han, Yang, et al., 2022; Kang et al., 2022). Specifically, proprioceptive impairments are mainly observed in the ankle joint, are more pronounced during inversion movements, and may become more evident under demanding functional tasks such as landing compared with standing. Collectively, these findings have expanded understanding of CAI, suggesting that ankle proprioception is not “globally” impaired in CAI and these detected impairment characteristics may affect the effectiveness of proprioceptive assessment and rehabilitation of CAI. While it has been well acknowledged that proprioception plays a pivotal role in movement control, effective motor control depends on the accurate integration of sensory information across both spatial and temporal domains. However, previous work focused on the spatially-related characteristics of proprioception, while possible temporally-related characteristics associated with CAI have not been well explored.
In our recent work, a novel, portable device, Smartphone Proprioception for Ankle Navigation (SPAN) was developed to assess temporally related aspects of ankle proprioception. SPAN was derived from the Active Movement Discrimination Apparatus (AMEDA) (Shi et al., 2023, 2024), with further modifications made to manipulate position exposure time (PET), or duration for “holding” target positions in testing proprioceptive sensitivity (Shi et al., 2024). In a healthy population, prolongation of the PET was found to be associated with better test performance but had poorer between-occasion SPAN-score reliability (Shi et al., 2024), possibly due to individual differences in processing temporally-related information in proprioceptive inputs.
The exposure time of an ankle position may affect proprioceptive performance in CAI. A previous network meta-analysis suggested that compared to a complex program incorporating dynamic balance exercise, a relatively simple static balance exercise program is more likely to improve ankle proprioception in CAI (Han, Luan, et al., 2022), suggesting that maintaining a target position for a longer duration may influence the time-related neuromuscular stimuli, thereby affecting the availability of proprioceptive afferents or somatosensory processing (Goble et al., 2010). Understanding temporally-related proprioceptive impairments associated with CAI would be important for exercise prescription for this condition. Accordingly, the first aim of this study was about to investigate ankle proprioceptive performance under different position exposure times (PETs). Secondly, ankle proprioception performance is associated with the perceived severity of ankle instability (Han et al., 2021; Shao et al., 2022; Wang et al., 2024). Previous work suggested that the relationships between spatial-domain proprioception measures and perceived ankle instability vary across different motor tasks. However, it remains unclear whether ankle proprioception performance is consistent across different PET conditions and, more importantly, whether variations in PET influence the association between ankle proprioception performance and the perceived severity of ankle instability. Addressing these questions may provide a deeper understanding of the characteristics of proprioceptive impairments in individuals with CAI and help inform the development of proprioception-targeted rehabilitation strategies. We hypothesised that individuals with CAI would not demonstrate improved ankle proprioception performance under prolonged PET conditions and that the inability to benefit from a longer PET would be associated with greater perceived ankle instability.
Method
Participants
This study included between-day test-retest trials and cross-sectional comparisons, examining side-to-side differences for individuals with unilateral CAI and between-group differences between individuals with and without CAI. As per the inclusion criteria of CAI by the International Ankle Consortium (Gribble et al., 2013), the eligible CAI cohort (1) were aged over 18 years; (2) had one previous significant ankle sprain at least within 1 year, (3) self-reported two or more episodes of recurrent ankle sprains or ankle giving way; and (4) scored less than 24 out of 40 in the Cumberland ankle instability tool (CAIT), a self-administered 9-item instrument used to define CAI. In the Chinese version employed, it has a sensitivity of 80.7% and specificity of 84.9% (Li et al., 2021). For non-CAI participants they had to be older than 18 but have neither previous ankle sprains nor mechanical laxity defined by the reverse lateral anterior drawer test (Li et al., 2020). Those individuals with a significant ankle sprain three months before the enrolment, previous lower limb fracture, impaired vision, hearing loss, or any central or peripheral nerve pathologies that may impair the sensory functions were excluded from the study.
In addition to defining CAI, CAIT was also used to quantify the perceived severity of ankle instability for all participants (Li et al., 2021). In this study, the CAIT was self-administered for the randomly selected side of the individuals without CAI, and the symptomatic side of individuals with CAI (CAI-SS). For the non-CAI group, the tested side was randomly determined using a computer-generated randomisation sequence prior to data collection. In the case of individuals with previous bilateral ankle sprains or re-sprains, the self-reported worst side was considered as the symptomatic side (CAI-SS), and the contralateral side was considered as the asymptomatic side (CAI-AS) (Wright et al., 2014). This study was approved by the Swinburne University of Technology Human Research Ethics Committee (Ref: 20236854-12249).
Experimental Procedure
The SPAN test apparatus was used in assessing ankle proprioception performance for both sides of the CAI cohort (i.e., CAI-SS, and CAI-AS), and for the randomly selected side in the non-CAI cohort. SPAN consisted of a smartphone, a rocker board, and a stable platform. In preparation for assessing ankle proprioception, an Android smartphone installed with a customized App was placed on the lateral side of a rocker board, with functions for gathering real-time orientation coordinates and releasing auditory instructions (Figure 1). Participants were instructed to stand on the centre of the rocker board, aligning the longitudinal axis of their ipsilateral foot with the rotation axis of the board, while placing the contralateral foot on a stable platform of equivalent height. They then rotated the board downwards in the frontal plane via active ankle inversion. The trial procedure was; rotate board downwards, stop when beeped, return board to neutral position (i.e., baseline), make a verbal position judgment. The SPAN system operated by detecting real-time tilt of the board in the frontal plane and creating the four different inversion tilt test positions, positions 1 to 4: 5°, 7°, 9° and 11°. The zero-degree tilt baseline position is presented by a low-pitched beeping released by the smartphone, while the four tilt positions are all presented by a consecutive high-pitched beeping (Figure 1). The duration of auditory beeping is adjustable which allows the generation of different position exposure times (PETs) for participants to memorize and encode different movements and position information. In this study, each testing side was assessed at a short (0.25 s) and a prolonged PET(1 s), respectively. Ankle proprioception assessment by using SPAN. (A) baseline position in the sagittal view (B) baseline position in the frontal view (C) level 1–4 position in the frontal view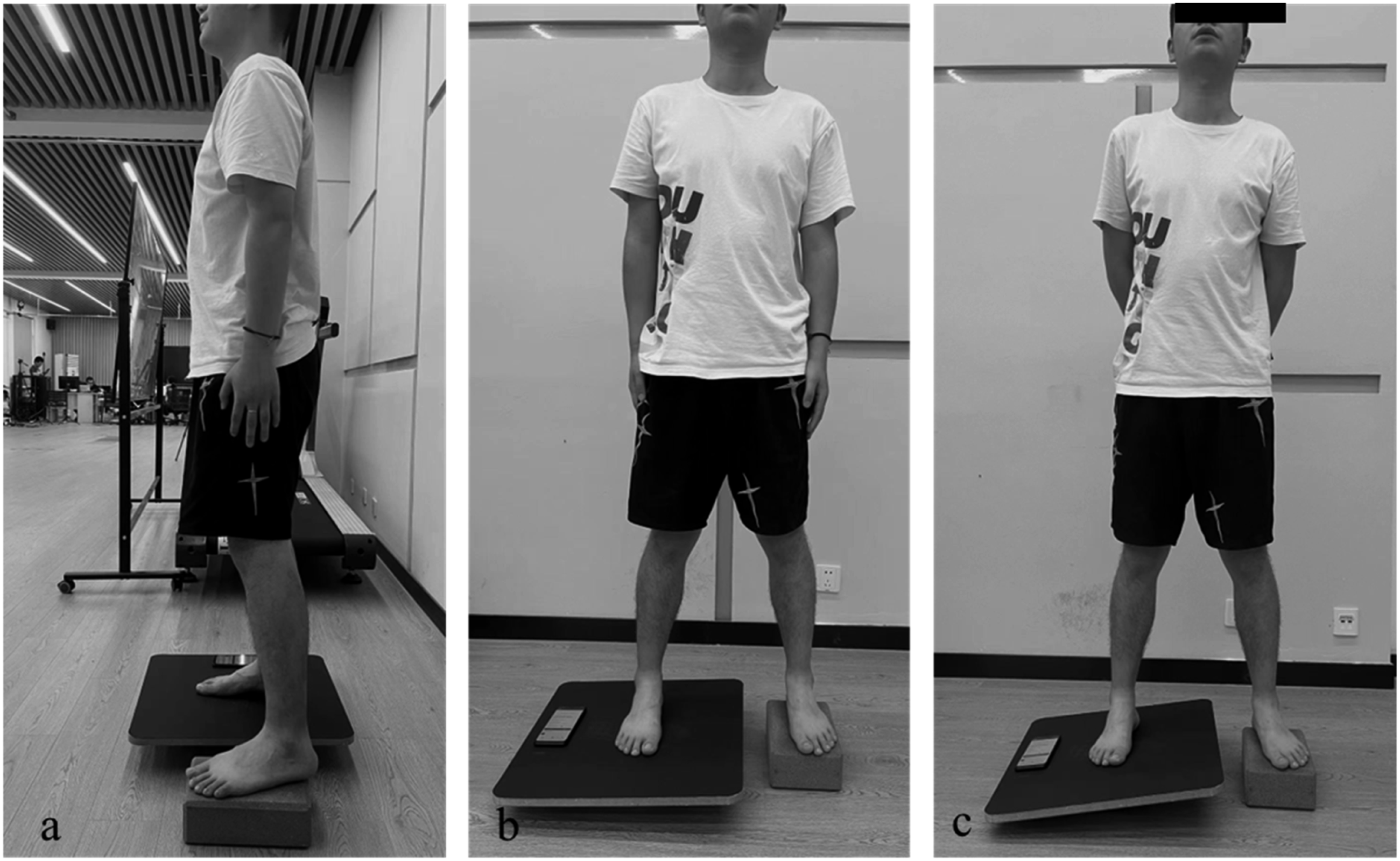
For each side being tested, a complete assessment consists of a familiarization session and a data collection session. In the familiarization session, the tested side is given 12 trials to experience the four tilt positions (i.e., targets), each with three presentations. For each trial, the participants are informed via sound prompts and then are instructed to start to rotate the board from the baseline position, downwards to one of targets. Then, they are required to hold this target upon the presentation of a high-pitched beeping, before returning upwards to the baseline (0°) position, represented by a low-pitched beeping, in preparation for the next trial. In the data collection session, each of the four targets is presented ten times in a random sequence; that is, 40 trials in total. For each trial, participants are required to rotate the board downwards to search for a position with high-pitched beeping, and thereafter orally report the perceived positions regarding these targets using numbers (i.e., 1–4) before the next trial starts.
Randomisation was conducted for both PET conditions and limb sides to minimise potential learning and fatigue effects. Notably, in the CAI group, both limbs (i.e., the CAI-SS and CAI-AS) were assessed within a single testing session, with up to 10 minutes provided for rest between assessments. The second testing session was completed within one week of the initial session and followed the same testing sequence for each participant.
Data and Statistical Analysis
All the numerical ankle inversion position responses were recorded, then paired with the actual position (i.e., level 1–4) to generate a 4 × 4 matrix, which was analysed using signal detection principles (Han et al., 2016). Receiver Operating Characteristic curves were generated based on three pairs of adjacent positions (1v2, 2v3, 3v4), and the mean Area Under the Curve (AUC) was calculated as the ankle movement discriminative ability score. An AUC close to or less than 0.50 indicated inferior ankle proprioception, suggesting random position judgments. Conversely, a score closes to 1.00 indicates excellent or superior ankle proprioception. Statistical analysis was performed via SPSS version 28.0.1.1 (IBM Corporation, Route 100, NY105089), with statistical significance set at a p-value of 0.05 or lower. Normality of all outcome data was examined using the Shapiro–Wilk test. Normally distributed data were described using mean ± standard deviation (SD), whereas non-normally distributed data were described using median and interquartile range (IQR; Q1–Q3). Demographic information was analysed with t tests and chi-square tests to determine the comparability between the two cohorts.
A two-way mixed effect intraclass correlation coefficient, i.e., ICC (3,1) was used to quantify intra-rater test-retest reliability, where values less than 0.5 are indicative of poor reliability, between 0.5 and 0.75 moderate reliability, between 0.75 and 0.90 good reliability, and 0.9 above excellent reliability(Koo & Li, 2016). Thereafter, the standard error of measurement (SEM) was calculated based on the ICC (3,1) value, through an equation that SEM equals pooled standard deviation (SDpooled) multiplied by the square root of 1-ICC. SEM was then used to calculate the minimal detectable changes at a confidence interval of 90% (MDC90). A two-way (2 × 3) repeated measure analysis of variance (ANOVA) was performed to explore Ankle (i.e., CAI-SS, CAI-AS, Non-CAI) and PET (i.e., 0.25 s, 1 s) main effects and their interactions, followed by t-tests to identify the origins of effects, i.e., paired t-test for side-to-side difference (CAI-SS vs CAI-AS) and within-group comparisons (0.25 s-PET vs 1 s-PET). Independent-groups t-tests were employed for between-group comparisons (non-CAI vs CAI-AS, or CAI-SS). Effect size was represented by using partial eta square(ƞp2), with a ƞp2 value equal to 0.01 representing a small size, 0.06 a medium effect size, and 0.14 a large effect size, respectively (Cohen, 2013). Pearson’s correlation analysis was used to examine the relationship between ankle proprioception performance measured under the two PET conditions in SPAN, while Spearman correlation analysis was conducted to investigate the associations between proprioception performance and CAIT scores. A r value less than 0.3 was recognized as poor correlation, 0.3 to 0.39 as weak, 0.4 to 0.7 as moderate, and 0.7 or above as strong; a rho value less than 0.2 was recognized as poor correlation, 0.2 to 0.39 as weak, 0.4 to 0.59 as moderate, and 0.6 or above as strong (Akoglu, 2018).
Results
Demographic Information for All Participants
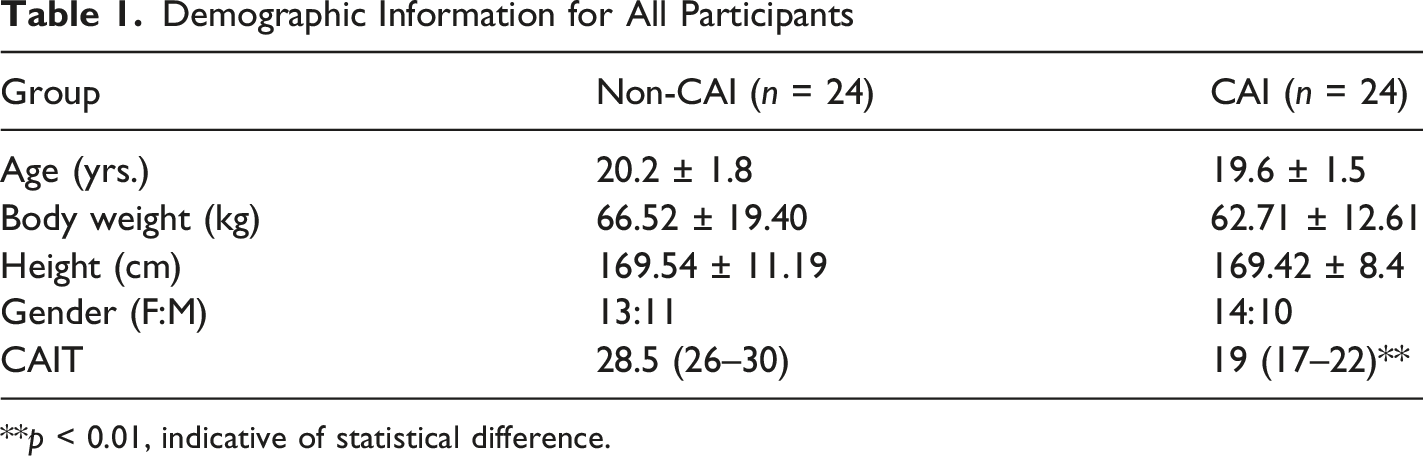
**p < 0.01, indicative of statistical difference.
Ankle Proprioception Scores Measured Under Different PET Conditions
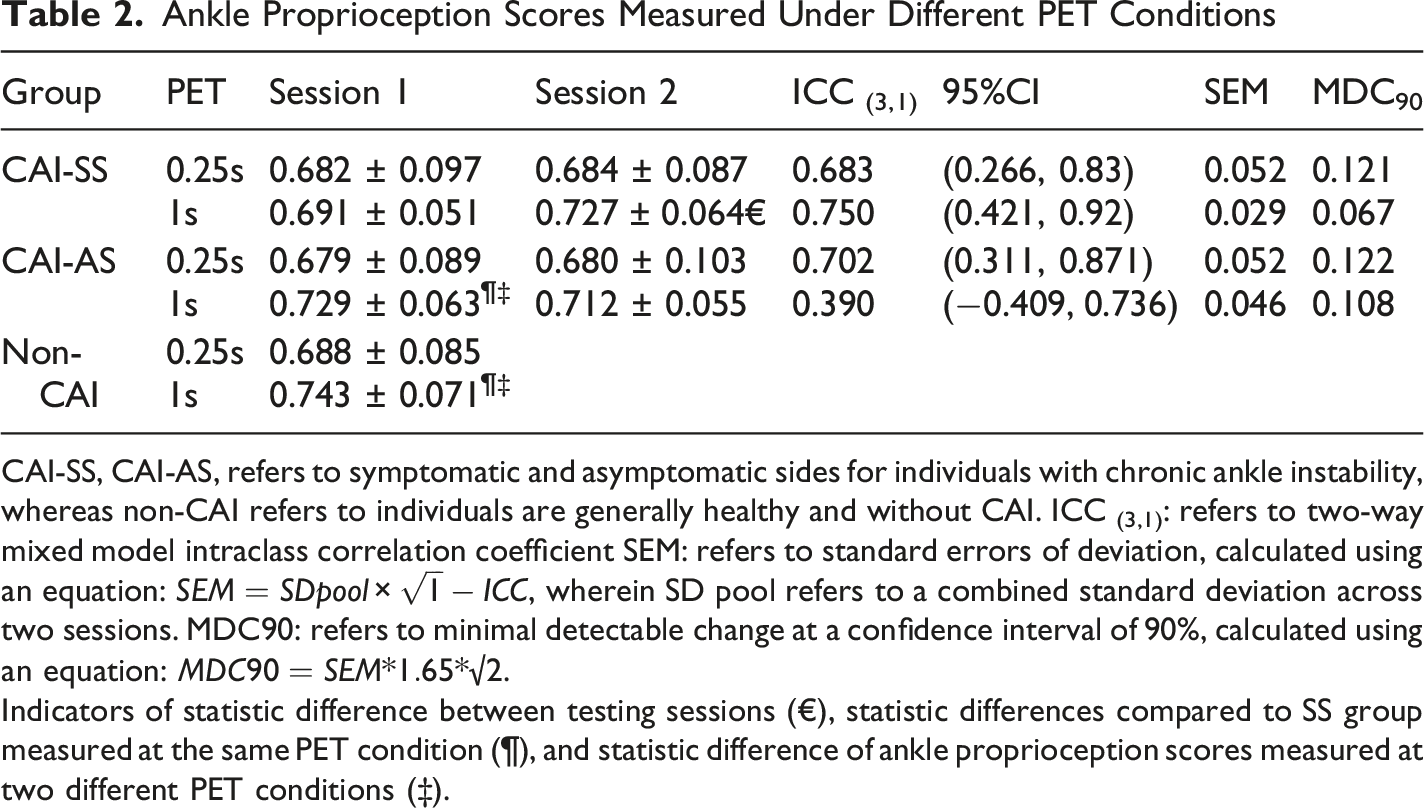
CAI-SS, CAI-AS, refers to symptomatic and asymptomatic sides for individuals with chronic ankle instability, whereas non-CAI refers to individuals are generally healthy and without CAI. ICC (3,1): refers to two-way mixed model intraclass correlation coefficient SEM: refers to standard errors of deviation, calculated using an equation:
Indicators of statistic difference between testing sessions (€), statistic differences compared to SS group measured at the same PET condition (¶), and statistic difference of ankle proprioception scores measured at two different PET conditions (‡).
Repeated measures ANOVA showed a significant PET effect (F = 14.01, p ≤ 0.001, ƞp 2 = 0.17), yet with neither Symptomatic/Asymptomatic Ankle effect nor interaction (all p > 0.05), with the overall ankle proprioception scores at a PET of 1.0s significantly higher than that at a PET of 0.25 s (Mean difference (MD) = 0.038, p ≤ 0.001). Notably, it was in the non-CAI cohort and the CAI-AS limb where ankle proprioception scores improved from the prolongation of PET (MD = 0.050–0.055, p = 0.001–0.013), not the CAI-SS (p > 0.05) (Figure 2). Ankle proprioception scores for the non-CAI and CAI-AS were comparable (p > 0.05); both were significantly higher than that for the CAI-SS at a PET of 1.0 s (MD = 0.052 ± 0.017, t = 2.91, p = 0.006; MD = 0.038 ± 0.012, t = 3.13, p = 0.05). In contrast, at a PET of 0.25 s, there were neither a significant intra-group nor inter-group difference (both p > 0.05) (Figure 2). As regards correlation analysis, ankle proprioception performance at the two PET conditions showed a moderate correlation with each other (r = 0.43, p = 0.002). CAIT scores demonstrated a weak but significant correlation with the ankle proprioception performance at a PET of 1.0 s (rho = 0.288, p = 0.047), but insignificant with that at a PET of 0.25 s (rho = −0.16, p > 0.05). Ankle proprioceptive scores of CAI and non-CAI participants at two PETs CAI-SS, CAI-AS: symptomatic side and asymptomatic side of individuals with chronic ankle instability (CAI); Non-CAI: individuals without CAI; PET: position exposure time. **p < 0.001, *p < 0.05, indicative of significant differences
Discussion
This study explored the temporal characteristics of SPAN-measured ankle inversion proprioception in individuals with CAI with the aim of evaluating test-retest reliability and performance differences under varying PET conditions (0.25 s vs. 1 s). Additionally, ankle proprioceptive performance was compared between the CAI and non-CAI cohorts to evaluate the discriminative ability of SPAN at both within- and between-group levels. Test-retest reliability analysis suggested that SPAN exhibited moderate between-days reliability at a PET of 0.25 s for both sides of individuals with unilateral CAI, whilst at a PET of 1 s, test-retest reliability was classified as good for the CAI-SS, but poor for the CAI-AS. At a PET of 1 s, SPAN demonstrated discriminative ability in distinguishing CAI-SS from CAI-AS, or non-CAI, and a weak but significant correlation with CAIT scores. Combined with our previous observation, SPAN showed opposite observations under a PET of 1 s, with the symptomatic ankles showing better test-retest reliability, in contrast to the asymptomatic or healthy ankles. Interestingly, several researchers have noted this phenomenon in terms of knee joint position sense (JPS), wherein pathological groups showed better intra-rater test-retest reliability, compared to healthy controls. Given that pain may be a factor, these authors pointed out that such observations can be insightful, as proprioception assessments primarily target pathological populations (Baert et al., 2018; Han et al., 2021; Smith et al., 2013).
Previous studies have reported that prolongation of the PET can demonstrate improvement of proprioceptive performance in healthy populations (Goble et al., 2010; Shi et al., 2024). However, the present study, based on the CAI cohort, produced a different effect. Specifically, no significant difference existed among the CAI-SS, CAI-AS and non-CAI at a PET of 0.25 s, while as the PET was prolonged to one second, ankle proprioceptive performance for the asymptomatic ankles (i.e., CAI-AS, Non-CAI) both improved, whereas the CAI-SS did not. With elongated PET-induced gains in ankle proprioceptive performance, CAI-AS and non-CAI showed better scores at a PET of 1.0 s. Thus CAI-SS demonstrated an inability to use exposure time-related proprioceptive information to achieve better movement control at the ankle. Consequently, the prolongation of PET further accentuated the inherited proprioceptive disparity between symptomatic and asymptomatic ankles. The observed mean difference values at a PET of 1 s for the CAI-AS and non-CAI relative to CAI-SS were between 0.038 and 0.052. Although these values did not exceed the calculated MDC90(0.067) for the CAI-SS, they were greater than both the ipsilateral SEM (0.029), a conventional estimate on measurement error, and the observed test-retest gains (0.036). This suggests that the observed differences were unlikely to be explained solely by random measurement variation or familiarization effects although they should be interpreted cautiously as they did not exceed the MDC threshold. Further investigations regarding SPAN are desirable to establish its anchor-based minimally clinical important difference (MCID) which (King, 2011), has argued may approximate to SEM rather than MDC (Turner et al., 2010).
We propose that the discriminative capacity of SPAN scores in relation to CAI may stem from the combined effect of introducing the PET variable and the unique design of SPAN. Unlike the original AMEDA methods that utilize a series of physical stops to restrain the extent of ankle inversion without the possibility of control of exposure time (Han et al., 2016), SPAN relies on “holding” strategies to ensure that ankle movement terminates; that is, the participants in this study were required to execute active control on each designated ankle inversion position. As previously suggested, a standing AMEDA protocol could not detect intra-group differences in this cohort (Han et al., 2021; Shi et al., 2023). In contrast, in the SPAN protocol, the prolongation of PET may result in more proprioceptive inputs or more processing in the somatosensory cortex, while the participants were required to execute eccentric eversion to “anchor” the movement status and position of the moveable board. Conceptually, the added active component regarding ankle inversion control in SPAN can align with neuromuscular control on the unstable surfaces. However, the current findings are not able to be ascribed to a standalone peripheral sensory deafferentation or centrally maladaptive plasticity (Freeman, 1965; Hertel, 2008). To determine the underlying mechanisms, more research work is warranted, firstly, to reveal the relationship between the activation of ankle evertors (e.g., peroneus longus) and SPAN-measured ankle proprioceptive performance. Previous research have proposed peroneal muscle strength weakness as one contributing factor for the development of CAI (Thompson et al., 2018). It is plausible that, in comparison to ankles without symptoms in this study (i.e., CAI-AS, non-CAI), CAI-SS with peroneal muscle weakness may have more challenges in “locking” the targeting joint position on the moveable component, so as to ensure the “steadiness” of proprioceptive inputs. Secondly, further research is warranted to understand the proprioception-mediated hierarchy and laterality during central motor processing. Some evidence has suggested that centrally involved proprioceptive impairments tended to be bilateral in individuals with unilateral CAI (Sousa et al., 2017; Wikstrom et al., 2010). The current results suggest that non-CAI showed similar ankle proprioception scores as the CAI-AS (i.e., 0.741 vs 0.729), without statistical significance.
In addition, this study also examined whether proprioceptive performance is associated with the severity of a CAI patient’s perceived ankle instability. Previously, task-specific AMEDA protocols showed significant correlations with Cumberland ankle instability tool (CAIT) scores (Han et al., 2021; Shao et al., 2023). As a well-recognized instrument used to quantify the perceived severity of ankle instability, the CAIT functions by collecting individuals' perceptions derived from recalled memories related to their ankle stability in the execution of daily and sports activities (Li et al., 2021; Wright et al., 2014). Likewise, relative to the conventional methods wherein participants were assessed in standing positions or on the dynamometer (Han et al., 2016), AMEDA-concept protocols were then modified by adding a more challenging motor task, e.g., walking (Huang et al., 2024) or landing (Kang et al., 2022), which further enhanced the spatially-related complexity of proprioceptive processing during the execution of movement tasks. However, such tasks may pose a risk of re-injury, and therefore might not be suitable for individuals with injury-related fear or persistent pain (Al Adal et al., 2019) and their applications may be not generalized to the other clinical populations with a severe neuromuscular disorder. e.g., stroke. In contrast, SPAN works to regulate the temporally related complexity of the proprioceptive process. Correlation analysis here suggested that ankle proprioceptive score at a PET of 1.0 s was moderately associated with that obtained at a PET of 0.25 s, which reflects the homogeneity of proprioceptive information captured by SPAN, irrespective of varied temporal parameters. In accordance with the previous findings from functionally-integrated AMEDA protocols (Han et al., 2021; Shao et al., 2023), SPAN showed a significant correlation with the CAIT scores at a PET of 1.0 s, indicating its concurrent validity in clinical practice. Moreover, the relationship reflected the detected ankle proprioceptive impairments at a prolonged PET condition, which together suggest that a rehabilitation program that intends to restore ankle proprioception accuracy for CAI cohorts should involve active and muti-changing ankle inversion control, such as “holding” for some seconds in different ankle inversion positions, given the pivotal role of the ankle joint in lower limb kinetics (Huang et al., 2024; Tait et al., 2022). This training strategy may potentially contribute to improving lower quadrant postural control and alleviating the perceived instability of the affected ankle during physical activity for this cohort.
This study was not without limitations. The sample size and a subsequent inability to perform subgroup analyses prevented control for some confounding factors (e.g., fitness level) that may affect ankle proprioception performance. This study also lacks other objective outcome measures to monitor the extent of muscle recruitment in the assessment. For example, the use of ergometers and EMG to investigate muscle activation at different PETs during the ankle proprioception assessment.
Conclusion
This study highlights the temporal aspect of proprioceptive impairments associated with CAI as measured with SPAN. Individuals with CAI were not able to use exposure time-related proprioceptive information to achieve better sensitivity scores, and this inability was significantly correlated with the perceived severity of ankle instability. Addition of factors such as the duration of “holding” ankle position in proprioceptive assessment may enhance neuromuscular rehabilitation programs.
Supplemental Material
Supplemental Material - Proprioceptive Impairment and Joint Position Exposure Time in Relation to Patient-Report Outcome With Chronic Ankle Instability
Supplemental Material for Proprioceptive Impairment and Joint Position Exposure Time in Relation to Patient-Report Outcome With Chronic Ankle Instability by Xiaojian Shi, Charlotte Ganderton, Roger Adams, Jia Han, Doa El-Ansary, Oren Tirosh in Perceptual and Motor Skills
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.